
Abstract
Background
The effect of psychopathology on swallowing ability tends to be an overlooked issue in the assessment of dysphagic patients, possibly overshadowed by the given prominence to organic pathologies and the difficulties on the management of these patients. In addition, it should also be kept in mind that a great number of psychotropic drugs can affect swallowing adding problematic clinical issues in this area. Despite this, assessment of dysphagia should be considered as an extremely important issue, due to its impact on basic symptomatology, course of illness and quality of life.
Objective
This review aims to be an overview of relevant data on psychopathology associated with dysphagia and impairment of swallowing function.
Materials and methods
An extensive bibliographic search was carried out in different medical databases (PubMed and Psycharticles) to comprehensively identify the most relevant publications available on dysphagia in eating disorders published until December 2020, according to the PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analysis) method. Research articles, either theoretical or empirical-based, published in peer-reviewed journals and in English language, were included. Case reports were also considered in the analysis when it was appropriate for completeness purposes. Titles and abstracts were reviewed according to the eligibility criteria.
Results
In total, 260 published studies were identified and 40 were finally selected after removal of duplicates and relevance. Primarily we investigated the correlation between dysphagia and eating disorders, analysing the complex relationship between the two conditions. Then we provided an overview of the assessment of dysphagic symptoms in other psychiatric syndromes.
Limits
No exclusion criteria or statistical methods were applied nor was an assessment of study-level or outcome-level bias applicable for our purpose. The topic is vast and research bias could not be excluded; moreover, data available are heterogeneous and lacking systematic approach.
Conclusions
With this review, the authors want to provide an overview of the most considerable and clinically useful information about the topic, focusing on some key points to disentangle psychiatric components from the complexity of patient with dysphagia. It should be a relevant concern for all clinicians and should be always thoroughly assessed, considered its frequency in clinical practice and its implications in every kind of patients’ morbidity, mortality and quality of life. Special attention should be paid to mentally ill patients, who might display complex and multiple comorbidities, as well as consequences of abnormal eating behaviours, occasionally exacerbated by psychotropic medications. More systematic studies are needed, while it seems clear that a multidisciplinary approach is pivotal in the assessment and management of dysphagic patients.
Level of evidence
Level I (evidence obtained from at least one properly designed randomized controlled trials; systematic reviews and meta-analyses; experimental studies).
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Deglutition is essential for natural nourishment. Dysphagia and difficulty in swallowing are frequent symptoms found in clinical practice. Practitioners often struggle in identifying its etiopathological genesis as it can be the expression of a large number of different nosographic categories. Basic aetiology of dysphagia may be simplified as mechanical/obstructive or neurological/muscular and prevalence varies in different age groups. Furthermore, it could be classified based on the location of oral/pharyngeal or oesophageal phase impairment [1]. Identifying functional origin of swallowing disorders seems to be one of the most difficult challenges, frequently leading to invasive and as expensive as unnecessary diagnostic procedures involving many different consultants.
There seems to be a mutual relationship between dysphagia and psychiatric disorders. Many different organic diseases can certainly cause swallowing impairment, but it must be considered that it can also be worsened by psychiatric comorbidities, like affective or anxious disorders, which in turn negatively influence outcomes and prognosis. Finally, these kinds of symptoms can also be exclusively expressions of various psychiatric disorders which can be distinguished one from another in relation to different psychopathological processes at the origin. Even though this distinction can look sophisticated and specific, it can be useful to recognize focal points to plan an adequate treatment and obtain resolution or significative reduction of symptoms. Research in this area is limited and heterogeneous and the link between these distinct components is far from being clear [2]. It is likely that alterations of some neuronal circuits in common (cingulate cortex, amygdala, basal ganglia) could lead to both psychopathological and functional symptomatic expressions. Data emerging from the literature show that affective symptoms are very frequent in patients suffering from dysphagia [3,4,5,6,7]. Within this framework, it is also possible that the individual’s affective state could amplify his own perceptions, contributing to a wrong cognitive experience of the swallowing act.
In this review, we would like to reappraise and discuss the relationship between dysphagia and psychopathology, trying to provide a useful overview for specialists in different disciplines. Since specific guidelines are lacking, deeper knowledge of the topic can help practitioners disentangle complex pathological manifestations.
Methods
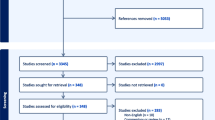
In this systematic review, the authors undertake a thorough analysis of recent literature on the topic. The PubMed and Psycharticles electronic databases were searched for literature published until December 2020, to comprehensively identify the most relevant publications available on dysphagia in eating disorders, according to the PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analysis) method [8]. Sequential combinations of the search terms “dysphagia OR swallowing disorder” and “anorexia nervosa”, “eating disorders” “avoidant/restrictive food intake disorder”, “bulimia nervosa”, “binge eating disorder”, “pica”, “rumination disorder” were used. Research articles, either theoretical or empirical-based, published in peer-reviewed journals and in English language, were included. Case reports were also considered in the analysis when it was appropriate for completeness purposes. Finally, the most relevant references were examined to obtain further important publications that may supplement the discussion. In total 260 studies were identified and 206 were screened after the removal of duplicates. The majority (167) were excluded bond on relevance or abstract or title content. Forty studies were finally included. No exclusion criteria or statistical methods were applied nor was an assessment of study-level or outcome-level bias applicable for our purpose. Once systematically investigated the correlation between dysphagia and eating disorders, we summarized the relationship with other many psychiatric disorders, briefly describing their etiopathological and psychopathological features for differential diagnosis, patients’ management suggestions and treatment options (Fig. 1).

“Dysphagia and eating disorders” research flow diagram
This review represents an effort to approach such an interdisciplinary and poorly understood topic, trying to systematize an overview of the most considerable and clinically useful information.
Discussion
Dysphagia and eating disorders
The relationship between swallowing disorders and eating disorders is only apparently straightforward. Patients who suffer from eating disorders act dysfunctional eating behaviours, like restrictive, binge eating or purging conducts, consequently to dysmorphophobia: it is the expression of a disturbance in the way in which one’s body weight or shape is experienced [9, 10]. These patients fear the consequences of nutrition, as gaining weight or changing body shape. These features are absent in avoidant restrictive food Intake disorder [11] or in selective eating often found in patients with autistic spectrum disorder [12], which must be considered as a differential diagnosis during the initial assessment.
