
Abstract
Background
Idiopathic normal pressure hydrocephalus (iNPH) is a prevalent neurological disorder, but its diagnosis remains challenging. Dual-task (DT) walking performance is a reliable indicator of iNPH but less is known about the role of cognitive reserve (CR) in predicting DT walking performance.
Aims
The objective of this study was to evaluate the contribution of CR on DT walking in healthy controls (HC) and in iNPH patients (iNPH-P).
Methods
68 iNPH-P (77.2 +/- 6.7 years old) and 28 HC (74.5 +/- 5.7 years old) were evaluated on their single-task walking (Vsimple) and on 4 DT walking (walking and counting or counting backwards, naming animals, naming words beginning with the letter P) (Vcount, VcountB, Vanimals and Vletter respectively). The contribution of CR on the different DT walking speeds was compared between HC and iNPH-P. In iNPH-P, the contribution of CR on the walking speeds was compared with regard to other cognitive, functional, and socio-demographic variables.
Results
Simple linear regression demonstrated a moderate influence of CR on single and DT walking speed in iNPH-P (β > 0.3, p < .001) but not in HC where the relation was not significant. In iNPH-P, results showed that CR played a major role in explaining each of the single and DT walking speeds with NPH-scale.
Conclusion
As CR could be improved through the life cycle, these results support the idea of developing and supporting physical activity programs that will enrich social, physical, and cognitive resources to protect against age-related functional decline, especially in iNPH-P patients where the age-related deficits are greater.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Idiopathic normal pressure hydrocephalus (iNPH) is a prevalent reversible neurological disorder characterized by impaired locomotion, cognition, and urinary control with ventriculomegaly at brain imaging [1]. However, the diagnosis of iNPH remains challenging. Indeed, iNPH symptoms are not specific and can be found in other neurological disorders, such as Parkinson’s disease or Alzheimer’s disease (e.g. iNPH mimics) [2, 3]. There is also a lack of iNPH-specific diagnostic markers and several guidelines exist based on different criteria [4]. Therefore, depending on the guideline used, the prevalence of iNPH varies, which likely leads underdiagnosis [5]. The accuracy of diagnosing patients with iNPH can also be debated, as less than 60% of iNPH patients showed improvement after treatment [6]. This directly impacts the cost-effectiveness of the shunt intervention. However, recent studies found that adding dual-task walking to the cerebrospinal fluid tap test (CSF) may help to identify iNPH from its mimics [7, 8]. Indeed, iNPH patients were differentiated from the mimics by a greater improvement of their dual-task gait parameters (walking speed, stride length, step width, and stance duration) after the CSF tap test while, in single-task walking, gait improvements after the CSF tap test were similar between iNPH patients and iNPH mimics [8]. The difference in DT between the mimics and the patients could possibly be due to the lack of cognitive resources in iNPH patients which may resulted in greater impairments in DT before the CSF tap test. However, after the removal of the iNPH symptoms with the CSF tap test, it is conceivable that the DT walking would be largely improved compared to the mimics.
Indeed, dual-tasking consists of the simultaneous execution of two tasks, generally cognitive and/or motor tasks of different levels of complexity (for example, counting while walking). Under DT conditions, performance of one or both tasks can vary relative to single conditions because of competing demands. They are due to insufficient attentional resources or an inability to share these limited attentional resources between two or more concurrent tasks, thus causing a decline in performance [9, 10]. Resource competition has been found to be particularly pronounced in older adults with limited cognitive resources like in iNPH, and the DT paradigm has emerged as a promising marker for predicting cognitive impairment [11,12,13], fall risk [13,14,15] or frailty status [16,17,18] in older adults. However, the dual-task performance is not well understood as it could depend on many different factors such as age, frailty or other aspects of cognitive, physical/functional, psychosocial or social–demographic aging [18, 19].
The cognitive reserve (CR) strongly relies on the idea that there can be individual differences in how tasks are processed that can allow some people to cope better than others with brain changes in general and aging in particular [20]. CR suggests that the brain actively attempts to cope with brain damage by using pre-existing cognitive processes or by enlisting compensatory processes [21]. A recent study showed that CR played a role of moderator in the relationship between gait velocity under single and dual-task conditions and incident mobility impairment [22]. In other words, slower single-task walking and dual-task walking velocity predicted incident mobility impairment only among those individuals with low CR [22]. It is, thus, necessary to better understand which specific factors could influence dual-task walking performance in iNPH population as dual-task walking can help therapeutic decisions for neurosurgical shunt placement.
