
Abstract
Context
Dietary diversity score (DDS) has been known as a useful and convenient indicator of overall diet quality. Previous studies have reported the association between DDS and health problems such as diabetes, metabolic syndrome and cardiovascular disease.
Objectives
This systematic review and meta-analysis aimed to assess the association between dietary diversity score (DDS) and cardio-metabolic risk factors such as obesity and overweight, lipid profile, blood pressure, metabolic syndrome (MetS) and diabetes.
Data sources
We systematically searched PubMed and NLM Gateway, Scopus and Institute of Scientific Information (ISI) by up to October 2019.
Data extraction
All observational studies which assessed the association of DDS with cardio-metabolic risk factors including anthropometric measures, blood pressure, lipid profile, glycemic indices and MetS without limitation in time of publication and language were included and critically reviewed by two independent experts. Random-effects meta-analysis was used to estimate the effect sizes.
Data analysis
Among 843 documents retrieved from literature search, 23 studies met the inclusion criteria for systematic review, and 18 studies were eligible for meta-analysis. Random-effects meta-analysis showed that the association of DDS with obesity, abdominal obesity, overweight, body mass index, MetS, diabetes, blood pressure, and lipid profile (TC, LDL, HDL) was not statistically significant. On the other hand, the association of DDS and TG was statistically significant (SMD: − 0.23, 95% CI − 0.45, − 0.01).
Conclusions
Our findings revealed that there was no significant association between DDS and cardio-metabolic risk factors. Reassessment of the overall DDS tool as a criterion of diet quality and production of new and valid DDS standard tools is highly desirable. More high-quality studies are also needed to confirm the findings of this study.
Study registration
This study is registered as PROSPERO CRD42020157127.
Level of evidence
Level I, systematic reviews and meta-analyses.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Cardio-metabolic syndrome (CMS) is a complex clustering of metabolic and cardiovascular risk factors including dyslipidemia, systemic hypertension, central obesity, and dysglycemia [1]. Nowadays, with obesity and diabetes growing in prevalence, CMS is on the rise around the world [2, 3]. Increased prevalence of CMS and its subsequent outcomes in the cardiovascular, cerebrovascular, renal, and endocrine systems impose harmful effects on the world population [4].
An even more alarming fact is that cardiometabolic risk factors (CMRFs) are not limited to adults. In most countries, the prevalence of CMRFs has been increasing in the pediatric population owing to the rise in childhood overweight and obesity [2]. Dietary pattern and nutritional factors are among the major modifiable risk factors of obesity and metabolic disorders [5, 6]. Epidemiological studies have shown the priority of overall dietary pattern assessment in preventing chronic diseases compared with evaluation of single nutrients or food effects [7, 8]. Assessment of dietary diversity is a dietary approach to ensure high quality diets [9, 10]. Furthermore, dietary diversity is associated with adequate intake of all groups of foods and nutrients such as macronutrients and micronutrients that are protective elements against chronic diseases [11, 12].
Dietary diversity score (DDS) has been known as a useful, convenient, and inexpensive indicator of overall diet quality in large-scale surveys [13, 14]. DDS appraises all food groups diversity within a diet based on a dietary guidance [15]. Accordingly, a higher DDS is indicative of a healthier diet, and is associated with meeting all the essential nutrient requirements [16]. Previous studies have reported the association between DDS and health problems such as diabetes, metabolic syndrome, cardiovascular disease and cancer [17, 18]. In recent years, many investigators have evaluated the association between DDS and some CMRFs such as hyperlipidemia [8, 19], hypertension [8], high blood glucose [20], and abdominal obesity [21, 22]. These studies have shown controversial results in terms of beneficial or negative associations. Therefore, there is no conclusive result about the effect of DDS on cardio-metabolic risk factors. In 2016, the authors of the first systematic review and meta-analysis on the relationship between DDS and obesity failed to show any significant relationship between BMI status and high or low DDS [23].
To our knowledge, up to now, there is no comprehensive systematic review and meta-analysis about the association between DDS and CMRFs. To clarify this association, we performed a systematic review and meta-analysis of the literature.
Methods
To assess the association of DDS with cardio-metabolic risk factors, we conducted a systematic review through which all related documents were searched in international databases including PubMed and NLM Gateway, Scopus, and Institute of Scientific Information (ISI) up to October 2019. The relevant references in the selected articles were also reviewed. The protocol of present study is registered on the PROPERO with code CRD42020157127.
