
Abstract
Racial minorities report lower perceived quality of care received compared to non-Hispanic White Americans, resulting in racial disparities in patient satisfaction. Medical mistrust, defined as a lack of confidence in the medical establishment and the intentions of medical personnel, is more prevalent among racial minority groups and is associated with poorer health outcomes. This study examines the prevalence and racial differences of patient/caregiver medical mistrust and its relationship to patient satisfaction among the pediatric patient population at a large urban academic medical center. A cross-sectional anonymous survey was conducted for caregivers of pediatric families seen at an urban tertiary care facility, including demographic information, the Patient Satisfaction Questionnaire (PSQ), and the Group-Based Medical Mistrust Scale (GBMMS). Linear regressions and mediation analyses were performed, examining race-based medical mistrust and associations with patient satisfaction. Sixty-seven surveys (67% Black/African American, 24% White) were completed. Black/African American participants reported higher levels of medical mistrust (M = 2.29, SD = 0.88 vs. M = 1.37, SD = 0.50; p < .001), which was associated with lower patient satisfaction (p < .001). In a parallel mediation analysis, disaggregating the GBMMS into three subscales, a significant indirect relationship emerged between race and patient satisfaction via the subscale lack of support from healthcare providers (95% CI [− 1.52, − .02], p < .05). Black/African American participants were more likely to have medical mistrust, and greater medical mistrust was significantly associated with lower patient satisfaction. Black/African American participants were significantly more likely to perceive lower support from healthcare providers which, in turn, was associated with lower patient satisfaction. These findings identify potential areas for intervention to improve Black/African American patients’ experience with healthcare.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
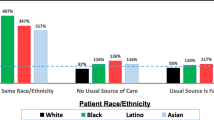
Racial and ethnic disparities in the overall quality of health and in healthcare access have been well documented in existing literature [1,2,3]. This includes significant disparities in healthcare-seeking behaviors among racial minority groups such as greater reliance on emergency medicine versus primary care services [4, 5]. Arnett et al. examined the usual source of medical care among 1408 Black/African American and White adults in the United States (US) and found that Black/African American patients were significantly more likely than White adults to endorse the use of the emergency department (ED) and hospital outpatient services compared to primary care services, even after adjusting for relevant demographic and health-related variables [4]. Other studies have supported these findings, showing that non-Hispanic Black/African Americans are twice as likely to use the ED compared to non-Hispanic Whites (80.4 vs. 43.5 visits per 100 person-years) [6] and less likely to report having a primary care provider [7]. The potential overreliance on ED services among racial minority groups may compromise their likelihood of receiving effective preventive care and adequate chronic disease management [8, 9].
Significant differences have also been reported in patients’ satisfaction with received care, with racial minorities more likely to report lower quality of care and communication-related problems with providers [10, 11]. A recent study using the Urban Institute’s Health Reform Monitoring Survey found that more than 20% of Black/African American families reported unfair treatment, a rate twice that of other races [12]. Various structural and social contributors to disparities in healthcare satisfaction have been highlighted in existing literature, one of which is medical mistrust [13].
Medical mistrust is conceptualized as a lack of confidence in the medical establishment or in the intentions and behavior of medical personnel [14]. Medical mistrust often develops as an adaptive mechanism to personally or vicariously experience group-based discrimination and/or differential treatment [15]. Existing literature has shown that Black/African Americans and other racial and ethnic minority groups are significantly more likely than non-Hispanic White individuals to experience discriminatory treatment both within and outside of the medical establishment [15, 16]. Self-reported and recounted discriminatory experiences, in turn, have been shown to predict greater mistrust in the healthcare system [17]. Thus, it is unsurprising that racial/ethnic minority groups, particularly Black/African Americans, often endorse significantly higher medical mistrust than non-Hispanic White Americans [17, 18]. Existing research has identified a significant association between medical mistrust, underutilization of healthcare services, and, for individuals who are care-engaged, lower patient satisfaction [19]. Additionally, the theoretical model entitled “Perceptions of Racism and Mistrust in Health Care” hypothesizes that perception of racism may influence cultural mistrust and thereby affect satisfaction with care [20]. Little is understood about these associations within the pediatric and pediatric caregiver populations, but evidence suggests there are differences in perception of care within these populations that require further study [12].
