
Abstract
Purpose
This study aims to evaluate and compare the scores of a self-reported measurement of orthorexia nervosa among Turkish people who engage in different levels of physical activity (sedentary individuals, recreational athletes and competitive athletes).
Methods
Data for this study were collected through a self-administered online questionnaire between March and April 2020 in Turkey. The questionnaire consisted of two parts: personal information (sociodemographic and anthropometric information, training and dieting regime) and the ORTO-11 Scale. Only the items in the revised scale (ORTO-R) were used for analysis. Measurement invariance was tested and latent means were compared across different activity groups, sexes and levels of education.
Results
Analysis was done with a total of 877 participants (514 sedentary, 271 recreationally active, and 91 competitive athletes). Mean age of participants was 29.12 ± 11.15. Sedentary people were less likely to follow a particular diet. Configural, metric and partial scalar invariance were proven across three groups of physical activity and the difference between latent means was found nonsignificant (competitive vs sedentary: CR = − 0.53, p = 0.592; competitive vs recreational: CR = 0.25, p = 0.724; sedentary vs. recreational: CR = − 1.35, p = 0.183). Configural, metric and full scalar invariance were proven across sexes and different levels of education, and difference between latent means was found nonsignificant (CR = − 1,11, p = 0.272; CR = − 0.53, p = 0.587, respectively).
Conclusion
In conclusion, people who compete at sports events, exercise regularly at a recreational level, or lead a sedentary life have similar scores in ORTO-R. Also, females did not score higher than males.
Level of evidence
Level III, case-control analytic study.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Eating disorders, as classified in Diagnostic and Statistical Manual of Mental Disorders-V (DSM-V) are limited to anorexia nervosa, bulimia nervosa, binge eating disorder and other specified feeding or eating disorder [1]. However, this classification is criticized for being a poor reflection of clinical reality [2]. Although not included in the DSM-V and International Classification of Disease-10 (ICD-10), orthorexia nervosa (ON) describes a pathological fixation on healthy eating, a concept introduced by Bratman in 1997 [3]. The term “ortho” means “proper, correct” and it refers to the obsession of eating proper food. There is an ongoing debate regarding the diagnostic criteria of ON. Nevertheless, there are two main features of ON diagnosis: (a) an obsessive focus on “healthy” eating and (b) clinically impairing compulsive behavior and mental preoccupation [4, 5]. First criterion describes extreme emotional distress with feelings of anxiety and shame following a violation of the diet, compulsive behavior and/or mental preoccupation regarding affirmative and restrictive dietary practices believed by the individual to promote optimum health, and growing dietary restrictions over time. The second criterion may manifest itself as the following: malnutrition; impairment of social, academic or vocational functioning and feeling of self-worth excessively dependent on compliance with self-defined “healthy” eating behavior [4]. Some other unique features of ON are avoidance of foods contaminated with additives, toxic compounds, or large quantities of fat, salt, sugar or other unhealthy ingredients, and an undue emphasis on food processing methods and storage products [6].
In general, athletes are under high risk of eating disorders. When examined for eating disorders criteria in DSM-IV, 13.5% of athletes suffered from subclinical or clinical eating disorders [7]. The highest prevalence of eating disorders was observed among female athletes who performed aesthetic sports (42%), but male athletes also have higher rates of eating disorders than non-athlete peers [7]. Studies on ON among athletes are also growing in number. Reports show that Italian female athletes had a higher tendency for orthorexic behavior than non-athletes. However, this difference was not prevalent between male athletes and non-athletes [8]. Swedish exercise science students had higher tendency of ON compared to business school students [9]. Also, Swedish female fitness center participants who exercised more frequently had higher scores on Bratman’s Orthorexia Test [10]. Clifford et al. reported that athletes who exercise more than 10 h a week scored lower in ORTO-15 than those who exercised less than 10 h a week [11]. Among university students from the USA, ON was related to the time spent doing strength-training exercises for men, and aerobic exercises for women [12]. One study from Hungary found statistically significant difference in ORTO-15 scores of people that engage in different levels of physical activity. Albeit the statistical significance, the clinical significance of this finding is doubtful as the mean scores were different only by 0.4 between the highest and the lowest activity group [13]. Another study examined the student-athletes in the United Kingdom and in contrast to the findings of the abovementioned studies, they reported that athletes did not have a higher tendency of ON compared to non-athlete students [11].
