
Abstract
Purpose
Medical students have a higher risk of developing psychological issues, such as feeding and eating disorders (FEDs). In the past few years, a major increase was observed in the number of studies on the topic. The goal of this review was to estimate the prevalence risk of FEDs and its associated risk factors in medical students.
Methods
Nine electronic databases were used to conduct an electronic search from the inception of the databases until 15th September 2021. The DerSimonian–Laird technique was used to pool the estimates using random-effects meta-analysis. The prevalence of FEDs risk in medical students was the major outcome of interest. Data were analyzed globally, by country, by research measure and by culture. Sex, age, and body mass index were examined as potential confounders using meta-regression analysis.
Results
A random-effects meta-analysis evaluating the prevalence of FEDs in medical students (K = 35, N = 21,383) generated a pooled prevalence rate of 17.35% (95% CI 14.15–21.10%), heterogeneity [Q = 1528 (34), P = 0.001], τ2 = 0.51 (95% CI 0.36–1.05), τ = 0.71 (95% CI 0.59–1.02), I2 = 97.8%; H = 6.70 (95% CI 6.19–7.26). Age and sex were not significant predictors. Body mass index, culture and used research tool were significant confounders.
Conclusion
The prevalence of FEDs symptoms in medical students was estimated to be 17.35%. Future prospective studies are urgently needed to construct prevention and treatment programs to provide better outcomes for students at risk of or suffering from FEDs.
Level of evidence
Level I, systematic review and meta-analysis.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The Diagnostic and Statistical Manual of Mental Disorders, 5th Edition defined Feeding and Eating Disorders (FEDs) as enduring disruption of eating or eating-related behavior that results in altered food consumption or absorption and substantially affects physical or psychosocial functioning [1]. Diagnostic criteria are provided for pica, rumination disorder, avoidant/restrictive food intake disorder, anorexia nervosa, bulimia nervosa, and binge-eating disorder [1]. Psychopathologically, FEDs represent heterogeneous variety of problems that are underpinned by body appearance and weight concerns [2].
Environmental risk factors were found to focus on most of the previous research on FEDs [3]; and were consequently held responsible for the development of FEDs. This is evident by events and influences in a person's life, including diet culture, the media, trauma, and weight teasing, as examples of environmental variables [3]. Previous studies showed multiple biopsychosocial influences implicated in FEDs and/or disordered feeding and eating symptoms [4]. Among other risk factors are a sociocultural idealization of thinness variables, personality traits, and chronic stress [5].
Symptoms of FEDs are significantly comorbid with many other mental health problems, such as depression, post-traumatic stress disorder, and anxiety [6,7,8,9]. Studies previously found an increasing prevalence of FEDs crossing age, gender, and culture [10,11,12]. Sociodemographic factors were found to be associated with FEDs [4, 13]. The most consistent factors linked to higher FEDs prevalence and incidence were as follows: female sex, younger age, sexual and physical abuse, participation in esthetic or weight-oriented sports, and heritability [13]. Mortality ratios are the highest in persons with FEDs compared to other mental disorders, with higher ratios among anorexia nervosa patients [5, 14,15,16]. Suicidal attempts and suicide ideation are also high in patients with FEDs [16, 17].
Many studies reported a high prevalence of mental health problems in medical students [18,19,20]. In their systematic review and meta-analysis published in 2018, Jahrami and colleagues found that the summary prevalence of eating disorders risk in medical students was 10.4% [21]. This review has shown that eating disorders symptoms were more prevalent in female medical students [21]. Other past studies reported high FEDs risks and prevalence in medical students because of the academic requirements and high workload, their young age, elevated BMI, body image, self-image, and exposure to sicknesses and death during their medical studies [21,22,23,24]. Moreover, earlier literature reports found increased prevalence of FEDs in Western countries, suggesting that despite globalization, Western culture could be a potential factor impacting the development of feeding and eating problems [25].
Mental health stigma is one of the major barriers to seeking help and in medical students in particular, because of social attitudes towards people with mental disorders and self-image and social expectations from them as future physicians [26,27,28,29]. The high prevalence of mental health problems and mental health stigma in medical students call for further studies to understand the prevalence and seeking help moods for each mental health disorder. This systematic review and meta-analysis aimed (1) to pool results of the global prevalence of FEDs symptoms in medical students, and (2) to assess whether this prevalence varies as a function of sex, age, BMI, or culture. Given that reported stress levels and mental health symptoms have been increasing slightly over the past years among students [30,31,32], we hypothesized to find an increased prevalence of FEDs symptoms in our target population. Additionally, we hypothesized that prevalence of FEDs symptoms would be higher among females, students with higher BMI and those from Western countries. Our review efforts have focused on examining the cumulative prevalence rate of FEDs symptoms in medical students of a variety of age groups, genders, and cultural and ethnic backgrounds. We acknowledge that FEDs encompass a large variety of heterogenous symptoms and we are interested in assessing whether they meet threshold levels and also those who are at risk of developing them. This is analogous to the new eating disorder category was introduced in the DSM-5, Unspecified Feeding and Eating Disorders (UFED), within which symptoms are neither diagnosis-specific nor clinically significant.
Methods
Prior the start of the project the protocol was registered on PROSPERO CRD42021275637. The population or problem/intervention or exposure/comparison and outcome (PICO) approach was used to define the review problem. The problem was eating disorders symptoms. The Intervention/exposure was being a medical student. The comparison was within group analysis by age, gender, research tool, country and culture. The outcome was prevalence rate [33]. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020 (PRISMA 2020) statement was used as a guide for conducting and reporting this review [34]. The Data extraction for complex meta-analysis (DECiMAL) guide was used to extract all data [35]. The systematic review was screened and coded using RAYYAN, a free online tool of digital technologies such as natural language processing, artificial intelligence, and machine learning [36]. WebPlotDigitizer v4.5, an open-source web-based tool, was used to extract numerical data from plot images [37]. References were managed using EndNote 9.3.3.
Database searches
Reviewers FFR and HJ conducted an electronic search using nine electronic academic databases (1-American Psychological Association PsycINFO; Cumulative Index to Nursing and Allied Health Literature (CINAHL); EBSCOhost Research Platform; Embase; MEDLINE; ProQuest; ScienceDirect; Scopus; and Web of Science). These databases were searched from the inception of each source to 15th September 2021.
Crossmatching keywords chosen based on key phrases and the Medical Subjects Headings was part of the search strategy. In a (All Fields) search, the Boolean logic operators [(OR) within lists], [(AND) between lists] were utilized to create the search. The lists were as follows: List A: medical student (OR) medical intern (OR) student doctor (OR) medical trainee (OR) medical pupil. (AND) List B: eating disorder (OR) feeding disorder (OR) eating problem (OR) eating attitude (OR) eating symptoms (OR) eating behavior.
We did not apply any limitations during our initial search. Manual screening of the references of the identified papers was also conducted by the review team.
Inclusion and exclusion criteria
Observational studies examining the prevalence rate of FEDs symptoms in undergraduate medical students were included. Specific inclusion criteria included: (1) studies must have been published in the English language; (2) published before 15th September 2021; (3) focused on undergraduate medical students, and (4) revealed the prevalence of FEDs symptoms/risk in the target population. In this review, FEDs risk was defined as significant changes in feeding or eating patterns along with psychological changes. Included studies should have used any validated, standardized tools to screen for FEDs risk, including Eating Attitudes Test-26 (EAT-26) [38], SCOFF Questionnaire [39], Eating Disorder Examination Questionnaire (EDE-Q) [40], and Eating Disorder Inventory (EDI) [41]. Thus, we reported estimates for FEDs symptoms/risk based on self-report questionnaires that cannot qualify for a specific clinical diagnosis. After symptoms screening, a structured interview by a clinician is needed to confirm the diagnosis. Detailed description of the clinical scales involved in the systematic review and meta-analysis of FEDs among medical students, psychometric properties, cut-off points and full citation presented in Table 1.