This study aims to evaluate the contribution of CR on DT walking in healthy controls (HC) and iNPH patients (iNPH-P). Our first hypothesis was that the relation between CR and dual-task walking is higher in iNPH-P compared to HC. The second hypothesis was that a high level of CR measured by the level of education is positively correlated with a high dual-task walking speed in each speed condition and that this variable contributes more importantly to the dual-task walking speed than other specific clinical measures in iNPH-P.
Materials and methods
Participants
Sixty-eight iNPH patients (iNPH-P) and 28 healthy controls (HC) were included in this retrospective study from the NPH cohort recruited at a tertiary referral hospital between March 2017 and February 2020 according to a previously described protocol [7]. Briefly, iNPH-P patients were recruited when they met the iNPH consensus guideline criteria [1]. The patients’ gait was analyzed twice, before and then 24 h after a CSF tapping of 40 ml according to a standardized protocol [7, 23]. Exclusion criteria included: acute medical illness in the past three months, orthopedic or rheumatologic disorders interfering with gait, patients receiving CSF tapping in the 3 months preceding the assessment, a change in the treatment between the two gait assessments, unable to walk a minimum of 15 m without a walking aid and not able to perform the dual-task evaluation (walking while backward counting, naming animals or letter). Gait disorders, cognitive impairment, and urinary disturbance were graded using the iNPH grading scale [24]. The iNPH grading scale was used to separately evaluate the severity of each of the three disorders. The score of each domain ranges from 0 to 4 with higher scores indicating worse symptoms. The study protocol was approved by the Institutional Review Board of the Geneva University Hospital (Protocol 09-160R). All subjects gave informed consent according to the ethical standards set forth in the declaration of Helsinki (1983).
Dual-task gait protocol
Patients were asked to walk at their self-selected speed on a 10-m walkway in single and in four randomized dual-task conditions: forward counting from 1 (Vcount); backward counting from 50 (VcountB); phonemic verbal fluency (enumerating words starting by letter p) (Vletter); and categorical verbal fluency (generating animals’ name) (Vanimals). A standardized instruction for the dual-tasks was given by the physical therapist: to walk and to perform the cognitive task at the best of their capacity without prioritization. Mean value and coefficient of variability of spatiotemporal gait parameters (that include walking speed) were computed based on the measurement of the heel marker trajectories on a 10 meters’ distance with an optoelectronic system including 12 cameras (Oqus7+, Qualisys Sweden). The gait assessment was conducted before and 24 h after CSF tap test pre-CSF tap test, which is described in the Geneva’s protocol [7].
Cognitive reserve
CR could be estimated using different proxies such as the level of education, premorbid intelligence quotient (IQ) or vocabulary size measured by the number of words pronounced in 1mn [21, 25]. In this study, CR was measured with the level of education measured in three categories (1, 2 and 3, respectively up to 9 years of education or elementary school, 9–12 years or apprentices, more than 12 years, or higher education) in HC and iNPH-P and expressed in years in iNPH-P.
Covariates
Then, the influence of CR was compared with other variables such as age and gender as socio-demographic variables, the total score of MMSE (Mini mental State Examination) as an indication of the cognitive function, NPH scale, disease duration in months, the age-related white matter changes (ARWMC) and global health status score (GHS) as functional/physical variables. Specifically, the NPH grading scale allows quantifying the NPH symptoms in gait, cognition, and miction using a Likert scale from 0 to 12 [24]. The ARWMC was used to quantify the burden of white matter disease in all the brain and its sub-regions [26]. Then, the GHS (0–10) summarizes the presence of the following comorbidities: diabetes, chronic heart failure, arthritis, hypertension, depression, stroke, PD (Parkinson’s disease), chronic obstructive pulmonary disease, angina, and myocardial infarction [27].
