
Abstract
Background
Obesity has been proven to be a risk factor for type 2 diabetes mellitus (T2DM) through numerous pathogenetic mechanisms. Unexpectedly, some studies suggest that subjects with overweight/obesity and T2DM have better clinical outcome than their normal weight peers. This finding is described as “obesity paradox” and calls into question the importance of weight loss in this specific population.
Objective
This article is a narrative overview on the obesity and type 2 diabetes mellitus, particularly regarding the obesity paradox in T2DM patients.
Methods
We used as sources MEDLINE/PubMed, CINAHL, EMBASE, and Cochrane Library, from inception to March 2020; we chose 30 relevant papers regarding the association of obesity with clinical outcome and mortality of patients affected by T2DM.
Results
Many studies report that in patients with T2DM, overweight and obesity are associated with a better prognosis than underweight or normal weight, suggesting the presence of an obesity paradox. However, these studies have numerous limitations due to their mainly retrospective nature and to numerous confounding factors, such as associated pathologies, antidiabetic treatments, smoking habit, lack of data about distribution of body fat or weight history.
Conclusion
Literature data regarding the phenomenon of obesity paradox in T2DM patients are controversial due to the several limitations of the studies; therefore in the management of patients with overweight/obesity and T2DM is recommended referring to the established guidelines, which indicate diet and physical activity as the cornerstone of the treatment.
Level of evidence
Level V: narrative review.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Epidemiological studies show an increasing prevalence and incidence of type 2 diabetes mellitus (T2DM) and obesity over the past decades.
In 2014, in the world, 422 million people (8.5% of the adult population) had diabetes and in more than 90% of cases it was T2DM. Diabetes caused directly 1.5 million deaths in 2012, with an additional 2.2 million due to the increased risk of fatal cardiovascular diseases. Many of these deaths (43%) occur under the age of 70 [1].
The prevalence of obesity nearly doubled worldwide since 1980 [2] and severe obesity, that is associated with the highest mortality risk, is a rapidly growing segment of the global epidemic [3]. In 2016, more than 39% and 13% of the adults were affected by overweight and obesity, respectively [4].
Obesity is known to be the main risk factor for a number of non-communicable diseases; overweight and obesity account for 44% of the diabetes cases, 23% of the ischemic heart diseases, and 7–41% of some cancers [3]. T2DM is the morbidity most strongly associated with obesity: the prevalence of T2DM is three to seven times higher in obese adults compared to normal-weight ones. Adults with body mass index (BMI) > 35 kg/m2 are 20 times as likely to develop T2DM compared to those with a BMI between 18.5 and 24.9 kg/m2 [5]. Moreover, 80% of T2DM patients are with overweight or obesity; the strong relationship between the two conditions led to the notion of “diabesity” [5,6,7].
However, the impact of obesity on the clinical outcome of people affected by T2DM is debated; some studies suggest that individuals with overweight/obesity and diabetes have lower mortality compared with normal weight subjects.
This article is a narrative overview on the obesity and type 2 diabetes mellitus, particularly regarding the “obesity paradox” in T2DM patients.
Methods
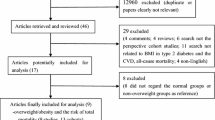
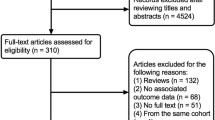
We used as sources MEDLINE/PubMed, CINAHL, EMBASE, and Cochrane Library, from inception to 2020. Keywords: obesity paradox, type 2 diabetes, overweight, obesity, mortality, body mass index, visceral obesity, waist-to-hip ratio, waist circumference. In addition we hand-searched references from the retrieved articles and explored a number of related web sites. After discussion we identified 116 references and selected 30 relevant clinical studies.
This paper belongs to the Topical Collection ‘‘Obesity Paradox”.
Obesity and diabetes: pathogenetic mechanisms
Diabetes is mainly characterized by two metabolic defects: the reduced capacity of the peripheral tissue to respond to insulin and the β-cell dysfunction, expressed by inadequate insulin secretion in response to insulin resistance and hyperglycemia. Obesity has a negative impact on both ones [8, 9].
Central (intra-abdominal) obesity, observed in the majority of patients with T2DM, is associated with insulin resistance, mainly in the adipose tissue, liver and skeletal muscle [5]. The discovery of macrophage infiltration in the abdominal adipose tissue and the unbalanced production of adipocyte protein factors and hormones (adipokines) allowed a better understanding of the mechanisms governing the development of insulin resistance. Furthermore, in the obese state, the cellular uptake of non-esterified fatty acids (NEFAs) is increased and the subsequent β-oxidation impaired, contributing to the accumulation of intermediate lipid metabolites and causing defects in the insulin signaling pathway [10].
Insulin resistance has a proatherogenic effect and doubles per se the risk for cardiovascular disease, which is the ultimate cause of death in about 80% of patients with T2DM [11].
Adipose tissue and insulin-resistance
Adipose tissue operates like an endocrine organ modulating metabolism by releasing NEFAs, glycerol, pro-inflammatory cytokines (TNF, IL-6, MCP-1) and hormones (anti-hyperglycemic leptin and adiponectin and pro-hyperglycemic resistin and RBP4).
NEFAs increasing may be the most critical factor in modulating insulin-sensitivity [12, 13]. Plasma NEFAs are elevated in insulin resistant states. On the contrary, insulin resistance is improved when plasma NEFAs levels are reduced. Moreover, increased cellular NEFAs concentrations inhibit insulin secretion, stimulate gluconeogenesis and promote severe tissue insulin resistance [14].
Increased plasma NEFAs levels are the result of different pathophysiological events [15] and the reported link between plasma NEFAs and T2DM is stronger for the level of adiposity as opposed to insulin sensitivity and/or glycemic control, highlighting the close association of obesity with the development of T2DM [14].
The adipokines TNF, IL-6, MCP-1 are implicated in the induction of insulin resistance up-regulating potential mediators of inflammation (JNK and NF-kB pathways) [16].
The TNF-α, mainly produced by macrophages infiltrating adipose tissue, decreases the expression of insulin receptor (IR) and also causes reduced oxidation of NEFAs in hepatocytes and skeletal muscle cells. The reduced rate of NEFAs oxidation results in increased accumulation of intermediate bioactive lipid metabolites, which in turn inhibit IR substrates activity [10].
IL-6 can act both centrally and on peripheral tissues so as to influence glucose homeostasis and body weight in different ways [17]. Adipose tissue produces approximately 15–35% of total human circulating levels of IL-6 and visceral adipose tissue produces three to four times more IL-6 than subcutaneous fat. Elevated IL-6 plasma levels are associated with an increasing of NEFAs levels [18] and have been described in patients with T2DM, especially in those who had features of insulin resistance [19]. IL-6 may have a role in the development of insulin resistance in adipocytes and hepatocytes decreasing the expression of IR and IR substrate [20].
Resistin is expressed primarily in adipose tissue infiltrating macrophages, its expression is up-regulated in type 2 diabetes [21] and induces insulin resistance, as well as Retinol Binding Protein 4 (RBP-4) [22, 23].
Leptin inhibits insulin secretion from pancreatic β-cells in vitro and in vivo and has the additional effect of reducing pre-proinsulin gene expression [24]. Moreover, the presence of high leptin plasma levels in obese individuals involves an increased concentration of inflammatory markers [25].
Adiponectin acts as insulin-sensitizer, stimulating fatty acid oxidation by AMPK and PPARγ, otherwise high levels of adiponectin preserve β-cell mass; the low levels found in obesity and T2DM would contribute to insulin resistance [10, 26].
