
Abstract
Urticaria is a common inflammatory dermatosis characterized by transient, usually intensely itching wheals mediated by mast cells. Urticarial lesions can also be mimicked by other skin diseases. Differential diagnoses of urticaria should be considered if the single urticarial skin lesion persists for more than 24 h, if hyperpigmentation, scaling, or blistering occurs, if the lesions are not itching, or if fever or arthralgias are reported. In these cases, histologic examination and thorough serologic diagnostic may help to differentiate other dermatoses, such as vasculitis, autoimmune bullous skin diseases, drug reactions, or autoinflammatory syndromes. This article summarizes common differential diagnoses of urticaria.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Urticaria is mast cell-mediated and characterized by transient wheals with anemic halo that last less than 24 h before fading to normal skin. Hives are itching, and in some cases a burning sensation is reported [1, 2]. Urticaria is a visual diagnosis; however, also other dermatoses present with urticarial skin lesions, for example, when erythematous, non-scaling, sharply demarcated, solitary or partly confluent papules to plaques are present.
Differential diagnoses of urticaria should therefore be considered if urticarial lesions persist for more than 24 h at the same site, the lesions heal with hyperpigmentation, or there is only moderate or no itching. The appearance of blisters or scaling would also be unusual. In these cases, the diagnosis of urticaria is unlikely, so further differential diagnoses should be clarified by histologic examination and serologic analyses. Lack of response to antihistamines and omalizumab (the recommended standard therapy for chronic spontaneous urticaria (CsU) [3]), as well as fever or joint symptoms, should also lead to additional diagnostics.
This article provides an overview of the diseases in which urticarial skin lesions may occur and thus should be differentiated from urticaria in terms of differential diagnosis. In the following, autoinflammatory diseases (e.g., Schnitzler syndrome), autoimmune bullous dermatoses (e.g., bullous pemphigoid), or drug reactions are presented as possible differential diagnoses of urticaria, but also assistance for the medical history and extended diagnostics is given.
Urticarial skin lesions in autoinflammatory and autoimmune diseases
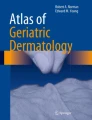
If general symptoms such as fatigue, arthralgia or fever occur simultaneously with the urticarial skin lesions [4, 5], a congenital or acquired autoinflammatory syndrome must be considered [3, 4]. In this case, the single urticarial lesion persists typically longer than 24 h, postinflammatory hyperpigmentation may occur, and burning, rather than itching is reported (Table 1). Histologic examination of a lesion reveals characteristic neutrophil-rich infiltrates, which, together with serology, allow a more accurate differentiation of differential diagnoses (Table 2). Neutrophil-rich infiltrates with urticarial skin lesions (Fig. 1a) typically occur in autoinflammatory diseases, such as Schnitzler syndrome ([6]; Fig. 1b), Still disease ([7]; Fig. 1c), or familial cryopyrin-associated periodic syndromes (CAPS) [8], but also in Sweet syndrome [9]. Rarely, they are also found in autoimmune (e.g., systemic and cutaneous lupus erythematosus) and rheumatic (e.g., rheumatoid arthritis) diseases.

a Clinical picture of a histologically neutrophilic urticarial dermatosis. b Schnitzler syndrome. c Still’s disease. d Hypocomplementemic urticarial vasculitis in subacute cutaneous lupus erythematosus. e Papular urticarial atopic eczema. f, g Granuloma annulare. h Erythema annulare centrifugum. i Maculopapular cutaneous mastocytosis. j, k Bier anemic spots, cyanosis, urticaria-like eruption (BASCULE) syndrome
Histologic examination can distinguish these differential diagnoses from urticaria. Recently, neutrophilic urticarial dermatosis (NUD) was shown in Schnitzler syndrome, Still’s disease, CAPS, collagenoses, or rheumatoid arthritis, which is characterized by a neutrophil-rich infiltrate with epitheliotropism of neutrophils on the epidermis and sweat glands [10,11,12]. Epitheliotropism is not found in urticaria.