Search strategy
The main routes for the development of search strategies were extracted from "dietary diversity score”, "DDS", "diet quality score”, "food variety score" and all related terms to cardio metabolic risk factors (Table 1).
Inclusion and exclusion criteria
Studies were eligible for inclusion in this review as follows:
(a) Quantitative observational research design (e.g., cross-sectional); (b) Assess associations between DDS and CMRFs; (c) No limitation for time of researches or publications; (d) No limitation for language of papers; (e) No limitation for age and gender. Experimental studies in animals and those with duplicate citations were excluded. The studies that were limited to subgroup populations also were excluded. For multiple unique source publications, the most complete source of data included.
Quality assessment and data extraction strategy
Results of searches saved in Endnote software. Through three phase of refinement; titles, abstracts, and full texts were reviewed, respectively. The quality assessment of the included documents was conducted by two researchers, independently. We assessed the quality of the included studies using the Newcastle–Ottawa Quality Assessment scale [24]. Regarding quality assessment, the kappa statistic for agreement was 0.94. Probable discrepancy resolved by third expert opinion. The data were extracted from moderate and high quality studies.
The data were extracted using a checklist including general information of the study and its citation; population characteristics; methodological information of study (study region, scope of study (local study or survey), sample size, age and sex and interested measured outcomes which include overweight and/or obesity, abdominal obesity, metabolic syndrome, diabetes, BMI, waist circumference, level of lipid profile and blood pressure.
Statistical analysis
Odds ratio (OR) with 95% confidence interval (CI) was considered as the effect size for association of DDS with CMRFs as binary outcomes (obesity, overweight, abdominal obesity, diabetes, MetS) in meta-analysis. Moreover, in some studies, means (SD) of CMRFs were compared between the highest and lowest DDS, for which we used standardized mean difference (SMD) as the effect size in meta-analysis. The Chi-square based Q test and I square statistics used to assess the heterogeneity between studies. The result of Q test was regarded to be statistically significant at P < 0.1. In case of severe heterogeneity between studies regarding the reported effect sizes, pooled effect size was estimated using random-effect meta-analysis model (with the Der-Simonian and Laird method). Moreover, a forest plot was used to present the result of meta-analysis schematically. To identify possible sources of heterogeneity, subgroup analysis was done. Publication bias was evaluated using Egger’s test and it was presented schematically using funnel plots. The analyses were conducted using STATA 11 software. P values less than 0.05 were considered statistically significant.
Ethical considerations
The protocol of this study was approved by the ethical committee of Alborz University of Medical Sciences. All the included studies would be cited in all reports and all future publications.
Results
Search results and characteristics of the included studies
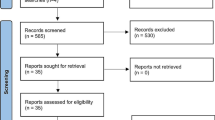
Figure 1 shows the detailed process of data refinement and studies selection. Using the above-mentioned search engines, 843 original research studies were identified (PubMed: 97, ISI: 215, Scopus: 531). After reviewing titles, abstracts, and full texts, 825 articles were excluded, because their design and population were not interested or there was not assessing DDS for individuals. In the final step, full texts were reviewed for cited references and five more articles were included. Finally, 23 observational studies (22 cross-sectional and one cohort) [8, 12, 13, 16, 19,20,21,22, 25,26,27,28,29,30,31,32,33,34,35,36,37,38,39] published between 2005 and 2018 were included according to the inclusion/exclusion criteria. Characteristics of the included studies were presented in Table 2. Fourteen studies were conducted in Asia [8, 12, 13, 19,20,21,22, 25, 26, 29, 35,36,37,38], five in Africa [28, 30, 32,33,34], two in North America [16, 39], one in South America [31] and one in Europe [27]. A relevancy assessment and quality control identified a total of 50,287 study subjects based on the inclusion/exclusion criteria (The sample size of included studies ranged from 113 to 17,825) were studied. Among 23 enrolled studies, 18 articles reported required data (OR and/or mean and SD across DDS categories) for the meta-analysis. Therefore, meta-analysis was performed on them. Five other studies were systematically reviewed [12, 16, 30, 37, 39]. Nineteen articles studied on healthy adults (ranged from 18 to 67 years) and 4 articles studied on children [12, 16, 32, 34]. 24-h recalls (n = 18) and FFQ (n = 5) [8, 13, 20, 22, 27] were the most common dietary assessment methods. To score dietary diversity, nine studies used five main groups according to the Food Guide Pyramid [8, 13, 16, 19, 22, 26, 27, 37, 39], 1 study used six [36] and another one used seven food groups [28], 4 studies used nine [12, 20, 34, 38], four articles used 12 [21, 25, 32, 35], one used 14 [30] and three studies used 24 food groups [29, 32, 33].