β-Cells declined function
Obesity-linked type 2 diabetes is characterized by the failure of pancreatic β-cell mass and function due to an increased metabolic demand in order to compensate for insulin resistance [27]. If the alterations of the β-cells may be causal to the pathogenesis of obesity-linked T2DM or suggestive of hardworking β-cells attempting to produce sufficient insulin for compensation is unclear [28]. In obese patients a continued decline in β-cells function has been described; one of the possible mechanisms involved could be the increasing in NEFAs plasma concentrations, that prevent the expected compensatory β-cell response [29].
The well documented loss of pancreatic β-cell mass in T2DM is believed to be the result of combined stresses (oxidative, inflammatory) directed specifically at the β-cell [30]. The elevated blood glucose levels frequently observed in diabetes contribute through glucotoxic effects on the β-cell and harmful effects on insulin-sensitivity [29].
β-cell dysfunction also contributes to the pathogenesis of T2DM [31], and the loss of normal β-cell function possibly precedes the loss of β-cells [32]. Even if the underlying causes of β-cell dysfunctions are not fully understood, the common dysfunctional characteristics in type 2 diabetes are: diminished glucose sensing, increased basal insulin secretion, blunted first-phase insulin secretory response to glucose, increased proinsulin/insulin ratio [30] and a presume decreased insulin production [28, 33].
Distribution of body fat
The distribution of body fat is itself a critical determinant of insulin sensitivity [34]. White adipose tissue (WAT), consisting of subcutaneous and visceral fat, has an important role in the regulation of fatty acid homeostasis. Subcutaneous WAT is by far the largest adipose depot within the human body. Visceral WAT (mainly composed by omental, mesenteric, retroperitoneal and epicardial fat) constitutes about 15% of total fat in obese individuals. The infiltration of macrophages, which most characterizes the visceral fat, leads to the secretion of bioactive signaling proteins, the adipokines, playing an essential role in the development, exacerbation and maintenance of an insulin resistant state [10].
Along with visceral fat, ectopic fat storage plays an important role in insulin resistance [35, 36]; accumulation of excess lipids in liver and skeletal muscle contribute to the development of insulin resistance, not only in that organs, but also at systemic level [37, 38].
In obesity, the increased infiltration of macrophages and other immune cells, in visceral and ectopic fat, leads to a state of chronic, low-grade, local and systemic inflammation. Local inflammation may induce alterations in metabolism and the storage capacity of dietary lipid in adipocytes [39, 40]. Furthermore the systemic inflammation, may affect insulin signalling and metabolism of non-adipose tissues, like the liver and skeletal muscle, contributing to the accumulation of ectopic fat and development of insulin resistance [35, 41] by establishing a vicious circle.
Genetic and environmental factors
Since the sixties a role of genetic factors and environment has been hypothesized in the pathogenesis of T2DM [42]. To date we know more than 50 loci, mainly related to the function of the Beta-cell, implicated in the etiology of the disease [43, 44]; none of the known genes, however, is highly predictive per se of the risk to develop T2DM; what is really important, in the pathogenesis of the disease, is the interaction between predisposing genotypes and deleterious environmental factors. Increased caloric intake, low physical activity, a diet rich in saturated fatty acids are some of the modifiable factors implied in the development of insulin-resistance, obesity, beta cell dysfunction and, lastly, T2DM [44, 45].
Obesity paradox and type 2 diabetes: controversial results
In light of all the data mentioned above, regarding the pathogenetic link between obesity and T2DM, it would be reasonable to suppose that weight loss can be beneficial and lead to better clinical outcomes in T2DM patients with overweight and obesity [46, 47]. However, results from longitudinal observational studies suggest that individuals with overweight/obesity and diabetes have lower mortality and better outcomes with respect to the cardiovascular diseases associated, than their normal weight peers [48, 49]. These results, that may appear counter-intuitive, represent the “obesity paradox” [50,51,52,53,54], already described in subjects with overweight/obesity and acute coronary syndrome or hearth failure or stroke too [55,56,57,58,59,60]. The obesity paradox has led some Authors to suggest that patients with established chronic diseases should avoid weight loss [61] because adipose tissue could represent an energy reserve during acute exacerbations of the illness [62].
So, the discussion can concern to the relevance of the obesity paradox with respect to the prognosis of T2DM, and also to the importance of weight loss in the treatment of overweight and obese people with T2DM.
Many studies provide observations favoring the existence of an obesity paradox in T2DM, describing an inverse relationship between BMI and mortality, or a J- or U-shape association. In a multicenter, prospective, observational study, to evaluate the risk factors for mortality among patients with T2DM, McEwen et al. observed that subjects with normal weight experienced higher mortality than subjects with overweight or obesity [63]. Similarly, Kokkinos et al. in a cohort of 4156 patients with T2DM, reported that normal weight subjects had a higher mortality than those with class II obesity [64]. These results were confirmed by Lin et al. that, in a large population of T2DM, shows that a BMI ≥ 27.5 kg/m2 was associated with less hospitalization and mortality than lower BMI categories; patients with BMI ≤ 18.5 kg/m2 had the poorest prognosis [65]. In the same way, a prospective study of a cohort of 2161 Asian diabetic patients showed the obesity paradox describing a U-shaped association between BMI and all cause mortality; the latter was highest for BMI ≤ 22.5 or ≥ 30 kg/m2. The association remained after adjustment for sex, smoking status, age and kidney function [66].
Doehner et al. [67] in a study including 5202 patients with T2DM and cardiovascular comorbidity, with a follow-up of 34.5 months, showed that patients with overweight and obesity had a lower mortality compared to patients with normal weight. Similarly, a post hoc analysis from the Trial Evaluating Cardiovascular Outcomes with Sitagliptin (TECOS), that enrolled patients affected by T2DM and atherosclerotic cardiovascular disease, showed that subjects with overweight or first class obesity had a lower cardiovascular risk than those who were under or normal weight; in patients with class II and III obesity, the risk was similar to the first class [68].
The presence of an obesity paradox was also suggested by Park et al. in a population of 1338 stroke patients with T2DM, the incidence of major adverse cardiovascular events was less frequent in the overweight and obese groups with respect to the normal weight one [69].
Mulnier et al. [70] in a cohort of 44,230 patients with T2DM, reported that those with a BMI 15–19 or ≥ 30 kg/m2 had an increased risk of mortality compared with a BMI 20–24 kg/m2, but without significant mortality risk difference in those with a BMI 25–29 kg/m2 compared to BMI 20–24 kg/m2.
Logue et al. in a retrospective study by using records of 106,640 patients with T2DM, reported that patients with normal weight (20–25 kg/m2) or with class II obesity (≥ 35 kg/m2) exhibited higher mortality compared with the overweight group [48].
Costanzo et al. in a cohort of 10,568 patients with T2DM followed for a median of 10.6 years, also showed survival advantages for the subjects with BMI 25.0–29.9 kg/m2 compared to normal weight or obese BMI categories (J-shape association) [71].
Zhao et al. [72] in a prospective cohort study of 19,478 black and 15,354 white patients with T2DM, reported a U-shape association: subjects with BMI 30–35 kg/m2 were generally at lower risk of death than subjects with underweight, normal weight and with class II obesity; overweight was a risk factor only in the black race.
Finally, Lee et al. [73] in a large prospective study, examining the associations between BMI and mortality in individuals with normoglycemia, impaired fasting glucose (IFG), newly diagnosed diabetes and prevalent diabetes, confirmed a U-shaped association between BMI and mortality in T2DM, showing lowest mortality between 25.0 and 29.4 kg/m2 in patient with newly diagnosed diabetes.
In spite of mentioned findings supporting the presence of the obesity paradox in diabetes (Table 1), other authors [74,75,76] have shown opposite results (Table 2).
