
Abstract
Background
Progression of cerebral small vessel disease (cSVD) markers has been studied in different races/ethnic groups. However, information from individuals of Amerindian ancestry is lacking. We sought to evaluate progression patterns of cSVD markers in community-dwelling older adults of Amerindian ancestry.
Methods
Following a longitudinal prospective study design, participants of the Atahualpa Project Cohort aged ≥ 60 years received a baseline brain MRI and clinical interviews. Those who also received a brain MRI at the end of the study were included. Poisson regression models were fitted to assess cSVD markers progression according to their baseline load after a median follow-up of 6.5 ± 1.4 years. Logistic regression models were fitted to assess interrelations in the progression of the different cSVD markers at the end of the study.
Results
The study included 263 individuals (mean age: 65.7 ± 6.2 years). Progression of white matter hyperintensities (WMH) was noticed in 103 (39%) subjects, cerebral microbleeds in 25 (12%), lacunes in 12 (5%), and enlarged basal ganglia-perivascular spaces (BG-PVS) in 56 (21%). Bivariate Poisson regression models showed significant associations between WMH severity at baseline and progression of WMH and enlarged BG-PVS. These associations became non-significant in multivariate models adjusted for clinical covariates. Logistic regression models showed interrelated progressions of WMH, cerebral microbleeds and enlarged BG-PVS. The progression of lacunes was independent.
Conclusions
Patterns of cSVD marker progression in this population of Amerindians are different than those reported in other races/ethnic groups. The independent progression of lacunes suggests different pathogenic mechanisms with other cSVD markers.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Frequency and progression patterns of sporadic cerebral small vessel disease (cSVD) have extensively been studied in White and Asian populations, and to a lesser degree in Blacks [1,2,3,4,5,6,7,8,9,10,11,12]. However, information from persons of Amerindian ancestry is lacking. The World Bank estimates that 42 million indigenous people (Amerindians) live in Latin America, accounting for about 8% of the region’s population [13]. Many of these individuals are settled in rural areas, and about 40% of them live in poverty with limited access to technology needed to diagnose cSVD. Moreover, cSVD is often unrecognized in these settings because many affected individuals remain asymptomatic for years and restricted healthcare resources preclude early recognition of neuroimaging markers that preceded the onset of subsequent clinical consequences such as overt strokes and vascular dementia.
During the past decade, a population of older adults of Amerindian ancestry living in rural Ecuador has comprehensively been investigated to assess the prevalence and correlates of the different cSVD markers in this ethnic group. Overall, these studies have documented a high frequency of cSVD markers in this population [14,15,16,17], as well as a significant association between non-traditional risk factors—high social risk, sympathetic overactivity—and progression of white matter hyperintensities (WMH) of presumed vascular origin (a reliable marker of cSVD) [18, 19]. However, little is known on whether the different cSVD markers in Amerindians progress independently or interrelated or if this progression is different than that reported in other races/ethnic groups. This knowledge can provide clues on mechanisms involved in their pathogenesis.
Seizing on this population-based prospective cohort, the present study aims to assess patterns and interrelations of the progression of the different cSVD markers as well as their relationships with demographics, level of education, and traditional cardiovascular risk factors.
Methods
Study population
Atahualpa is a rural village located in coastal Ecuador. As previously detailed, the population is homogeneous regarding race/ethnicity, levels of education, socio-economic status, and dietary habits [14,15,16,17]. Phenotypic characteristics of the population provide support for their Amerindian ancestry. These include olive-moderate brown skin (Type IV in the Fitzpatrick scale), dark brown eyes and hair, short stature, and a predominantly elliptic hard palate [20].
Study design
Following a longitudinal prospective study design, Atahualpa residents aged ≥ 60 years were identified by means of door-to-door surveys, and those who had a baseline brain MRI between 2012 and 2019, and were actively participating in the Atahualpa Project Cohort as of May 2021, were invited to receive a follow-up brain MRI. Characteristics of individuals who did not receive MRIs were compared to those who completed the study. The study followed the STROBE checklist (The Strengthening the Reporting of Observational Studies in Epidemiology) [21]. We explored the pattern of progression of the different cSVD markers after taking into account the relevance of covariates of interest. Participants were followed starting at baseline MRI. The study design contemplated follow-up MRIs with sufficient exposure time that allowed enough statistical power to detect the hypothesized difference. The achieved sample of this prospective study has adequate power to detect planned differences.