Flow chart of the number of studies selected into the meta-analysis
Qualitative synthesis
Data from five other studies, including children (two studies) [12, 16] and healthy adults (three studies) [30, 37, 39], could not be pooled. All of the five articles evaluated the relation of DDS with BMI. Only in Kant et al. study, in addition to body mass index, the relationship between DDS and lipid profile and blood pressure was also examined [39]. The results of Fernadez et al. study [16] and Zhao et al. study [12] which investigate the association between DDS and BMI in children were inconsistent. Fernadez et al. reported that girls and older children had greater DDS (P = 0.04, P = 0.03) and greater healthy variety score, overall variety, and DDS were associated with greater annual increases in z-score of BMI prospectively (β[SE] = 0.009 [0.004], P = 0.04; β[SE] = 0.007 [0.003], P = 0.02; β[SE] = 0.003 [0.001], P = 0.02, respectively). Whereas Zhao et al. reported that in children > 6 years old, dietary diversity indicators were negatively associated with BMI and BAZ, just opposite to that of children ≤ 6 years old. Furthermore, in comparison of 3 food diversity indicators between overweight or obese children and normal-weight children, the results failed to find a significant association between food diversity indicators and obesity status, too. Kant et al. and Tiew et al. [37] reported a negative association between DDS and BMI. Their results showed that those being overweight or obese, and those with lower WHR were found to have a significantly poorer dietary diversity, while Keding et al. [30] revealed that BMI directly correlated with DDS, suggesting that the greater the diversity of foods and food groups eaten, the higher the BMI. Moreover, in Kant et al. study, a negative relationship was observed between DDS and lipid profile and blood pressure. A meta-analysis was not performed due to insufficient data. These results of included studies in systematic review (qualitative synthesis) are shown in Table 3.
Quantitative synthesis
Overall, of the studies included in the meta-analysis, eight had examined the relation of DDS and obesity [22, 25, 26, 31, 32, 34, 35, 38], five articles reported the relation between DDS and overweight [12, 22, 26, 31, 33] and four articles assessed relationship between DDS and metabolic syndrome [19, 20, 29, 36], four reported association of DDS with abdominal obesity [19, 21, 25, 38], BMI and WC [8, 13, 21, 27]. In addition to these indices, 2 studies also evaluated the relation of DDS and diabetes [21, 28], lipid profiles such as TG, TC, LDL and HDL, and blood pressure (systolic and diastolic blood pressure) [8, 13]. These results of included studies in meta-analysis are shown in Table 4.
The association of DDS with obesity-related outcomes
DDS with obesity, abdominal obesity, and overweight
Our meta-analysis based on eight papers [22, 25, 26, 31, 32, 34, 35, 38] with a total of 21,796 subjects failed to reach a significant association between DDS and obesity (OR = 0.98; 95% CI 0.92,1.05) with substantial heterogeneity (Q = 39.57; P = ˂ 0.001; I2% = 82.3).
Subgroup analysis based on age group revealed that there was no significant relationship between DDS and obesity in both adults (OR = 0.98; 95% CI 0.91, 1.04) and children (OR = 3.3; 95% CI 0.07,6.54). In the subgroup analysis, a significant inverse relationship between higher DDS and reduced risk of obesity was observed among studies whose participants were women (OR = 0.41; 95% CI 0.18, 0.7), whereas the analysis on studies with both sexes did not show a significant association (OR = 1.19; 95% CI 0.86, 1.51) and one study which assessed the relationship between DDS and obesity in men showed a significant direct association (OR = 3.4; 95% CI 1.2, 5.6).
The results of meta-analysis on articles which studied the relation of DDS and abdominal obesity (4 studies, number of participants = 2887) and overweight (5 studies, number of participants = 19,578) failed to show significant relationship (OR = 1.17; 95% CI 0.6, 1.73) with absolute heterogeneity (Q = 22.45; P = ˂ 0.001; I2% = 86.6) and (OR = 1.03; 95% CI 0.73, 1.31) with substantial heterogeneity (Q = 14.73; P = 0.005; I2% = 72.9).