Patients suffering from eating disorders often complain about gastrointestinal and oesophageal symptoms to justify the avoidance of food intake, leading to unnecessary invasive and expensive further investigations and interfering with rehabilitation programmes [13, 14]. According to a recent review of the literature, most gastrointestinal symptoms reported seem to meet criteria for functional disorders, while structural, immunological disorders or food intolerances showed prevalence rates comparable to general population. In the studies considered, functional oesophageal disorders, like dysphagia, functional heartburn and retrosternal pain, displayed a prevalence rate of 23–51% in patients with eating disorders [15, 16]. Correlations among these symptoms, underweight, restrictive/binging behaviours or psychological traits were not found [15,16,17]. They seem to be characterized by marked instability and high turn-over, with prevalent persistence in a 12-month follow-up [17]. Another Italian study failed in finding a correlation between the improvement of oesophageal symptoms and psychopathological distress scores after treatment [13]. Furthermore, many symptoms, included dysphagia, showed different improving responses after weight rehabilitation in various studies [13, 16]. Hence, it is still difficult to assume predictive or causal factors for functional gastrointestinal symptoms onset in eating disorders [15].
Moreover, it should be kept in mind that gastrointestinal symptoms may represent the expression of severe organic complications [14, 18]. Weight loss experienced by patients who suffer from Anorexia Nervosa (AN) could lead to severe swallowing muscle hyposthenia which may or may not be associated with chronic gastrointestinal reflux and gastrointestinal muscle atrophy caused by self-induced vomit [18]. Oropharyngeal dysphagia seems to be related to lower BMI in more compromised patients, as the result of the severe underweight status, and longer length of hospitalization [18]. In a recent case report, a case of oesophageal dysphagia due to oesophageal ulcers probably induced by autophagic mechanisms secondary to starvation and malnutrition is described [19].
Studies describing swallowing difficulties in AN with instrumental examinations are lacking. Though several alterations are found in severe stages of the disease as a likely consequence of physical decay, these seem not to be frequent in early stages, when it could be hypothesized that psychological factors play a pivotal role. Unfortunately, few studies are found, with several limitations and small sample sizes, so it is difficult to characterize the swallowing process in patients with AN [20].
Unfortunately, literature is scarce when other eating disorders are considered. Gastrointestinal symptoms are frequent in patients suffering from Bulimia Nervosa (BN) and are often misdiagnosed or misinterpreted. Only an older study carried out in 1989 considered characteristics of oral motor and swallowing function in BN, finding some abnormalities in a limited group of patients (absence of pharyngeal and velar gag reflex, inhibition of tactile pharyngeal stimulation, mucosal structural and sensitive alterations, abnormal oesophageal motor patterns) [21]. Delayed gastric emptying and impaired contractile antrum function seem to be quite frequent in BN. Their aetiology is not clear, and the literature is lacking, but some authors hypothesized muscular atrophy and electrolytes imbalance resulting from self-induced vomit as possible causes [22]. Frequent acid exposure of the upper gastrointestinal tract due to recurrent induced vomiting could lead to swallowing impairment and severe complications as oesophageal irritation, esophagitis, oesophageal strictures, Barrett’s oesophagus and adenocarcinoma [23, 24], even though the association between BM and gastroesophageal reflux is controversial [25].
Finally, it could be reasonable to consider an individualized approach to refractory symptoms in patients with eating disorders [24].
Patients diagnosed with Binge Eating Disorder (BED) could complain of upper and lower gastrointestinal symptoms. According to data resulting from a study by Cremonini et al., BED could lead to gastrointestinal morbidity. Acid reflux could be the condition underlying dysphagic symptoms, but according to available data, the relationship between gastrointestinal symptoms and BED has still to be cleared [26].
For completeness, few cases are described of sudden dysphagia developed after ingestion of foreign bodies due to Pica, a rare eating disorder consisting in eating non-nutritive or non-food substances inappropriately to developmental level or cultural believes [9] that could reveal itself as a possible consequence of iron deficiency [27, 28].
Literature offers many examples, mainly through case reports, of primary oesophageal dysmotility disorders misdiagnosed as eating disorders [29,30,31,32,33,34,35,36,37,38]. An organic condition showing significant symptomatic overlap seems to be achalasia [39]. Achalasia is a rare oesophageal motor disorder with unknown aetiology, often starting with dysphagia and many other upper gastrointestinal symptoms. It is characterized by altered oesophageal peristalsis and increased/normal resting pressure of the lower oesophageal sphincter without complete relaxation during swallowing [39]. This condition shares numerous physical, behavioural and psychological features with eating disorders, leading to delayed diagnosis and treatment [39, 40]. It should be considered primarily in case of atypical presentation of the disorder, like the absence of imperative drive to lose weight or body image distortion as well as uncontrollable vomiting (during sleep), regurgitation of non-digested food, frequent and persistent swallowing difficulties occurring after liquid intake, at night or in public, stereotyped behaviours during meals, history of aspiration pneumonia [39] or change in symptoms characteristics, frequency and severity [41, 42]. There are many case reports of patients of different ages initially diagnosed with AN and finally identified as suffering from achalasia after a specific diagnostic assessment. Oesophageal manometry represents a “gold standard” [39]. Some authors stated that eating disorders could represent a risk factor for achalasia through decreased gastric motility and myenteric plexus damage due to recurrent vomiting [41]. Differential diagnosis could be challenging, above all in prepuberal age children, always considering that a comorbidity between the two conditions could always be possible [29,30,31,32,33,34,35,36,37,38,39, 41, 43]. Only a case report was found about the misdiagnosis of juvenile Alexander Disease, a rare sporadic leukoencephalopathy that can mimic AN in the early stages [44].