Neuroimaging protocol
Both baseline and follow-up MRIs were performed with the same equipment (Philips Intera 1.5 T; Philips Medical Systems, Eindhoven, the Netherlands), following protocols that represented standards for research on cSVD at the time of baseline MRIs [22]. Imaging studies included two-dimensional multi-slice turbo spin-echo T1-weighted (TR 594, TE 15), fluid-attenuated inversion recovery (FLAIR) (TR 9000, TE 120, TI 2500), T2-weighted (TR 4500, TE 100), and T2*-weighted gradient-recalled echo (TR 686, TE 23) sequences in the axial plane, as well as a FLAIR sequence in the sagittal plane. The pre-established brain imaging package delivered by the manufacturer was used to standardize applicability by technicians.
MRI readings focused on WMH of presumed vascular origin, cerebral microbleeds (CMB), lacunes of presumed vascular origin, and enlarged basal ganglia-perivascular spaces (BG-PVS).22 WMH were defined as lesions appearing hyperintense on the T2-weighted sequence that remained bright on FLAIR (without cavitation). These lesions were graded according to the modified Fazekas scale, which recognizes three degrees of severity of WMH: mild, moderate and severe [23]. Mild WMH refers to the imaging of periventricular caps or thin lesions and punctate hyperintensities in the subcortical white matter. Moderate WMH is characterized by a smooth periventricular halo and subcortical foci begin to merge. In severe WMH, there is extension of periventricular lesions into the subcortical white matter and large confluent subcortical foci are observed. CMB were identified and rated according to the microbleed anatomical rating scale; only definite CMB were included (well-defined, small, rounded or circular, hypointense lesions located in deep cerebral structures) [24]. Lacunes of presumed vascular origin were defined as fluid-filled cavities measuring > 3 mm but < 20 mm located in the territory of a perforating arteriole [25]. Enlarged BG-PVS were defined as small (< 3 mm) structures of CSF intensity that followed the orientation of perforating arteries [26]. Enlarged BG-PVS were assessed in the single slice with the highest number of these structures on one side, and were rated according to a widely used quantitative scale [27]. Consequently, from 1 to 10 enlarged BG-PVS generated a score of 1, 11–20 a score of 2, 21–40 a score of 3, and > 40 a score of 4.
WMH progression was defined as the increase in at least one grade in the Fazekas scale in the follow-up MRI. CMB and lacunes progression were defined as the appearance of new CMB or lacunes in the follow-up, respectively (either in subjects who were free of these lesions at baseline or in those who developed additional lesions). Enlarged BG-PVS progression was defined as the increase in one grade in the enlarged BG-PVS scale (Fig. 1).

Neuroimaging markers of cerebral small vessel disease. Panel A progression of white matter hyperintensities of presumed vascular origin (fluid-attenuated inversion recovery); Panel B presence of a new lacune of presumed vascular origin in the left basal ganglia (T1-weighted); Panel C progression of enlarged basal-ganglia perivascular spaces in the right basal ganglia (T2-weighted); and Panel D appearance of new cerebral microbleeds (T2*-weighted gradient-recalled echo)
Both, baseline and follow-up MRIs were independently read by one neuroradiologist and one neurologist blinded to clinical information. Kappa coefficients for interrater agreement for the different cSVD markers at baseline and follow-up were 0.91 and 0.93 for WMH, 0.82 and 0.80 for CMB, 0.88 and 0.92 for lacunes, and 0.84 and 0.78 for enlarged BG-PVS. Discrepancies were resolved by consensus.