Zahir et al. [76] in a cohort of 10,575 Australian adults, comparing BMI and mortality, found a significantly higher mortality among obese patients respect to normal weight ones in the total sample, as well as in the subgroup of patients with T2DM. Even in a recent prospective study of 1282 T2DM, a greater BMI, and in particular a greater abdominal obesity, was associated with an increased mortality; in this study there was no evidence of the obesity paradox [77].
Similarly, Eeg-Olofsson et al. [78] studying 13,087 patients of the Swedish National Diabetes Register, observed a direct linear relationship, estimating a 20% increasing in mortality risk for each additional 5 BMI kg/m2 unit.
Other observations concern the possible presence of the obesity paradox in subjects with diabetes and heart failure (HF). Adamopoulos et al. examining the association between obesity and outcomes in cohorts of HF patients with and without T2DM, showed that in patients with chronic mild to moderate HF and T2DM, obesity confers no paradoxical survival benefit [79]. Recently, similar results have been reported by other authors [80].
Limitations of the studies on obesity paradox and diabetes
Two recent systematic reviews [81, 82] conclude that many studies show evidence of the obesity paradox in T2DM, but if this finding may be generalizable to all patients with T2DM remains controversial: the presence of confounding factors may contribute to the heterogeneity of the observations reported [69, 81,82,83].
The majority of the aforementioned studies are retrospective; discussing their possible limitations, a first observation could regard the time of BMI evaluation: in most of the researches, the obesity index is evaluated after the onset of diabetes, not allowing to exclude a possible reverse causation. A study which included measurements of BMI before diabetes diagnosis in incident cases showed no evidence of the obesity paradox [74]. This study, referring to the participants of the Health Professionals Follow-up Study and Nurses’ Health Study cohorts, with follow-up of up to 36 years and 3083 deaths from all causes collectively, showed that there was a direct linear relationship between BMI and mortality, with the lowest mortality risk in the BMI class 22.5–24.9 kg/m2 [74].
Furthermore only once BMI detection may not describe an individual’s weight history [82, 84]. In a recent study, using a single BMI baseline measurement, a significant inverse association between overweight and mortality was observed; however this association was reversed taking in consideration the maximum BMI over 16 years of weight history [84].
The majority of the studies use BMI to classify obesity, but it is a measure of excess weight per height, that does not capture information on body fat distribution and fails to distinguish between fat and muscle mass. The use of other indices to define the distribution of adipose tissue, such as the waist circumference, the hip-to-waist ratio or the waist-to-height ratio could overcome the limits of BMI. The body fat distribution has indeed a greater influence on cardiometabolic risk than BMI: the visceral adipose tissue plays the most important role in development of obesity-associated metabolic disorders [85, 86]. To our knowledge, there is no demonstration of an obesity paradox based on a direct measurement of body fat. Bozorgmanesh et al. reported in a sample of 1322 new-onset diabetic patients the absence of obesity paradox after adjustment for waist and hip circumferences [87]; studies based only on the BMI may misrepresents some diabetic patients as “normal” when indeed excess visceral adiposity is present, predisposing to adverse cardiometabolic outcomes [88].
In this regard, low muscle mass has been independently associated with mortality [89] and in some cases a BMI corresponding to normal weight could actually hide a pathological condition known as sarcopenia, typical of the elderly, characterized by an excessive proportion of fat due to a loss of muscle tissue and associated with an adverse clinical outcome [90]. Therefore, it is possible that higher mortality in normal weight subjects could be associated primarily with muscle mass deficit and not low adiposity [91]. Moreover, recent researches have demonstrated that greater muscle strength (determined for example by the handgrip strength) predicts lower risk of mortality in both diabetic and not-diabetic subjects [92,93,94].
Therefore, studies regarding the obesity paradox should also take in account physical exercise and changes in body weight during the course of the disease because both can influence the mortality rate; Church et al. as well as Mc Auley et al. showed no significant association between BMI and mortality after adjustment for cardiorespiratory fitness in males with diabetes [95,96,97]. This observation was also supported by a recent study by Whelton et al. including 8528 patients with type 2 diabetes and stratified by cardiometabolic capacity: obesity paradox was present in patients with low or moderate fitness, while in patients with high cardiometabolic capacity there was no significant association between BMI and mortality [98].
Other possible limitations in the studies on the obesity paradox and T2DM may concern smoking status, age and associated treatments.
Preston and Stokes, observing the absence of the obesity paradox among non-smoking participants of their study, concluded that higher mortality in normal weight participants could be explained by the strong inverse correlation between obesity and smoking [99]. Some years later, Badrick et al. with a large population-based cohort study, estimating the Hazard Ratios (HRs) for the association of BMI with all-cause mortality, stratified by smoking status, reported the evidence of obesity paradox only in smokers, with and without T2DM, supporting the importance of smoking as a strong confounding factor [75].
Yano et al. observed the obesity paradox phenomenon in older populations with T2DM, but not younger ones [100]. Zoppini et al. found that in older patients (age ≥ 65 years) with T2DM, the highest BMI group (≥ 29.9 kg/m2) was associated with lowest all-cause mortality; by contrast, among patients < 65 years, the highest BMI category (≥ 30.9 kg/m2) had a higher mortality compared to patients in the lowest BMI quartile (≤ 25.4 kg/m2) [101]. It is possible that age is one of the most important confounding factor in some conditions [102].
Studies regarding subjects with overweight/obesity are frequently characterized by selection bias: in clinical practice, patients with obesity are considered to have a greater cardiovascular risk than normal weight peers, and they usually undergo screening tests (such as cardiac or blood vessel ultrasound), which could allow in some cases an earlier detection of some diseases and therefore their preventive treatment. Moreover, patients with T2DM and obesity are treated more aggressively from the early stages of the disease, with newer drugs, such as GLP-1 analogues or SGLT2 inhibitors, which have a protective role on cardiovascular risk; the use of these new drugs per se could be a bias [71, 103].
Finally, it is necessary to well characterize the associated pathologies; in fact patients with underweight could have severe concomitant diseases (such as cancers) which could explain their reduced body weight and their worse prognosis.
Considering the long list of confounding factors that can affect studies regarding the association between obesity and T2DM, Tobias and Manson, in a recent review, have concluded that the obesity paradox in T2DM is likely an artifact of biases, and once these are accounted for, it is evident that compared with normal body weight, excess body weight is associated with a greater mortality risk [104]. Similarly Lajous et al. have argued that the obesity paradox could be explained by a selection bias due to the stratification for the BMI and not for other unmeasured risk factors, such as lifestyle and genes [105]. In this regard, some authors have showed that lean subjects affected by T2DM have a greater genetic susceptibility with a major risk for diabetic complications and poor prognosis [106, 107].
Obesity paradox and weight loss interventions in T2DM patients
In clinical practice patients with overweight/obesity and diabetes are advised to lose weight in order to improve their health status [108]; this recommendation may be complicated by the concept of the obesity paradox and by the observation that unintentional weight loss appear to be associated with worse long-term survival in these patients [67]. Recently, a meta-analysis exploring the effect of weight change on all-cause mortality showed that, compared with a stable weight, weight loss was associated with an increased risk of all-cause mortality and cardiovascular disease mortality in overweight or obese adults with diabetes. However, from the same study it appeared that intentional weight loss was not associated with changes in all-cause mortality or cardiovascular disease mortality [109]. Therefore it could be important to discern between different types of weight loss: intentional or unintentional; the latter could depend by concomitant disease, which could predispose to a worse prognosis.