The objective of this study was to identify the prevalence and magnitude of medical mistrust, as well as the extent to which different dimensions of medical mistrust are associated with patient care satisfaction at a tertiary healthcare center in Baltimore, Maryland among caregivers of children in Pediatric ambulatory and inpatient care. This will add to the sparse literature on pediatric caregiver experiences of mistrust and directly address the associations of mistrust with patient satisfaction, which has not been wholly explored elsewhere for this population. Our aim was to optimize patient satisfaction by improving our understanding of the patient experience and subsequently developing interventions to enhance patient-provider interactions.
Methods
This study was conducted in October 2020 over a 2-week period using a cross-sectional survey. Prospective participants were recruited from an outpatient primary care clinic and general inpatient pediatric floor to capture a broader range of perspectives and lived experiences among participants. This study was approved by the University of Maryland Baltimore (UMB) institutional review board. To meet study eligibility, participants had to be aged 18–21 or caregivers of patients (if patient < 18 years of age), able to read and understand English, and physically or cognitively able to provide written responses. Prospective participants who met study inclusion criteria received written information about the study, as well as their rights as research participants, and informed consent was obtained from all individual participants included in this study. Participants completed a set of surveys with the average time for study participation/completion being approximately 5–10 min.
Race was assessed as part of a demographic questionnaire using a single multiple-choice item. Participants selected a race that best described them from the following options: (1) American Indian or Alaska Native, (2) Asian, (3) Black or African American, (4) Native Hawaiian/ Other Pacific Islander, (5) White, or (6) other race.
Medical mistrust was assessed using the Group-Based Medical Mistrust Scale (GBMMS). The GBMMS is a 12-item questionnaire that has been utilized and validated among diverse populations in the US [21,22,23]. Importantly, the GBMMS was not validated among adolescents < 18 at the time of this study, limiting enrollment to adult patients being treated in pediatric facilities, and caregivers of pediatric patients. The GBMMS uses a 5-point Likert-type scale for the response key, ranging from 1 (strongly disagree) to 5 (strongly agree). This assessment tool references previous experiences of race-based discrimination/differential treatment within the healthcare establishment as well as feelings of mistrust one holds toward healthcare workers, pharmacological treatment, and the medical care system at large [21]. The GBMMS can be used as a single measure (by calculating a single mean score) or can be broken up into three subscales, consisting of the suspicion subscale, the group disparities in healthcare subscale, and the lack of support from healthcare providers subscale. Prior studies have reported high internal consistency reliability between these subscales [21,22,23].
A modified version of the Patient Satisfaction Questionnaire (PSQ) was used to assess patient care satisfaction (adapted from Ware et al., 1983) [24]. The PSQ was modified for this study in order to address the specific purpose of the study and consisted of a 3-item self-report measure using a 5-point Likert-type scale for the response key, ranging from 1 (strongly disagree) to 5 (strongly agree). The modified PSQ included the following statements: “I’m very satisfied with the medical care I receive,” “If I have a medical problem, I can reach someone for help without any problem,” and “There are things about the medical care I receive that could be better.” Each item was utilized as a separate outcome measure to systematically examine potential differences in the relationship between race and medical mistrust for care satisfaction, help-seeking efficacy, and perception that improvement is needed in the care received.
General demographic information was collected as part of this study. This included age (years), self-identified race, ethnicity (Latina/Hispanic or non-Latina/Hispanic), and gender (woman, man, transgender woman, transgender man, gender queer, other, or I prefer not to say). Level of education (no diploma, high school diploma or the equivalent, some college but no degree, bachelor’s degree, master’s degree, or professional or doctoral degree) and household income (free response) were not analyzed separately, but these factors were adjusted for during data analysis.