Covariate investigated
Demographics, level of education, and cardiovascular health metrics proposed by the American Heart Association were assessed at the time of baseline MRI and were selected as potential confounders. Cardiovascular health metrics in the poor range were assigned to current smokers, to individuals with a body mass index ≥ 30 kg/m2, and to those with no moderate or vigorous activity, ≤ 1 component of the American Heart Association’s healthy diet, blood pressure ≥ 140/90 mmHg, fasting glucose ≥ 126 mg/dL, and total cholesterol blood levels ≥ 240 mg/dL [28]. Less than 15% of the population with vascular risk factors received proper therapy during the study years.
Statistical analysis
Data analysis was carried out by the use of STATA version 17 (College Station, TX, USA). Univariate comparisons for either continuous or categorical variables utilized linear models, except when non-parametric models were warranted. To calculate person-years of follow-up, we considered the time from baseline to follow-up MRIs. Poisson regression models were fitted to estimate the rate of progression of cSVD markers after taking into account cSVD markers load at baseline as well as clinical covariates, and the time between both MRIs. We used the goodness of fit chi-squared test for Poisson regression, which corroborated the fit of Poisson models to the data. Logistic regression models were fitted to estimate interrelations in the progression of the different cSVD markers. Smoking was not included in any model due to collinearity with other predictors.
Results
Recruitment process
A total of 478 individuals aged ≥ 60 were enrolled in the Atahualpa Project Cohort between 2012 and 2019. Of them, 403 (84%) received a baseline MRI of the brain and clinical interviews. Among the 75 non-eligible individuals, 36 died or emigrated before the MRI, 19 declined consent, 17 were severely disabled or had contraindications for MRI, and three had missing clinical information. Of 403 subjects that started the study, 263 (65%) had a follow-up MRI and were included in final analyses. Ninety of the 140 excluded study participants died, and the remaining 50 either declined further consent, became disabled, or emigrated between baseline and follow-up MRI. Follow-up time between baseline and follow-up brain MRIs was 1711 person-years (95% CI 1665–1757 years), and the mean follow-up was 6.5 ± 1.4 years (range 2.2–9.1 years).
Baseline characteristics of study participants
The mean (± SD) age of 263 participants at the time of baseline MRI was 65.7 ± 6.2 years (median age: 63.9 years; age range: 60–91 years), 149 (57%) were women, and 192 (73%) had primary school education only. Individual cardiovascular health metrics in the poor range included: smoking status: 11 (4%), body mass index: 63 (24%), physical activity: 12 (5%), diet: 11 (4%), blood pressure: 104 (40%), fasting glucose: 72 (27%), and total cholesterol blood levels: 41 (16%). On baseline MRI, 131 individuals (50%) had mild, 33 (13%) had moderate, and nine (3%) had severe WMH (the remaining 90 [34%] did not have WMH). CMB were present in 22 (8%) and lacunes in 21 (8%) subjects. Abnormally enlarged BG-PVS were documented in 56 (21%) individuals (46 had grade 2 and 10 had grades 3–4); the remaining 207 participants had grade 1 enlarged BG-PVS, which is considered normal.
Differences across included and non-included individuals
As mentioned, 75 individuals were excluded for not receiving a baseline MRI and 140 did not receive a follow-up MRI (n = 215). Table 1 shows differences across excluded and included individuals, which were expected since most of the former died or became disabled during the follow-up. For the subset of 140 individuals who had a baseline—but not a follow-up—MRI, all cSVD markers were significantly more frequent when compared to the analyzed population.
cSVD markers at follow-up
At follow-up, 112 (43%) individuals had mild, 67 (25%) had moderate, and 32 (12%) had severe WMH (the remaining 52 subjects [20%] did not have WMH). A total of 103 (39%) individuals had MRI evidence of WMH progression. Progression from none-to-mild WMH was observed in 33 cases, from none-to-moderate in five, from mild-to-moderate in 42, from mild-to-severe in 10, and from moderate-to-severe in 13. Also at follow-up MRI, 47 (18%) individuals had CMB and 33 (13%) had lacunes. CMB progression was noticed in 25 (10%) individuals, and lacunes progression in 12 (5%). Abnormally enlarged BG-PVS were recognized in 99 (38%) individuals (77 had grade 2 and 22 had grades 3–4). The remaining 164 individuals (62%) had enlarged BG-PVS grade 1 (normal). Overall, 56 (21%) individuals had evidence of enlarged BG-PVS progression. Progression from grade 1 to 2 was observed in 41 cases, from grade 2 to grades 3–4 in 14, and from grade 1 to grades 3–4 in one.