Since distinguishing between the conditions described could be challenging, a standardized assessment approach could be recommended, aiming to select only the more severely ill patients that really need invasive diagnostic exams and, at the same time, to avoid a superficial management [45]. The diagnostic approach to patients with eating disorders complaining gastrointestinal symptoms should be guided primarily by clinical history (onset of symptoms, history of purging or restrictive behaviours, kind of food selected) and by the quality of symptoms, while a general screening for some disturbances, such as irritable bowel syndrome, celiac disease, food allergies or intolerances, cannot be recommended according to available current literature [16]. Only more severely ill patients should be screened for signs and symptoms of oropharyngeal dysphagia, like the incidence of previous aspiration pneumonia episodes, coughing or choking with food and liquid or complaints about difficulty in swallowing, trying to identify patients at high risk of aspiration. A speech-language pathologist evaluation could be useful and, if needed, patients could be addressed to a more in-depth examination through additional instrumental tests to detect functional or structural abnormalities in oropharyngeal or oesophageal swallowing phase. For this aim, a cluster of standardized questions could be an advantageous tool. In patients suffering from oropharyngeal dysphagia, traditional swallowing therapy may help to improve nutritional and hydration status and reduce the risk of aspiration [18, 46, 47].
Differential diagnosis
Dysphagia and anxiety disorders
Dysphagia or swallowing difficulties can be found in Post-traumatic Stress Disorder or Anxiety Disorders, such as Panic Disorder, Social Phobia or Specific Phobia. Although these symptoms are not the most frequently reported, they revealed a remarkable rate: some studies found that swallowing complaints occurred nearly in 40% of patients suffering from Panic Disorder, with little differences between females and men [48,49,50]. Anxiety or intense fear arising when the patient is exposed to the phobic object (i.e. social situation in which the subject is exposed to others’ judgment, a situation that caused vomit/suffocation) is the common element among all these psychopathological categories [51]. Some authors define this set of symptoms as “swallowing anxiety” and recognize them as a potential worsening factor, since it leads to inconsistency in drug use, negatively affecting patients’ functionality and heightening the risk of relapses [52]. The common behavioural response consists in avoiding the phobic object or situation (“phagophobia”): the subjects develop symptoms that imitate oral apraxia with intact pharyngoesophageal, neurologic functions and linguistic abilities [53, 54]. Deglutition-related traumatic experiences seem to have a correlation with phagophobia, which may also be associated to panic disorder, obsessive compulsive disorder and separation anxiety symptoms [52]. It seems also to share some characteristics and similar comorbidities with functional dysphagia, a psychologically based swallowing problem not associated with clinically relevant fear and anxiety symptoms, and globus pharyngeus [52]. Some authors found such a strong relationship between the two syndromes, that they defined them as parts of a psychopathological continuum [51]. Intensity of anxious symptoms can condition the type of food they avoid, and, in some cases, cause severe consequences on both the organic (weight loss, metabolic ad hydro-electrolytic alterations) and psychosocial side (social withdrawal, depression, anxiety and panic attacks) becoming extremely difficult to treat [7, 52, 55].
Unfortunately, this condition has not been extensively evaluated and data often is limited to case reports and affected by the heterogeneity of the definitions used. Thus, is not possible to describe a univocal evidence-based treatment strategy. Cognitive-Behavioural Therapy seems to be a common useful treatment approach. It is combined in many cases with other techniques (psychoeducation, exposure therapy, muscle relaxation, group therapy, hypnosis, Eye Movement Desensitization and Reprocessing—EMDR) and pharmacological treatment. This one seems confined to antidepressants and benzodiazepines [53].
Dysphagia and functional disorders
Functional Neurologic Disorders (DSM 5) [9] or Conversion Disorder shows a great impact on clinical practice. It consists of sensitive or motor symptoms, usually under voluntary control, that are not explained by any neurological syndrome and lead to significant impairment of individual’s global functioning. They are classified as “Somatic Symptoms and Related Disorders” and it can be specified if it shows “with swallowing symptoms” [9]. Functional dysphagia is, in the end, defined by Roma III criteria for gastroenterological functional symptoms [56]. Three symptoms during at least three of the six months preceding diagnosis must be present: feeling of difficulty in bolus pharyngo-oesophageal transit, no evidence of previous gastroesophageal reflux disease, no histopathological evidence of oesophagus motility disease. “Globus pharyngis” or “globus hystericus” is a subjective feeling of a lump or foreign body in the throat when one attempts to swallow [52]. Patients use to describe their feeling as a lump, foreign body, “ball-like”, “hair”, itching, swelling, scratching sensation in the throat and is often followed by pharyngeal irritation symptoms, like throat cleaning and chronic cough [57, 58]. Classically it improves with eating and it is not associated with odynophagia or dysphagia [59]. It seems to be related to a multifactorial aetiology and some studies found a correlation with psychological distress, especially anxiety and depression. Mostly it is a benign disorder, even though it is long-lasting, recurrent and difficult to treat. That’s why explanation and reassurance are pivotal in patients’ management. The nosographic translation from “hysteria/psychogenic disorder” (DSM, DSM II) to “functional disorder” [9] reflects the focus transition from a psychologic aetiology to a bio-psycho-social interpretation model [60,61,62], other than appearing more suitable for a medical context [63]. It is important to point out that conversion disorder should not be an exclusion diagnosis, but a result of a multidisciplinary diagnostic-therapeutic process. Patients often show high levels of frustration because specialists remain sceptical towards them and sometimes they take into account “simulation” of symptoms. Identifying this population has important implications on clinical practice, as it is one of the most frequent conditions observed by neurologists [63, 64]. This population often shows the same discomfort and subjective disability as patients who suffer from neurological diseases. Second, they present higher levels of unemployment and use more disability-related state financial benefits than neurological population [65]. They have often psychiatric comorbidities (like Anxiety Disorders, Panic Disorder, Depression, Obsessive–Compulsive Disorder, Eating Disorders, Post-traumatic Stress Disorder) that condition each other and show common risk factors (adverse experience in infancy and stressful life events, among others). There is not enough knowledge about the pathophysiological mechanisms of these functional disturbances [57]. There are not even evidence-based guidelines on this topic. Treatment should be personalized and based on a good risk–benefit assessment [66]. Primarily, specialists should recognize cases at high risk of malignancies, focusing their attention on symptoms which need further evaluation (dysphagia, odynophagia, throat pain, lateralization, weight loss), reflux symptoms or psychological distress. A clinical evaluation of the neck should follow. The use of instrumental evaluation routinely is controversial since most patients do not need further investigations. An empirical Proton-Pump Inhibitors treatment could be a useful strategy to save instrumental examinations to non-responders. In case of negative clinical investigations and persistence of bolus sensation patients could be addressed to speech therapy, cognitive–behavioural therapy or treatment with antidepressants [59]. One of the essential elements of an efficient management is the foundation of a solid therapeutic alliance, starting from an extensive anamnestic record. It may lead to a reduction of “doctor shopping” practice, costs and risks of invasive diagnostic procedures. Clinicians should guide patients to understand symptoms and, if it is not possible, to act interpersonal/behavioural strategies [67], even with the help of caregivers.