Analysis
Statistical analysis was conducted using IBM SPSS Statistics Version 28. Pearson’s product-moment correlation was used to determine associations between the different variables of interest (degree of medical mistrust and patient satisfaction). A simple linear regression was utilized to determine the relationship between the continuous independent variable (i.e., medical mistrust) and the continuous outcome variable (i.e., level of patient satisfaction). As part of the data analysis, the Hayes PROCESS macro for SPSS (model 4) was also employed to assess the hypothesized single mediation models (Fig. 1). Mediation analyses were conducted adjusting for the following empirically or conceptually relevant background variables: age, gender, education, income, and location of service. Previous studies have reported high internal reliability between the GBMMS subscales using Cronbach’s alpha [21,22,23]; therefore, we assessed internal consistency reliability using Cronbach’s alpha.

Single mediation depiction of mistrust model
Results
There were 67 participants, seen at an outpatient primary care clinic or admitted to a general inpatient pediatrics ward. Of the total participants, 85% were parents/caregivers, and 15% were patients above the age of 18. Caregivers ranged in age from 22–40 years. Most identified as female, had less than a bachelor’s degree, and were employed either full or part-time. Over 60% reported an annual income below $40,000. Most participants self-identified as non-Hispanic, with 46% Black/African American, 24% White, and 3% reporting Hispanic/Latin origin.
Black/African American participants reported significantly more medical mistrust than White participants. However, there was no significant difference in care satisfaction by race (Table 1). In assessing bivariate relationships between race, medical mistrust, and patient satisfaction outcomes, race was significantly associated with medical mistrust but not directly related to any of the patient satisfaction outcomes. However, medical mistrust was significantly correlated with all patient satisfaction outcomes (Table 2).
A simple linear regression was conducted to determine the bivariate relationship between medical mistrust and the three outcome measures. Results suggested that medical mistrust predicts lower satisfaction with care (p < 0.001), lower confidence in being able to reach a provider for medical support (p < 0.001), and a greater likelihood of believing that the care they received could be better (p < 0.001). Single mediation analyses were conducted to determine the relationship between race and patient satisfaction outcomes (i.e., “satisfied with care,” “reaching for help,” and “could be better”) through medical mistrust. All mediation analyses were conducted adjusting for the following theoretically or empirically salient variables: age, gender, education, and location of service.
In the first mediation analysis, where “satisfied with care” was utilized as an outcome, there was no significant direct or indirect relationship between race and patient satisfaction through medical mistrust (model = − 0.1682, SE = 0.1647, 95% CI [− 0.5286, 0.1250]). When examining “reaching for help” as an outcome, a significant indirect relationship between race and outcome through medical mistrust emerged, such that Black/African American patients had significantly more medical mistrust, which, in turn, was associated with lower confidence in being able to reach a provider for help if experiencing a medical issue. In the final single mediation analysis utilizing “could be better” as the outcome variable, a significant indirect relationship emerged between race and this outcome through medical mistrust, such that Black/African American patients had significantly more medical mistrust, which, in turn, was associated with a higher rating on the item “There are things about the medical care I receive that could be better.”
An exploratory analysis was conducted using a parallel mediation model where the GBMMS was separated into three subscales (i.e., “suspicion,” “group disparities in health care services,” and “lack of support from health care providers”) and assessed as separate mediators in the relationship between race and the construct “satisfied with care.” A significant indirect relationship was noted between race and satisfaction with care through “lack of support from providers” (model = − 0.7002, SE = 0.3823, 95% CI [− 1.5206, − 0.0197]). Black/African American participants were more likely to perceive lower support from providers which was associated with lower satisfaction with care.
Internal consistency was assessed in this study with α = 0.95 for the full sample, α = 0.93 for the suspicion subscale, α = 0.91 for the group disparities in the healthcare subscale, and α = 0.75 for the lack of support from healthcare providers subscale, suggesting good internal consistency.
Discussion
The present study examined the relationship between medical mistrust and patient satisfaction and racial differences in those associations. Black/African American patients were more likely than White patients to have medical mistrust, and greater medical mistrust was significantly associated with lower patient satisfaction (Fig. 1). The structure of this study also allows for the exploration of different dimensions of mistrust (i.e., suspicion, perceived group disparities in healthcare subscale, lack of support from healthcare providers) (Fig. 2). In mediation analysis, there was a significant indirect relationship between race and satisfaction with care reported as “lack of support from providers,” suggesting that Black/African American patients were more likely to perceive lower support from providers which, in turn, was associated with lower patient care satisfaction.