DDS with BMI and waist circumferences
The results from the meta-analyses failed to show a significant relationship between DDS and body mass index (4 studies, number of participants = 3898, SMD: 0.32, 95% CI − 0.01, 0.65) and waist circumference (4 studies, number of participants = 3898, SMD: 0.05, 95% CI − 0.31, 0.41) but there was considerable heterogeneity among estimates (Q = 27.59; P = ˂ 0.001; I2% = 89.1) and (Q = 32.89; P = ˂ 0.001; I2% = 90.9), respectively.
The association of DDS with MetS
Our meta-analysis on five studies with 5701 participants that assessed the relation of DDS with MetS showed there was no significant association between quartiles of DDS and risk of metabolic syndrome (OR = 0.80; 95% CI 0.71, 1.81) with substantial heterogeneity (Q = 25.65; P = 0.005; I2% = 84.4).
The association of DDS with diabetes
There was no significant association between DDS and risk of diabetes (2 studies, number of participants = 4410, OR = 1.06; 95% CI 0.94, 1.18) with non-considerable heterogeneity (Q = 1.73; P = 0.19; I2% = 42.3) and blood pressure (2 studies, number of participants = 348).
Systolic blood pressure (OR = − 2.43; 95% CI − 5.83, 0.97), substantial heterogeneity (Q = 117.28; P = ˂ 0.001; I2% = 99.1) and diastolic blood pressure (OR = − 0.94; 95% CI − 2.64, 0.76) with considerable heterogeneity (Q = 41.18; P = ˂ 0.001; I2% = 97.6).
The association of DDS with lipid profile
The result of meta-analysis on 2 studies with 348 participants which evaluate relation of DDS with lipid profile revealed an inverse association between higher DDS and lower level of TG (SMD − 0.23, 95% CI − 0.45, − 0.01) without considerable heterogeneity (Q = 0.48; P = 0.49; I2% = 0.0), whereas there was no significant relation between DDS and level of TC (SMD − 0.37, 95% CI − 1.13, 0.39) with substantial heterogeneity (Q = 8.88; P = < 0.001; I2% = 88.7), LDL (SMD − 2.0, 95% CI − 5.92, 1.92, 0.19) with obvious heterogeneity (Q = 164.38; P = < 0.001; I2% = 99.4) and HDL (SMD 0.19, 95% CI − 0.029, 0.41) without obvious heterogeneity (Q = 0.01; P = 0.93; I2% = 0.0).
Publication bias
The funnel plot assessment by visual inspection was done and revealed that it is quite symmetrical and no publication bias for any variable was demonstrated. Similarly, the Egger's test also showed that there was no publication bias.
Risk of Bias
Table 5 shows the individual and summary risk of bias assessments of the included articles based on Newcastle–Ottawa Quality Assessment scale. The majority of studies were assessed as having low risk of bias across domains.
Discussion
To the best of our knowledge, the present systematic review and meta-analysis is the first comprehensive study assessing the relationship between DDS and cardio-metabolic risk factors including overweight, obesity, abdominal obesity, metabolic syndrome, diabetes, blood pressure and lipid profile.
Our results showed that in the case of BMI, five studies reported that increased DDS was positively associated with BMI [8, 13, 16, 21, 30], whereas three studies showed an inverse relationship between DDS and BMI [12, 27, 39]. Overall, ten studies had studied obesity and overweight in relation to DDS. Two studies failed to find an association between obesity/overweight and DDS [32, 33]. Six studies reported a direct association between obesity and DDS [23, 26, 31, 34, 35, 38], while two studies reported an inverse association [25, 37]. Out of four studies which assessed the association between abdominal obesity and DDS, two articles reported positive association [21, 38] and two study reported negative [19, 25]. Consistent with a previous systematic review and meta-analysis [23], our results failed to show a significant association between DDS, BMI, and overweight/obesity/abdominal obesity. However, in a systematic review by Asghari and colleagues [40], scoring on the basis of dietary diversity has direct association with weight gain. One of the reasons for the discrepancy between the results of their study (Asghari et al.) and the present study may be the smaller number of included articles and, therefore, the smaller sample size.