Aucott et al. [110] have highlighted that the effect of weight loss on all-cause mortality was different for the category of initial BMI: when the initial BMI was greater than 35 kg/m2, weight loss was associated with increased all-cause mortality, by the way, they cannot determine from their data if, in their population, the weight loss was intentional or not. Zamora et al. showing no benefit from the obesity paradox for diabetic patients with hearth failure, have suggested that in these patients weight reduction to improve metabolic control and other cardiovascular associated risks factors might be recommended [80]. Moreover some authors, recalling the results of the Look AHEAD [111] and other epidemiological studies [112] conclude that the controversial findings regarding obesity paradox should not change current clinical recommendation about the importance of weight loss in T2MD subjects with overweight or obesity [105, 113], confirming that, in these patients, weight loss may be a primary goal of treatment and it permits a sustained remission of T2DM [47, 114]. Furthermore, the high rates of remission of T2DM after bariatric surgery are well known. The Swedish Obese Subjects (SOS) study, a prospective, long-term trial involving a subgroup of 2.010 obese subjects who underwent bariatric surgery, shows that patients with T2DM at baseline, experience 72% of disease remission 2 years after surgical treatment and are protect by macrovascular complications as compared with not-surgical subjects [115]. The efficacy of bariatric surgery, also defined “metabolic surgery” is so much established that a BMI > 35 kg/m2 (and in some cases > 30 kg/m2) in a subject affected by T2DM represents an indication for surgical treatment [116].
Conclusion
Results from clinical studies regarding the possibility of the obesity paradox in patients with T2DM are controversial. The benefit of overweight/obesity in patients with type 2 diabetes, showed in some studies, may arise due to reverse causation and other confounding factors (smoking status, concomitant therapies, physical activity, low muscle mass). To better understand the possible role of the obesity paradox in subjects with T2DM, more adequate data analysis and more accurate methods of investigations are needed: performing randomized clinical control trials, considering larger samples with longer follow up and well characterizing the population characteristics (confounding factors, intentionality of weight loss, body composition and fat distribution). The results of the available studies must be interpreted cautiously and they should not change current clinical practice regarding weight management in patients with overweight or obesity and T2DM, remaining focused on practicing physical activity and eating in adequate manner in order to lose weight preserving lean mass and improving metabolic outcomes, quality of life and lifespan too.
What is already known on this subject?
-
The prevalence of T2DM is three to seven times higher in obese adults compared to normal-weight ones.
-
80% of T2DM patients are with overweight or obesity; the strong relationship between the two conditions led to the notion of “diabesity”.
-
Some studies, even in recent times, suggest that individuals with overweight/obesity and diabetes have lower mortality compared with normal weight subjects.
What does this study add?
-
Reports that in patients with T2DM, overweight and obesity are associated with a better prognosis than underweight or normal weight have numerous limitations due to their mainly retrospective nature and to numerous confounding factors, such as associated pathologies, antidiabetic treatments and lack of data about distribution of body fat or weight history.
-
The benefit of overweight/obesity in patients with T2DM showed in some studies may arise due to reverse causation and other confounding factors (smoking status, concomitant therapies, physical activity, low muscle mass).
-
Weight loss seems associated with an increased risk of all-cause mortality and cardiovascular disease mortality in T2DM subjects with overweight or obesity but intentional weight loss was not associated with changes in all-cause mortality or cardiovascular disease mortality.
-
Controversial findings regarding obesity paradox should not change current clinical recommendation about the importance of weight loss in T2MD subjects with overweight or obesity, confirming that, in these patients, weight loss preserving lean mass and improving metabolic outcomes remains the primary goal of treatment.
Data availability
Not applicable.
Code availability
Not applicable.
References
World Health Organization (2016) Global report on diabetes. https://apps.who.int/iris/bitstream/handle/10665/204871/9789241565257_eng.pdf?sequence=1&isAllowed=y. Accessed 12 June 2020.
Finucane MM, Stevens GA, Cowan MJ, Danaei G, Lin JK, Paciorek CJ, Singh GM, Gutierrez HR, Lu Y, Bahalim AN, Farzadfar F, Riley LM, Ezzati M, Global Burden of Metabolic Risk Factors of Chronic Diseases Collaborating Group (Body Mass Index) (2011) National, regional, and global trends in body-mass index since 1980: systematic analysis of health examination surveys and epidemiological studies with 960 country-years and 9.1 million participants. Lancet 377:557–567. https://doi.org/10.1016/S0140-6736(10)62037-5
Frühbeck G, Toplak H, Woodward E, Yumuk V, Maislos M, Oppert JM, Executive Committee of the European Association for the Study of Obesity (2013) Obesity: the gateway to ill health—an EASO position statement on a rising public health, clinical and scientific challenge in Europe. Obes Facts 6:117–120. https://doi.org/10.1159/000350627
World Health Organization. Obesity and Overweight: fact sheet. https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight. Accessed 12 June 2020.
Mokdad AH, Ford ES, Bowman BA, Dietz WH, Vinicor F, Bales VS, Marks JS (2003) Prevalence of obesity, diabetes, and obesity-related health risk factors. JAMA 289:76–79. https://doi.org/10.1001/jama.289.1.76
Hossain P, Kawar B, El Nahas M (2007) Obesity and diabetes in the developing world—a growing challenge. N Engl J Med 356:213–215. https://doi.org/10.1056/NEJMp068177
Centers for Disease Control and Prevention (2004) Prevalence of overweight and obesity among adults with diagnosed diabetes United States, 1988–1994 and 1999–2002. Morb Mortal Wkly Rep 53:1066–1068
Butler AE, Janson J, Bonner-Weir S, Ritzel R, Rizza RA, Butler PC (2003) Beta-cell deficit and increased beta-cell apoptosis in humans with type 2 diabetes. Diabetes 52:102–110. https://doi.org/10.2337/diabetes.52.1.102
Kahn SE, Hull RL, Utzschneider KM (2006) Mechanisms linking obesity to insulin resistance and type 2 diabetes. Nature 444:840–846. https://doi.org/10.1038/nature05482