Dysphagia and psychotic disorders
Swallowing disorders are frequent in patients suffering from schizophrenia and other psychotic disorders. Since they show higher morbidity than general population and patients suffering from other psychiatric illnesses [68,69,70], at least an organic cause should be taken into consideration. Many types of dysphagia have been recognized in psychiatric patients, even though they often coexist in clinical practice, so a clear distinction might be difficult [71]. Two main aetiologic categories are found: antipsychotic treatments collateral effects (first extrapyramidal effects, even if sialorrhea and xerostomia play a significant role) and abnormal behaviours that may occur during a psychotic illness (e.g., PICA, fast-eating syndrome). Dysphagia and swallowing abnormalities can also be associated with low concentration and distractibility during meals [72]. Furthermore, in some cases, the hypothesis that dysphagic symptoms are part of a delusion of control or a somatic passivity phenomenon cannot be excluded [73]. Dysphagia could lead to malnutrition, aspiration and cause choking deaths more frequently in schizophrenia and organic psychotic illnesses, even independently to medication [74]. The fact that psychiatric patients could have low cognition of these problems and could show difficulties in expressing their distress adds more complexity to assessment and management [71]. There are no systematic studies focused on this condition, almost all publications found on the topic agreed about the necessity of a systematic approach to diagnosis through a multidimensional and multidisciplinary team to understand the nature of dysphagic symptoms in psychotic patients. The same is applied to treatment attitude, which includes adjustment of pharmacological therapy, avoiding medications that could worsen symptoms when possible, caregivers education and monitoring during meals, dietary modification, long-term speech (logopaedic) rehabilitation, screening for proper oral health to avoid edentulism [71, 75, 76]. This can lead to the development of active and passive strategies to reduce the incidence of aspiration episodes [72].
Dysphagia and psychotropic medications
A substantial number of patients suffering from dysphagia are taking psychotropic drugs according to the literature [77]; thus, it is necessary to consider the iatrogenic aetiology as a potential cause of the disorder [78]. Attention has been addressed to this theme since the second half of the last century [79] and has grown after the FDA warning published in 2005 (http://www.fda.gov/cder/drug/advisory/antipsychotics.htm) in relation to high number of patient deaths by pneumonia among those treated with neuroleptic drugs (haloperidol, chlorpromazine, perphenazine and others). In particular, elderly patients and patients with cognitive impairment seem to present the highest risk [1]. Neuroleptic drugs are not the only psychotropic category associated with risk of dysphagia: antiepileptic, anticholinergic drugs and benzodiazepines [1], which are frequently added to neuroleptic drugs in most severely ill patients [80], can also cause dysphagia adding further choking/aspiration risk, although their mechanism of action at the level of central nervous system is not clear [78]. The iatrogenic origin of dysphagia could be an effect directly derived from agents’ mechanism of action or their secondary side effect [78]. They can directly impair both deglutition phases, but also cause alterations of the state of consciousness, of the oesophageal motility and a reduction of the cough reflex probably via both sensory (afferent) and motor (efferent) components. Furthermore, side effects of antipsychotic drugs, because of their dopamine and histamine effects, such as parkinsonism, acute dystonic reactions and tardive dyskinesia, including their significant role in inducing hypersalivation, sedation and xerostomia, can lead to dysphagia episodes and severe consequences like choking and pneumonia. For an exhaustive overview of mechanisms and consequences of drug-induced dysphagia see Cicala et al. [1]. A systematic review regarding 18 studies published by Miarons Font and Rofes Salsench [77] shows that antipsychotic drugs that are associated with higher dysphagia incidence were haloperidol among first-generation antipsychotics (followed by thioridazine hydrochloride, sulpiride, chlorpromazine) and risperidone among second-generation antipsychotics (followed by clozapine, olanzapine, quetiapine). These data regarding second-generation antipsychotics suggest that dysphagia cannot be simply explained by nigrostriatal effects (extrapyramidal syndrome and tardive dyskinesia) by D2 receptors antagonism. Multiple receptor actions are probably involved: antihistaminergic (with sedation and cough reflex reduction), anticholinergic (xerostomia, impaired bolus transit), catecholaminergic (muscle tone). They all have a great impact on the first two phases of swallowing. Data from this review is discordant and heterogeneous, so more observational studies and randomized clinical trials are necessary. The authors lead to the conclusion that iatrogenic aetiology must be considered for both typical and atypical antipsychotic drugs [77]. Thus, it is particularly problematic to define a causality of drug reactions in patients at high basal risk of swallowing impairment, as elderly people with dementia or intellectual disability [1, 77]. Randomized clinical trials involving newer recently marketed antipsychotics do not include information on the prevalence of these effects, maybe because individuals involved seem to be relatively healthy [1]. Reducing or, when it is possible, discontinuing drugs with the strongest side effects, switching to a different antipsychotic with a more favourable side effects profile or adding anticholinergic drugs, depending on the situation could all be useful strategies to reduce antipsychotics’ impact on deglutition [1]. Providing an adequate caloric intake is pivotal to prevent malnutrition in patients who develop drug-induced dysphagic symptoms. A nutritionist consultation might be useful to elaborate a feeding program adequate to the type and degree of impairment and that fits the nutritional patient’s need, preventing the risk of aspiration at the same time. Nutritional parameters and weight should be regularly checked, and meals supervised. Patients showing severe tardive dyskinesia or parkinsonism should be directly and routinely asked about swallowing difficulties, to prevent late diagnosis due to their difficulty in reporting such symptoms and patient’s medication history should be evaluated to primarily determine the cause of these symptoms [81].