The differential diagnoses of urticaria with emphasis on autoinflammation, Schnitzler’s disease, and CAPS were recently summarized in a comprehensive review [4].
In clinically similar urticarial vasculitis (Fig. 1d), which can be divided into normocomplementemic and hypocomplementemic forms [4], histologic changes include fibrin deposition in vessel walls typical of vasculitis [13]. From a histologic perspective, it is controversial whether urticarial vasculitis is a primary leukocytoclastic vasculitis or whether vessel wall damage is secondary due to a massive diapedesis of neutrophils with activation in the vessel environment. In line with this, a recently published paper suggests that normocomplementary urticarial vasculitis and CsU may be the same disease in some patients, albeit with different degrees of inflammatory activity [14].
Furthermore, a neutrophil-rich infiltrate is also present in delayed pressure urticaria [15], accompanied by painfulness and burning (in approximately 75% of patients) over and above itching [16].
Urticarial skin changes in inflammatory skin diseases
Urticarial skin lesions can also occur in very different inflammatory dermatoses. Histology helps to confirm the diagnosis in these cases. These include eczema diseases, such as atopic dermatitis in particular (Fig. 1e) or the annular plaques of granuloma annulare (Fig. 1f and g). Figurate erythemas may also resemble centrally fading, borderline wheals [17], such as early erythema annulare centrifugum when the typical scaling is still absent in the border region (Fig. 1h) or erythema marginatum in the prodromal stage of hereditary angioedema. Mast cell degranulation due to friction (“Darier sign”) in maculopapular cutaneous mastocytosis (formerly: urticaria pigmentosa; Fig. 1i) should not be confused with urticaria by definition. Transient urticaria-like changes also occur in BASCULE syndrome (Bier anemic spots, cyanosis, urticaria-like eruption), a vasomotor syndrome that occurs particularly in children on the lower extremity when standing and completely remits when walking or lying down (Fig. 1j and k; [18]).
Cryoproteinemia
Cryoglobulins are antibodies (mostly IgM) that precipitate at temperatures below 37 °C and cause skin symptoms such as acrocyanosis, cold-induced itching, erythema, and urticarial plaques as well as Raynaud’s phenomenon, livedo reticularis, or necrosis, especially on the lower legs [19]. They are classified as type I with monoclonal gammopathies (mostly IgG or IgM), type II with polyclonal IgG and monoclonal IgM, or type III with polyclonal IgG and IgM [19]. They occur in the context of plasmacytoma (type I), infection, especially with hepatitis C virus (80% of types II and III), or collagenosis (types II and III). The focus here is on treatment of the underlying disease.
Cold agglutinins are antibodies (mostly IgM, rarely IgG or IgA) that are able to bind to erythrocytes and thereby induce hemolysis [20]. Typical skin manifestations include cold-associated acrocyanosis, Raynaud’s phenomenon, to skin necrosis. The formation of cold agglutinins may be primarily due to autoantibodies or secondarily associated with viral (Epstein–Barr virus, hepatitis B/C, cytomegalovirus) or bacterial infections (Mycoplasma pneumoniae, Legionella, Chlamydia) as well as hematologic neoplasms (plasmacytomas, non-Hodgkin lymphomas) [20]. However, the correct quantification of cryoglobulins as well as cold agglutinins, collectively cryoproteins, is prone to artifacts due to sensitive transport conditions [19, 20]. While the analysis of cryoproteins was recommended in the 2011 urticaria guideline, it is not in the current guideline [1]. Although cold agglutinins were reported in 47% and cryoglobulins in 27% of patients with proven cold urticaria [21], a recent meta-analysis shows no association between cold urticaria and cryoglobulins [22], so that a different mechanism of cold urticaria must be assumed.
However, in the presence of an atypical history or clinic, unremarkable baseline diagnosis, and a severe form of cold urticaria, the differential diagnosis of cryoglobulinemia and symptomatic cold agglutinins should be considered.