Papaetis GS, Papakyriakou P, Panagiotou TN (2015) Central obesity, type 2 diabetes and insulin: exploring a pathway full of thorns. Arch Med Sci 11:463–482. https://doi.org/10.5114/aoms.2015.52350
Meigs JB, Rutter MK, Sullivan LM, Fox CS, D'Agostino RB Sr, Wilson PW (2007) Impact of insulin resistance on risk of type 2 diabetes and cardiovascular disease in people with metabolic syndrome. Diabetes Care 30:1219–1225. https://doi.org/10.2337/dc06-2484
Roden M, Price TB, Perseghin G, Petersen KF, Rothman DL, Cline GW, Shulman GI (1996) Mechanism of free fatty acid-induced insulin resistance in humans. J Clin Invest 97:2859–2865. https://doi.org/10.1172/JCI118742
Shulman GI (2000) Cellular mechanisms of insulin resistance. J Clin Invest 106:171–176. https://doi.org/10.1172/JCI10583
Hansen D, Dendale P, Beelen M, Jonkers RA, Mullens A, Corluy L, Meeusen R, van Loon LJ (2010) Plasma adipokine and inflammatory marker concentrations are altered in obese, as opposed to non-obese, type 2 diabetes patients. Eur J Appl Physiol 109:397–404. https://doi.org/10.1007/s00421-010-1362-5
Il’yasova D, Wang F, D’AgostinoRBJr, Hanley A, Wagenknecht LE, (2010) Prospective association between fasting NEFA and type 2 diabetes: impact of post-load glucose. Diabetologia 53:866–874. https://doi.org/10.1007/s00125-010-1657-4
Shoelson SE, Lee J, Goldfine AB (2006) Inflammation and insulin resistance. J Clin Invest 116:1793–1801. https://doi.org/10.1172/JCI29069
Bastard JP, Lagathu C, Caron M, Capeau J (2007) Point-counterpoint:interleukin-6 does/does not have a beneficial role in insulin sensitivity and glucose homeostasis. J Appl Physiol 102:821–822. https://doi.org/10.1152/japplphysiol.01353.2006
Kopp HP, Kopp CW, Festa A, Krzyzanowska K, Kriwanek S, Minar E, Roka R, Schernthaner G (2003) Impact of weight loss on inflammatory proteins and their association with the insulin resistance syndrome in morbidly obese patients. Arterioscler Thromb Vasc Biol 23:1042–1047. https://doi.org/10.1161/01.ATV.0000073313.16135.21
Hrnciar J, Avdicova M, Gabor D, Hrnciarova M, Chamulova M, Jakubikova K, Kaliska G, Kikova V, Kovar F, Kreze A Jr, Lepej J, Okapcova J, Szentivanyi M (2013) Prevalence of metabolic syndrome, insulin resistance, and microvascular angina pectoris in 500 consecutive patients referred to coronarography. Endocr Regul 47:33–38. https://doi.org/10.4149/endo_2013_01_33
Rotter V, Nagaev I, Smith U (2003) Interleukin-6 (IL-6) induces insulin resistance in 3T3-L1 adipocytes and is, like IL-8and tumor necrosis factor alpha, overexpressed in human fat cells from insulin resistant subjects. J Biol Chem 278:45777–45784. https://doi.org/10.1074/jbc.M301977200
Barnes KM, Miner JL (2009) Role of resistin in insulin sensitivity in rodents and humans. Curr Protein Pept Sci 10:96–107. https://doi.org/10.2174/138920309787315239
Janke J, Engeli S, Boschmann M, Adams F, Böhnke J, Luft FC, Sharma AM, Jordan J (2006) Retinol-binding protein 4 in human obesity. Diabetes 55:2805–2810. https://doi.org/10.2337/db06-0616
Graham TE, Yang Q, Blüher M, Hammarstedt A, Ciaraldi TP, Henry RR, Wason CJ, Oberbach A, Jansson PA, Smith U, Kahn BB (2006) Retinol binding protein 4 and insulin resistance in lean, obese, and diabetic subjects. N Engl J Med 354:2552–2563. https://doi.org/10.1056/NEJMoa054862
Askari H, Tykodi G, Liu J, Dagogo-Jack S (2010) Fasting plasmaleptin level is a surrogate measure of insulin sensitivity. J Clin Endocrinol Metab 95:3836–3843. https://doi.org/10.1210/jc.2010-0296
Martin SS, Qasim A, Reilly MP (2008) Leptin resistance: a possible interface of inflammation and metabolism in obesity-related cardiovascular disease. J Am Coll Cardiol 52:1201–1210. https://doi.org/10.1016/j.jacc.2008.05.060
Dunmore SJ, Brown JE (2013) The role of adipokines in beta-cell failure of type 2 diabetes. J Endocrinol 216:T37–45. https://doi.org/10.1530/JOE-12-0278
Rhodes CJ (2005) Type 2 diabetes-a matter of β-cell life and death? Science 307:380–384. https://doi.org/10.1126/science.1104345
Leahy JL, Hirsch IB, Peterson KA, Schneider D (2010) Targeting beta-cell function early in the course of therapy for type 2 diabetes mellitus. J Clin Endocrinol Metab 95:4206–4216. https://doi.org/10.1210/jc.2010-0668
Carpentier A, Mittelman SD, Lamarche B, Bergman RN, Giacca A, Lewis GF (1999) Acute enhancement of insulin secretion by FFA in humans is lost with prolonged FFA elevation. Am J Physiol 276:1055–1066. https://doi.org/10.1152/ajpendo.1999.276.6.E1055
Halban PA, Polonsky KS, Bowden DW, Hawkins MA, Ling C, Mather KJ, Powers AC, Rhodes CJ, Sussel L, Weir GC (2014) β-Cell failure in type 2 diabetes: postulated mechanisms and prospects for prevention and treatment. Diabetes Care 37:1751–1758. https://doi.org/10.1210/jc.2014-1425
Prentki M, Nolan CJ (2006) Islet beta cell failure in type 2 diabetes. J Clin Invest 116:1802–1812. https://doi.org/10.1172/JCI29103
Kahn SE, Zraika S, Utzschneider KM, Hull RL (2009) The beta cell lesion in type 2 diabetes: there has to be a primary functional abnormality. Diabetologia 52:1003–1012. https://doi.org/10.1007/s00125-009-1321-z
Wajchenberg BL (2007) beta-cell failure in diabetes and preservation by clinical treatment. Endocr Rev 28:187–218. https://doi.org/10.1210/10.1210/er.2006-0038
Cnop M, Landchild MJ, Vidal J, Havel PJ, Knowles NG, Carr DR, Wang F, Hull RL, Boyko EJ, Retzlaff BM, Walden CE, Knopp RH, Kahn SE (2002) The concurrent accumulation of intra-abdominal and subcutaneous fat explains the association between insulin resistance and plasma leptin concentrations: distinct metabolic effects of two fat compartments. Diabetes 51:1005–1015. https://doi.org/10.2337/diabetes.51.4.1005
Trouwborst I, Bowser SM, Goossens GH, Blaak EE (2018) Ectopic fat accumulation in distinct insulin resistant phenotypes; targets for personalized nutritional interventions. Front Nut 5:77. https://doi.org/10.3389/fnut.2018.00077
Shulman GI (2014) Ectopic fat in insulin resistance, dyslipidemia and cardiometabolic disease. N Engl J Med 371:1131–1141. https://doi.org/10.1056/NEJMra1011035
Snel M, Jonker JT, Schoones J, Lamb H, de Roos A, Pijl H, Smit JW, Meinders AE, Jazet IM (2012) Ectopic fat and insulin resistance: pathophysiology and effect of diet and lifestyle interventions. Int J Endocrinol. https://doi.org/10.1155/2012/983814
van der Kolk BW, Goossens GH, Jocken JW, Blaak EE (2016) Altered skeletal muscle fatty acid handling is associated with the degree of insulin resistance in overweight and obese humans. Diabetologia 59:2686–2696. https://doi.org/10.1007/s00125-016-4104-3
Stinkens R, Goossens GH, Jocken JW, Blaak EE (2015) Targeting fatty acid metabolism to improve glucose metabolism. Obes Rev 16:715–757. https://doi.org/10.1111/obr.12298
Bluher M (2010) The distinction of metabolically 'healthy' from 'unhealthy' obese individuals. Curr Opin Lipidol 21:38–43. https://doi.org/10.1097/MOL.0b013e3283346ccc