Specific exclusion criteria were: (1) studies that combined medical and non-medical students in the same group without analyzing subgroup data; (2) studies that assessed mental health problems rather than the prevalence of FEDs; (3) inability to get the full text even after contacting the authors. In case of duplication of dataset in the literature, the first publication was included in the meta-analysis.
Outcomes and measures
For each study, we reported the total sample size and the event rate. The event rate was categorized using pre-defined cut-off scores from continuous measures of eating pathology risk, to determine FEDs risk in medical students as a primary outcome. Cut-off scores were established by the developers of these tools to indicate a risk of FEDs (e.g., a score of ≥ 20 points on EAT-26 or a score of ≥ 2 points on SCOFF). As secondary outcomes, the studies were compared concerning variability in the prevalence of FEDs risk based on age and sex of participants, country of study, Western vs non-Western culture, and tool used in the study.
Two members of the review team independently evaluated studies for eligibility and screened titles, abstracts, and full-texts. Two independent members of the team performed initial data extraction and assessed quality. In case of disagreement, discussion with the senior reviewer/expert clinician, HJ and a consensus by the panel resolved any conflicts regarding the appropriateness of the study to include in the review.
Data extraction was standardized by collecting the following variables: study characteristics, including author name, year, sample size, country (Western/non-Western), and measure used. Participant characteristics including mean age (years), sex (proportion of female participants), mean body mass index (BMI) (kg/m2), and the main findings of the event rate of FEDs symptoms in medical students in each study. Western countries were those defined by the United Nations as members of the Western European and Other States group (Andorra, Australia, Austria, Belgium, Canada, Denmark, Finland, France, Germany, Greece, Iceland Ireland, Israel, Italy, Liechtenstein, Luxembourg, Malta, Monaco, Netherlands, New Zealand, Norway, Portugal, San Marino, Spain, Sweden, Switzerland, Turkey, United Kingdom of Great Britain and Northern Ireland, and United States of America) [42]. Email communication was used to request missing data from the corresponding author of the included studies.
Quality assessment using the Newcastle–Ottawa Scale (NOS)
Quality assessment was performed using the NOS [43]. Three elements were examined using the NOS checklist (participant’s selection, comparability, and outcome and statistics). NOS is based on a star rating system, with each study receiving a maximum of nine stars (cross-sectional and cohort studies) or ten stars (case–control studies) [43]. In this review, a study with a score ≥ of 8 has good quality and low risk of bias, a score of 5–7 has a moderate quality and moderate risk of bias), and a score of 0–4 has low quality and high risk of bias.
Data synthesis and statistical analyses
In this meta-analysis, data were pooled in accordance to the DerSimonian-Laird method [44], with the pooled prevalence and the 95% confidence interval having been reported. Random-effects Meta-analysis is a technique for synthesizing data based on the assumption that actual effects vary across studies [45]. The random-effects model assumes that each study estimates a different true effect, and that this true effect has a distribution (usually a normal distribution) [45]. The choice of a model must be based exclusively on whatever model best fits the distribution of effect sizes and takes into consideration the relevant source(s) of error. When a research is taken from the published literature, the random effects model is usually a better fit [46]. Data were displayed graphically using Forest plots [47]. Researchers used these confidence intervals to determine whether an impact is substantial; accordingly Drapery plots [48] and P-curve analysis were also reported [49].
We assessed study heterogeneity using the I2 statistic; a value of 75–100% was represented as a high heterogeneity [50]. The H was also reported as a mathematical transformation that describes the proportion of total variation in study estimates due to heterogeneity is I2 [50]. This review also assessed the between-study heterogeneity using Cochran’s Q statistics [51], tau2 (τ2), and tau (τ) [50].
We performed a leave-one-out sensitivity analysis (Jackknife analysis) by eliminating one study at a time to verify that our results were not influenced by a single study [52]. When the probability of publication is influenced by its findings, this is known as a publication bias [53].
The inclusion of outliers may jeopardize the meta-analysis’ validity and robustness. Outliers were therefore discovered and eliminated. If the study’s confidence interval does not match the pooled effect’s confidence interval, it is classified as an outlier [54].
To investigate publication bias, funnel plots were employed as a visual tool [55]. To conduct a rigorous analysis of publication bias, Kendall’s rank-order correlations [56] and Egger’s regression [55] were utilized. The trim and fill approach developed by Duval and Tweedie [57] to generate adjusted point estimates to correct for funnel plot asymmetry owing to probable publication bias was pre-planned to handle any bias.
In a meta-analysis, confounders analysis is the use of a method to find and account for systematic differences in the size of the effect or outcome that is being meta-analyzed [50, 58]. Meta-regression is one type of confounders analysis in which the observed effect sizes are regressed on one or more study characteristics [59]. There are other ways to conduct a confounders analysis; for example, one could simply subgroup studies according to categorical potential confounders [50].
All data analyses were performed using R software for Statistical Computing [60]. Package ‘PRISMA2020’ was used for making a selection flow diagram [61]. The packages ‘meta’ [62] and ‘metafor’ [63] were used to perform all meta-analytics. Quality assessment plots were produced using risk-of-bias visualization ‘robvis’ [64]. The traffic light plot, which tabulates the judgment for each study in each area of the NOS, was used to graphically show the findings of the quality evaluation [64]. For all investigations, a summary plot (weighted) was generated to show the proportion of information inside each judgment for each domain [64].
Results
Descriptive description of the studies included
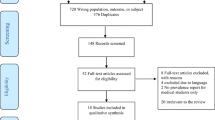
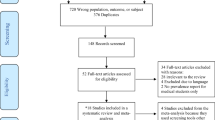
From the inception of the databases through September 15, 2021, the search was conducted. A total of 1528 records were identified through electronic database searches and other sources. After removing duplicate records, there were 944 records left. Records marked as ineligible by automation tools and records removed for other reasons were 659. We screened 285 and excluded 164 based on criteria. We evaluated 121 prospective articles in their entirety. Ninety-seven papers were excluded, including narrative, systematic and comment essays, letters to the editor, position statements, irrelevant literature, duplicate papers, and incorrectly classified publications. A total of 28 studies were included in the systematic review and meta-analysis. The search procedure was depicted in Fig. 1 using the PRISMA2020 flowchart.

PRISMA 2020 flow diagram for study selection
A total of 28 independent studies [24, 65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91] (28 cross-sectional studies, 35 subgroups, i.e., multiple tools, or multiple data points) comprising 21,383 participants from 20 countries were included in the analyses. The countries were: Austria N = 2; Egypt N = 1; France N = 2; Germany N = 2; Hungary N = 4; India N = 5; Korea N = 1; Lebanon N = 4; Malaysia N = 1; Malaysia N = 1; Mexico N = 1; Morocco N = 1; Norway N = 1; Palestine N = 2; Poland N = 1; Romania N = 1; Saudi Arabia N = 2; Spain N = 1; Thailand N = 1; and United States N = 1.