Blistering autoimmune dermatoses
In the case of urticarial skin lesions, autoimmune dermatoses should be considered, especially in older patients, even without visible blisters. Such an initial, “premonitory” bullous pemphigoid (BP, Fig. 2a) or the recently described IgM pemphigoid [23] usually manifests with wheals, marked itching and scratch excoriations, without blister formation, and is therefore often misjudged as urticaria or eczema [24]. In the course, the typical bulging bullae first appear on healthy or urticarial skin (Fig. 2b and c). BP is mediated by tissue-derived and circulating autoantibodies directed against hemidesmosomal skin structural proteins (BP180/BPAG2/collagen XVII and BP230/BPAG1) [25]. These are mostly of IgG subtypes (Fig. 2d), IgA, IgM, and rarely IgE. These autoantibodies can be detected in serum by enzyme-linked immunosorbent assay (ELISA) and indirect immunofluorescence microscopy. This is supplemented by direct immunofluorescence microscopy of a perilesional biopsy taken at approximately 2 cm from the blister margin. For the therapy of bullous autoimmune dermatoses, clobetasol-containing externals on the entire integument [26] and oral dapsone are used initially. BP activity control is usually evident under these; in the short term, oral prednisolone may also be indicated (0.5–1 mg/kg body weight descending dosage for < 2 weeks). Limited efficacy has been shown for doxycycline. Immunosuppressants such as azathioprine or mycophenolate are available if dapsone is not tolerated or insufficient to control BP. In refractory disease, efficacy has been described for omalizumab, dupilumab [27,28,29], and rituximab, intravenous immunoglobulins, and/or plasmapheresis/immunoadsorption off-label in single cases or smaller cohorts of patients [26].

Differential diagnoses of urticarial exanthema: bullous autoimmune dermatoses and drug exanthema. a Overview of premonitory bullous pemphigoid (BP). b Thigh with initial bulla at BP manifestation. c Bulging bulla on urticarial plaque in BP. d Direct immunofluorescence with junctional IgG deposition in BP (green IgG-FITC, red Evans blue). e Urticarial plaque with excoriation in dermatitis herpetiformis Duhring. f Direct immunofluorescence with IgA deposits in the dermal papillae tips (green IgA-FITC, red Evans blue). g, h Drug exanthema after amoxicillin. i Urticarial plaques on the trunk after amoxicillin
Furthermore, urticarial skin lesions may occur in dermatitis herpetiformis Duhring (Fig. 2e). The lesions are intensely itchy and mostly localized on the shoulders, knees, and gluteal and occur in approximately 8% of patients with gluten-sensitive enteropathy (celiac disease) [30]. This disease is characterized by IgA antibodies against epidermal transglutaminase‑3 [31], whereas in celiac disease the IgA antibodies are directed against tissue transglutaminase‑2. The IgA deposits are detectable by direct immunofluorescence microscopy of the skin in the dermal papillary syringes (Fig. 2f). With strict avoidance of a gluten-containing diet, anti-eTG3 IgA antibodies decrease over time to below the detection limit. Under therapy with dapsone for a mean duration of 2 years, remission can be achieved on a gluten-free diet [32].
Drug reactions
In drug reactions, urticarial plaques can be caused by different mechanisms ([33]; Table 3). Anaphylaxis occurs after clinically inapparent sensitization on second contact with the allergen with IgE-mediated mast cell degranulation. The main anaphylaxis-inducing drugs are antibiotics and non-opioid analgesics, with different phenotypes described [34]. In addition to the exclusive reaction of the skin with urticaria, the respiratory organs, cardiovascular system, and/or gastrointestinal tract are also affected, depending on the trigger and individual factors. Drug exanthema of the late type (type Ivb; [35]; Fig. 2g, h, and i) should be differentiated. Diagnostics of choice are prick and intradermal testing, in special cases the titrated basophil activation test (BAT) and placebo-controlled exposure testing [36,37,38]. For therapy, it is initially important to stop the allergen intake, and in addition, depending on the severity, adrenaline, antihistamine, and glucocorticoids are indicated [36, 37].