Statistics
Descriptive statistics presented socio-demographic variables and all the dual-task walking speed conditions (Vsimple, Vcount, VcountB, Vanimals, Vletter) in iNPH-P and HC participants (Table 1). Student’s t-test was applied, or Mann-Whitney when the variable deviated from normality, to compare each variable between the two groups. Then, a simple linear regression was applied between each speed (Vsimple, Vcount, VcountB, Vanimals and Vletter) and CR measured with the level of education in category (0–3). A comparison of the relation between the influence of CR on the different speeds between NPH-P and NPH-C was assessed with a two-way ANOVA with each speed as a dependent variable and the level of education (1–3) and groups (iNPH-P, HC) as fixed factors. To go further on iNPH-P group only, a Spearman’s rho correlation or Pearson was applied when appropriated between the 5 walking speed conditions (Vsimple, Vcount, VcountB, Vanimals, Vletter) and age, gender, CR, MMSE, NPH-scale, disease duration, ARWMC and GHS separately. To determine which of these 8 variables can better influence the walking speed in single and DT walking conditions, multiple linear regression analysis (MLRA) was applied to each of the walking speed condition as dependent variables with the covariates mentioned above which are age, gender, CR, MMSE, NPH-scale, disease duration, ARWMC and GHS. The MLRA was used with the stepwise method that removed at each step the least useful predictor. For each of the simple or multiple linear regression, normality, or skewness around − 2 and 2 was checked as well as heteroscedasticity and collinearity (VIF < 5). The independence of errors was also checked with a Durbin-Watson value between 1.5 and 2.5. All statistical analyses were performed with JASP (version 0.16.6, JASP Team (2023), The Netherlands).
Results
Sixty-eight iNPH-P (mean aged: 77.2 +/- 6.7 years old) and 28 HC (mean aged: 74.5 +/- 5.7 years old) were recruited for this study (Table 1).
Concerning the influence of CR measured with the level of education in categories on each of the different walking conditions, the simple linear regression was only significant in iNPH-P compared to HC where the regression was not significant (Table 2). There was also a moderate positive association between CR and the different walking conditions in iNPH-P as shown by the standardized coefficient in the linear regression (β > 0.4, p < .001) (Table 2). Thus, the influence of CR on the different walking speeds seemed to be applicable only in iNPH-P.
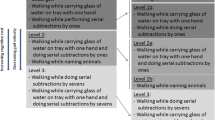
Also, ANOVA results highlighted that the different walking speeds were not significantly different among the different CR levels (1, 2 or 3 based on their educational level) (CR: p > .05) except for Vletter (p = .029) where the walking speed significantly increase with a higher level of CR (Fig. 1). However, all the walking speeds were significantly higher in HC compared to iNPH-P (GROUP: p < .001) (Fig. 1). No significant differences were found in the effect CR (1, 2, 3) *group (iNPH-P, HC) (p > .05).

ANOVA results with errors bars (confidence intervals 95%) comparing walking speeds (Vsimple, Vcount, VcountB, Vanimals and Vletter) between GROUPS (HC and iNPH-P) through their different educational levels (CR). Each p-value for the independent variable GROUP and CR is shown. *p < .05, **p < .01, ***p < .001
When focusing only on iNPH-P, correlation coefficients highlighted that only NPH-scale was significantly correlated to all the walking speeds with a moderate strength (R²>0.3, p < .01) (Table 3). Age was also negatively correlated to the walking speed but with a weak strength (R²<0.3, p < .05) (Table 3). The total score of MMSE was correlated to the walking speeds except with Vcount and Vletter when GHS was significantly correlated with VcountB, Vanimals and Vletter but not with Vsimple nor Vcount. Gender and disease duration were not significantly correlated to the different walking speeds (Table 3). As mentioned before, CR was moderately correlated with the walking speeds in iNPH-P (Table 2) and (Table 3).
To explore which variables could play a major role in explaining the physical performance through single and dual-task walking speeds, multiple linear regression analysis (MLRA) was used. The MLRA for each of the different walking speeds (Vsimple, Vcount, VcountB, Vanimals, Vletter) was built with age, gender, disease duration, educational level (CR), NPH scale, GHS and ARWMC as variables. Each model was significant and explained more than 35% of the variability of the different speeds with the best model for VcountB (F (4.63) = 12.880, p < .001) (Table 4). Results identified CR, NPH scale, and age as the main contributors to all the different walking speeds with an averaged slope in each model of 0.366, -0.302, -0.297 respectively. The positive slope coefficient for CR means that an increase in CR is associated with an increase in walking speed and inversely for NPH scale and age as the slope is negative. GHS appeared to be also a contributor for VcountB, Vanimals and Vletter with a slope coefficient of -0.226, -0.206, and − 0.216 respectively, p < .05 (Table 4).