Five studies [68, 71, 72, 82, 90] utilized two screening tools to assess FEDs symptomatology. Furthermore, one study was cross-sectional at two time points [90]. The tools used were: Eating Attitudes Test-26 (EAT-26) N = 11; Sick, Control, One Stone, Fat, Food (SCOFF) N = 7; Eating Disorder Inventory-I/II (EDI) N = 6; Anorexia Nervosa Inventory for Self-Rating (ANIS) N = 3; Eating Disorder Examination- Questionnaire (EDEQ) N = 3; Eating Disturbance Scale (EDS) N = 2; ORTO-15 N = 2; and Dutch Eating Behavior Questionnaire N = 1.
The mean sample size was 611 (95% C.I. 445–776) participants. The median was 538 and the minimum and maximum were 90 and 2551, respectively. Participants were mainly females 65% (95% C.I. 59–70%), four studies focused only on female participants. The mean age was 21.8 years (95% C.I. 21.1–22.3 years), and the median was 22 years. The mean BMI was 22.1 kg/m2 (95% C.I. 21.8–22.4 kg/m2), and the median was 22 kg/m2. About 60% of the studies were published after 2018, with 40% being in the past two years. Only one study collected data from medical students during the COVID-19 pandemic.
The mean NOS quality score was 7.2 ± 0.75 and ranged from 5.0 to 8.0. Detailed examination of quality assessment for each study included in the meta-analysis is presented in Fig. 2. According to the summary results, 91% of the studies were of excellent quality, while the rest were of moderate quality. The majority of the risk bias was found in the selection dimension, especially in the sample size and representativeness, as shown in Fig. 3. Table 2 lists the summary characteristics of all considered studies.

Traffic light plot of included studies

Summary plot of the assessment of risk of bias
FEDs risk in medical students: a meta-analysis
Global assessment of FEDs risk in medical students
Using all available studies, a random-effects meta-analysis evaluated the prevalence of FEDs symptoms in medical students (K = 35, N = 21,383), and generated a pooled prevalence rate of 17.35% (95% CI 14.15–21.10%), heterogeneity [Q = 1528 (34), P = 0.001], τ2 = 0.51 (95% CI 0.36–1.05), τ = 0.71 (95% CI 0.59–1.02), I2 = 97.8%; H = 6.70 (95% CI 6.19–7.26). Using any FEDs measure in medical students, the raw prevalence estimates for FEDs problems varied from 5 to 74%. Figure 4 depicts the forest plot of the meta-analysis of FEDs risk in medical students using all assessment measures. Figure 5 presents the drapery plots of FEDs symptoms in medical students.

Meta-analysis of FEDs symptoms in medical students

Drapery plots of FEDs symptoms in medical students
A (leave-one-out) sensitivity analysis found that no study had a greater than 1% impact on the global prevalence estimate of FEDs risk in medical students. Influence analysis was used to identify and eliminate outliers in our meta-analysis. Results of outliers’ analysis revealed that nine studies contributed with thirteen data points were mathematical outliers [65, 66, 71, 72, 78, 81, 82, 87, 90]. After removing all outlier studies, meta-analytic results revealed random-effects model of the prevalence of FEDs in medical students of 16.58% (95% CI 15.25–17.99%), heterogeneity Q = 72.71 (21) P < 0.0001, τ2 = 0.03 (95% CI 0.01–0.11); τ = 0.18 (95% CI 0.12–0.33), I2 = 71.1% (95% CI 55.6–81.2%); H = 1.86 (95% CI 1.50–2.31).
Visual inspection to funnel plot in Fig. 6 showed no significant publication bias, Egger’s regression (P = 0.05) and Begg's rank correlation test (P = 0.21) confirmed the absence of publication bias. Thus, the trim-and-fill technique was unnecessary to estimate and compensate for the quantity and findings of missing studies. Detailed influence analysis on the effect size and the heterogeneity markers is depicted in Fig. 7.

Funnel plot of FEDs symptoms in medical students

Influence analysis of FEDs symptoms in medical students
Meta-regression analysis revealed that neither age nor sex moderated the global prevalence rate of FEDs risk in medical students (P = 0.65 and P = 0. 0.85, respectively). After controlling for age and sex, BMI was a strong statistical confounder in both univariate meta-regression analysis (P = 0.001); and multivariate meta-regression analysis (P = 0.001, Fig. 8). These findings are further detailed in Table 3.

Meta-regression between BMI and FEDs symptoms in medical students.
FEDs risk in medical students by country
Nine countries had two or more studies, allowing to perform a subgroup meta-analysis. Results showed that overall pooled prevalence rate of FEDs symptoms in medical students varied significantly (Q = 263 (18), P < 0.0001), with the lowest being in Austria (K = 2, N = 758) and Hungary (K = 2, N = 3014), and the highest being in Lebanon (K = 4, N = 1509) [prevalence risk: 07.05% (95% CI 03.34–14.29%), 07.81% (95% CI 04.79–12.48%), and 33.43% (95% CI 12.00–64.90%), respectively]. Heterogeneity significantly improved for India (16.33% (95% CI 13.56–19.54%), I2 = 50.6%); Germany (12.36% (95% CI 08.44–17.74%), I2 = 46.2%); Saudi Arabia (12.11% (95% CI 09.42–15.43%), I2 = 59.8%); and France (17.97% (95% CI 15.97–20.17%), I2 = 31.2%). Detailed prevalence of FEDs risk in medical students by country is presented in Table 3.
FEDs risk in medical students by culture
Participants from non-Western cultures had a statistically higher prevalence of FEDs risk in medical students compared to participants from Western cultures [Q = 6.41(1), P = 0.01]. Specifically, pooled prevalence rate of FEDs symptoms in participants from non-Western cultures (K = 21, N = 10,304) was 20.97% (95% CI 15.74–27.36%), I2 = 98%, τ2 = 0.64; and the overall pooled prevalence rate of FEDs symptoms in participants from Western cultures (K = 14, N = 11,079) was 12.98% (95% CI 10.18–16.42%), I2 = 96%, τ2 = 0.25. Detailed prevalence of FEDs risk in medical students by culture is presented in Table 3.
FEDs risk in medical students by measure
Six tools were used to measure the prevalence of FEDs symptoms in medical students. Detailed prevalence of FEDs risk in medical students by measure is presented in Table 3.
The most common research measure was the Eating Attitude Test-26 (EAT-26) with 32% of the studies using this measured (K = 11, N = 6486). Results from EAT-26 showed an overall prevalence rate of FEDs symptoms in medical students of 17.85% (95% CI 13.82–22.76%), I2 = 95.2%; τ2 = 0.49. The highest pooled prevalence rate of FEDs symptoms in participants [51.75% (95% CI 13.12–88.40%)] was obtained using the ORTO-15 measure (K = 2, N = 1747). The lowest pooled prevalence rate of FEDs symptoms in participants [08.97% (95% CI 04.97–15.63%)] was obtained using the Eating Disorder Inventory (EDI-I/II) (K = 6, N = 4851). Detailed descriptions of the measures used in various studies are included in the legend of Table 3.
Studies that used Eating Disorder Examination Questionnaire (EDE-Q) (K = 3, N = 711) appeared to be the best in terms of heterogeneity with I2 = 0%, suggesting that results obtained by EDE-Q are consistent in different sample groups.
Discussion
A total of 21,383 medical students executed from 35 research data belong to 20 countries were included in this systematic review and meta-analysis. This review demonstrated that 17.35% of medical students screened positive for FEDs symptoms. Meta-regression analysis showed that FEDs symptoms were not associated with age nor sex. However, increased BMI was a strong statistical predictor of FEDs symptoms. A statistically significant difference was obtained between non-Western vs Western cultured students (P = 0.001), explaining differences between countries. The highest prevalence of FEDs symptoms was obtained by ORTO-15 suggesting that orthorexia nervosa (ON) symptoms, which is a FEDs characterized by an unhealthy obsession with healthy eating being the major concern.