Furthermore, non-allergic drug reactions (formerly “pseudoallergy”) may manifest as urticaria and angioedema. These may already occur at first contact, as for example the Mas-related G protein-coupled receptor X2 (MRGPRX2) is activated on mast cells in an IgE-independent manner [39, 40]. This receptor was described in 2015 and still all relevant ligands are not fully elucidated. By comparing patients with perioperative anaphylaxis and healthy individuals, it was shown under control by gene-silencing of MRGPRX2 that morphine derivatives, vancomycin, and cisatracurium can activate the receptor [41]. Ciprofloxacin, octreotide, paroxetine, clomipramine, icatibant, and vancomycin have also been identified as ligands in cell culture, preclinical models, and in some cases by skin testing [42]. The role of polymorphisms explaining the different triggers and responses is currently the subject of research.
Non-opioid analgesics (formerly NSAIDs) can trigger urticarial and non-allergic reactions in addition to type I allergic mechanisms via, for example, inhibition of Cox‑1 and secondary leukotriene elevation [43, 44]. As a consequence, a known CsU may exacerbate, a CsU may be triggered, or anaphylaxis may be induced. While acetyl-salicylic acid has been the most common trigger, ibuprofen is currently the causative agent with increasing frequency of use [43].
Urticarial skin lesions in food-induced anaphylaxis
If wheals occur intermittently and recurrently, urticarial exanthema may be a symptom of anaphylaxis. If the trigger cannot be determined from the patient’s medical history, a rare food allergy may be present. These include food-dependent exercise-induced anaphylaxis (FDEIA) and wheat-dependent exercise-induced anaphylaxis (WDEIA). In this case, urticarial exanthema or higher grade anaphylaxis occurs after consumption of gluten-containing foods in conjunction with physical exertion, infections, medications (especially non-opioid analgesics [NOAs] such as aspirin, diclofenac) or alcohol. Anti-tri a 19-IgE (omega‑5 gliadin) is detectable in the blood [45].
Also to be considered in case of nocturnal anaphylaxis or long delay to the last food intake is the alpha-Gal syndrome. This is typically triggered by a tick bite leading to sensitization to the animal sugar galactose-α‑1,3‑galactose (alpha Gal) and presents in the clinical effector phase after consumption of this sugar, which is mainly found in red meat [46].
In lipid transfer protein (LTP) syndrome, wheal formation or anaphylaxis can be triggered intermittently after consumption of fruits and vegetables, even in cooked form. The marker allergen for LTP syndrome is the heat-stable lipid transfer protein of peach (Pru p 3) [47].
A specific anamnesis for other symptoms of anaphylaxis is indicative of food-induced urticarial reactions in the sense of grade I anaphylaxis. These include a feeling of weakness, palpitations and restlessness as symptoms of cardiovascular reactions, a dry cough or whistling as involvement of the respiratory tract or gastrointestinal cramps, diarrhea and/or vomiting occurring simultaneously with skin symptoms in the case of gastrointestinal involvement.
Psychovegetative differential diagnoses
Finally, erythema and pruritus, especially on the upper trunk, décolleté, and neck in the setting of panic attacks or hypertensive crises can be observed. These skin lesions do not show the typical morphology of hives, are not elevated/tactile, and lack an anemic border. A recent example is the reaction after vaccination with a COVID-19 mRNA vaccine. Initial reports of allergic reactions in allergy patients were based on a clinical impression, and allergy diagnosis and workup of these reactions were incomplete. A careful workup of specialized allergy centers in Germany showed that an allergic sensitization is mostly not detectable, correspondingly no recurrence of symptoms upon re-vaccination and thus a psychovegetative genesis is likely [48]. In this case, the measurement of vital signs and blood pressure is helpful, as well as an accurate history of recent events and a tryptase determination within 1–3 h after the reaction to exclude mast cell activation.