Gancheva S, Jelenik T, Álvarez-Hernández E, Roden M (2018) Interorgan metabolic crosstalk in human insulin resistance. Physiol Rev 98:1371–1415. https://doi.org/10.1152/physrev.00015.2017
Neel JV (1962) Diabetes mellitus: a “thrifty” genotype rendered detrimental by "progress"? Am J Hum Genet 14:353–362
Fuchsberger C, Flannick J, Teslovich TM et al (2016) The genetic architecture of type 2 diabetes. Nature 536:41–47. https://doi.org/10.1038/nature18642
Kahn SE, Cooper ME, Del Prato S (2014) Pathophysiology and treatment of type 2 diabetes: perspectives on the past, present and future. Lancet 383:1068–1083. https://doi.org/10.1016/S0140-6736(13)62154-6
Kolb H, Martin S (2017) Environmental/lifestyle factors in the pathogenesis and prevention of type 2 diabetes. BMC Med 15:131. https://doi.org/10.1186/s12916-017-0901-x
Hamman RF, Wing RR, Edelstein SL, Lachin JM, Bray GA, Delahanty L, Hoskin M, Kriska AM, Mayer-Davis EJ, Pi-Suny-er X, Regensteiner J, Venditti B, Wylie-Rosett J (2006) Effect of weight loss with lifestyle intervention on risk of diabetes. Diabetes Care 29:2102–2107. https://doi.org/10.2337/dc06-0560
Lean ME, Leslie WS, Barnes AC, Brosnahan N, Thom G, McCombie L, Peters C, Zhyzhneuskaya S, Al-Mrabeh A, Hollingsworth KG, Rodrigues AM, Rehackova L, Adamson AJ, Sniehotta FF, Mathers JC, Ross HM, McIlvenna Y, Stefanetti R, Trenell M, Welsh P, Kean S, Ford I, McConnachie A, Sattar N, Taylor R (2018) Primary care-led weight management for remission of type 2 diabetes (DiRECT): an open-label, cluster-randomised trial. Lancet 391:541–551. https://doi.org/10.1016/S0140-6736(17)33102-1
Logue J, Walker JJ, Leese G, Lindsay R, McKnight J, Morris A, Philip S, Wild S, Sattar N, on behalf of the Scottish Diabetes Research Network Epidemiology Group (2013) Association between BMI measured within a year after diagnosis of type 2 diabetes and mortality. Diabetes Care 36:887–893. https://doi.org/10.2337/dc12-0944
Thomas G, Khunti K, Curcin V, Molokhia M, Millett C, Majeed A, Paul S (2014) Obesity paradox in people newly diagnosed with type 2 diabetes with and without prior cardiovascular disease. Diabetes Obes Metab 16:317–325. https://doi.org/10.1111/dom.12217
Flegal KM, Kit BK, Orpana H, Graubard BI (2013) Association for all-cause mortality with overweight and obesity using standard body mass index categories: systematic review and meta-analysis. JAMA 309:71–82. https://doi.org/10.1001/jama.2012.113905
Hainer V, Aldhoon-Hainerova I (2013) Obesity paradox does exist. Diabetes Care 36:276–281. https://doi.org/10.2337/dcS13-2023
Standl E, Erbach M, Schnel O (2013) Defending the con side: obesity paradox does not exist. Diabetes Care 36:282–286. https://doi.org/10.2337/dcS13-2040
Bosello O, Donataccio MP (2013) Obesity paradox. Eat Weight Disord 18:447–448. https://doi.org/10.1007/s40519-013-0080-5
Bosello O, Donataccio MP, Cuzzolaro M (2016) Obesity or obesities? Controversies on the association between body mass index and premature mortality. Eat Weight Disord 21:165–174. https://doi.org/10.1007/s40519-016-0278-4
Doehner W, Schenkel J, Anke S, Springer J, Audebert H (2013) Overweight and obesity are associated with improved survival, functional outcomes, and stroke recurrence after acute stroke or transient ischaemic attack: observations from the TEMPiS trial. Eur Heart J 34:268–277. https://doi.org/10.1093/eurheartj/ehs340
Curtis JP, Selter JG, Wang Y, Rathore SS, Jovin IS, Jadbabaie F, Kosiborod M, Portnay EL, Sokol SI, Bader F, Krumholz HM (2005) The obesity paradox body mass index and outcomes in patients with heart failure. Arch Intern Med 165:55–56. https://doi.org/10.1001/archinte.165.1.55
Angerås O, Albertsson P, Karason K, Råmanddal T, Matejka G, James S, Lagervist B, Rosengren A, Omerovis E (2013) Evidence for obesity paradox in patients with acute coronary syndrome: a report from the Swedish Coronary Angiography and Angioplasty Registry. Eur Heart J 34:345–353. https://doi.org/10.1093/eurheartj/ehs217
Franz MJ (2013) The obesity paradox and diabetes. Diabetes Spectrum 26:145–151. https://doi.org/10.2337/diaspect.26.3.145
Carnethon MR, Rasmussen-Torvik LJ, Palaniappan L (2014) The obesity paradox in diabetes. Curr Cardiol Rep 16:446. https://doi.org/10.1007/s11886-013-0446-3
Forlivesi S, Cappellari M, Bonetti B (2020) Obesity paradox and stroke: a narrative review. Eat Weight Disord. https://doi.org/10.1007/s40519-020-00876-w
Anker SD, von Haehling S (2011) The obesity paradox in heart failure: accepting reality and making rational decisions. Clin Pharmacol Ther 90:188–190. https://doi.org/10.1038/clpt.2011.72
Prescott HC, Chang VW (2018) Overweight or obese BMI is associated with earlier, but not later survival after common acute illnesses. BMC Geriatr. https://doi.org/10.1186/s12877-018-0726-2
McEwen LN, Kim C, Karter AJ, Haan MN, Ghosh D, Llantz PM, Mangione CM, Thompson TJ, Herman WH (2007) Risk factors for mortality among patients with diabetes. Diabetes Care 30:1736–1741. https://doi.org/10.2337/dc07-0305
Kokkinos P, Myers J, Faselies C, Doumas M, Kheifbek R, Nylen E (2012) BMI-mortality paradox and fitness in African American and Caucasian men with type 2 diabetes. Diabetes Care 35:1021–1027. https://doi.org/10.2337/dc11-2407
Lin CC, Li CI, Liu CS, Lin WY, Lin CH, Chiang JI, Yang SY, Li TC (2019) Obesity paradox in associations between body mass index and diabetes-related hospitalization and mortality in patients with type 2 diabetes: retrospective cohort studies. Diabetes Metab 45:564–572. https://doi.org/10.1016/j.diabet.2019.02.007
Kuo JF, Hsieh YT, Mao IC, Lin SD, Tu ST, Hsieh MC (2015) The Association between body mass index and all-cause mortality in patients with type 2 diabetes mellitus. Medicine. https://doi.org/10.1097/MD.0000000000001398
Doehner W, Erdman E, Cairns R, Clark AL, Dormandy JA, Ferrannini E, Anker SD (2012) Inverse relation of body weight and weight change with mortality and morbidity in patients with type 2 diabetes and cardio-vascular co-morbidity: an analysis of the PROactive study population. Int J Cardiol 162:20–26. https://doi.org/10.1016/j.ijcard.2011.09.039
Pagidipati NJ, Zheng Y, Green JB, McGuire DK, Mentz RJ, Shah S, Aschner P, Delibasi T, Rodbard HW, Westerhout CM, Holman RR, Peterson ED, on behalf of the TECOS Study Group (2019) Association of obesity with cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease: Insights from TECOS. Am Heart J 219:47–57. https://doi.org/10.1016/j.ahj.2019.09.016
Park H, Lee HW, Yoo J, Lee HS, Nam HS, Kim YD, Heo JH (2019) Body mass index and prognosis in ischemic stroke patients with type 2 diabetes mellitus. Front Neurol 10:563. https://doi.org/10.3389/fneur.2019.00563