Discussion
The present study aimed to evaluate the contribution of CR on DT walking in healthy controls (HC) and iNPH patients (iNPH-P). The first hypothesis of this study was partially validated as the simple linear regression highlighted a moderate positive association between CR and the different walking speeds as shown by the standardized coefficient in the linear regression (β > 0.4, p < .001) (Table 2) but only applicable in iNPH-P and not in HC. Then, the multiple linear regression analysis highlighted the role of education, above and beyond all the other considered factors, as the best predictor of dual-task walking speed variability in the specific iNPH population which confirmed the second hypothesis.
First, a moderate positive association between CR and the different walking speeds was shown by the standardized coefficient in the simple linear regression (Table 2). However, these results were applicable only in iNPH-P but not in HC (Table 2). These findings were not in line with previous studies that found significant interaction effects of CR with walking speed under ST (b = 0.09, 95% CI [0.01;0.17], z = 2.30, p = .02) and DT (b = 0.10, 95% CI [0.02;0.17], z = 2.55, p = .01) conditions in normal aging [22]. Many studies also found that single gait speed increases with the highest level of education in normal aging [28, 29]. The non-significant results in HC could be explained by the low repartition of the HC participants in the category 1 of the level of education. Indeed, as Fig. 1 highlighted, there was a large standard deviation in the first category of the level of education, explained by only two HC participants included in this group. Thus, by increasing the number of participants in this category, the correlation between CR and mobility performance (Vsimple, Vcount, VcountB, Vanimals and Vletter) would have been greater and similar to previous studies. However, the present findings reinforce the idea that the level of education contributes to cognitive reserve as a compensatory factor of aging declines [21, 30]. Holtzer et al. [31] found that CR was associated with a lower risk of developing incident mobility impairment (odds ratio (OR) = 0.819, 0.67–0.98, p = .038 (unadjusted)), which illustrates the protective role of CR against age-related declines. Education may increase the predisposition for greater physical and mental stimulation during the entire lifetime which, in turn, may generally contribute to greater CR and, more specifically, to higher flexibility in dual-task contexts, as shown here with a higher walking speed in DT and elsewhere [32, 33]. The protective effect of CR against adverse health outcomes appeared to be greater in the population with the greatest cognitive and functional impairments, thus the iNPH-P (see MMSE score, TUG time, and 10 m-walk test in Table 1). These results are interesting as the recommendation proposed by O’Brien’s study could be all the more interesting in vulnerable populations like iNPH-P [22]. Indeed, O’Brien et al. [22] supported the idea that the moderating role of CR in the relationship between gait velocity and incident mobility impairment highlights the importance of building and maintaining one’s reserve capabilities in order to protect against age-related functional decline. Research has shown that CR can increase throughout the life span in response to enriching social, physical, and cognitive activities [34], suggesting that healthcare providers and those involved in caring for older adults should recommend participation in such activities to support healthy aging. It could be an interesting recommendation in the specific iNPH-P population where the effect of CR on mobility performance seemed to be higher.