In accordance with our first hypothesis, this meta-analysis found an overall prevalence of FEDs symptoms in medical students of 17.35%, hence showing an increase as compared to previous research. Indeed, an earlier meta-analysis using the same methods in 2018 reported an overall prevalence rate of FEDs symptoms in medical students to be 10.40% [21]. Moreover, medical students displayed higher prevalence rates of FEDs symptoms as compared to community samples across the globe [e.g., Canada (N = 31,130, 50.9% female, risk of lifetime history of an eating disorder of 4.54%) [92], Spain (N = 4334, 55.9% females, prevalence of population at risk for eating disorders of 2.2% for men and 15.3% for women) [93], Australia (N = 3034, 67% female, prevalence of eating disorder behaviors of 6.4%) [94], London (N = 1,698, 56.6% female, prevalence of reported disordered eating of 10%) [95], US (N = 100 000, 50% female, annual prevalence of eating disorders occurring at age 21 years for males 7.4% and females 10.3%) [96], and six European countries (Belgium, France, Germany, Italy, the Netherlands and Spain) (N = 4139, 51.6% female, lifetime estimated prevalence of eating disorders 0.48–2.15%) [97]]. Over the past years, the student population is increasingly facing high amounts of stress leading to more prevalent mental health challenges. The WHO World Mental Health International College Student project found ‘rising’ and ‘widely distributed’ rates of mental disorders among students in 19 colleges across 8 countries [98]. Medical students have been found to be exposed to more stressors and to experience more mental health issues as compared to students from other fields [99,100,101], and to age-matched general population [102]. This might explain the significant increase in the FEDs symptoms observed in medical students between 2018 and 2021. However, the extent to which the medical students’ population might be at a specific high risk for FEDs compared to other populations remains unknown [90]. Future studies comparing FEDs symptoms of medical students with that of non-medical students and of the general population might shed light on the role of medical education-related factors (e.g., the choice of a medical career) on the prevalence of FEDs risk.
We expected to find higher FEDs symptoms among female students than males. However, our review showed that both male students are at a comparable risk of FEDs symptoms compared to females. FEDs has long been thought to be a disease that mainly affects early teenage girls; nevertheless, the frequency of FEDs in men is on the rise, requiring care providers' attention to battle these complicated biopsychological diseases [103]. The stigma associated with male FEDs is a significant concern. The misconception that FEDs primarily affects women has resulted in feelings of guilt and isolation in men who are affected, delaying their seeking of assistance and therapy. As a result, initiatives should be developed to make care more accessible to both men and women.
Furthermore, according to our secondary hypothesis, we expected to find a higher prevalence risk of FEDs in medical students with western background. However, our findings provided evidence against this hypothesis. In addition, the increase in prevalence of FEDs symptoms was mainly observed in participants from non-Western countries. This might be explained by the fact that FEDs is a global problem, and as the world's population and westernization expand, so do reports of FEDs in non-Western cultures. Consistent with this finding, Weigel et al. found that medical students from the newly formed German states reported higher levels of drive for thinness and body dissatisfaction as compared to a historical sample of East German medical students, suggesting “an acculturation to Western beauty ideals” [91]. In the same line, a meta-analysis of 94 studies using the EDI by Podar and Allik found more pronounced symptoms of eating disorders in non-Western than Western participants [104]. There has been a rise in body dissatisfaction within the population, particularly in university students in non-Western civilizations [105]. Fiji has contributed to a better knowledge of eating disorders in non-Western cultures throughout the world [106, 107]. The conventional definition of beauty in Fiji was a female figure that was heavier, rounder, and softer. Back to late 1990s, eating disorders rise steeply after the introduction of media and Western television [106]. Body dissatisfaction, dieting, the desire to lose weight, the slim ideal, and disordered eating practices were all on the rise as risk factors. Fijian society’s definition of female beauty was also redefined as a more ‘Westernized’ ‘thin ideal’ [108].
Our findings supported the hypothesis that elevated BMI is associated with greater FEDs symptoms in medical students. Indeed, there is some evidence that suggests that increased weight is associated with different types of FEDs symptoms [109] and is one of the risk factors for their development and maintenance [110,111,112]. For instance, a recent online survey of a large cohort of 13,341 individuals seeking medical weight correction assistance found that obesity was associated with a higher eating disorders risk [113]. Yilmaz et al. [121] found that premorbid metabolic factors in addition to weight could be relevant factors to the etiology of FED. However, it is worth noting that existing literature regarding the relationship between eating disorders and BMI was mainly limited to adolescents or students, and has shown mixed results [114,115,116,117,118,119]. For example, Sanlier et al. surveyed university students in Turkey and found that there was not a significant difference in EAT-40 scores (Eating attitudes and eating disorders test) according to gender and BMI classification [120]. Contrarily, a low premorbid weight was considered as a key biological risk factor or early manifestation of an emerging disease process in anorexia nervosa [121]. These inconsistent findings call for further epidemiological studies on the link between BMI and FEDs risk.
The current review is the largest and most updated systematic review and meta-analysis on the topic, which represents its major strength. To manage bias, detect outliers, and assess heterogeneity, robust statistical tests were utilized. The generalizability of the present review's results is also expected to be good because the pooled sample size was extremely big and the participants were recruited from a variety of nations. The second strength of this review is based on using the best available standards that enable objective evaluation of the quality of published evidence using a comprehensive and detailed assessment of the risk of bias of a large number of studies. Finally, this meta-analysis resolved uncertainty when studies disagree regarding FEDs in medical students.
Despite these strengths, certain limitations need to be discussed. The major limitation of this review are the focus on English language papers only. However, to the author’s knowledge, non-English papers were very few in peer review journals. Another limitation was the presence of increased heterogeneity. In addition, there is a lack of direct comparison between medical students and other populations (e.g., non-medical students, the general population). Moreover, we have suggested an increase of the prevalence of FEDs risk among medical students based on a prior meta-analysis published in 2018 by Jahrami et al. using the same methods; however, comparing our current findings with this previous work may be affected by the type of FEDs included in the meta-analyses. Finally, all studies included in this meta-analysis presented self-reported data, and none of them included individuals with clinically diagnosed FEDs.
Conclusion
The prevalence of FEDs symptoms in medical students was estimated to be increasing in the past few years, reaching a pooled prevalence rate of 17.35%. The findings of future prospective studies are urgently required to better understand the interactions between the risk factors and to use the information to construct prevention and treatment programs, in order to provide better outcomes for students at risk to or suffering from FEDs.
What is already known on this subject?
-
Previous literature has pointed that medical students displayed higher prevalence rates of eating disorders risk as compared to the general population; which calls for further studies on this topic.
-
Female medical students were reported to be at more risk for eating disorders than male medical students. Other risk factors for FEDs have also been reported among this population, including elevated BMI and western origin.
What does this study add?
-
This review showed that the overall prevalence rate of FEDs symptoms in medical students (17.35%) was higher than those reported in prior research.
-
Male and female students were affected similarly by risk of FEDs symptoms, which implies that efforts should be made to provide stigma-free care access for FEDs problems to male students.
-
Medical students from non-Western cultures reported higher prevalence of FEDs compared to students from Western cultures, highlighting that prominent attention should be given to FEDs problems in medical schools in non-Western countries.