Conclusion
Deglutition is a complex sensorimotor behaviour and its impairment could lead to severe consequences on the organic side. Dysphagia should be a relevant concern for clinicians and should not be overlooked in patients’ assessment, considered its frequency in clinical practice and its implications in patients’ morbidity, mortality and quality of life. Not only psychologists and psychiatrists might show particular interest in this topic, but it also could be useful for all specialists outside mental health, considering the overlap between organic and psychopathologic symptomatology. It is generally difficult to identify causal or predictive factors for gastrointestinal manifestations in eating disorders; thus, studies involving imaging or instrumental examinations are lacking at any phase of the disease course. Therefore, swallowing impairment in other mental disorders is less documented, but still common (see Table 1).
Special attention should be paid to mentally ill patients, who might display complex and multiple comorbidities with additional choking risk factors such as poor eating habits, impaired dentition, comorbid neurological diseases [1], as well as consequences of abnormal eating behaviours, occasionally exacerbated by psychotropic medications. Furthermore, psychiatric comorbidity is a potential contributing factor to swallowing symptoms, which has an established negative impact on course, management and compliance to treatment of organic diseases. The literature concerning this topic is scanty, generally recent and lacking in international guidelines. Despite this, published knowledge agreed on the need of multidisciplinary management of patients displaying swallowing disorders, from the diagnostic assessment to the implementation of treatment and rehabilitation strategies.
It should be important to proceed with a detailed study of swallowing symptoms with more clinical trials, to better understand the aetiopathogenesis of functional manifestations, avoiding direct and indirect management costs, and clear the role of psychopathological manifestation as well as psychopharmacotherapy, especially in high-risk populations.
What is already known on this subject?
Dysphagia is a condition frequently detected in clinical practice, whose diagnostic assessment and treatment management often involve several consultants. Identifying the aetiology of swallowing disorders is indeed challenging, due to the complexity of potentially involved causal processes, including psychopathology. Increasing awareness on the topic might have many implications in resource management, clinical outcomes, and impact on patients’ quality of life.
What does this study add?
This review aimed at providing a systematic overview of psychopathology associated with dysphagia for all consultants, especially outside mental health. It might help enlightening some usually overlooked issues, clarifying some key points, and underlying the importance of a multidisciplinary approach finally entailing an optimization of patients’ management.
Strengths and limits
The main strength of this review is its purpose to systematize the heterogeneous and fragmented data on psychopathological implications of dysphagia, trying to provide some key points, which might be useful in clinical practice.
Some limitations are related to the heterogeneity of available data itself, mainly lacking in systematic approach or recent clinical studies. The topic is vast and research bias could not be excluded. It is hoped that further studies would help to deepen what already emerged from this review. It would be especially interesting to clarify mechanisms underlying dysphagic symptoms in eating disorders through more clinical studies involving instrumental as well as psychometric evaluations.
References
Cicala G, Barbieri MA, Spina E, de Leon J (2019) A comprehensive review of swallowing difficulties and dysphagia associated with antipsychotics in adults. Expert Rev Clin Pharmacol 12(3):219–234. https://doi.org/10.1080/17512433.2019.1577134
Verdonschot RJCG, Baijens LWJ, Vanbelle S, van de Kolk I, Kremer B, Leue C (2017) Affective symptoms in patients with oropharyngeal dysphagia: a systematic review. J Psychosom Res 97:102–110. https://doi.org/10.1016/j.jpsychores.2017.04.006
Manor Y, Balas M, Giladi N, Mootanah R, Cohen JT (2009) Anxiety, depression and swallowing disorders in patients with Parkinson’s disease. Parkinsonism Relat Disord 15(6):453–456. https://doi.org/10.1016/j.parkreldis.2008.11.005
Nguyen NP, Frank C, Moltz CC, Vos P, Smith HJ, Karlsson U et al (2005) Impact of dysphagia on quality of life after treatment of head-and-neck cancer. Int J Radiat Oncol Biol Phys 61(3):772–778. https://doi.org/10.1016/j.ijrobp.2004.06.017
Verdonschot RJ, Baijens LW, Serroyen JL, Leue C, Kremer B (2013) Symptoms of anxiety and depression assessed with the Hospital Anxiety and Depression Scale in patients with oropharyngeal dysphagia. J Psychosom Res 75(5):451–455. https://doi.org/10.1016/j.jpsychores.2013.08.021
Verdonschot RJ, Baijens L, Vanbelle S, Florie M, Kremer B, Leue C (2016) The relationship between fiberoptic endoscopic evaluation of swallowing outcome and symptoms of anxiety and depression in dysphagic patients. Laryngoscope 126(5):E199–E207. https://doi.org/10.1002/lary.25698