Concerning iNPH-P specifically, the multiple linear regression analysis highlighted that the role of CR measured by the level of education was the best predictor with NPH-scale of single and dual-task walking speed above and beyond all the other considered factors (Table 4). This is in line with a study that has shown through an MLRA that education was the best predictor of dual-task cost variability in healthy aging above and beyond all the other considered factors which were age, general cognitive abilities measured with the MOCA score, and secondary task efficiency [33]. Interestingly, the other important variables that explain walking speed in iNPH-P were NPH scale, age and GHS. The NPH scale considered three domains of NPH which are gait impairments, urinary disturbances, and cognitive impairment [24]. As the NPH-scale is closely related to gait performance, its correlation with single and dual-task walking is not so surprising. What is surprising is that, despite the close link of NPH scale with gait, CR was the most correlated with walking speed in each model (Table 4) except in VcountB. Age was the third contributive variable to single and dual-task walking speeds with a negative slope suggesting that single and dual-task walking speeds decrease with aging. Many studies shared these results where single and dual-task walking performances were strongly influenced by age [18]. GHS, which is a global score that considers various aspects of health status such as diabetes, chronic heart failure, arthritis, hypertension, depression, stroke, chronic obstructive pulmonary disease, angina, or myocardial infarction, was also a major contributive variable to VcountB, Vanimals and Vletter with a mean negative slope of -0.216 in all models (Table 4). The negative slope means that slower gait speed is associated with a higher GHS-score and, thus, a higher number of comorbidities. No study has demonstrated the effect of this precise GHS-score on walking performance, but it has already been shown that low gait speed was associated with a higher number of medications (OR = 4.28, 95% CI [1.63, 11.2]), and a higher number of depressive symptoms (OR = 1.31, 95% CI [1.09, 1.58]) [35]. Busch et al. [28] also found that slower gait speed was associated with cardiovascular disease. This is of special importance as cerebrovascular conditions, a major consequence of cardiovascular disease, are often reported in iNPH [36, 37]. Gait and especially dual-task walking requires a high level of cognitive capacities such as sustaining attention and executive function [38]. As patients with comorbidities had poorer performance in executive functions and memory compared to controls [39, 40], it could be hypothesized that this cognitive limitation leads to a decline in walking performance when the cognitive capacity is exceeded during high attention-demanding task in accordance with the capacity limitations hypothesis [41] which could explain the correlation obtained in MLRA. However, with respect to these different clinical variables, CR remained the most contributive variable of the single and dual-task walking conditions.
Limitations
Finally, this study replicated previous findings on the positive contribution of CR on mobility performance usually measured by walking speed. Also, the results of this study highlighted new variables that highly contributed to single and dual-task walking speed such as NPH-scale, age or GHS (Table 4) in a population with an important number of iNPH patients. Noted that radiological measures for iNPH such as DESH or the radscale were not analyzed in this study but it should be interesting to take into account [4]. However, several limitations need to be discussed. As mentioned before, the unequal repartition of the iNPH-P and HC participants through the three categories of the level of education makes the interpretation and the comparison between the two groups difficult. Also, it is important to notice that the level of education was measured continuously in iNPH-P which is the most common way to assess the level of education while, in HC, only the categorical variable was accessible which could influence the correlation results and bring a ceiling effect. Concerning the MLRA, the guideline ratio for a linear regression to detect reasonable-size effects with reasonable power is to have 1 covariate for at least 10 participants [42]. Based on this recommendation, it was expected to have 80 participants as the MLRA included 8 covariates but only 68 participants were included in this study. Thus, the MLRA’s result may not be generalized to other new data as including too many covariates relative to the number of participants can lead to overfitting, where the model fits the noise in the data rather than the underlying patterns. Thus, it could be interesting to test the model on a new set of data to check for replicability and overfitting. In this study, only direct correlations were tested but future studies should explore the moderation between each covariate rather than direct effects. Analyzing moderator effects could offer a greater contrast in gait speed changes across conditions, especially in iNPH population to better characterize the responder to CSF tap test and improve the diagnosis. It is also important to notice that the patients unable to perform the dual task were not include in this study which may limit the representativeness of this specific iNPH population.
Conclusions
In summary, this study found that single and dual-task performance was strongly related to CR in iNPH-P but not in HC. Indeed, the relation between CR measured with the level of education and different walking speeds (Vsimple, Vcount, VcountB, Vanimals, Vletter) seemed to be different between the two groups. CR was also more closely related to single and dual-task walking speeds than other clinical variables such as age, gender, NPH scale, MMSE score, disease duration, and comorbidity burden measured with the GHS and ARWMC in the specific iNPH-P population. As CR could be improved through the life cycle [34], these results support the idea of developing and supporting physical activity programs or other activities that will enrich social, physical and cognitive resources in order to protect against age-related functional decline, especially in the specific iNPH-P population.
Data availability
No datasets were generated or analysed during the current study.