References
APA (2013) Diagnostic and statistical manual of mental disorders: DSM-5. United States
Fairburn CG, Harrison PJ (2003) Eating disorders. Lancet 361(9355):407–416. https://doi.org/10.1016/s0140-6736(03)12378-1
Mazzeo SE, Bulik CM (2009) Environmental and genetic risk factors for eating disorders: what the clinician needs to know. Child Adolesc Psychiatr Clin N Am 18(1):67–82. https://doi.org/10.1016/j.chc.2008.07.003
Culbert KM, Racine SE, Klump KL (2015) Research Review: What we have learned about the causes of eating disorders—a synthesis of sociocultural, psychological, and biological research. J Child Psychol Psychiatry 56(11):1141–1164. https://doi.org/10.1111/jcpp.12441
Rantala MJ, Luoto S, Krama T, Krams I (2019) Eating disorders: an evolutionary psychoneuroimmunological approach. Front Psychol 10:2200. https://doi.org/10.3389/fpsyg.2019.02200
Keski-Rahkonen A, Mustelin L (2016) Epidemiology of eating disorders in Europe: prevalence, incidence, comorbidity, course, consequences, and risk factors. Curr Opin Psychiatry 29(6):340–345. https://doi.org/10.1097/yco.0000000000000278
Swinbourne J, Hunt C, Abbott M, Russell J, St Clare T, Touyz S (2012) The comorbidity between eating disorders and anxiety disorders: prevalence in an eating disorder sample and anxiety disorder sample. Aust N Z J Psychiatry 46(2):118–131. https://doi.org/10.1177/0004867411432071
Mischoulon D, Eddy KT, Keshaviah A, Dinescu D, Ross SL, Kass AE et al (2011) Depression and eating disorders: treatment and course. J Affect Disord 130(3):470–477. https://doi.org/10.1016/j.jad.2010.10.043
Brewerton TD (2007) Eating disorders, trauma, and comorbidity: focus on PTSD. Eat Disord 15(4):285–304. https://doi.org/10.1080/10640260701454311
Hoek HW (2016) Review of the worldwide epidemiology of eating disorders. Curr Opin Psychiatry 29(6):336–339. https://doi.org/10.1097/yco.0000000000000282
Sweeting H, Walker L, MacLean A, Patterson C, Räisänen U, Hunt K (2015) Prevalence of eating disorders in males: a review of rates reported in academic research and UK mass media. Int J Mens Health. https://doi.org/10.3149/jmh.1402.86
Smink FR, van Hoeken D, Hoek HW (2012) Epidemiology of eating disorders: incidence, prevalence and mortality rates. Curr Psychiatry Rep 14(4):406–414. https://doi.org/10.1007/s11920-012-0282-y
Mitchison D, Hay PJ (2014) The epidemiology of eating disorders: genetic, environmental, and societal factors. Clin Epidemiol 6:89–97. https://doi.org/10.2147/CLEP.S40841
Arcelus J, Mitchell AJ, Wales J, Nielsen S (2011) Mortality rates in patients with anorexia nervosa and other eating disorders. A meta-analysis of 36 studies. Arch Gen Psychiatry 68(7):724–731. https://doi.org/10.1001/archgenpsychiatry.2011.74
Rosling AM, Sparén P, Norring C, von Knorring AL (2011) Mortality of eating disorders: a follow-up study of treatment in a specialist unit 1974–2000. Int J Eat Disord 44(4):304–310. https://doi.org/10.1002/eat.20827
Suokas JT, Suvisaari JM, Gissler M, Löfman R, Linna MS, Raevuori A et al (2013) Mortality in eating disorders: a follow-up study of adult eating disorder patients treated in tertiary care, 1995–2010. Psychiatry Res 210(3):1101–1106. https://doi.org/10.1016/j.psychres.2013.07.042
Steinhausen HC (2009) Outcome of eating disorders. Child Adolesc Psychiatr Clin N Am 18(1):225–242. https://doi.org/10.1016/j.chc.2008.07.013
Onyishi M, Talukdar D, Sanchez R (2016) Prevalence of clinical depression among medical students and medical professionals: a systematic review study. Arch Med. https://doi.org/10.21767/1989-5216.1000178
Quek TT-C, Tam WW-S, Tran BX, Zhang M, Zhang Z, Ho CS-H et al (2019) The global prevalence of anxiety among medical students: a meta-analysis. Int J Environ Res Public Health 16(15):2735. https://doi.org/10.3390/ijerph16152735
Jahrami H, Dewald-Kaufmann J, MeA-I F, AlAnsari AMS, Taha M, AlAnsari N (2020) Prevalence of sleep problems among medical students: a systematic review and meta-analysis. J Public Health 28(5):605–622. https://doi.org/10.1007/s10389-019-01064-6
Jahrami H, Sater M, Abdulla A, AlAnsari A (2019) Eating disorders risk among medical students: a global systematic review and meta-analysis. Eat Weight Disord-Stud Anorex Bulim Obes 24(3):397–410
Bosi M, Nogueira J, Alencar C, Moreira J (2016) Body image and eating behavior among medical students: eating disorders among medical students. Epidemiology (Sunnyvale) 6:256. https://doi.org/10.4172/2161-1165.1000256
Jahrami H, Saif Z, Faris MA, Levine MP (2019) The relationship between risk of eating disorders, age, gender and body mass index in medical students: a meta-regression. Eat Weight Disord 24(2):169–177. https://doi.org/10.1007/s40519-018-0618-7
Brumboiu MI, Cazacu I, Zunquin G, Manole F, Mogosan CI, Porrovecchio A et al (2018) Nutritional status and eating disorders among medical students from the Cluj-Napoca University centre. Clujul Med 91(4):414
Syurina EV, Bood ZM, Ryman FVM, Muftugil-Yalcin S (2018) Cultural Phenomena believed to be associated with orthorexia nervosa—opinion study in Dutch health professionals. Front Psychol 9:1419. https://doi.org/10.3389/fpsyg.2018.01419
Hankir AK, Northall A, Zaman R (2014) Stigma and mental health challenges in medical students. BMJ Case Rep. https://doi.org/10.1136/bcr-2014-205226
Giasuddin NA, Levav I, Gal G (2014) Mental health stigma and attitudes to psychiatry among Bangladeshi medical students. Int J Soc Psychiatry 61(2):137–147. https://doi.org/10.1177/0020764014537237
Gold JA, Johnson B, Leydon G, Rohrbaugh RM, Wilkins KM (2015) Mental health self-care in medical students: a comprehensive look at help-seeking. Acad Psychiatry 39(1):37–46. https://doi.org/10.1007/s40596-014-0202-z
Kopera M, Suszek H, Bonar E, Myszka M, Gmaj B, Ilgen M et al (2015) Evaluating explicit and implicit stigma of mental illness in mental health professionals and medical students. Community Ment Health J 51(5):628–634. https://doi.org/10.1007/s10597-014-9796-6
Asher BlackDeer A, Patterson Silver Wolf DA, Maguin E, Beeler-Stinn S (2021) Depression and anxiety among college students: understanding the impact on grade average and differences in gender and ethnicity. J Am Coll Health. https://doi.org/10.1080/07448481.2021.1920954
Wiens K, Bhattarai A, Pedram P, Dores A, Williams J, Bulloch A et al (2020) A growing need for youth mental health services in Canada: examining trends in youth mental health from 2011 to 2018. Epidemiol Psychiatr Sci 29:e115. https://doi.org/10.1017/s2045796020000281
Abdelaziz AMY, Alotaibi KT, Alhurayyis JH, Alqahtani TA, Alghamlas AM, Algahtani HM et al (2017) The association between physical symptoms and depression among medical students in Bahrain. Int J Med Educ 8:423–427. https://doi.org/10.5116/ijme.5a2d.16a3