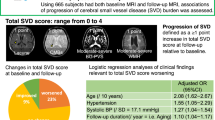
Unadjusted analyses showed differences across individuals who had cSVD markers progression compared to those who did not (Table 2). Individuals with WMH progression were older and less often obese than their counterparts without progression. Individuals with enlarged BG-PVS progression were older and more often hypertensive than those who did not have progression of this marker. WMH progression was interrelated with CMB and enlarged BG-PVS progression. Lacunes progressed independently of all other markers of cSVD, and CMB and enlarged BG-PVS also progressed independently of each other.
cSVD marker severity at baseline and progression
To assess associations between cSVD markers basal loads and their progressions, we fitted separate Poisson regression models using cSVD markers progression as dependent variables. Unadjusted models showed significant associations between WMH basal load and progression (IRR: 1.38; 95% CI 1.19–1.59) and between enlarged BG-PVS basal load and progression (IRR: 1.50; 95% CI 1.11–2.04). However, these associations became non-significant when clinical covariates were taken into account (Table 3). CMB and lacunes basal loads were collinear with CMB and lacunes progression, respectively. Likewise, CMB progression and poor diet, as well as lacunes progression and poor physical activity, were collinear. Age at baseline was the single covariate remaining significant in the model assessing WMH progression. Otherwise, no covariates remained independently significant in these multivariate models.
Interrelations between cSVD marker progression
Using progression of the different cSVD markers as dependent variables, we fitted logistic regression models to assess interrelations in the progression of these markers. Parsimonious models, adjusted for demographics and removing covariates near to p = 1 in fully adjusted models, showed interrelated progression of WMH with CMB (OR: 2.76; 95% CI 1.07–7.11) and with enlarged BG-PVS (OR: 4.37; 95% CI 2.16–8.83). Lacunes progressed independently to the progression of the other cSVD markers (Table 4).
Discussion
This longitudinal prospective population-based cohort, conducted in community-dwelling older adults of Amerindian ancestry, shows that the progression of cSVD markers differs from that reported in other races/ethnic groups. WMH, CMB, and enlarged BG-PVS progressions remain interrelated after relevant clinical covariates are taken into account. Lacunes progress independently of the other cSVD markers.
There are no previous reports on the interrelated progression of cSVD markers in Amerindians. However, important pieces of evidence may be gathered from studies conducted in other races/ethnic groups. A longitudinal study conducted in Singapore (346 individuals attending a memory clinic, followed for about 2 years) revealed that arterial hypertension was associated with WMH progression, and age with CMB progression. In the Singapore study, the most important factor for cSVD markers progression was cSVD load at baseline [5]. In the Shanghai Aging Study, WMH severity at baseline predicted progression of all markers of cSVD. However, progression was heterogeneous and interrelations of progression among the different cSVD markers were not estimated [7].
The Rotterdam Scan Study, a population-based cohort that included a White population, followed 668 individuals for three years [29]. This study used WMH and lacunes as cSVD markers of interest, and found that WMH basal load, increasing age, being women, arterial hypertension, smoking, and having lacunes at baseline were associated with increased WMH progression. In the Rotterdam Scan Study, WMH progression was tightly associated with lacunes progression, suggesting a shared pathogenic mechanism. Interrelated progression of WMH and lacunes has also been reported in other studies among White populations [30, 31]. In the Atherosclerosis Risk in Communities Study, including Black and White participants, 901 stroke-free individuals had a follow-up brain MRI about 10 years after baseline [6]. The study only considered progression of WMH and lacunes. It was found that both markers progressed together and this progression was associated with an increased incidence of stroke. Data from the Swedish National Study on Aging and Care in Kungsholmen (325 individuals followed for almost six years) also showed that baseline loads of WMH, lacunes and enlarged BG-PVS predicted interrelated progression of these cSVD markers [8]. In contrast, we did not find such associations, suggesting that—at least in Amerindians—lacunes might be associated to pathogenic mechanisms independent of cSVD such as intracranial atherosclerotic disease or embolism. However, comparisons must be interpreted with caution since not all studies take into account the four cSVD markers used in the present study and protocols used for assessing progression (particularly WMH progression) are heterogeneous. Moreover, some studies are restricted to patients with stroke or attending a memory clinic, and may not be representative of the population at large.