There are contradictory findings in the literature regarding athletes and ON. Therefore, this study aims to evaluate and compare the scores of a self-reported measurement of orthorexia nervosa among Turkish people with different levels of sports engagement, namely sedentary individuals, recreationally active people and competitive athletes.
Methods
Data collection
Data for this cross-sectional study were collected through a self-administered online questionnaire between March and April 2020. The study was announced via social media accounts, web sites and relevant forum pages, with special focus on reaching the athletic population. The questionnaire consisted of two parts: personal information (demographics, body weight, height, education level, employment status, presence of any chronic diseases, exercising frequency and duration, sports branch, having participated in a national/international sports competition as an athlete in the last year, following any particular diet) and the ORTO-11 Scale. Participants who had a chronic disease were excluded from the analysis as it may alter their dietary behavior. The following options were given when participants’ dietary habits were questioned: Alkaline diet, diabetic diet, high protein diet, intermittent fasting, low-calorie diet, low-carbohydrate diet, low-fat–low-cholesterol diet, Mediterranean diet, salt-restricted diet, vegan–vegetarian–pescetarian diet, other. More than one option could be marked.
The dataset generated and analyzed during the current study is available in the Mendeley repository [14].
ORTO-11 and ORTO-R Scales
ORTO-15 was developed by Donini et al. as a valid self-assessment tool for ON [15] and its cultural adaptation to Turkish was made by Arusoğlu et al. [16]. Four items which had smaller factor loadings than 0.50 were removed from the scale in the Turkish adaptation. Therefore, the Turkish adaptation of the ORTO-15 is referred to as ORTO-11. Cronbach α coefficient of ORTO-11 is 0.62, which denotes acceptable internal consistency [16]. ORTO-11 consists of 11 items, and each item is rated on a Likert scale of 4 points. Individuals are asked to respond using the phrases “always, often, sometimes, never” to represent how much they agreed with those phrases. All items except for item 6 are scored as follows: always 1, often 2, sometimes 3, and never 4. Item 6 is scored reversely. Lower scores indicate a higher tendency towards orthorexia nervosa. Validity study of the ORTO-11 was done with participants between the ages 19 and 66. Therefore, the population of the current study is limited to the same age range.
There are several national adaptations of ORTO-15 which contain a different set of items due to its unstable factorial structure across different populations. Therefore, Rogoza and Donini suggest using the revised version of ORTO-15 (ORTO-R) instead [17]. Revised scale consists of only six items and allows cross-national comparisons. As ORTO-R overcomes some of the main limitations of ORTO-15, in our study although participants have completed the full ORTO-11, we have analyzed the six items suggested by Rogoza and Donini, and reported our main outcome as ORTO-R score [17].
Participants
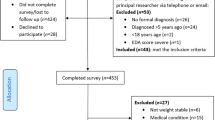
A total of 928 participants were enrolled in the study, 51 of which were later excluded as they declared having a chronic disease which may affect their dietary behaviors. Analysis was conducted with 877 questionnaires. Descriptive characteristics of participants are summarized in Table 1. Among the total of 877 participants, 514 were sedentary, 271 were recreationally active and 91 were competitive athletes. The youngest participant was 19 years old and the oldest was 66. The non-sedentary participants in the study practised a variety of sports disciplines. The number of participants from each discipline is given in Table 2.
Data analysis
Individuals from varying levels of physical activity were included in the study; later they were grouped as “sedentary”, “recreationally active” and “competitive athlete” for analysis. The competitive athlete group consisted of participants who took part in a national or international competition in the last year. The sedentary group consisted of participants who declared doing no exercise at all, or exercise only 1–2 days a week, for less than half an hour. All remaining participants were considered recreationally active.