To find out the source of heterogeneity, subgroup analysis was performed based on sex and age. Subgroup analyses according to sex in studies reporting ORs of overweight/obesity suggested a complete absence of heterogeneity in studies whose participants were only women or men. Furthermore, another subgroup analysis based on age showed the absence of heterogeneity in studies that assessed the association of DDS with obesity in children, while those studies that assessed this association in adults had a substantial heterogeneity. Perhaps the reason for non- significant results was the inconsistency of the results of primary studies and there was a great deal of contradiction between the primary studies. Moreover, our results showed a protective effect of DDS on obesity in women. The different effects and contradictory findings in men and women may be due to the effects of hormonal changes and more weight gain over time in women, as well as receiving higher amounts of energy in men compared to women and as a result being in challenge with controlling fat and sodium intake in men.
Three studies reported blood pressure and lipid profile as an outcome. Two of these articles showed negative association between systolic blood pressure and lipid profile with DDS, whereas one study showed no significant relationship. The results of our study did not show a significant relationship between DDS and blood pressure and lipid profile except the level of TG. According to our analysis, higher quartile of DDS had protective and decreasing relationship with level of TG. These findings were inconsistent with a previous study which showed a relationship between FGDS (food group dietary score) and serum lipid levels [41]. The medium FGDS category had the highest mean triglyceride level, consistent with the higher obesity rate, whereas the low FGDS category had an association with the lowest total serum cholesterol, LDL-cholesterol and highest HDL-cholesterol levels. An inverse association was found between overall dietary score and blood pressure, high LDL-cholesterol levels [8, 42], hypercholesterolaemia, diabetes [8], and triglycerides [42], all known CVD risk factors in adults.
Two studies reported that increased DDS was significantly associated with decreased risk of metabolic syndrome, while three studies failed to identify a significant association between DDS and metabolic syndrome. Furthermore, in the two studies evaluating the relationship between the diet diversity score and OR of diabetes, no significant relationship was reported.
Unfortunately, regarding the relationship between diet diversity score and metabolic syndrome and diabetes, so far, not only no secondary study was done, but also the number of initial studies is too small to see definitive results.
This study had several limitations. First, some studies reported the DDS–BMI/blood pressure and lipid profile association only at baseline [8, 13, 21, 27]. Unfortunately, because researchers used different food groups to calculate DDS, we were unable to show to what extent the DDS contributed to individual foods or food groups. In fact, studies used a range of defined food groups to score diversity and most studies used dietary recall rather than a food frequency questionnaire to examine the diversity of the diet. Since the tool used to calculate and assessing dietary diversity scores plays an important role in determining the relationship with risk factors such as obesity, it seems that the use of a food frequency questionnaire is the most appropriate tool for assessing long-term diet diversity. Considering the fact that overweight individuals adopt a healthier diet to manage their weight, conflicting results could also be explained partly by this confounding factor. Moreover, most of the included studies did not adjust for two important confounders: drug therapy, supplements intake, energy intake and socioeconomic status. Adjustment for energy intake and socioeconomic status in future studies is highly recommended. It should be borne in mind that due to the lack of data, we were unable to include five studies in the meta-analysis. Moreover, studies that clearly stated that they used DDS were included in our meta-analysis and other dietary scores such as FDS and FGDS did not enter in our study. In the present meta-analysis, we compared cardio-metabolic risk factors between participants with the highest and lowest DDS to evaluate the linear association between DDS and variables; however, the association may be curvilinear (U-shaped). Despite these limitations, the study has notable strengths such as using comprehensive assessment of a variety of cardio-metabolic risk factors in adults and children, with a relatively large participant number and the use of a random effects model for overall analysis.
In conclusion, our systematic review and meta-analysis showed that there was no significant association between DDS and most of the CMRFs. On the other hand, our results showed an inverse association between DDS and TG. The situation may be due to different methods for assessing DDS as well as various methods used to evaluate dietary intake. Reassessment of the overall DDS tool as a criterion of diet quality and production of new and valid DDS standard tools is highly desirable. In addition, further longitudinal studies and field trials are recommended to confirm these findings.
What is already known on this subject?
In primary studies, there is no conclusive result about the beneficial or negative effect of DDS on cardio-metabolic risk factors and up to now, there is no comprehensive systematic review and meta-analysis about the association between DDS and CMRFs. To clarify this association, we performed a systematic review and meta-analysis of the literature.