Methley AM, Campbell S, Chew-Graham C, McNally R, Cheraghi-Sohi S (2014) PICO, PICOS and SPIDER: a comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv Res 14(1):579. https://doi.org/10.1186/s12913-014-0579-0
Page MJ, Moher D, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD et al (2021) PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ 372:n160
Pedder H, Sarri G, Keeney E, Nunes V, Dias S (2016) Data extraction for complex meta-analysis (DECiMAL) guide. Syst Rev 5(1):212. https://doi.org/10.1186/s13643-016-0368-4
Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A (2016) Rayyan—a web and mobile app for systematic reviews. Syst Rev 5(1):1–10
PLOTCON: WebPlotDigitizer (2017) https://automeris.io/WebPlotDigitizer/. Accessed July 20, 2021
Garner DM, Olmsted MP, Bohr Y, Garfinkel PE (1982) The eating attitudes test: psychometric features and clinical correlates. Psychol Med 12(4):871–878. https://doi.org/10.1017/s0033291700049163
Morgan JF, Reid F, Lacey JH (2000) The SCOFF questionnaire. Western J Med 172(3):164
Mond JM, Hay PJ, Rodgers B, Owen C (2006) Eating disorder examination questionnaire (EDE-Q): norms for young adult women. Behav Res Ther 44(1):53–62. https://doi.org/10.1016/j.brat.2004.12.003
Garner DM, Olmstead MP, Polivy J (1983) Development and validation of a multidimensional eating disorder inventory for anorexia nervosa and bulimia. Int J Eat Disord 2(2):15–34. https://doi.org/10.1002/1098-108X(198321)2:2%3c15::AID-EAT2260020203%3e3.0.CO;2-6
Nations U (2021) https://www.un.org/dgacm/en/content/regional-groups. Accessed 18 Sept 2021
Luchini C, Stubbs B, Solmi M, Veronese N (2017) Assessing the quality of studies in meta-analyses: advantages and limitations of the Newcastle Ottawa Scale. World J Meta-Anal 5(4):80–84
Jackson D, White IR, Thompson SG (2010) Extending DerSimonian and Laird’s methodology to perform multivariate random effects meta-analyses. Stat Med 29(12):1282–1297
Shuster JJ (2010) Empirical vs natural weighting in random effects meta-analysis. Stat Med 29(12):1259–1265
Borenstein M, Hedges L, Rothstein H (2007) Meta-analysis: fixed effect vs. random effects. Meta-analysis.com
Lewis S, Clarke M (2001) Forest plots: trying to see the wood and the trees. BMJ 322(7300):1479–1480
Rücker G, Schwarzer G (2021) Beyond the forest plot: the drapery plot. Res Synth Methods 12(1):13–19
van Aert RC, Wicherts JM, van Assen MA (2016) Conducting meta-analyses based on p values: reservations and recommendations for applying p-uniform and p-curve. Perspect Psychol Sci 11(5):713–729
Higgins JP, Thompson SG (2002) Quantifying heterogeneity in a meta-analysis. Stat Med 21(11):1539–1558
Huedo-Medina TB, Sánchez-Meca J, Marin-Martinez F, Botella J (2006) Assessing heterogeneity in meta-analysis: Q statistic or I2 index? Psychol Methods 11(2):193
Patsopoulos NA, Evangelou E, Ioannidis JP (2008) Sensitivity of between-study heterogeneity in meta-analysis: proposed metrics and empirical evaluation. Int J Epidemiol 37(5):1148–1157. https://doi.org/10.1093/ije/dyn065
Mathur MB, VanderWeele TJ (2020) Sensitivity analysis for publication bias in meta-analyses. J Roy Stat Soc: Ser C (Appl Stat) 69(5):1091–1119
Viechtbauer W, Cheung MW (2010) Outlier and influence diagnostics for meta-analysis. Res Synth Methods 1(2):112–125. https://doi.org/10.1002/jrsm.11
Egger M, Smith GD, Schneider M, Minder C (1997) Bias in meta-analysis detected by a simple, graphical test. BMJ 315(7109):629–634. https://doi.org/10.1136/bmj.315.7109.629
Kendall M, Gibbons JD (1990) Rank correlation methods edward arnold. A division of Hodder & Stoughton, a Charles Griffin title. Oxford University Press, London, pp 29–50
Duval S, Tweedie R (2000) A nonparametric, “Trim and Fill” method of accounting for publication bias in meta-analysis. J Am Stat Assoc 95(449):89–98. https://doi.org/10.2307/2669529
Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ et al (2019) Cochrane handbook for systematic reviews of interventions. John Wiley & Sons, New York
Higgins JP, Thompson SG (2004) Controlling the risk of spurious findings from meta-regression. Stat Med 23(11):1663–1682. https://doi.org/10.1002/sim.1752
R: 4.1.1. https://www.R-project.org/ (2021). Accessed 05/05/2020.
Haddaway N, McGuinness L, Pritchard C (2021) PRISMA2020: R package and ShinyApp for producing PRISMA 2020 compliant flow diagrams (Version 0.0. 2)
Schwarzer G, Schwarzer MG (2012) Package ‘meta’. The R foundation for statistical computing, 9
Viechtbauer W (2010) Conducting meta-analyses in R with the metafor package. J Stat Softw 36(3):1–48
McGuinness LA, Higgins JP (2021) Risk-of-bias VISualization (robvis): an R package and Shiny web app for visualizing risk-of-bias assessments. Res Synth Methods 12(1):55–61
Ali EAA, Shehata WM (2020) Eating disorder risk among medical students at Tanta University, Egypt. Egyptian J Community Med 38(4):17
Azzouzi N, Ahid S, Bragazzi NL, Berhili N, Aarab C, Aalouane R et al (2019) Eating disorders among Moroccan medical students: cognition and behavior. Psychol Res Behav Manag 12:129
Barayan S, Al-Yousif Z, Sabra A (2018) Prevalence of eating disorders among female university medical students in Dammam, Saudi Arabia. Int J Med Health Sci 7(3):107–112
Bizri M, Geagea L, Kobeissy F, Talih F (2020) Prevalence of eating disorders among medical students in a lebanese medical school: a cross-sectional study. Neuropsychiatr Dis Treat 16:1879
Chan YL, Samy AL, Tong WT, Islam MA, Low WY (2020) Eating disorder among Malaysian University students and its associated factors. Asia Pacific J Public Health 32(6–7):334–339
Chaudhari B, Tewari A, Vanka J, Kumar S, Saldanha D (2017) The relationship of eating disorders risk with body mass index, body image and self-esteem among medical students. Ann Med Health Sci Res 7(3):144
Damiri B, Safarini OA, Nazzal Z, Abuhassan A, Farhoud A, Ghanim N et al (2021) Eating disorders and the use of cognitive enhancers and psychostimulants among university students: a cross-sectional study. Neuropsychiatr Dis Treat 17:1633
Farchakh Y, Hallit S, Soufia M (2019) Association between orthorexia nervosa, eating attitudes and anxiety among medical students in Lebanese universities: results of a cross-sectional study. Eat Weight Disord-Stud Anorex Bulim Obes 24(4):683–691
Herzog DB, Pepose M, Norman DK, Rigotti NA (1985) Eating disorders and social maladjustment in female medical students. J Nerv Mental Dis 173:734
Iyer S, Shriraam V (2021) Prevalence of eating disorders and its associated risk factors in students of a medical college hospital in South India. Cureus. 13(1):e12926
Joja O, von Wietersheim J (2012) A cross-cultural comparison between EDI results of Romanian and German students. Procedia Soc Behav Sci 33:1037–1041