In the present study of Amerindians, the progression of lacunes occurred independently of WMH, CMB, and BG-PVS progression, suggesting that the former may not be exclusively related to cSVD. In this view, we have recently reported that lacunes of presumed vascular origin are more frequently associated with intracranial atherosclerotic disease than with cSVD and that only one-fourth of the effect of intracranial atherosclerosis on lacunes was mediated by WMH [32].
The present study has some limitations. Inasmuch as the identification of individuals by means of door-to-door surveys supposes a lack of selection bias, non-included individuals were older, had more cardiovascular risk factors, and a more severe cSVD burden than those who were included. However, the same differences have been reported in other studies that attempted to differentiate non-included and included individuals [5]. In the present study, differences across excluded and included individuals were likely related to the SARS-CoV-2 pandemic, since old individuals (particularly those who had COVID-19 and remained with respiratory sequelae) did not accept the practice of follow-up MRIs. This was reflected in the rate of declined consent, which increased substantially from the first (baseline) to the second (follow-up) invitation. Another factor that limited the number of individuals included this study was the high mortality rate related to COVID-19 in the village [33], and the fear of older adults to remain in a village with poor sanitary resources, which are evidenced by the excess numbers of deaths and emigration from 2020 to 2021, compared to those occurring from 2012 to 2019. The modified Fazekas scale may be less reliable than volumetry to assess slight changes in WMH severity in the follow-up [34], and this may be perceived as another limitation of this study. It is also possible that some unmeasured confounders may be responsible for at least part of the findings of the present study. Indeed, recent studies showed the importance of non-traditional risk factors (sympathetic overactivity, high social risk) in the progression of WMH in the study population [18, 19]. In addition, the fact that less than 15% of the population with vascular risk factors received proper therapy during the study years precluded assessment of the impact of medications on cSVD markers progression, as has been demonstrated in other studies [35]. The good side of this is that we had the opportunity to assess cSVD progression in a virtually untreated population, which gave us more clear estimates of the natural history of cSVD marker progression.
Despite these limitations, the study has several strengths that include its population-based design, the racial homogeneity of the study population, the systematic assessment of cardiovascular risk factors and cSVD markers by means of uniform and standardized protocols, and the practice of baseline and follow-up MRIs using the same equipment and procedures.
In conclusion, this is the first study showing patterns of cSVD markers progression in Amerindians, which differed with those reported in other races/ethnic groups, mostly by the little contributory role of cardiovascular risk factors on cSVD progression and the fact that lacunes progressed independently to the other cSVD markers. This knowledge may open new avenues of research for comparison of cSVD progression patterns across different races/ethnic groups. This, in turn, will allow a better understanding of the natural history of cSVD markers in these vulnerable populations. Exploring their possible different pathogenic mechanisms, may help implement policies and cost-effective intervention strategies to reduce consequences of covert cSVD.
Data availability
Aggregated data from this study are available from the corresponding author upon written request.