Practical procedure
In the presence of urticarial skin lesions, a detailed medical history should be obtained, especially in the case of atypical findings. Table 1 provides information on important medical history questions for differential diagnosis. On physical examination, the skin lesions should be examined closely and, in addition to the typical morphology of hives, attention should be paid to details of differential diagnostic significance such as blisters, scaling, and purpura. In the case of chronic, recurrent skin lesions that are absent at the doctor’s appointment, photographic documentation by the patient is helpful. Tables 2 and 3 provide an overview of further diagnostic procedures for the classification of urticarial skin lesions.
Abbreviations
- Alpha Gal:
-
Galactose-α‑1,3‑galactose
- ANA:
-
Antinuclear antibody
- BASCULE:
-
Bier anemic spots, cyanosis, urticaria-like eruption
- BAT:
-
Basophil activation test
- BP:
-
Bullous pemphigoid
- CAPS:
-
Cryopyrin-associated periodic syndromes
- CBC:
-
Complete blood count
- CRP:
-
C‑reactive protein
- CsU:
-
Chronic spontaneous urticaria
- DPU:
-
Delayed pressure urticaria
- ELISA:
-
Enzyme-linked immunosorbent assay
- ESR:
-
Erythrocyte sedimentation rate
- FDEIA:
-
Food-dependent exercise-induced anaphylaxis
- Ig:
-
Immunoglobulin
- LTP:
-
Lipid transfer protein
- MRGPRX2:
-
Mas-related G protein-coupled receptor X2
- NSAID:
-
Non-opioid analgesics
- NUD:
-
Neutrophilic urticarial dermatosis
- SLE:
-
Systemic lupus erythematosus
- WDEIA:
-
Wheat-dependent exercise-induced anaphylaxis
References
Zuberbier T, Altrichter S, Bauer S, Brehler R, Brockow K. Dressler C et al. S3-Leitlinie Urtikaria. Teil 1: Klassifikation und Diagnostik der Urtikaria – deutschsprachige Adaptation der internationalen S3-Leitlinie. J Dtsch Dermatol Ges. 2023;21:81–95.
Kolkhir P, Gimenez-Arnau AM, Kulthanan K, Peter J, Metz M, Urticaria MM. Nat Rev Dis Primers. 2022;8:61.
Zuberbier T, Altrichter S, Bauer S, Brehler R, Brockow K, Dressler C, et al. S3-Leitlinie Urtikaria. Teil 2: Therapie der Urtikaria – deutschsprachige Adaption der internationalen S3-Leitlinie. J Dtsch Dermatol Ges. 2023;21:202–16.
Bonnekoh H, Krause K, Kolkhir P. Chronic recurrent wheals—If not chronic spontaneous urticaria, what else? Allergol. Select. 2023;7:8–16.
Matsuda T, Takimoto-Ito R, Lipsker D, Kambe N. Similarities and differences in autoinflammatory diseases with urticarial rash, cryopyrin-associated periodic syndrome and Schnitzler syndrome. Allergol Int. 2023;72:385–93.
Simon A, Asli B, Braun-Falco M, De Koning H, Fermand JP, Grattan C, et al. Schnitzler’s syndrome: diagnosis, treatment, and follow-up. Allergy. 2013;68:562–8.
Yamaguchi M, Ohta A, Tsunematsu T, Kasukawa R, Mizushima Y, Kashiwagi H, et al. Preliminary criteria for classification of adult Still’s disease. J Rheumatol. 1992;19:424–30.
Welzel T, Kuemmerle-Deschner JB. Diagnosis and Management of the Cryopyrin-Associated Periodic Syndromes (CAPS): What Do We Know Today? J Clin Med. 2021;10.