Descriptive analysis was performed for demographic characteristics, training regime and diet preferences of participants. Differences between groups in age and BMI were compared with analysis of variance test. For categorical variables such as sex, level of education and employment status, differences between groups were analyzed with chi-square test.
For analysis of ORTO-R scores, a confirmatory factor analysis (CFA) was performed. Model fit was assessed using Chi-square (χ2), p value, degree of freedom (df), comparative fix index (CFI), Tucker–Lewis index (TLI), root mean square error of approximation (RMSEA), standardized root mean square residual (SRMR), weighted root mean square residual (WRMR) and relative non-centrality index (RNI). Cutoff values of fit indices were accepted as follows: CFI, TLI and RNI > 0.90; RMSEA and SRMR < 0.08 and WRMR < 1 [18,19,20]. Coefficient omega is reported as a measurement of reliability [21].
The model was tested for measurement invariance (MI) across groups using multi-group CFA, hierarchically. When testing for the configural invariance, loadings and intercepts were estimated freely. Metric (weak) invariance was tested only when configural invariance was supported. All factor loadings were constrained when testing for metric invariance. Later, scalar (strong) invariance was tested by constraining both the loadings and the intercepts. When full scalar invariance was not supported, partial invariance was tested. Then latent means were compared using the critical value (CR) which is calculated by dividing parameter estimate by its standard error. A CR value > 1.96 is considered statistically significant [19].
Analysis of variance and chi-square tests were used to compare the sociodemographic and anthropometric characteristics across groups. A Chi-square test of independence test was performed to analyze the relation between diet behavior and activity status. A p value < 0.05 was considered significant. All analyses were done with R Software 3.6.2 [22].
Results
Age, sex, body mass index, level of education and employment status of participants were compared across three groups of activity levels. Differences between age, BMI and employment status were nonsignificant. However, the distribution of sex and education level of participants among groups had significant differences, as shown in Table 1.
Dietary habits of participants
Seventy-eight percent of the sedentary (n = 402), 64.13% of competitive athletes (n = 59) and 59.41% of the recreationally active (n = 161) did not follow any particular diet. The remaining of the participants followed at least one diet. A chi-square test of independence was performed to examine the relationship between diet behavior (no diet vs. at least one diet) and activity status. The relation between these variables was significant, χ2 (2, 877) = 32.71, p < 0.001. Sedentary people were less likely to follow a diet. Diet preferences of participants who follow a specified diet are visualized in Fig. 1.

Diet preferences of participants (sum of percentages exceed 100 because some athletes started following more than one diet.)
ORTO-R scores
First, we tested a single-factor model’s fit to our data. Data fitted poorly to the single-factor model [χ2(9) = 81.133, p < 0.001, CFI = 0.944, TLI = 0.906, RMSEA = 0.096 [0.077, 0.115], RNI = 0.944, WRMR = 1.56, SRMR = 0.066]. Later, we added a method factor to the three items that Rogoza and Donini had suggested [17]. The introduction of the method factor has improved the model fit to an acceptable level [(χ2(5) = 30.514, p < 0.001, CFI = 0.980, TLI = 0.940, RMSEA = 0.076 [0.052, 0.103], RNI = 0.980, WRMR = 0.962, SRMR = 0.045]. The omega coefficient showed that measurement of the ORTO-R was reliable (ω = 0.72). Although further analysis reported below was run with the second model, we provide the measurement invariance test results of the first model as wellFootnote 1.
Table 3 displays the results for measurement invariance tests of ORTO-R across activity groups, sex, and education levels. Invariance tests showed that the configural invariance model across activity groups had an acceptable model fit. When factor loadings were constrained to test for metric invariance, model fit was still acceptable and the change in CFI was below 0.01. Having supported metric invariance, scalar invariance was tested. However, full scalar invariance was not supported across groups. Therefore, partial invariance was tested by setting “item 3” to vary. When item 3 was freed, we failed the Lagrange Multiplier test (p = 0.502) and ΔCFI remained lower than 0.01. Having established partial invariance across groups, we proceeded by comparing the latent means. Neither the difference between the latent means of competitive athletes and sedentary individuals nor between competitive athletes and recreationally active was significant (CR = − 0.53, p = 0.592; CR = 0.25, p = 0.724). The difference between the latent means of sedentary and recreational athletes was also nonsignificant (CR = − 1.35, p = 0.183).