References
Relkin N, Marmarou A, Klinge P, Bergsneider M, McL Black P (2005) Diagnosing idiopathic normal-pressure hydrocephalus. Neurosurgery 57:S24–S216
Jeppsson A, Wikkelsö C, Blennow K et al (2019) CSF biomarkers distinguish idiopathic normal pressure hydrocephalus from its mimics. J Neurol Neurosurg Psychiatry ; 1117–1123
Magdalinou NK, Ling H, Smith JDS, Schott JM, Watkins LD, Lees AJ (2013) Normal pressure hydrocephalus or progressive supranuclear palsy? A clinicopathological case series. J Neurol 260:1009–1013
Nakajima M, Yamada S, Miyajima M et al (2021) Guidelines for management of idiopathic normal pressure hydrocephalus (third edition): endorsed by the Japanese society of normal pressure hydrocephalus. Neurol Med Chir (Tokyo) 61:63–97
Andersson J, Rosell M, Kockum K, Lilja-Lund O, Söderström L, Laurell K (2019) Prevalence of idiopathic normal pressure hydrocephalus: a prospective, population based study. PLoS ONE 14:1–11
Sundström N, Malm J, Laurell K et al (2017) Incidence and outcome of surgery for adult hydrocephalus patients in Sweden. Br J Neurosurg Br J Neurosurg 31:21–27
Allali G, Laidet M, Armand S et al (2017) A combined cognitive and gait quantification to identify normal pressure hydrocephalus from its mimics: the Geneva’s protocol. Clin Neurol Neurosurg 160:5–11
Allali G, Laidet M, Beauchet O, Hermann FR, Assal F, Armand S (2013) Dual-task related gait changes after CSF tapping: a new way to identify idiopathic normal pressure hydrocephalus. J Neuroeng Rehabil 10:117
Abernethy (1988) Dual-task methodology and motor skills research: some applications and methodological constraints. J Hum Mov Stud 14(3): 101–132. J Hum Mov Stud. ; 14: 101–132
Yogev-Seligmann G, Rotem-Galili Y, Dickstein R, Giladi N, Hausdorff JM (2012) Effects of explicit prioritization on dual task walking in patients with Parkinson’s disease. Gait Posture 35:641–646
Ehsani H, Mohler MJ, O’connor K, Zamrini E, Tirambulo C, Toosizadeh N (2019) The association between cognition and dual-tasking among older adults: the effect of motor function type and cognition task difficulty. Clin Interv Aging 14:659–669
Bahureksa L, Najafi B, Saleh A et al (2016) The impact of mild cognitive impairment on gait and balance: a systematic review and meta-analysis of studies using instrumented assessment. Gerontology 63:67–83
Martínez-Ramírez A, Martinikorena I, Lecumberri P et al (2016) Dual task gait performance in frail individuals with and without mild cognitive impairment. Dement Geriatr Cogn Disord 42:7–16
Wollesen B, Mattes K, Rönnfeldt J (2017) Influence of age, gender and test conditions on the reproducibility of dual-task walking performance. Aging Clin Exp Res 29:761–769
Bayot M, Dujardin K, Dissaux L et al (2020) Can dual-task paradigms predict falls better than single task? – a systematic literature review. Neurophysiol Clin
Giusti Rossi P, Pires De Andrade L, Hotta Ansai J et al (2019) Dual-task performance: influence of frailty, level of physical activity, and cognition. J Geriatr Phys Ther 42:E142–E147
Cadore EL, Casas-Herrero A, Zambom-Ferraresi F et al (2015) Do frailty and cognitive impairment affect dual-task cost during walking in the oldest old institutionalized patients? Age (Omaha) 37:1–9
Piche E, Chorin F, Gerus P, Jaafar A, Guerin O, Zory R (2022) Effects of age, sex, frailty and falls on cognitive and motor performance during dual-task walking in older adults. Exp Gerontol 171:112022
Campos-Magdaleno M, Pereiro A, Navarro-Pardo E, Juncos-Rabadán O, Facal D (2021) Dual-task performance in old adults: cognitive, functional, psychosocial and socio-demographic variables. Aging Clin Exp Res
Stern Y (2009) Cogn Reserve Neuropsychologia 47:2015–2028
Stern Y (2002) What is cognitive reserve ? Theory and research application of the reserve concept. ; 448–460
O’Brien C, Holtzer R (2021) Cognitive reserve moderates associations between walking performance under single- and dual-task conditions and incident mobility impairment in older adults. Journals Gerontol - Ser Biol Sci Med Sci 76:E314–E320
Gallia GL, Rigamonti D, Williams MA (2006) The diagnosis and treatment of idiopathic normal pressure hydrocephalus. Nat Clin Prat Neurol 2:375–381