Cohen PR. Sweet’s syndrome—a comprehensive review of an acute febrile neutrophilic dermatosis. Orphanet J Rare Dis. 2007;2:34.
Broekaert SM, Boer-Auer A, Kerl K, Herrgott I, Schulz X, Bonsmann G, et al. Neutrophilic Epitheliotropism is a Histopathological Clue to Neutrophilic Urticarial Dermatosis. Am J Dermatopathol. 2016;38:39–49.
Ehrchen J. Neurophilic urticarial dermatosis. Hautarzt. 2016;67:403–13.
Gusdorf L, Lipsker D. Neutrophilic urticarial dermatosis: an entity bridging monogenic and polygenic autoinflammatory disorders, and beyond. J Eur Acad Dermatol Venereol. 2020;34:685–90.
Puhl V, Bonnekoh H, Scheffel J, Hawro T, Weller K, von den Driesch P, et al. A novel histopathological scoring system to distinguish urticarial vasculitis from chronic spontaneous urticaria. Clin Transl Allergy. 2021;11:e12031.
Bonnekoh H, Jelden-Thurm J, Allenova A, Chen Y, Cherrez-Ojeda I, Danilycheva I, et al. Urticarial Vasculitis Differs from Chronic Spontaneous Urticaria in Time to Diagnosis, Clinical Presentation, and Need for Anti-Inflammatory Treatment: An International Prospective UCARE Study. J Allergy Clin Immunol Pract. 2023;11(9):2900-2910.e21
Haas N, Toppe E, Henz BM. Microscopic morphology of different types of urticaria. Arch Dermatol. 1998;134:41–6.
Dover JS, Black AK, Ward AM, Greaves MW. Delayed pressure urticaria. Clinical features, laboratory investigations, and response to therapy of 44 patients. J Am Acad Dermatol. 1988;18:1289–98.
Boehner A, Neuhauser R, Zink A, Ring J. Figurierte Erytheme – Aktueller Stand und diagnostisches Vorgehen. J Dtsch Dermatol Ges. 2021;19:963–72.
Baurens N, Briand C, Giovannini-Chami L, De Guillebon De Resnes JM, Hubiche T, Chiaverini C, et al. Case Report, Practices Survey and Literature Review of an Under-Recognized Pediatric Vascular Disorder: The BASCULE Syndrome. Front Pediatr. 2022;10:849914.
Takada S, Shimizu T, Hadano Y, Matsumoto K, Kataoka Y, Arima Y, et al. Cryoglobulinemia (review). Mol Med Rep. 2012;6:3–8.
Gabbard AP, Booth GS. Cold Agglutinin Disease. Clin Hematol Int. 2020;2:95–100.
Bizjak M, Kosnik M, Terhorst-Molawi D, Dinevski D, Maurer M. Cold Agglutinins and Cryoglobulins Associate With Clinical and Laboratory Parameters of Cold Urticaria. Front Immunol. 2021;12:665491.
Ginter K, Ahsan DM, Bizjak M, Krause K, Maurer M, Altrichter S, et al. Cryoglobulins, Cryofibrinogens, and Cold Agglutinins in Cold Urticaria: Literature Review, Retrospective Patient Analysis, and Observational Study in 49 Patients. Front Immunol. 2021;12:675451.
Boch K, Hammers CM, Goletz S, Kamaguchi M, Ludwig RJ, Schneider SW, et al. Immunoglobulin M pemphigoid. J Am Acad Dermatol. 2021;85:1486–92.
Lamberts A, Meijer JM, Pas HH, Diercks GFH, Horvath B, Jonkman MF. Nonbullous pemphigoid: Insights in clinical and diagnostic findings, treatment responses, and prognosis. J Am Acad Dermatol. 2019;81:355–63.
Hammers CM, Stanley JR. Mechanisms of Disease: Pemphigus and Bullous Pemphigoid. Annu Rev Pathol. 2016;11:175–97.