Lee SJ, Cloninger CR, Chae H (2015) Cloninger’s temperament and character traits in medical students of Korea with problem eating behaviors. Compr Psychiatry 59:98–106
Pitanupong J, Jatchavala C (2017) Atypical eating attitudes and behaviors in Thai medical students. Siriraj Med J 69(1):5–10
Plichta M, Jezewska-Zychowicz M (2019) Eating behaviors, attitudes toward health and eating, and symptoms of orthorexia nervosa among students. Appetite 137:114–123
Paola PP, Luis M (2020) Estudio del riesgo de presentar trastornos alimentarios en un grupo de estudiantes de licenciatura y posgrado de instituciones mexicanas. Espacio I+D, Innovación más Desarrollo IX(23):54–68. https://doi.org/10.31644/IMASD.23.2020.a04
Ramaiah RR (2015) Eating disorders among medical students of a rural teaching hospital: a cross-sectional study. Int J Community Med Public Health 2:25
Ahmed SU (2018) Prevalence of eating disorders among medical students in Ipoh. Perak, Malaysia
Rathner G, Rumpold G (1994) Convergent validity of the eating disorder inventory and the anorexia nervosa inventory for self-rating in an austrian nonclinical population. Int J Eat Disord 16(4):381–393
Rostad IS, Tyssen R, Løvseth LT (2021) Symptoms of disturbed eating behavior risk: Gender and study factors in a cross-sectional study of two Norwegian medical schools. EatBehav 43:101565
Sepulveda A, Carrobles J, Gandarillas A, Poveda J, Pastor V (2007) Prevention program for disturbed eating and body dissatisfaction in a Spanish university population: a pilot study. Body Image 4(3):317–328
Sharma M, Singh SK, Tiwari P, Chauhan N (2019) Body image perception, eating attitude and influence of media among undergraduate students of medical college in Delhi: a cross sectional study. Int J Res Med Sci 7(12):4627
Spillebout A, Dechelotte P, Ladner J, Tavolacci MP (2019) Mental health among university students with eating disorders and irritable bowel syndrome in France. Rev Epidemiol Sante Publique 67(5):295–301
Taha AAAE-A, Abu-Zaid HA, Desouky DE-S (2018) Eating disorders among female students of Taif University, Saudi Arabia. Arch Iran Med 21(3):111–117
Tavolacci M, Delay J, Grigioni S, Déchelotte P, Ladner J (2018) Changes and specificities in health behaviors among healthcare students over an 8-year period. PloS one 13(3):e0194188
Thangaraju SI, Karpagalakshmi R, Arumuganathan S, Usaid S, Devi SS, Sethumadhavan V (2020) A cross-sectional study on prevalence of eating disorder and body image disturbance among female undergraduate medical students. J Ment Health Hum Behav 25(1):53
Túry F, Szabó P, Dukay-Szabó S, Szumska I, Simon D, Rathner G (2021) Eating disorder characteristics among Hungarian medical students: changes between 1989 and 2011. J Behav Addict 9(4):1079–1087
Weigel A, Hofmeister D, Pröbster K, Brähler E, Gumz A (2016) Eating pathology in medical students in Eastern Germany: comparison with general population and a sample at the time of the German reunification. Eat Weight Disord-Stud Anorex Bulim Obes 21(3):445–451
Pedram P, Patten SB, Bulloch AGM, Williams JVA, Dimitropoulos G (2021) Self-reported lifetime history of eating disorders and mortality in the general population: a canadian population survey with record linkage. Nutrients. https://doi.org/10.3390/nu13103333
Gandarillas A, Febrel C, Galán I, León C, Zorrilla B, Bueno R (2004) Population at risk for eating disorders in a Spanish region. Eat Weight Disord 9(3):179–185. https://doi.org/10.1007/bf03325064
Wong MNT, Hay P (2020) Exploring associations between age of onset and quality of life of people with eating disorder behaviours and weight/shape overvaluation: a general population study. Australas Psychiatry 28(6):660–663. https://doi.org/10.1177/1039856220928873
Solmi F, Hatch SL, Hotopf M, Treasure J, Micali N (2014) Prevalence and correlates of disordered eating in a general population sample: the South East London Community Health (SELCoH) study. Soc Psychiatry Psychiatr Epidemiol 49(8):1335–1346. https://doi.org/10.1007/s00127-014-0822-3
Ward ZJ, Rodriguez P, Wright DR, Austin SB, Long MW (2019) Estimation of eating disorders prevalence by age and associations with mortality in a simulated nationally representative US cohort. JAMA Netw Open 2(10):e1912925. https://doi.org/10.1001/jamanetworkopen.2019.12925
Preti A, Girolamo G, Vilagut G, Alonso J, Graaf R, Bruffaerts R et al (2009) The epidemiology of eating disorders in six European countries: results of the ESEMeD-WMH project. J Psychiatr Res 43(14):1125–1132. https://doi.org/10.1016/j.jpsychires.2009.04.003
Auerbach RP, Mortier P, Bruffaerts R, Alonso J, Benjet C, Cuijpers P et al (2018) WHO world mental health surveys international college student project: prevalence and distribution of mental disorders. J Abnorm Psychol 127(7):623–638. https://doi.org/10.1037/abn0000362
Al-Dabal BK, Koura MR, Rasheed P, Al-Sowielem L, Makki SM (2010) A Comparative study of perceived stress among female medical and non-medical university students in Dammam, Saudi Arabia. Sultan Qaboos Univ Med J 10(2):231–240
Shad R, Thawani R, Goel A (2015) Burnout and sleep quality: a cross-sectional questionnaire-based study of medical and non-medical students in India. Cureus 7(10):e361. https://doi.org/10.7759/cureus.361
Seedhom AE, Kamel EG, Mohammed ES, Raouf NR (2019) Predictors of perceived stress among medical and nonmedical college students, Minia, Egypt. Int J Prev Med 10:107. https://doi.org/10.4103/ijpvm.IJPVM_6_18
Quek TT, Tam WW, Tran BX, Zhang M, Zhang Z, Ho CS et al (2019) The global prevalence of anxiety among medical students: a meta-analysis. Int J Environ Res Public Health. https://doi.org/10.3390/ijerph16152735
Sangha S, Oliffe JL, Kelly MT, McCuaig F (2019) Eating disorders in males: how primary care providers can improve recognition, diagnosis, and treatment. Am J Mens Health 13(3):1557988319857424. https://doi.org/10.1177/1557988319857424
Podar I, Allik J (2009) A cross-cultural comparison of the eating disorder inventory. Int J Eat Disord 42(4):346–355. https://doi.org/10.1002/eat.20616
Pike KM, Dunne PE (2015) The rise of eating disorders in Asia: a review. J Eat Disord 3:33. https://doi.org/10.1186/s40337-015-0070-2
Becker AE, Burwell RA, Gilman SE, Herzog DB, Hamburg P (2002) Eating behaviours and attitudes following prolonged exposure to television among ethnic Fijian adolescent girls. Br J Psychiatry 180:509–514. https://doi.org/10.1192/bjp.180.6.509
Becker AE (2004) Television, disordered eating, and young women in Fiji: negotiating body image and identity during rapid social change. Cult Med Psychiatry 28(4):533–559. https://doi.org/10.1007/s11013-004-1067-5