Kubo Y, Kazui H, Yoshida T et al (2007) Validation of grading scale for evaluating symptoms of idiopathic normal-pressure hydrocephalus. Dement Geriatr Cogn Disord 25:37–45
Stern Y (2012) Cognitive reserve in ageing and Alzheimer’s disease. Lancet 11:1006–1012
Wahlund LO, Barkhof F, Fazekas F et al (2001) A new rating scale for age-related white matter changes applicable to MRI and CT. Stroke 32:1318–1322
Mahoney JR, Verghese J, Holtzer R, Allali G (2014) The evolution of mild parkinsonian signs in aging. J Neurol 261:1922–1928
Busch TDA, Duarte YA, Pires Nunes D et al (2015) Factors associated with lower gait speed among the elderly living in a developing country: a cross-sectional population-based study. BMC Geriatr 15:1–9
Gale CR, Allerhand M, Sayer AA, Cooper C, Deary IJ (2014) The dynamic relationship between cognitive function and walking speed: the English Longitudinal Study of Ageing. Age (Omaha) ; 36
Scarmeas N, Stern Y (2010) Cognitive reserve and lifestyle. J Clin Exp Neuropsychol 25:625–633
Holtzer R, Ross D, O’brien C, Izzetoglu M, Wagshul ME (2022) Cognitive reserve moderates the efficiency of prefrontal cortex activation patterns of gait in older adults. Journals Gerontol - Ser Biol Sci Med Sci 77:1836–1844
Puccioni O, Vallesi A (2012) Conflict resolution and adaptation in normal aging: the role of verbal intelligence and cognitive reserve. Psychol Aging 27:1018–1026
Vallesi A (2016) Dual-task costs in aging are predicted by formal education. Aging Clin Exp Res 28:959–964
Najar J, Östling S, Gudmundsson P et al (2019) Cognitive and physical activity and dementia: a 44-year longitudinal population study of women. Neurology 92:E1322–E1330
Kyrdalen IL, Thingstad P, Sandvik L, Ormstad H (2019) Associations between gait speed and well-known fall risk factors among community-dwelling older adults. Physiother Res Int 24:1–6
Eklund SA, Israelsson H, Carlberg B, Malm J (2022) Vascular risk profiles for predicting outcome and long-term mortality in patients with idiopathic normal pressure hydrocephalus: comparison of clinical decision support tools. J Neurosurg 138:476–482
Israelsson H, Carlberg B, Wikkelsö C et al (2015) Cardiovascular risk factors are associated with idiopathic normal pressure Hydrocephalus. Fluids Barriers CNS 12:O41
Yogev-Seligmann G, Hausdorff JM, Giladi N (2008) The role of executive function and attention in gait. Mov Disord 23:329–342
Lugtenburg A, Voshaar RCO, Zelst W, Van, Schoevers RA, Enriquez-Geppert S, Zuidersma M (2017) The relationship between depression and executive function and the impact of vascular disease burden in younger and older adults. Age Ageing 46:697–701
Sadanand S, Balachandar R, Bharath S (2016) Memory and executive functions in persons with type 2 diabetes: a meta-analysis. Diabetes Metab Res Rev 32:132–142
Reuter-Lorenz PA, Jonides J, Smith EE et al (2000) Age differences in the frontal lateralization of verbal and spatial working memory revealed by PET. J Cogn Neurosci 12:174–187
Harrell FE (2001) Regression modeling strategies: with applications to linear models, logistic regression, and survival analysis. Springer US
Acknowledgements
Not applicable.
Funding
This study was supported by the Swiss National Science Foundation (SNSF grant #320030_173153) and Geneva University Hospitals (PRD grant #8-2019-II).
Open access funding provided by University of Geneva
Author information
Authors and Affiliations
Contributions
EP analyzed and interpreted the data of this study. All authors were major contributors in writing the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study protocol was approved by the Institutional Review Board of the Geneva University Hospital (Protocol 09-160R). All subjects gave informed consent according to the ethical standards set forth in the declaration of Helsinki (1983).
Consent for publication
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Piche, E., Armand, S., Allali, G. et al. The contribution of cognitive reserve in explaining the dual-task walking performance in iNPH patients: comparison with other cognitive, functional, and socio-demographic variables. Aging Clin Exp Res 36, 190 (2024). https://doi.org/10.1007/s40520-024-02829-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s40520-024-02829-0