Schmidt E, Sticherling M, Sardy M, Eming R, Goebeler M. Hertl M et al. S2k-Leitlinie zur Therapie des Pemphigus vulgaris/foliaceus und des bullosen Pemphigoids: 2019 Update. J Dtsch Dermatol Ges. 2020;18:516–27.
Lonowski S, Sachsman S, Patel N, Truong A, Holland V. Increasing evidence for omalizumab in the treatment of bullous pemphigoid. JAAD Case Rep. 2020;6:228–33.
Lamberts A, Kotnik N, Diercks GFH, Meijer JM, Di Zenzo G, Pas HH, et al. IgE autoantibodies in serum and skin of non-bullous and bullous pemphigoid patients. J Eur Acad Dermatol Venereol. 2021;35:973–80.
Olbrich H, Sadik CD, Ludwig RJ, Thaci D, Boch K. Dupilumab in Inflammatory Skin Diseases: A Systematic Review. Biomolecules. 2023;13:634.
Reunala T, Hervonen K, Dermatitis Herpetiformis ST. An Update on Diagnosis and Management. Am J Clin Dermatol. 2021;22:329–38.
Sardy M, Karpati S, Merkl B, Paulsson M, Smyth N. Epidermal transglutaminase (TGase 3) is the autoantigen of dermatitis herpetiformis. J Exp Med. 2002;195:747–57.
Elwenspoek MMC, Jackson J, O’Donnell R, Sinobas A, Dawson S, Everitt H, et al. The accuracy of diagnostic indicators for coeliac disease: A systematic review and meta-analysis. PLoS ONE. 2021;16:e258501.
Pichler WJ. Immune pathomechanism and classification of drug hypersensitivity. Allergy. 2019;74:1457–71.
Hanschmann T, Francuzik W, Dolle-Bierke S, Hofmeier KS, Grabenhenrich L, Rueff F, et al. Different phenotypes of drug-induced anaphylaxis-Data from the European Anaphylaxis Registry. Allergy. 2023;78:1615–27.
Torres MJ, Canto G. Hypersensitivity reactions to corticosteroids. Curr Opin Allergy Clin Immunol. 2010;10:273–9.
Ring J, Beyer K, Biedermann T, Bircher A, Fischer M, Fuchs T, et al. Guideline (S2k) on acute therapy and management of anaphylaxis: 2021 update: S2k-Guideline of the German Society for Allergology and Clinical Immunology (DGAKI), the Medical Association of German Allergologists (AeDA), the Society of Pediatric Allergology and Environmental Medicine (GPA), the German Academy of Allergology and Environmental Medicine (DAAU), the German Professional Association of Pediatricians (BVKJ), the Society for Neonatology and Pediatric Intensive Care (GNPI), the German Society of Dermatology (DDG), the Austrian Society for Allergology and Immunology (OGAI), the Swiss Society for Allergy and Immunology (SGAI), the German Society of Anaesthesiology and Intensive Care Medicine (DGAI), the German Society of Pharmacology (DGP), the German Respiratory Society (DGP), the patient organization German Allergy and Asthma Association (DAAB), the German Working Group of Anaphylaxis Training and Education (AGATE). Allergo J Int. 2021;30:1–25.
Muraro A, Worm M, Alviani C, Cardona V, DunnGalvin A, Garvey LH, et al. EAACI guidelines: Anaphylaxis. Allergy. 2021;2022(77):357–77.
Seidl U, Heine G. Principles of allergy diagnostics. Z Rheumatol. 2023;82:298–306.
McNeil BD, Pundir P, Meeker S, Han L, Undem BJ, Kulka M, et al. Identification of a mast-cell-specific receptor crucial for pseudo-allergic drug reactions. Nature. 2015;519:237–41.
Babina M, Guhl S, Artuc M, Zuberbier T. Allergic FcepsilonRI- and pseudo-allergic MRGPRX2-triggered mast cell activation routes are independent and inversely regulated by SCF. Allergy. 2018;73:256–60.