Mulnier HE, Seaman HE, Raleigh VS, Soedamah-Muthu SS, Colhoun HM, Lawrenson RA (2006) Mortality in people with type 2 diabetes in the UK. Diabet Med 23:516–521. https://doi.org/10.1111/j.1464-5491.2006.01838.x
Costanzo P, Cleland JG, Pellicori P, Clark AL, Hepburn D, Kilpatrick ES, Perrone-Filardi P, Zhang J, Atkin SL (2015) The obesity paradox in type 2 diabetes mellitus: relationship of body mass index to prognosis: a cohort study. Ann Intern Med 162:610–618. https://doi.org/10.7326/M14-1551
Zhao W, Katzmarzyk PT, Horswell R, Wang Y, Li W, Johnson J, Heymseld SB, Cefalu WT, Ryan DH, Hu G (2014) Body mass index and the risk of all-cause mortality among patients with type 2 diabetes mellitus. Circulation 130:2143–2151. https://doi.org/10.1161/CIRCULATIONAHA.114.009098
Lee EY, Lee YH, Yi SW, Shin SA, Yi JJ (2017) BMI and all-cause mortality in normoglycemia, impaired fasting glucose, newly diagnosed diabetes, and prevalent diabetes: a cohort study. Diabetes Care 40:1026–1033. https://doi.org/10.2337/dc16-1458
Tobias DK, Pan A, Jackson CL, O’Reilly EJ, Ding EL, Willett WC, Manson JE, Hu FB (2014) Body-mass index and mortality among adults with incident type-2 diabetes. N Engl J Med 370:233–244. https://doi.org/10.1056/NEJMoa1304501
Badrick E, Sperrin M, Buchan IE, Renehan AG (2017) Obesity paradox and mortality in adults with and without incident type 2 diabetes: a matched population-level cohort study. BMJ Open Diabetes Res Care 10:5. https://doi.org/10.1136/bmjdrc-2016-000369
Zahir SF, Griffin A, Veerman JL, MaglianoDJ SJE, Cao KL, Mehdi AM (2019) Exploring the association between BMI and mortality in australian women and men with and without diabetes: the ausdiab study. Diabetologia 62:754–758. https://doi.org/10.1007/s00125-019-4830-4
Tate J, Knuiman M, Davis WA, Davis TME, Bruce DG (2019) A comparison of obesity indices in relation to mortality in type 2 diabetes: the Fremantle Diabetes Study. Diabetologia 63:528–536. https://doi.org/10.1007/s00125-019-05057-8
Eeg-Olofsson K, Cederholm J, Nilsson PM, Zethelius B, Nunez L, Gudbjörnsdóttir S, Eliasson B (2009) Overweight, obesity and cardiovascular diseases and mortality in type 2 diabetes: an observational study in 13,087 patients. Diabetologia 52:65–73. https://doi.org/10.1007/s00125-008-1190-x
Adamopoulos C, Meyer P, Desai RV, Karatzidou K, Ovalle F, White M, Aban I, Love TE, Deedwania P, Anker SD, Ahmed A (2011) Absence of obesity paradox in patients with chronic hearth failure and diabetes mellitus: a propensity-matched study. Eur J Hearth Fail 13:200–206. https://doi.org/10.1093/eurjhf/hfq159
Zamora E, Lupón J, Enjuanes C, Pascual-Figal D, de Antonio M, Domingo M, Comín-Colet J, Vila J, Peñafiel J, Farré N, Alonso N, Santesmases J, Troya M, Bayés-Genís A (2016) No benefit from the obesity paradox for diabetic patients with hearth failure. Eur J Hearth Fail 18:851–858. https://doi.org/10.1002/ejhf.576
Kwon Y, Kim HJ, Park S, Park YG, Cho KH (2017) Body mass index-related mortality in patients with type 2 diabetes and heterogeneity in obesity paradox studies: a dose-response meta-analysis. PLoS ONE 3:12. https://doi.org/10.1371/journal.pone.0168247
Han SJ, Boyko EJ (2018) The evidence for an obesity paradox in type 2 diabetes mellitus. Diabetes Metab J 42:179–187. https://doi.org/10.4093/dmj.2018.0055
Jong CB, Li HY, Pan SL, Hsieh MY, Su FY, Chen KC, Yin WH, Chan SH, Wu YW, Wang KY, Chang KC, Hwang JJ, Wu CC (2019) Relationship between body mass index, antidiabetic agents and midterm mortality in patients with both type 2 diabetes mellitus and acute coronary syndrome. J Am Heart Assoc. https://doi.org/10.1161/JAHA.118.011215
Yu E, Ley SH, Manson JE, Willett W, Satija A, Hu FB, Stokes A (2017) Weight history and all cause and cause-specific mortality in three prospective cohort studies. Ann Intern Med 166:613–620. https://doi.org/10.7326/M16-1390
Neeland IJ, TurerAT ACR, Berry JD, Rohatgi A, Das SR, Khera A, Vega GL, McGuire DK, Grundy SM, de Lemos JA (2015) Body fat distribution and incident cardiovascular disease in obese adults. J Am Coll Cardiol 65:2150–2151. https://doi.org/10.1016/j.jacc.2015.01.061
Hayashi T, Boyko EJ, McNeely MJ, Leonetti DL, Kahn SE, Fujimoto WY (2008) Visceral adiposity, not abdominal subcutaneous fat area, is associated with an increase in future insulin resistance in Japanese Americans. Diabetes 57:1269–1275. https://doi.org/10.2337/db07-1378
Bozorgmanesh M, Arshi B, Sheikholeslami F, Azizi F, Hadaegh F (2014) No obesity paradox-BMI incapable of adequately capturing the relation of obesity with all-cause mortality: an inception diabetes cohort study. Int J Endocrinol. https://doi.org/10.1155/2014/282089
Lim S, Meigs JB (2013) Ectopic fat and cardiometabolic and vascular risk. Int J Cardiol 169:166–176. https://doi.org/10.1016/j.ijcard.2013.08.077
Kim JH, Lim S, Choi SH, Kim KM, Yoon JW, Kim KW, Lim JY, Park KS, Jang HC (2014) Sarcopenia: an independent predictor of mortality in community-dwelling older Korean men. J Gerontol A Biol Sci Med Sci 69:1244–1252. https://doi.org/10.1093/gerona/glu050
Marzetti E, Calvani R, Tosato M, Cesari M, Di Bari M, Cherubini A, Collamati A, D'Angelo E, Pahor M, Bernabei R, Landi F, SPRINTT Consortium (2017) Sarcopenia: an overview. Aging Clin Exp Res 29:11–17. https://doi.org/10.1007/s40520-016-0704-5
Batsis JA, Mackenzie TA, Emeny RT, Lopez-Jimenez F, Bartels SJ (2017) Low lean mass with and without obesity, and mortality: results from the 1999–2004 National Health and Nutrition Ex-amination Survey. J Gerontol A Biol Sci Med Sci 72:1445–1451. https://doi.org/10.1093/gerona/glx002
Rantanen T, Harris T, Leveille SG, Visser M, Foley D, Masaki K, Guralnik JM (2000) Muscle strength and body mass index as long-term predictors of mortality in initially healthy men. J Gerontol A Biol Sci Med Sci 55:M168–M173. https://doi.org/10.1093/gerona/55.3.m168
Leong DP, Teo KK, Rangarajan S, Lopez-Jaramillo P, Avezum A Jr, Orlandini A, Seron P, Ahmed SH, Rosengren A, Kelishadi R, Rahman O, Swaminathan S, Iqbal R, Gupta R, Lear SA, OguzA YK, Zatonska K, Chifamba J, Igumbor E, Mohan V, Anjana RM, Gu H, Li W, Yusuf S, Prospective Urban Rural Epidemiology (PURE) Study investigators (2015) Prognostic value of grip strength: findings from the prospective urban rural epidemiology (PURE) study. Lancet 386:266–273. https://doi.org/10.1016/S0140-6736(14)62000-6
Hamasaki H, Kawashima Y, Katsuyama H, Sako A, Goto A, Yanai H (2017) Association of handgrip strength with hospitalization, cardiovascular events, and mortality in Japanese patients with type 2 diabetes. Sci Rep 7:7041. https://doi.org/10.1038/s41598-017-07438-8
Church TS, Cheng YJ, Earnest CP, Barlow CE, Gibbons LW, Priest EL, Blair SN (2004) Exercise capacity and body composition as predictors of mortality among men with diabetes. Diabetes Care 27:83–88. https://doi.org/10.2337/diacare.27.1.83