Parallel mediation depiction of mistrust model
Medical mistrust has been shown to be significantly associated with worse outcomes across the healthcare continuum including underutilization of available healthcare resources and services [4, 25], lower levels of treatment adherence [26], and lower likelihood of participating in clinical research [27,28,29,30], translating to variations in both short-term and long-term treatment outcomes. This highlights the important implications of our findings for care delivery. In a meta-analysis of 47 studies, Birkhäuer et al. examined the relationship between trust and various health outcomes, identifying medical mistrust as a potential predictor of adverse clinical symptoms, poorer quality of life, decreased prevention-seeking behaviors, and lower satisfaction with received medical care [14, 31].
Present study findings are consistent with existing literature indicating race as a significant correlate to medical mistrust [17] and medical mistrust as a significant predictor of lower patient care satisfaction [19, 32]. In the context of such findings, it is important that health-promoting initiatives acknowledge potential historical and contemporary socio-structural contributors to medical mistrust among Black/African Americans and engage in efforts to reduce contributors to medical mistrust and mitigate the negative effects of medical mistrust among racial and ethnic minority patient groups.
Existing studies have indicated that a multicultural and diverse medical workforce is a potential avenue for cultivating greater trust among minority groups [33]. This may be accomplished through intentional efforts to recruit a diverse and multicultural student body in health professional schools and create the needed social infrastructure in medical schools and medical centers to accommodate for and encourage diversity and inclusion [34, 35]. A healthcare workforce that mirrors the patient demographic served can help engender greater trust, increase patient comfort, and may lead to positive medical outcomes [36]. Greenwood et al. found that Black/African American newborns who are cared for by White physicians are twice as likely to suffer mortality than when cared for by Black/African American physicians [37]. Such finding offers early indication into the protective potential of physician–patient racial concordance and underscores the importance of investing in a racially diverse and multicultural medical workforce that represents patient demographics.
In the present study, Black/African American patients disproportionally endorsed items suggesting a belief that providers do not have the best interest of their racial/ethnic group in mind, feel as if information is sometimes hidden from them, and note personal experiences of being treated poorly or unfairly by healthcare professionals. Existing literature suggests that race-based stereotyping and implicit bias can significantly contribute to unequal treatment/provision of medical services, even among physicians who believe provided care to be egalitarian [38]. It is imperative that medical training institutions and healthcare organizations actively engage in efforts that reduce race-based implicit biases among providers and enhance structurally informed and culturally sensitive care. Continuing efforts to address these potential areas of concern may increase patient satisfaction and help patients feel more confident and comfortable in reaching out for help when necessary, while simultaneously helping medical institutions to meet desired patient satisfaction metrics.
The main limitation of this study was that as a cross-sectional study, causation inferences are not possible. The sample size of the study and the fact that it is a single-institution study may limit its generalizability, thus supporting the need to expand this work to other institutions. The timing of this study may further limit its generalizability as it was conducted in October 2020, representing a period not only significant for its discussions of the impact of race and racism at a national level, which may have affected responses. Future studies are needed to determine the impact of this timeframe on results. The location of the study in Baltimore, MD may be a further limitation for generalizability, as social injustices and health disparities were spotlighted in this region after the death of Freddie Gray [39]. Additionally, this timeframe was amidst the COVID-19 pandemic, in which generalized mistrust of the US healthcare system increased overall, significantly higher among Black/African American persons and other marginalized communities [40,41,42]. Future studies should explore this impact and consider changes in outcomes over time. Furthermore, exploration of the effect of parental age and caregiver lived experiences may be important considerations in future studies, understanding that age and individual experiences can impact trust and engagement with the healthcare system [43]. Additional studies directly evaluating the pediatric population under age 18 and youth mistrust would add to current understanding.