What does this study add?
Our results showed an inverse association between DDS and TG but we don’t observed any significant association between DDS and other CMRFs (obesity and overweight, BMI, diabetes, metabolic syndrome and lipid profile). These results may be due to the lack of a unified method in estimating DDS, so it seems that it needs to reassessment of the overall DDS tool and production of new and valid DDS standard tools to achieve conclusive results.
Change history
29 April 2021
A Correction to this paper has been published: https://doi.org/10.1007/s40519-021-01192-7
References
Grundy SM, Brewer HB Jr, Cleeman JI, Smith SC Jr, Lenfant C (2004) Definition of metabolic syndrome: report of the National Heart, Lung, and Blood Institute/American Heart Association conference on scientific issues related to definition. Circulation 109(3):433–438. https://doi.org/10.1161/01.CIR.0000111245.75752.C6
Kelli HM, Kassas I, Lattouf OM (2015) Cardio metabolic syndrome: a global epidemic. J Diabetes Metab 6(513):2. https://doi.org/10.4172/2155-6156.1000513
Ash-Bernal R, Peterson LR (2006) The cardiometabolic syndrome and cardiovascular disease. J Cardiometab Syndr 1(1):25–28. https://doi.org/10.1111/j.0197-3118.2006.05452.x
Anand SS, Yusuf S (2011) Stemming the global tsunami of cardiovascular disease. The Lancet 377(9765):529–532. https://doi.org/10.1016/S0140-6736(10)62346-X
Lutsey PL, Steffen LM, Stevens J (2008) Dietary intake and the development of the metabolic syndrome. Circulation 117(6):754–761. https://doi.org/10.1161/CIRCULATIONAHA.107.716159
de la Iglesia R, Loria-Kohen V, Zulet M, Martinez J, Reglero G, Ramirez-de-Molina A (2016) Dietary strategies implicated in the prevention and treatment of metabolic syndrome. Int J Mol Sci 17(11):1877. https://doi.org/10.3390/ijms17111877
Millen BE, Quatromoni PA, Pencina M, Kimokoti R, Nam B-H, Cobain S et al (2005) Unique dietary patterns and chronic disease risk profiles of adult men: the Framingham nutrition studies. J Am Diet Assoc 105(11):1723–1734. https://doi.org/10.1016/j.jada.2005.08.007
Azadbakht L, Mirmiran P, Esmaillzadeh A, Azizi F (2006) Dietary diversity score and cardiovascular risk factors in Tehranian adults. Public Health Nutr 9(6):728–736. https://doi.org/10.1079/PHN2005887
Kennedy E (2004) Dietary diversity, diet quality, and body weight regulation. Nutr Rev 62(suppl 2):S78–S81. https://doi.org/10.1111/j.1753-4887.2004.tb00093.x
Vandevijvere S, De Vriese S, Huybrechts I, Moreau M, Van Oyen H (2010) Overall and within-food group diversity are associated with dietary quality in Belgium. Public Health Nutr 13(12):1965–1973. https://doi.org/10.1017/S1368980010001606
Hatløy A, Torheim LE, Oshaug A (1998) Food variety—a good indicator of nutritional adequacy of the diet? A case study from an urban area in Mali, West Africa. Eur J Clin Nutr 52(12):891. https://doi.org/10.1038/sj.ejcn.1600662
Zhao W, Yu K, Tan S, Zheng Y, Zhao A, Wang P et al (2017) Dietary diversity scores: an indicator of micronutrient inadequacy instead of obesity for Chinese children. BMC Public Health 17(1):440. https://doi.org/10.1186/s12889-017-4381-x
Farhangi MA, Jahangiry L (2018) Dietary diversity score is associated with cardiovascular risk factors and serum adiponectin concentrations in patients with metabolic syndrome. BMC Cardiovasc Disord 18(1):68. https://doi.org/10.1186/s12872-018-0807-3
Nachvak SM, Abdollahzad H, Mostafai R, Moradi S, Pasdar Y, Rezaei M et al (2017) Dietary diversity score and its related factors among employees of Kermanshah University of Medical Sciences. Clin Nutr Res 6(4):247–255. https://doi.org/10.7762/cnr.2017.6.4.247
Rathnayake KM, Madushani P, Silva K (2012) Use of dietary diversity score as a proxy indicator of nutrient adequacy of rural elderly people in Sri Lanka. BMC Res Notes 5(1):469. https://doi.org/10.1186/1756-0500-5-469