Navines-Ferrer A, Serrano-Candelas E, Lafuente A, Munoz-Cano R, Martin M, Gastaminza G. MRGPRX2-mediated mast cell response to drugs used in perioperative procedures and anaesthesia. Sci Rep. 2018;8:11628.
Kumar M, Duraisamy K, Chow BK. Unlocking the Non-IgE-Mediated Pseudo-Allergic Reaction Puzzle with Mas-Related G‑Protein Coupled Receptor Member X2 (MRGPRX2). Cells. 2021;10:1033.
Blanca-Lopez N, Soriano V, Garcia-Martin E, Canto G, Blanca M. NSAID-induced reactions: classification, prevalence, impact, and management strategies. J Asthma Allergy. 2019;12:217–33.
Kowalski ML, Makowska JS, Blanca M, Bavbek S, Bochenek G, Bousquet J, et al. Hypersensitivity to nonsteroidal anti-inflammatory drugs (NSAIDs)—classification, diagnosis and management: review of the EAACI/ENDA(#) and GA2LEN/HANNA. Allergy. 2011;66:818–29.
Scherf KA, Brockow K, Biedermann T, Koehler P, Wieser H. Wheat-dependent exercise-induced anaphylaxis. Clin Exp Allergy. 2016;46:10–20.
Steinke JW, Platts-Mills TA, Commins SP. The alpha-gal story: lessons learned from connecting the dots. J Allergy Clin Immunol 2015;135:589–96; quiz 97
Skypala IJ, Asero R, Barber D, Cecchi L, Diaz Perales A, Hoffmann-Sommergruber K, et al. Non-specific lipid-transfer proteins: Allergen structure and function, cross-reactivity, sensitization, and epidemiology. Clin Transl Allergy. 2021;11:e12010.
Worm M, Alexiou A, Bauer A, Treudler R, Wurpts G, Dickel H, et al. Management of suspected and confirmed COVID-19 (SARS-CoV-2) vaccine hypersensitivity. Allergy. 2022;77:3426–34.
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
M. Sulk received honoraria and travel support from AstraZeneca, Bencard, BioCryst, CSL-Behring, HAL Allergy, Novartis, Sanofi, Takeda, Unna Academy outside the submitted work; memberships in ABD, AeDA, DGAKI, EAACI. S.A. Braun received honoraria and travel support from Almirall, Amgen, Beiersdorf, Kyowa Kirin, Lilly, L’Oréal, Novartis outside the submitted work; memberships in ADF, ADH, DDG, ISDP. Financial support received from the German Federal Ministry of Research and Education (FKZ: 16KISA115K, 01IS22004B) and the EU (FKZ: 16KISA115K) and Galderma. C.M. Hammers received honoraria from JJP Biologics, Argenx and viDATherapeutics outside of this work. Financial support received from Deutsche Forschungsgemeinschaft, Collaborative Research Center (CRC) 1526—Pathomechanisms of Antibody-mediated Autoimmunity (PANTAU)—Insights from Pemphigoid Diseases (Grant No.: 454193335), Project A05. Memberships in DGAKI, DgfI, ADF, DDG, ESDR, JSID. G. Heine received honoraria from Allergopharma, Abbvie, Biotest, Eli-Lilly and Sanofi outside this work; memberships in DGAKI, DDG, DgfI, BDG, ABD, DKG. Financial support received from Deutsche Forschungsgemeinschaft, Collaborative Research Center (CRC) 1526—Pathomechanisms of Antibody-mediated Autoimmunity (PANTAU)—Insights from Pemphigoid Diseases (Grant No.: 454193335), Project A02 and S01. Memberships in ABD, DGAKI, EAACI. C.C. Albers and M. Wulf declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Sulk, M., Albers, C.C., Wulf, M. et al. Hives but no urticaria—what could it be?. Allergo J Int 32, 309–317 (2023). https://doi.org/10.1007/s40629-023-00274-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40629-023-00274-5