Conclusion
The goal of this study was to examine the magnitude of medical mistrust among Black/African American and White patients and to assess the relationship between medical mistrust and patient care satisfaction. Black/African American patients had more medical mistrust than White patients, and medical mistrust was, in turn, significantly associated with lower patient satisfaction. This study suggests that efforts being undertaken to improve patient satisfaction may also demonstrate positive effects on medical mistrust, and future studies should consider this as an important outcome to evaluate. Further research is needed to demonstrate interventional approaches toward identifying and mitigating potential contributors to medical mistrust and to reduce the negative effects of medical mistrust among vulnerable populations in the US.
Data Availability
Data and analysis available upon request.
Code Availability
Not applicable.
Abbreviations
- PSQ:
-
Patient Satisfaction Questionnaire
- GBMMS:
-
Group-Based Medical Mistrust Scale
References
Penner LA, Hagiwara N, Eggly S, Gaertner SL, Albrecht TL, Dovidio JF. Racial healthcare disparities: a social psychological analysis. Eur Rev Soc Psychol. 2013;24(1):70–122. https://doi.org/10.1080/10463283.2013.840973.
Flores G. Racial and ethnic disparities in the health and health care of children. Pediatrics. 2010;125(4):e979–1020. https://doi.org/10.1542/peds.2010-0188.
Cheng TL, Emmanuel MA, Levy DJ, Jenkins RR. Child health disparities: what can a clinician do? Pediatrics. 2015;136(5):961–8. https://doi.org/10.1542/peds.2014-4126.
Arnett MJ, Thorpe RJ, Gaskin DJ, Bowie JV, LaVeist TA. Race, medical mistrust, and segregation in primary care as usual source of care: findings from the exploring health disparities in integrated communities study. J Urban Health. 2016;93(3):456–67. https://doi.org/10.1007/s11524-016-0054-9.
Parast L, Mathews M, Martino S, Lehrman WG, Stark D, Elliott MN. Racial/ethnic differences in emergency department utilization and experience. J Gen Intern Med. 2022;37(1):49–56. https://doi.org/10.1007/s11606-021-06738-0.
Rui P, Kang K, Ashman JJ. National Hospital Ambulatory Medical Care Survey: 2016 emergency department summary tables. Published 2016. Accessed January 19, 2024. https://www.cdc.gov/nchs/data/ahcd/nhamcs_emergency/2016_ed_web_tables.pdf.
Walls CA. The emergency department as usual source of medical care: estimates from the 1998 National Health Interview Survey. Acad Emerg Med. 2002;9(11):1140–5. https://doi.org/10.1197/aemj.9.11.1140.
Rust G. Practical barriers to timely primary care access. Arch Intern Med. 2008;168(15):1705. https://doi.org/10.1001/archinte.168.15.1705.
Maeng DD, Hao J, Bulger JB. Patterns of multiple emergency department visits: do primary care physicians matter? Perm J. 2017;21(2). https://doi.org/10.7812/TPP/16-063.
Saha S, Arbelaez JJ, Cooper LA. Patient–physician relationships and racial disparities in the quality of health care. Am J Public Health. 2003;93(10):1713–9. https://doi.org/10.2105/AJPH.93.10.1713.
Cuevas AG, O’Brien K, Saha S. African American experiences in healthcare: “I always feel like I’m getting skipped over.” Health Psychol. 2016;35(9):987–95. https://doi.org/10.1037/hea0000368.
Gonzalez D, et al. To what extent are parents and children exposed to bias and unfair treatment in health care?, Urban Institute. United States of America. 2023. Retrieved from https://policycommons.net/artifacts/4572207/to-what-extent-are-parents-and-children-exposed-to-bias-and-unfair-treatment-in-health-care/5395793/ on 23 Jun 2024
Hunt KA, Gaba A, Lavizzo-Mourey R. Racial and ethnic disparities and perceptions of health care: does health plan type matter? Health Serv Res. 2005;40(2):551–76. https://doi.org/10.1111/j.1475-6773.2005.00372.x.
Tekeste M, Hull S, Dovidio JF, et al. Differences in medical mistrust between Black and White women: implications for patient–provider communication about PrEP. AIDS Behav. 2019;23(7):1737–48. https://doi.org/10.1007/s10461-018-2283-2.