Fernandez C, Kasper NM, Miller AL, Lumeng JC, Peterson KE (2016) Association of dietary variety and diversity with body mass index in US preschool children. Pediatrics 137(3):e20152307. https://doi.org/10.1542/peds.2015-2307
Kastorini C-M, Milionis HJ, Esposito K, Giugliano D, Goudevenos JA, Panagiotakos DB (2011) The effect of Mediterranean diet on metabolic syndrome and its components: a meta-analysis of 50 studies and 534,906 individuals. J Am Coll Cardiol 57(11):1299–1313. https://doi.org/10.1016/j.jacc.2010.09.073
Terry P, Giovannucci E, Michels KB, Bergkvist L, Hansen H, Holmberg L et al (2001) Fruit, vegetables, dietary fiber, and risk of colorectal cancer. J Natl Cancer Inst 93(7):525–533. https://doi.org/10.1093/jnci/93.7.525
Azadbakht L, Mirmiran P, Azizi F (2005) Dietary diversity score is favorably associated with the metabolic syndrome in Tehranian adults. Int J Obes 29(11):1361. https://doi.org/10.1038/sj.ijo.0803029
Gholizadeh F, Moludi J, Yagin NL, Alizadeh M, Nachvak SM, Abdollahzad H et al (2018) The relation of Dietary diversity score and food insecurity to metabolic syndrome features and glucose level among pre-diabetes subjects. Prim Care Diabetes 12(4):338–344. https://doi.org/10.1016/j.pcd.2018.03.003
Jayawardena R, Byrne NM, Soares MJ, Katulanda P, Yadav B, Hills AP (2013) High dietary diversity is associated with obesity in Sri Lankan adults: an evaluation of three dietary scores. BMC Public Health 13(1):314. https://doi.org/10.1186/1471-2458-13-314
Karimbeiki R, Pourmasoumi M, Feizi A, Abbasi B, Hadi A, Rafie N et al (2018) Higher dietary diversity score is associated with obesity: a case–control study. Public Health 157:127–134. https://doi.org/10.1016/j.puhe.2018.01.028
Salehi-Abargouei A, Akbari F, Bellissimo N, Azadbakht L (2016) Dietary diversity score and obesity: a systematic review and meta-analysis of observational studies. Eur J Clin Nutr 70(1):1–9. https://doi.org/10.1038/ejcn.2015.118
Deeks JJ, Dinnes J, D’Amico R, Sowden AJ, Sakarovitch C, Song F et al (2003) “Evaluating non-randomised intervention studies” (PDF). Health Technol Assess 7(27):27. https://doi.org/10.3310/hta7270
Abris GP, Provido SMP, Hong S, Yu SH, Lee CB, Lee JE (2018) Association between dietary diversity and obesity in the Filipino Women’s Diet and Health Study (FiLWHEL): a cross-sectional study. PLoS ONE 13(11):e0206490. https://doi.org/10.1371/journal.pone.0206490
Leila A, Ahmad E (2010) Dietary diversity score is related to obesity and abdominal adiposity among Iranian female youth. Public Health Nutr 14(1):62–69. https://doi.org/10.1017/S1368980010000522
Cano-Ibáñez N, Gea A, Martínez-González MA, Salas-Salvadó J, Corella D et al (2019) Dietary diversity and nutritional adequacy among an older spanish population with metabolic syndrome in the PREDIMED-Plus study: a cross-sectional analysis. Nutrients 11:958. https://doi.org/10.3390/nu11050958
Danquah I, Galbete C, Meeks K, Nicolaou M, Klipstein-Grobusch K et al (2018) Food variety, dietary diversity, and type 2 diabetes in a multi-center cross-sectional study among Ghanaian migrants in Europe and their compatriots in Ghana: the RODAM study. Eur J Nutr 57:2723–2733. https://doi.org/10.1007/s00394-017-1538-4
Jeong W, Jin B, Hwang E (2012) Prevalence of metabolic syndrome and assessment of food․ nutrient intakes among adult visitors of a Public Health Center in Korea. J Korean Soc Food Sci Nutr 41(2):205–212. https://doi.org/10.3746/jkfn.2012.41.2.205
Keding GB, Msuya JM, Maass BL, Krawinkela MB (2013) Obesity as a public health problem among adult women in rural Tanzania. Glob Health: Sci Pract. https://doi.org/10.9745/GHSP-D-13-00082
Ponce X, Ramirez E, Delisle H (2006) A more diversified diet among mexican men may also be more atherogenic. Am Soc Nutr. https://doi.org/10.1093/jn/136.11.2921