References
Schmidt R, Berghold A, Joniken H et al (2012) White matter lesion progression in LADIS: frequency, clinical effects, and sample size calculations. Stroke 43:2643–2647
Ding J, Sigurosson S, Jónsson PV et al (2017) Large perivascular spaces visible on magnetic resonance imaging, cerebral small vessel disease progression, and risk of dementia: the age, gene/environment susceptibility–Reykjavik Study. JAMA Neurol 74:1105–1112
Uiterwijk R, Staals J, Huijts M et al (2018) Framingham stroke risk profile is related to cerebral small vessel disease progression and lower cognitive performance in patients with hypertension. J Clin Hypertens (Greenwich) 20:240–245
Sarfo FS, Ovbiagele B, Gebregziabher M et al (2018) Stroke among young West Africans: evidence from the SIREN (stroke investigative research and educational network) large multisite case-control study. Stroke 49:1116–1122
Gyanwali B, Shaik MA, Tan BY et al (2019) Risk factors for and clinical relevance of incident and progression of cerebral small vessel disease markers in an Asian memory clinical population. J Alzheimers Dis 67:1209–1219
Koton S, Schneider ALC, Windham BG et al (2020) Microvascular brain disease progression and risk of stroke: the ARIC study. Stroke 51:3264–3270
Xia Y, Shen Y, Wang Y et al (2020) White matter hyperintensities associated with progression of cerebral small vessel disease: a 7-year Chinese urban community study. Aging (Albany NY) 10:8506–8522
Li Y, Kalpouzos G, Laukka EJ et al (2022) Progression of neuroimaging markers of cerebral small vessel disease in older adults: a 6-year follow-up study. Neurobiol Aging 112:204–211
Cai M, Jacob MA, van Loenen MR et al (2022) Determinants and temporal dynamics of cerebral small vessel disease: 14-year follow-up. Stroke. https://doi.org/10.1161/STROKEAHA.121.038099
Sudre CH, Smith L, Atkinson D et al (2018) Cardiovascular risk factors and white matter hyperintensities: difference in susceptibility in South Asians compared with Europeans. J Am Heart Assoc 7:e010533
Mok V, Srikanth V, Xiong Y et al (2014) Race-ethnicity and cerebral small vessel disease – comparison between Chinese and White populations. Int J Stroke 9:36–42
Della-Monte D, Dong C, Markert MS et al (2018) Carotid intima-media thickness is associated with white matter hyperintensities: the Northern Manhattan study. Stroke 49:304–311
Banco Mundial (2015) Latinoamérica Indígena en el Siglo XXI. Washington, D.C.: Banco Mundial. https://documents1.worldbank.org/curated/en/541651467999959129/pdf/Latinoam%C3%A9rica-ind%C3%ADgena-en-el-siglo-XXI-primera-d%C3%A9cada.pdf
Del Brutto OH, Mera RM, Del Brutto VJ et al (2015) White matter hyperintensities of presumed vascular origin: a population-based study in rural Ecuador (The Atahualpa Project). Int J Stroke 10:372–375
Del Brutto VJ, Zambrano M, Mera RM et al (2015) Population-based study of cerebral microbleeds in stroke-free older adults living in rural Ecuador: the Atahualpa project. Stroke 46:1984–1986
Del Brutto VJ, Ortiz JG, Brutto OH et al (2018) Total cerebral small vessel disease score and cognitive performance in community-dwelling older adults: results from the Atahualpa project. Int J Geriatr Psychiatry 33:325–331
Del Brutto OH, Mera RM, Recalde BY et al (2020) Cerebral small vessel disease in community-dwelling older adults living in remote rural settings. J Neurol Sci 416:117016
Del Brutto OH, Mera RM, Recalde BY et al (2022) High social risk influence progression of white matter hyperintensities of presumed vascular origin: a prospective study in community-dwelling older adults. Stroke. https://doi.org/10.1161/STROKEAHA.122.038561
Del Brutto OH, Mera RM, Costa AF et al (2022) Decreased nighttime heart rate variability and progression of white matter hyperintensities of presumed vascular origin. A prospective study in community-dwelling older adults. J Stroke Cerebrovasc Dis 31:106479
Castillo PR, Mera RM, Zambrano M et al (2014) Population-based study of facial morphology and excessive daytime somnolence. Pathophysiology 21:289–292
von Elm E, Altman DG, Egger M et al (2007) The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet 370:1453–1457