Ball K, Lawson W, Alim T. Medical mistrust, conspiracy beliefs & hiv-related behavior among African Americans. J Psychol Behav Sci. 2013;1(1).
Doescher MP. Racial and ethnic disparities in perceptions of physician style and trust. Arch Fam Med. 2000;9(10):1156–63. https://doi.org/10.1001/archfami.9.10.1156.
Bazargan M, Cobb S, Assari S. Discrimination and medical mistrust in a racially and ethnically diverse sample of California adults. Ann Fam Med. 2021;19(1):4–15. https://doi.org/10.1370/afm.2632.
Armstrong K, Ravenell KL, McMurphy S, Putt M. Racial/ethnic differences in physician distrust in the United States. Am J Public Health. 2007;97(7):1283–9. https://doi.org/10.2105/AJPH.2005.080762.
Molina Y, Kim S, Berrios N, Calhoun EA. Medical mistrust and patient satisfaction with mammography: the mediating effects of perceived self-efficacy among navigated African American women. Health Expect. 2015;18(6):2941–50. https://doi.org/10.1111/hex.12278.
Benkert R, Peters RM, Clark R, Keves-Foster K. Effects of perceived racism, cultural mistrust and trust in providers on satisfaction with care. J Natl Med Assoc. 2006;98(9):1532–40.
Thompson HS, Valdimarsdottir HB, Winkel G, Jandorf L, Redd W. The Group-Based Medical Mistrust Scale: psychometric properties and association with breast cancer screening. Prev Med (Baltim). 2004;38(2):209–18. https://doi.org/10.1016/j.ypmed.2003.09.041.
Shelton RC, Winkel G, Davis SN, et al. Validation of the group-based medical mistrust scale among urban Black men. J Gen Intern Med. 2010;25(6):549–55. https://doi.org/10.1007/s11606-010-1288-y.
Valera P, Boyas JF, Bernal C, Chiongbian VB, Chang Y, Shelton RC. A Validation of the group-based medical mistrust scale in formerly incarcerated Black and Latino men. Am J Mens Health. 2018;12(4):844–50. https://doi.org/10.1177/1557988316645152.
Ware JE, Snyder MK, Wright WR, Davies AR. Defining and measuring patient satisfaction with medical care. Eval Program Plann. 1983;6(3–4):247–63. https://doi.org/10.1016/0149-7189(83)90005-8.
LaVeist TA, Isaac LA, Williams KP. Mistrust of health care organizations is associated with underutilization of health services. Health Serv Res. 2009;44(6):2093–105. https://doi.org/10.1111/j.1475-6773.2009.01017.x.
Dale SK, Bogart LM, Wagner GJ, Galvan FH, Klein DJ. Medical mistrust is related to lower longitudinal medication adherence among African-American males with HIV. J Health Psychol. 2016;21(7):1311–21. https://doi.org/10.1177/1359105314551950.
Scharff DP, Mathews KJ, Jackson P, Hoffsuemmer J, Martin E, Edwards D. More than Tuskegee: understanding mistrust about research participation. J Health Care Poor Underserved. 2010;21(3):879–97. https://doi.org/10.1353/hpu.0.0323.
Smirnoff M, Wilets I, Ragin DF, et al. A paradigm for understanding trust and mistrust in medical research: the Community VOICES study. AJOB Empir Bioeth. 2018;9(1):39–47. https://doi.org/10.1080/23294515.2018.1432718.
Rajakumar K, Thomas SB, Musa D, Almario D, Garza MA. Racial differences in parents’ distrust of medicine and research. Arch Pediatr Adolesc Med. 2009;163(2):108. https://doi.org/10.1001/archpediatrics.2008.521.
Stevens EM, Patterson CA, Li YB, Smith-Whitley K, Barakat LP. Mistrust of pediatric sickle cell disease clinical trials research. Am J Prev Med. 2016;51(1):S78–86. https://doi.org/10.1016/j.amepre.2016.01.024.
Birkhäuer J, Gaab J, Kossowsky J, et al. Trust in the health care professional and health outcome: a meta-analysis. PLoS ONE. 2017;12(2):e0170988. https://doi.org/10.1371/journal.pone.0170988.