Sagbo H, Ekouevi DK, Ranjandriarison DT, Niangoran S, Bakai TA et al (2018) Prevalence and factors associated with overweight and obesity among children from primary schools in urban areas of Lomé, Togo. Public Health Nutr. https://doi.org/10.1017/S1368980017003664
Savy M, Martin-Prevel Y, Danel P, Traissac P, Dabire HB, Delpeuch F (2008) Are dietary diversity scores related to the socio-economic and anthropometric status of women living in an urban area in Burkina Faso? Public Health Nutr 11(2):132–141. https://doi.org/10.1017/S1368980007000043
Tadesse Y, Derso T, Alene KA, Wassie MM (2017) Prevalence and factors associated with overweight and obesity among private kindergarten school children in Bahirdar Town, Northwest Ethiopia: cross-sectional study. BMC Res Notes 10:22. https://doi.org/10.1186/s13104-016-2308-8
Tian X, Wu M, Zang J, Zhu Y, Wang H (2016) Dietary diversity and adiposity in Chinese men and women: an analysis of four waves of cross-sectional survey data. Eur J Clin Nutr. https://doi.org/10.1038/ejcn.2016.212
Tian X, Wu M, Zang J, Zhu Y, Wang H (2017) Gender difference of metabolic syndrome and its association with dietary diversity at different ages. Oncotarget 8(43):73568–73578. https://doi.org/10.18632/oncotarget.20625
Tiew KF, Chan YM, Lye MS, Loke SC (2014) Factors associated with dietary diversity score among individuals with type 2 diabetes mellitus. J Health Popul Nutr 32(4):665–676
Zhang Q, Chen X, Liu Z, Varma DS, Wan R, Zhao S (2017) Diet diversity and nutritional status among adults in southwest China. PLoS ONE 12(2):e0172406. https://doi.org/10.1371/journal.pone.0172406
Kant AK, Graubard BI (2005) A comparison of three dietary pattern indexes for predicting biomarkers of diet and disease. J Am Coll Nutr 24(4):294–303. https://doi.org/10.1080/07315724.2005.10719477
Asghari G, Mirmiran P, Yuzbashian E, Azizi F (2017) A systematic review of diet quality indices in relation to obesity. Br J Nutr. https://doi.org/10.1017/S0007114517000915
Oldewage-Theron WH, Egal AA (2014) A cross-sectional baseline survey investigating the relationship between dietary diversity and cardiovascular risk factors in women from the Vaal Region, South Africa. J Nurs Educ Pract. https://doi.org/10.5430/jnep.v4n1p50
Hoebeeck LI, Rietzschel ER, Langlois M, De Buyzere M, De Bacquer D, De Backer G et al (2011) The relationship between diet and subclinical atherosclerosis: results from the Asklepios study. Eur J Clin Nutr 65:606–613. https://doi.org/10.1038/ejcn.2010.286
Acknowledgements
The authors would like to express their appreciation to all participants and scientific and executive partners who took part in this study.
Funding
The research reported in this publication was approved and supported by the Alborz University of Medical Sciences, under Code No. [97164].
Author information
Authors and Affiliations
Contributions
MQ and MH participated in the study design and drafted the manuscript. SD and MQ participated in the study design and statistical analysis and drafted the manuscript. MH and HE contributed to the protocol development and drafted the manuscript. MK, AM, NK, AS and ME contributed to the data acquisition. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no competing interests.
Ethical approval
The present study was approved by the ethical committee of Alborz The University of Medical Science (IR.ABZUMS.REC.1398.186).
Informed consent
Since this study is a secondary study, the informed consent is not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Qorbani, M., Mahdavi-Gorabi, A., Khatibi, N. et al. Dietary diversity score and cardio-metabolic risk factors: an updated systematic review and meta-analysis. Eat Weight Disord 27, 85–100 (2022). https://doi.org/10.1007/s40519-020-01090-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40519-020-01090-4