Wardlaw JM, Smith EE, Biessels GJ et al (2013) Neuroimaging standards for research into small vessel disease and its contribution to ageing and neurodegeneration. Lancet Neurol 12:822–838
Pantoni L, Basile AM, Pracucci G et al (2005) Impact of age-related cerebral white matter changes on the transition to disability: the LADIS study: rationale, design and methodology. Neuroepidemiology 24:51–62
Gregoire SM, Chaudhary UJ, Brown MM et al (2009) The microbleed anatomical rating scale (MARS): reliability of a tool to map brain microbleeds. Neurology 73:1759–1766
Staals J, Makin SD, Doubal FN et al (2014) Stroke subtype, vascular risk factors, and total MRI brain small-vessel disease burden. Neurology 83:1228–1234
Doubal FN, MacLullich AM, Ferguson KJ et al (2010) Enlarged perivascular spaces on MRI are a feature of cerebral small vessel disease. Stroke 41:450–454
Potter GM, Chappell FM, Morris Z et al (2015) Cerebral perivascular spaces visible on magnetic resonance imaging: development of a qualitative rating scale and its observer reliability. Cerebrovasc Dis 39:224–231
Lloyd-Jones D, Hong Y, Labarthe D et al (2010) American heart association strategic planning task force and statistics committee. Defining and setting national goals for cardiovascular health promotion. The American heart association’s strategic impact goal through 2020 and beyond. Circulation 121:586–613
van Dijk EJ, Prins ND, Vrooman HA et al (2008) Progression of cerebral small vessel disease in relation to risk factors and cognitive consequences: Rotterdam Scan Study. Stroke 39:2712–2719
Schmidt R, Fazekas F, Kapeller P et al (1999) MRI white matter hyperintensities: three-year follow-up of the Austrian stroke prevention study. Neurology 53:132–139
Longstreth WT Jr, Arnold AM, Beauchamp NJ Jr et al (2005) Incidence, manifestations, and predictors of worsening white matter on serial cranial magnetic resonance imaging in the elderly: the cardiovascular health study. Stroke 36:56–61
Del Brutto OH, Mera RM (2022) Neuroimaging investigation of the intracranial vasculature is warranted in older adults with lacunes of presumed vascular origin. Neuroradiol J. https://doi.org/10.1177/19714009221083147
Del Brutto OH, Costa AF, Mera RM et al (2020) SARS-CoV-2-related mortality in a rural Latin American population. Int J Infect Dis 99:226–228
van Leijsen AMC, van Uden IWM, Ghafoorian M et al (2017) Nonlinear temporal dynamics of cerebral small vessel disease: the RUN DMC study. Neurology 89:1569–1577
Guo Y, Li Y, Liu X et al (2020) Assessing the effectiveness of statin therapy for alleviating cerebral small vessel disease progression in people ≥75 years of age. BMC Geriatr 20:292
Funding
Study supported by Universidad Espíritu Santo–Ecuador. The sponsor had no role in the design of the study, nor in data collection or analyses, or in the decision to submit this work for publication.
Author information
Authors and Affiliations
Contributions
OHB: study design, imaging readings, and manuscript drafting; RMM: statistical analysis of data; AFC: data collection and interpretation; DAR: data collection and interpretation; BYR: study coordinator; VJB: imaging readings and significant intellectual contribution to manuscript content. All authors read and approved the final version of the submitted manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The Ethics Committee of Hospital-Clínica Kennedy, Guayaquil, Ecuador (FWA 00030727) approved the study.
Informed consent
Study participants signed comprehensive informed consents at enrollment, as well as before the practice of follow-up MRIs.
Statement of human and animal rights
All human studies have been approved by the appropriate ethics committee and have therefore been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Del Brutto, O.H., Mera, R.M., Costa, A.F. et al. Patterns of progression of cerebral small vessel disease markers in older adults of Amerindian ancestry: a population-based, longitudinal prospective cohort study. Aging Clin Exp Res 34, 2751–2759 (2022). https://doi.org/10.1007/s40520-022-02223-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40520-022-02223-8