Verdonschot RJCG, Baijens LWJ, Vanbelle S, Florie M, Dijkman R, Leeters IPM, Kremer B, Leue C (2019) Medically unexplained oropharyngeal dysphagia at the University Hospital ENT Outpatient Clinic for dysphagia: a cross-sectional cohort study. Dysphagia 34(1):43–51. https://doi.org/10.1007/s00455-018-9912-9
Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 6(7):e1000097. https://doi.org/10.1371/journal.pmed.1000097
APA (American Psychiatric Association), (2013) Diagnostic and statistical manual of mental disorders, 5th edn. American Psychiatric Association, Arlington
Shapiro J, Franko DL, Gagne A (1997) Phagophobia: a form of psychogenic dysphagia. A new entity. Ann Otol Rhinol Laryngol 106(4):286–290. https://doi.org/10.1177/000348949710600404
Nakai Y, Nin K, Noma S, Hamagaki S, Takagi R, Teramukai S, Wonderlich SA (2017) Clinical presentation and outcome of avoidant/restrictive food intake disorder in a Japanese sample. Eat Behav 24:49–53. https://doi.org/10.1016/j.eatbeh.2016.12.004
Nicholls D, Bryant-Waugh R (2008) Eating disorders of infancy and childhood: definition, symptomatology, epidemiology, and comorbidity. Child Adolesc Psychiatr Clin N Am 18(1):17–30. https://doi.org/10.1016/j.chc.2008.07.008
Benini L, Todesco T, Frulloni L, Dalle Grave R, Campagnola P, Agugiaro F, Cusumano CD, Gabbrielli A, Vantini I (2010) Esophageal motility and symptoms in restricting and binge-eating/purging anorexia. Dig Liver Dis 42(11):767–772. https://doi.org/10.1016/j.dld.2010.03.018
Malczyk Ż, Oświęcimska JM (2017) Gastrointestinal complications and refeeding guidelines in patients with anorexia nervosa. Psychiatr Pol 51(2):219–229. https://doi.org/10.12740/PP/65274
Boyd C, Abraham S, Kellow J (2005) Psychological features are important predictors of functional gastrointestinal disorders in patients with eating disorders. Scand J Gastroenterol 40(8):929–935. https://doi.org/10.1080/00365520510015836
Kress IU, Paslakis G, Erim Y (2018) Differential diagnoses of food-related gastrointestinal symptoms in patients with anorexia nervosa and bulimia nervosa: a review of literature. Z Psychosom Med Psychother 64(1):4–15. https://doi.org/10.13109/zptm.2018.64.1.4
Boyd C, Abraham S, Kellow J (2010) Appearance and disappearance of functional gastrointestinal disorders in patients with eating disorders. Neurogastroenterol Motil 22(12):1279–1283. https://doi.org/10.1111/j.1365-2982.2010.01576.x
Holmes SR, Sabel AL, Gaudiani JL, Gudridge T, Brinton JT, Mehler PS (2016) Prevalence and management of oropharyngeal dysphagia in patients with severe anorexia nervosa: a large retrospective review. Int J Eat Disord 49(2):159–166. https://doi.org/10.1002/eat.22441
Masaki S, Watanabe T, Minaga K, Kamata K, Komeda Y, Kimura M, Kudo M (2020) Possible involvement of autophagy in esophageal ulcers in anorexia nervosa. Clin J Gastroenterol 13(4):473–476. https://doi.org/10.1007/s12328-019-01089-0
Santos CM, Cassiani RA, Dantas RO (2016) Videofluoroscopic evaluation of swallows in anorexia nervosa. Arq Gastroenterol 53(3):136–140. https://doi.org/10.1590/S0004-28032016000300003
Roberts MW, Tylenda CA, Sonies BC, Elin RJ (1989) Dysphagia in bulimia nervosa. Dysphagia 4(2):106–111. https://doi.org/10.1007/BF02407154
Kiss A, Bergmann H, Abatzi TA, Schneider C, Wiesnagrotzki S, Höbart J, Steiner-Mittelbach G, Gaupmann G, Kugi A, Stacher-Janotta G et al (1990) Oesophageal and gastric motor activity in patients with bulimia nervosa. Gut 31(3):259–265. https://doi.org/10.1136/gut.31.3.259
Brown CA, Mehler PS (2013) Medical complications of self-induced vomiting. Eat Disord 21(4):287–294. https://doi.org/10.1080/10640266.2013.797317
Sachs K, Mehler PS (2016) Medical complications of bulimia nervosa and their treatments. Eat Weight Disord 21(1):13–18. https://doi.org/10.1007/s40519-015-0201-4
Denholm M, Jankowski J (2011) Gastroesophageal reflux disease and bulimia nervosa—a review of the literature. Dis Esophagus 24(2):79–85. https://doi.org/10.1111/j.1442-2050.2010.01096.x
Cremonini F, Camilleri M, Clark MM, Beebe TJ, Locke GR, Zinsmeister AR, Herrick LM, Talley NJ (2009) Associations among binge eating behavior patterns and gastrointestinal symptoms: a population-based study. Int J Obes (Lond) 33(3):342–353. https://doi.org/10.1038/ijo.2008.272 (Erratum in: Int J Obes (Lond) 2010;34(1):214)
Mihailidou H, Galanakis E, Paspalaki P, Borgia P, Mantzouranis E (2002) Pica and the elephant’s ear. J Child Neurol 17(11):855–856. https://doi.org/10.1177/08830738020170111705
Coleman DL, Greenberg CS, Ries CA (1981) Iron-deficiency anemia and pica for tomato seeds. N Engl J Med 304(14):848. https://doi.org/10.1056/nejm198104023041421
Däbritz J, Domagk D, Monninger M, Foell D (2010) Achalasia mistaken as eating disorders: report of two children and review of the literature. Eur J Gastroenterol Hepatol 22(7):775–778. https://doi.org/10.1097/MEG.0b013e3283325d71
Desseilles M, Fuchs S, Ansseau M, Lopez S, Vinckenbosh E, Andreoli A (2006) Achalasia may mimic anorexia nervosa, compulsive eating disorder, and obesity problems. Psychosomatics 47(3):270–271. https://doi.org/10.1176/appi.psy.47.3.270
Duane PD, Magee TM, Alexander MS, Heatley RV, Losowsky MS (1992) Oesophageal achalasia in adolescent women mistaken for anorexia nervosa. BMJ 305(6844):43. https://doi.org/10.1136/bmj.305.6844.43
Goldsmith PJ, Decadt B (2012) Extreme achalasia presenting as anorexia nervosa. Case Rep Surg 2012:985454. https://doi.org/10.1155/2012/985454PMID:23091768