McAuley PA, Myers JN, Abella JP, Tan SY, Froelicher VF (2007) Exercise capacity and body mass as predictors of mortality among male veterans with type 2 diabetes. Diabetes Care 30:1539–1543. https://doi.org/10.2337/dc06-2397
McAuley PA, Kokkinos PF, Oliveira RB, Emerson BT, Myers JN (2010) Obesity paradox and cardiorespiratory fitness in 12,417 male veterans aged 40 to 70 years. Mayo Clin Proc 85:115–121
Whelton SP, McAuley PA, Dardari Z, Orimoloye OA, Brawner CA, Ehrman JK, Keteyian SJ, Al-Mallah M, Blaha MJ (2020) Association of BMI, fitness, and mortality in patients with diabetes: evaluating the obesity paradox in the Henry Ford Exercise Testing Project (FIT Project) cohort. Diabetes Care 43:677–682. https://doi.org/10.2337/dc19-1673
Preston SH, Stokes A (2014) Obesity paradox: conditioning on disease enhances biases in estimating the mortality risks of obesity. Epidemiology 25:454–461. https://doi.org/10.1097/EDE.0000000000000075
Yano Y, Kario K, Ishikawa S, Ojima T, Gotoh T, Kayaba K, Tsutsumi A, Shimada K, Nakamura Y, Kjii E (2013) Associations between diabetes, leanness, and the risk of death in the Japanese general population: the Jichi Medical School Cohort Study. Diabetes Care 36:1186–1192. https://doi.org/10.2337/dc12-1736
Zoppini G, Verlato G, Leuzinger C, Zamboni C, Brun E, Bonora E, Muggeo M (2003) Body mass index and the risk of mortality in type II diabetic patients from Verona. Int J Obes Relat Metab Disord 27:281–285. https://doi.org/10.1038/sj.ijo.802199
Femminò S, Pagliaro P, Penna C (2020) Obesity and cardioprotection. Curr Med Chem 27:230–239. https://doi.org/10.2174/0929867326666190325094453
Jamieson A, Finer N (2017) Can we reconcile 'the obesity paradox' with recent cardiovascular outcome trials in diabetes? Clin Obes 7:255–259. https://doi.org/10.1111/cob.12217
Tobias DK, Manson JE (2018) The obesity paradox in type 2 diabetes and mortality. Am J Lifestyle Med 12:244–251. https://doi.org/10.1177/1559827616650415
Lajous M, Bijon A, Fagherazzi G, Boutron-Ruault MC, Balkau B, Clavel-Chapelon F, Hernán MA (2014) Body mass index, diabetes, and mortality in French women: explaining away a “paradox”. Epidemiology 25:10–14. https://doi.org/10.1097/EDE.0000000000000031
Carnethon MR, de Chavez PJ, Biggs ML, Lewis CE, Pankow JS, Bertoni AG, Golden SH, Liu K, Mukamal KJ, Campbell-Jenkins B, Dyer AR (2012) Association of weight status with mortality in adults with incident diabetes. JAMA 308:581–590. https://doi.org/10.1001/jama.2012.928
Monami M, Cremasco F, Lamanna C, Colombi C, Desideri CM, Iacomelli I, Marchionni N, Mannucci E (2011) Glucagon-like peptide-1 receptor agonists and cardiovascular events: a meta-analysis of randomized clinical trials. Exp Diabetes Res. https://doi.org/10.1155/2011/215764
Look AHEAD Research Group1, Pi-Sunyer X, Blackburn G, Brancati FL, Bray GA, Bright R, Clark JM, Curtis JM, Espeland MA, Foreyt JP, Graves K, Haffner SM, Harrison B, Hill JO, Horton ES, Jakicic J, Jeffery RW, Johnson KC, Kahn S, Kelley DE, Kitabchi AE, Knowler WC, Lewis CE, Maschak-Carey BJ, Montgomery B, Nathan DM, Patricio J, Peters A, Redmon JB, Reeves RS, Ryan DH, Safford M, Van Dorsten B, Wadden TA, Wagenknecht L, Wesche-Thobaben J, Wing RR, Yanovski SZ (2007) Reduction in weight and cardiovascular disease risk factors in individuals with type 2 diabetes: one-year results of the look AHEAD trial. Diabetes Care 30:1374–1383. https://doi.org/10.2337/dc07-0048
Chen Y, Yang X, Wang J, Li Y, Ying D, Yuan H (2018) Weight loss increases all cause mortality in overweight or obese patients with diabetes. Medicine. https://doi.org/10.1097/MD.0000000000012075
Aucott LS, Philip S, Avenell A, Afolabi E, Sattar N, Wild S, on behalf of the Scottish Diabetes Research Network Epidemiology Group (2018) Patterns of weight change after the diagnosis of type 2 diabetes in Scotland and their relationship with glycaemic control, mortality and cardiovascular outcomes: a retrospective cohort study. BMJ. https://doi.org/10.1136/bmjopen-2015-010836
Look AHEAD Research Group, Wing RR, Bolin P, Brancati FL, Bray GA, Clark JM, Coday M, Crow RS, Curtis JM, Egan CM, Espeland MA, Evans M, Foreyt JP, Ghazarian S, Gregg EW, Harrison B, Hazuda HP, Hill JO, Horton ES, Hubbard VS, Jakicic JM, Jeffery RW, Johnson KC, Kahn SE, Kitabchi AE, Knowler WC, Lewis CE, Maschak-Carey BJ, Montez MG, Murillo A, Nathan DM, Patricio J, Peters A, Pi-Sunyer X, Pownall H, Reboussin D, Regensteiner JG, Rickman AD, Ryan DH, Safford M, Wadden TA, Wagenknecht LE, West DS, Williamson DF, Yanovski SZ (2013) Cardiovascular effects of intensive lifestyle intervention in type 2 diabetes. N Engl J Med 369:145–154. https://doi.org/10.1056/NEJMoa1212914
Ma C, Avenell A, Bolland M, Hudson J, Stewart F, Robertson C, Sharma P, Fraser C, MacLennan G (2017) Effects of weight loss interventions for adults who are obese on mortality, cardiovascular disease, and cancer: systematic review and meta-analysis. BMJ. https://doi.org/10.1136/bmj.j4849
Lean MEJ, Leslie WS, Barnes AC, Brosnahan N, Thom G, McCombie L, Peters C, Zhyzhneuskaya S, Al-Mrabeh A, Hollingsworth KG, Rodrigues AM, Rehackova L, Adamson AJ, Sniehotta FF, Mathers JC, Ross HM, McIlvenna Y, Welsh P, Kean S, Ford I, McConnachie A, Messow CM, Sattar N, Taylor R (2019) Durability of a primary care-led weight-management intervention for remission of type 2 diabetes: 2-year results of the DiRECT open-label, cluster-randomised trial. Lancet Diabetes Endocrinol 7:344–355. https://doi.org/10.1016/S2213-8587(19)30068-3
Lajous M, Banack HR, Kaufman JS, Hernan MA (2015) Should patients with chronic disease be told to gain weight? The obesity paradox and selection bias. Am J Med 128:334–336. https://doi.org/10.1016/j.amjmed.2014.10.043
Sjöström L (2013) Review of the key results from the Swedish Obese Subjects (SOS) trial—a prospective controlled intervention study of bariatric surgery. J Intern Med 273:219–234. https://doi.org/10.1111/joim.12012
Fried M, Yumuk V, Oppert JM, Scopinaro N, Torres A, Weiner R, Yashkov Y, Frühbeck G, International Federation for Surgery of Obesity and Metabolic Disorders-European Chapter (IFSO-EC), European Association for the Study of Obesity (EASO), European Association for the Study of Obesity Obesity Management Task Force (EASO OMTF) (2014) Interdisciplinary European guidelines on metabolic and bariatric surgery. Obes Surg 24:42–55. https://doi.org/10.1007/s11695-013-1079-8
Funding
None.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
For this type of study formal consent is not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Obesity Paradox.
Rights and permissions
About this article

Cite this article
Gravina, G., Ferrari, F. & Nebbiai, G. The obesity paradox and diabetes. Eat Weight Disord 26, 1057–1068 (2021). https://doi.org/10.1007/s40519-020-01015-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40519-020-01015-1