Williams LK, Ricciardelli LA, McCabe MP, Waqa GG, Bavadra K (2006) Body image attitudes and concerns among indigenous Fijian and European Australian adolescent girls. Body Image 3(3):275–287. https://doi.org/10.1016/j.bodyim.2006.06.001
Fan Y, Li Y, Liu A, Hu X, Ma G, Xu G (2010) Associations between body mass index, weight control concerns and behaviors, and eating disorder symptoms among non-clinical Chinese adolescents. BMC Public Health 10:314. https://doi.org/10.1186/1471-2458-10-314
Burrows A, Cooper M (2002) Possible risk factors in the development of eating disorders in overweight pre-adolescent girls. Int J Obes Relat Metab Disord 26(9):1268–1273. https://doi.org/10.1038/sj.ijo.0802033
Fairburn CG, Cooper Z, Doll HA, Welch SL (1999) Risk factors for anorexia nervosa: three integrated case-control comparisons. Arch Gen Psychiatry 56(5):468–476. https://doi.org/10.1001/archpsyc.56.5.468
Haines J, Neumark-Sztainer D (2006) Prevention of obesity and eating disorders: a consideration of shared risk factors. Health Educ Res 21(6):770–782. https://doi.org/10.1093/her/cyl094
Rukavishnikov GV, Verbitskaya EV, Vekovischeva OY, Bobrovsky AV, Kibitov AO, Mazo GE (2021) The association of obesity with eating disorders risk: online survey of a large cohort of Russian-speaking individuals seeking medical weight correction assistance. J Eat Disord 9(1):100. https://doi.org/10.1186/s40337-021-00456-y
Lynch W, Eppers K, Sherrodd J (2004) Eating attitudes of Native American and white female adolescents: a comparison of BMI- and age-matched groups. Ethn Health 9(3):253–266. https://doi.org/10.1080/1355785042000250094
Neumark-Sztainer D, Wall M, Larson NI, Eisenberg ME, Loth K (2011) Dieting and disordered eating behaviors from adolescence to young adulthood: findings from a 10-year longitudinal study. J Am Diet Assoc 111(7):1004–1011. https://doi.org/10.1016/j.jada.2011.04.012
Cheah WL, Hazmi H, Chang CT (2017) Disordered eating and body image issues and their associated factors among adolescents in urban secondary schools in Sarawak, Malaysia. Int J Adolesc Med Health. https://doi.org/10.1515/ijamh-2015-0044
Nagata JM, Garber AK, Tabler JL, Murray SB, Bibbins-Domingo K (2018) Prevalence and correlates of disordered eating behaviors among young adults with overweight or obesity. J Gen Intern Med 33(8):1337–1343. https://doi.org/10.1007/s11606-018-4465-z
Al-Kloub MI, Al-Khawaldeh OA, M AL, Batiha AM, Al-Haliq M (2019) Disordered eating in Jordanian adolescents. Int J Nurs Pract 25(1):e12694. https://doi.org/10.1111/ijn.12694
Harrison AN, James Bateman CCB, Younger-Coleman NOM, Williams MC, Rocke KD, Clato-Day Scarlett SC et al (2020) Disordered eating behaviours and attitudes among adolescents in a middle-income country. Eat Weight Disord 25(6):1727–1737. https://doi.org/10.1007/s40519-019-00814-5
Sanlier N, Yassibas E, Bilici S, Sahin G, Celik B (2016) Does the rise in eating disorders lead to increasing risk of orthorexia nervosa? Correlations with gender, education, and body mass index. Ecol Food Nutr 55(3):266–278. https://doi.org/10.1080/03670244.2016.1150276
Yilmaz Z, Gottfredson NC, Zerwas SC, Bulik CM, Micali N (2019) Developmental premorbid body mass index trajectories of adolescents with eating disorders in a longitudinal population cohort. J Am Acad Child Adolesc Psychiatry 58(2):191–199. https://doi.org/10.1016/j.jaac.2018.11.008
Szweda S, Thorne P (2002) The prevalence of eating disorders in female health care students. Occup Med (Lond) 52(3):113–119. https://doi.org/10.1093/occmed/52.3.113
Mond JM, Hay PJ, Rodgers B, Owen C, Beumont PJ (2004) Validity of the eating disorder examination questionnaire (EDE-Q) in screening for eating disorders in community samples. Behav Res Ther 42(5):551–567. https://doi.org/10.1016/s0005-7967(03)00161-x
Vetrone G, Cuzzolaro M, Antonozzi I, Garfinkel PE (2006) Screening for eating disorders: false negatives and eating disorders not otherwise specified. Eur J psychiatry 20(1):13–20
Fichter MM, Elton M, Sourdi L, Weyerer S, Koptagel-Ilal G (1988) Anorexia nervosa in Greek and Turkish adolescents. Eur Arch Psychiatry Neurol Sci 237(4):200–208. https://doi.org/10.1007/bf00449908
Van Strien T, Frijters JE, Bergers GP, Defares PB (1986) The Dutch Eating Behavior Questionnaire (DEBQ) for assessment of restrained, emotional, and external eating behavior. Int J Eat Disord 5(2):295–315
Roncero M, Barrada JR, Perpiñá C (2017) Measuring orthorexia nervosa: psychometric limitations of the ORTO-15. Span J Psychol 20:E41. https://doi.org/10.1017/sjp.2017.36
Garner DM, Garfinkel PE (1979) The eating attitudes test: an index of the symptoms of anorexia nervosa. Psychol Med 9(2):273–279. https://doi.org/10.1017/s0033291700030762
Fairburn CG, Beglin SJ (2008) Eating Disorder Examination Questionnaire (6.0). In: Fairburn CG (ed) Cognitive behavior therapy and eating disorders. Guilford Press, New York
Fichter MM, Keeser W (1980) Das anorexia-nervosa-inventar zur selbstbeurteilung (ANIS). Arch Psychiatr Nervenkr 228(1):67–89. https://doi.org/10.1007/BF00365746
Donini LM, Marsili D, Graziani M, Imbriale M, Cannella C (2004) Orthorexia nervosa: a preliminary study with a proposal for diagnosis and an attempt to measure the dimension of the phenomenon. Eat Weight Disord-Stud Anorex Bulim Obes 9(2):151–157
Rosenvinge JH, Perry JA, Bjørgum L, Bergersen TD, Silvera DH, Holte A (2001) A new instrument measuring disturbed eating patterns in community populations: development and initial validation of a five-item scale (EDS-5). Eur Eat Disord Rev: Prof J Eat Disord Assoc 9(2):123–132
Garner DM, Olmsted MP, Polivy J (1983) The eating disorder inventory: a measure of cognitive-behavioral dimensions of anorexia nervosa and bulimia. Anorex Nerv Recent Dev Res 3:173–184
Heiss S, Coffino JA, Hormes JM (2019) What does the ORTO-15 measure? Assessing the construct validity of a common orthorexia nervosa questionnaire in a meat avoiding sample. Appetite 135:93–99
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Human and animal rights
This article does not contain any studies with human participants or animals performed by any of the authors. Data were obtained from published studies available in the public domain.
Informed consent
For this type of study (systematic review and meta-analysis) formal consent is not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Fekih-Romdhane, F., Daher-Nashif, S., Alhuwailah, A.H. et al. The prevalence of feeding and eating disorders symptomology in medical students: an updated systematic review, meta-analysis, and meta-regression. Eat Weight Disord 27, 1991–2010 (2022). https://doi.org/10.1007/s40519-021-01351-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40519-021-01351-w