LaVeist TA, Nickerson KJ, Bowie JV. Attitudes about Racism, Medical Mistrust, and Satisfaction with Care among African American and White cardiac patients. Med Care Res Rev. 2000;57(1_suppl):146–61. https://doi.org/10.1177/1077558700057001S07.
Adams LM, Simoni JM. The need for multi-level mitigation of medical mistrust among social network members contributing to antiretroviral treatment nonadherence in African Americans living with HIV: comment on Bogart et al. (2016). Soc Sci Med. 2016;159:58–60. https://doi.org/10.1016/j.socscimed.2016.04.025.
Stanford FC. The importance of diversity and inclusion in the healthcare workforce. J Natl Med Assoc. 2020;112(3):247–9. https://doi.org/10.1016/j.jnma.2020.03.014.
Vereen RJ, Wolf MF. Physician workforce diversity is still necessary and achievable if it is intentionally prioritized. J Racial Ethn Health Disparities. 2024. https://doi.org/10.1007/s40615-024-01953-x.
Gomez LE, Bernet P. Diversity improves performance and outcomes. J Natl Med Assoc. 2019;111(4):383–92. https://doi.org/10.1016/j.jnma.2019.01.006.
Greenwood BN, Hardeman RR, Huang L, Sojourner A. Physician–patient racial concordance and disparities in birthing mortality for newborns. Proc Natl Acad Sci. 2020;117(35):21194–200. https://doi.org/10.1073/pnas.1913405117.
Hall WJ, Chapman MV, Lee KM, Merino YM, Thomas TW, Payne BK, Eng E, Day SH, Coyne-Beasley T. Implicit racial/ethnic bias among health care professionals and its influence on health care outcomes: a systematic review. Am J Public Health. 2015;105(12):e60-76. https://doi.org/10.2105/AJPH.2015.302903.
Alberti PM, Sutton KM, Cooper LA, Lane WG, Stephens S, Gourdine MA. Communities, social justice, and academic health centers. Acad Med. 2018;93(1):20–4. https://doi.org/10.1097/ACM.0000000000001678.PMID:28379933;PMCID:PMC5628097.
Minaya C, McKay D, Benton H, Blanc J, Seixas AA. Medical mistrust, COVID-19 stress, and intent to vaccinate in racial-ethnic minorities. Behav Sci (Basel). 2022;12(6):186. https://doi.org/10.3390/bs12060186.PMID:35735396;PMCID:PMC9219672.
Morgan KM, Maglalang DD, Monnig MA, Ahluwalia JS, Avila JC, Sokolovsky AW. Medical mistrust, perceived discrimination, and race: a longitudinal analysis of predictors of COVID-19 vaccine hesitancy in US adults. J Racial Ethn Health Disparities. 2023;10(4):1846–55. https://doi.org/10.1007/s40615-022-01368-6.
Allen JD, Fu Q, Shrestha S, Nguyen KH, Stopka TJ, Cuevas A, Corlin L. Medical mistrust, discrimination, and COVID-19 vaccine behaviors among a national sample U.S. adults. SSM Popul Health. 2022;20:101278. https://doi.org/10.1016/j.ssmph.2022.101278.
Katz E, Edelstein B, Turiano NA. Age as a moderator of health outcomes and trust in physicians. J Aging Health. 2024;36(5–6):308–19. https://doi.org/10.1177/08982643231187104.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by Rebka Tekeste and Rebecca Carter. Statistical analysis was performed by Natalie Davis and Mehrit Tekeste. The first draft of the manuscript was written by Rebka Tekeste, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics Approval
IRB approval was granted through the University of Maryland Medical Center Institutional Review Board. Ethics approval was not required.
Consent to Participate
Informed consent was obtained by all participants in this study.
Consent for Publication
Not applicable.
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Tekeste, R., Grant, M., Newton, P. et al. Prevalence of Medical Mistrust and Its Impact on Patient Satisfaction in Pediatric Caregivers. J. Racial and Ethnic Health Disparities (2024). https://doi.org/10.1007/s40615-024-02165-z
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1007/s40615-024-02165-z