Kenney RD (1984) Achalasia in an adolescent with behavioral features compatible with anorexia nervosa. J Adolesc Health Care 5(4):283–285. https://doi.org/10.1016/s0197-0070(84)80134-5
Letranchant A, Pigneur B, Flament M, Godart N (2020) Eating disorder or oesophageal achalasia during adolescence: diagnostic difficulties. Eat Weight Disord 25(1):87–90. https://doi.org/10.1007/s40519-018-0513-2
Marshall JB, Russell JL (1993) Achalasia mistakenly diagnosed as eating disorder and prompting prolonged psychiatric hospitalization. South Med J 86(12):1405–1407. https://doi.org/10.1097/00007611-199312000-00019
Richterich A, Brunner R, Resch F (2003) Achalasia mimicking prepubertal anorexia nervosa. Int J Eat Disord 33(3):356–359. https://doi.org/10.1002/eat.10144
Stacher G, Wiesnagrotzki S, Kiss A (1990) Symptoms of achalasia in young women mistaken as indicating primary anorexia nervosa. Dysphagia 5(4):216–219. https://doi.org/10.1007/BF02412690
Wright K, Smith MS, Mitchell J (1990) Organic diseases mimicking atypical eating disorders. Clin Pediatr (Phila) 29(6):325–328. https://doi.org/10.1177/000992289002900606
Reas DL, Zipfel S, Rø Ø (2014) Is it an eating disorder or achalasia or both? A literature review and diagnostic challenges. Eur Eat Disord Rev 22(5):321–330. https://doi.org/10.1002/erv.2307
Hallal C, Kieling CO, Nunes DL, Ferreira CT, Peterson G, Barros SG, Arruda CA, Fraga JC, Goldani HA (2012) Diagnosis, misdiagnosis, and associated diseases of achalasia in children and adolescents: a twelve-year single center experience. Pediatr Surg Int 28(12):1211–1217. https://doi.org/10.1007/s00383-012-3214-3
Kutuk MO, Guler G, Tufan AE, Toros F, Kaytanli U (2017) Achalasia as a complication of bulimia nervosa: a case report. S Afr J Psychiatr 23:996. https://doi.org/10.4102/sajpsychiatry.v23.996
Mohammed F, Whorwell PJ (2006) Psychological or organic vomiting. Eur J Gastroenterol Hepatol 18(7):781–783. https://doi.org/10.1097/01.meg.0000221851.32663.5b
Teufel M, Lamprecht G, Zipfel S, Schrauth M, Rapps N, Martens U, Gross G (2009) Vomiting and feeling fat—coincidence of achalasia and bulimia nervosa. Int J Eat Disord 42(1):90–92. https://doi.org/10.1002/eat.20582
Franzoni E, Van der Knaap MS, Errani A, Colonnelli MC, Bracceschi R, Malaspina E, Moscano FC, Garone C, Sarajlija J, Zimmerman RA, Salomons GS, Bernardi B (2006) Unusual diagnosis in a child suffering from juvenile Alexander disease: clinical and imaging report. J Child Neurol 21(12):1075–1080. https://doi.org/10.1177/7010.2006.00235
Gaudiani JL, Mehler PS (2016) Rare medical manifestations of severe restricting and purging: “Zebras,” missed diagnoses, and best practices. Int J Eat Disord 49(3):331–344. https://doi.org/10.1002/eat.22475
Holmes SR, Gudridge TA, Gaudiani JL, Mehler PS (2012) Dysphagia in severe anorexia nervosa and potential therapeutic intervention: a case series. Ann Otol Rhinol Laryngol 121(7):449–456. https://doi.org/10.1177/000348941212100705
Holmes SR, Gudridge TA, Gaudiani JL, Mehler PS (2012) Dysphagia in severe anorexia nervosa: a case report. Int J Eat Disord 45(3):463–466. https://doi.org/10.1002/eat.20971
Grant BF, Hasin DS, Stinson FS, Dawson DA, Goldstein RB, Smith S, Huang B, Saha TD (2006) The epidemiology of DSM-IV panic disorder and agoraphobia in the United States: results from the National Epidemiologic Survey on Alcohol and Related Conditions. J Clin Psychiatry 67(3):363–374. https://doi.org/10.4088/jcp.v67n0305
Sawchuk CN, Roy-Byrne P, Noonan C, Craner JR, Goldberg J, Manson S, Buchwald D, AI-SUPERPFP Team (2016) Panic attacks and panic disorder in the American Indian community. J Anxiety Disord. https://doi.org/10.1016/j.janxdis.2016.10.004
Sheikh JI, Leskin GA, Klein DF (2002) Gender differences in panic disorder: findings from the National Comorbidity Survey. Am J Psychiatry 159(1):55–58. https://doi.org/10.1176/appi.ajp.159.1.55
Okada A, Tsukamoto C, Hosogi M, Yamanaka E, Watanabe K, Ootyou K, Morishima T (2007) A study of psycho-pathology and treatment of children with phagophobia. Acta Med Okayama 61(5):261–269. https://doi.org/10.18926/AMO/32896
Budak E, Taymur İ, Önen S, Kanat BB, Akdeniz Ö, Demirci H (2018) Symptoms of swallowing anxiety in panic disorder patients and associated psychopathologic factors. Eat Weight Disord 23(4):487–497. https://doi.org/10.1007/s40519-017-0367-z
Baijens LW, Koetsenruijter K, Pilz W (2013) Diagnosis and treatment of phagophobia: a review. Dysphagia 28(2):260–270. https://doi.org/10.1007/s00455-013-9454-0
Kim TSY, Munshi T, Hussain M (2018) Resolution of severe psychogenic dysphagia with ECT in an elderly patient. Int Psychogeriatr 30(7):1081–1083. https://doi.org/10.1017/S1041610217002502
Sahoo S, Hazari N, Padhy SK (2016) Choking phobia: an uncommon phobic disorder, treated with behavior therapy: a case report and review of the literature. Shanghai Arch Psychiatry 28(6):349–352. https://doi.org/10.11919/j.issn.1002-0829.216055
Drossman DA (2016) Functional gastrointestinal disorders: history, pathophysiology, clinical features, and Rome IV. Gastroenterology 150(6):1262-1279.e2. https://doi.org/10.1053/j.gastro.2016.02.032
Clouse RE, Richter JE, Heading RC, Janssens J, Wilson JA (1999) Functional esophageal disorders. Gut 45(Suppl 2):II31–II36. https://doi.org/10.1136/gut.45.2008.ii31
Harvey PR, Theron BT, Trudgill NJ (2018) Managing a patient with globus pharyngeus. Frontline Gastroenterol 9(3):208–212. https://doi.org/10.1136/flgastro-2017-100844
Lee BE, Kim GH (2012) Globus pharyngeus: a review of its etiology, diagnosis and treatment. World J Gastroenterol 18(20):2462–2471. https://doi.org/10.3748/wjg.v18.i20.2462
Barnett C, Armes J, Smith C (2019) Speech, language and swallowing impairments in functional neurological disorder: a scoping review. Int J Lang Commun Disord 54(3):309–320. https://doi.org/10.1111/1460-6984.12448
Demartini B, D’Agostino A, Gambini O (2016) From conversion disorder (DSM-IV-TR) to functional neurological symptom disorder (DSM-5): when a label changes the perspective for the neurologist, the psychiatrist and the patient. J Neurol Sci 360:55–56. https://doi.org/10.1016/j.jns.2015.11.026
Tsui P, Deptula A, Yuan DY (2017) Conversion disorder, functional neurological symptom disorder, and chronic pain: comorbidity, assessment, and treatment. Curr Pain Headache Rep 21(6):29. https://doi.org/10.1007/s11916-017-0627-7
Eger Aydogmus M (2020) Social stigma towards people with medically unexplained symptoms: the somatic symptom disorder. Psychiatr Q. https://doi.org/10.1007/s11126-019-09704-6
Carson AJ, Brown R, David AS, Duncan R, Edwards MJ, Goldstein LH, Grunewald R, Howlett S, Kanaan R, Mellers J, Nicholson TR, Reuber M, Schrag AE, Stone J, Voon V (2012) UK-FNS. Functional (conversion) neurological symptoms: research since the millennium. J Neurol Neurosurg Psychiatry 83(8):842–850. https://doi.org/10.1136/jnnp-2011-301860
Carson A, Stone J, Hibberd C, Murray G, Duncan R, Coleman R, Warlow C, Roberts R, Pelosi A, Cavanagh J, Matthews K, Goldbeck R, Hansen C, Sharpe M (2011) Disability, distress and unemployment in neurology outpatients with symptoms ‘unexplained by organic disease.’ J Neurol Neurosurg Psychiatry 82(7):810–813. https://doi.org/10.1136/jnnp.2010.220640
Baumann A, Katz PO (2016) Functional disorders of swallowing. Handb Clin Neurol 139:483–488. https://doi.org/10.1016/B978-0-12-801772-2.00039-4
Riehl ME, Kinsinger S, Kahrilas PJ, Pandolfino JE, Keefer L (2015) Role of a health psychologist in the management of functional esophageal complaints. Dis Esophagus 28(5):428–436. https://doi.org/10.1111/dote.12219
Corcoran E, Walsh D (2003) Obstructive asphyxia: a cause of excess mortality in psychiatric patients. Irish J Psychol Med 20:88–90
Regan J, Sowman R, Walsh I (2006) Prevalence of dysphagia in acute and community mental health settings. Dysphagia 21:95–101
Wu WS, Sung KC, Cheng TJ, Lu TH (2015) Associations between chronic diseases and choking deaths among older adults in the USA: a cross-sectional study using multiple cause mortality data from 2009 to 2013. BMJ Open 5:e009464
Tang KT, Hsieh MH (2010) A case of schizophrenia with dysphagia successfully treated by a multidimensional approach. Gen Hosp Psychiatry 32(5):559.e11–3. https://doi.org/10.1016/j.genhosppsych.2010.01.012
Kulkarni DP, Kamath VD, Stewart JT (2017) Swallowing disorders in schizophrenia. Dysphagia 32(4):467–471. https://doi.org/10.1007/s00455-017-9802-6
Baheshree RD, Jonas SS (2012) Dysphagia in a psychotic patient: diagnostic challenges and a systematic management approach. Indian J Psychiatry 54(3):280–282. https://doi.org/10.4103/0019-5545.102464
Ruschena D, Mullen PE, Palmer S, Burgess P, Cordner SM, Drummer OH, Wallace C, Barry-Walsh J (2003) Choking deaths: the role of antipsychotic medication. Br J Psychiatry 183:446–450. https://doi.org/10.1192/bjp.183.5.446
Aquila I, Gratteri S, Sacco MA, Nuzzolese E, Fineschi V, Frati P, Ricci P (2018) Could the screening for correct oral health reduce the impact of death due to bolus asphyxia in adult patients? A forensic case report. Med Hypotheses 110:23–26. https://doi.org/10.1016/j.mehy.2017.10.018
Funayama M, Takata T, Koreki A (2019) Choking incidents among patients with schizophrenia may be associated with severity illness and higher-dose antipsychotics. Gen Hosp Psychiatry 59:73–75. https://doi.org/10.1016/j.genhosppsych.2018.09.001
Miarons Font M, Rofes Salsench L (2017) Antipsychotic medication and oropharyngeal dysphagia: systematic review. Eur J Gastroenterol Hepatol 29:1332–1339
Alonso JSE, Garcia IZ (2019) Drugs and dysphagia. Oropharyngeal Dysphagia. https://doi.org/10.1007/978-3-319-92615-5_8
Feldman PE (1957) An unusual death associated with tranquilizer therapy. Am J Psychiatry 113(11):1032–1033
Craig TJ (1980) Medication use and deaths attributed to asphyxia among psychiatric patients. Am J Psychiatry 137(11):1366–1373. https://doi.org/10.1176/ajp.137.11.1366
Weiden P, Harrigan M (1886) A clinical guide for diagnosing and managing patients with drug-induced dysphagia. Hosp Commun Psychiatry 37(4):396–398. https://doi.org/10.1176/ps.37.4.396
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest to declare that are relevant to the content of this article.
Funding
No funding was received for conducting this study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Massa, L., Fattori, B., Nacci, A. et al. Psychopathological aspects of dysphagia: a systematic review on correlations with eating disorders and other psychiatric conditions. Eat Weight Disord 27, 881–892 (2022). https://doi.org/10.1007/s40519-021-01227-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40519-021-01227-z