Later, invariance was tested across sexes and education levels. Configural invariance model fit indices across sexes were acceptable other than RMSEA (0.093). Kenny et al. suggest that in models with a small degree of freedom, RMSEA often falsely indicates a poor fitting model and recommend not computing RMSEA for small df models. In the configural invariance model across sexes, the df is 10. Model fit was accepted based on the paper of Kenny et al. [23]. Consequently, metric invariance was tested by constraining the factor loadings. Model fit was acceptable and ΔCFI was smaller than 0.01. Further, the intercepts were constrained to check for scalar invariance. Full scalar invariance was also proven. Having full scalar invariance, latent means were compared between sexes. The difference between latent means across sexes was nonsignificant (CR = − 1.11, p = 0.272).
Finally, invariance tests were done across two levels of education. Configural, metric and full scalar invariance were supported. Latent means were compared across two levels of education and the difference was nonsignificant (CR = − 0.53, p = 0.587).
Mean ORTO-R scores of participants are given in Table 4.
Discussion
This study evaluated the ORTO-R scores of people with different levels of sports engagement. Contradictory to many studies in the literature that report a higher tendency of ON among athletes [8,9,10,11,12,13], we found no difference between the ORTO-R scores of people who engage in different levels of physical activity. The clinical importance of the very small but statistically significant differences in ORTO-15 scores is particularly important when interpreting the abovementioned studies. Several studies use cut-off values and compare the prevalence of ON between athletic and non-athletic populations [9, 24], which is an arguable method considering the low capability of ORTO-15 scores in measuring prevalence [25]. In support of our findings, a study of UK student-athletes reported no significant difference between the ORTO-15 scores of athletes and non-athletes [11]. Also, a larger study conducted with Italian athletes found that male athletes and controls scored similarly in ORTO-15 (37.2 ± 4.3 vs. 37.7 ± 3.4, p = 0.124), whereas female athletes scored lower than non-athletes (36.7 ± 4.2 vs. 38.4 ± 3.9) [8]. One study found a significant positive correlation between exercise addiction and orthorexia nervosa among German fitness club members [26]. When connecting ON to exercise, it may be important to differentiate high levels of physical activity from exercise addiction. Indeed, when the motivational background of ON was studied, it was revealed that obsessive features of sport activities such as guilt over skipping training, counting calories during training played an important role in ON [27]. Like many other studies, our study lacks the distinction between level of physical activity and exercise addiction.
Although there are contradictory findings regarding the relationship between orthorexic behavior and exercise, there is enough evidence to suggest that any hypothetical relationship between the two entities is far from being as strong as the connection between other eating disorders and sports participation. For example, anorexia nervosa prevalence of adolescent athletes is almost 3 times higher than controls (7.0% vs. 2.3%) [28]. The prevalence of eating disorders diagnosed according to DSM-IV is more than twofold higher in female athletes than controls (20% in athletes vs 9% in controls) and 16-fold higher in male athletes (8% in athletes vs 0.5% in controls) [7].
Only 35.87% of the competitive athletes in our study followed a diet regime. This rate is lower than the reports of Pelly et al., who stated that 62% of athletes who competed in Delhi 2010 Commonwealth Games followed at least one diet [29]. Sedentary people in the current study were less likely to follow a specific diet and their preferred diet regimes were different from that of the recreational and competitive athletes. High-protein and low-carbohydrate diets were the two most commonly preferred diets by recreationally active people, whereas sedentary individuals followed a low-calorie and a low-fat, low-cholesterol diet more commonly. Interestingly, the most common diet regime followed by competitive athletes was a vegetarian/vegan diet (also including pescatarian and reducetarian diets) in our study. Although it was not the most preferred diet, the total of the vegetarian diet rate and the rate of athletes who avoid red meat in the aforementioned study also reached 20% [29]. Another study also reported that vegetarian/vegan/pescatarian diet was the most common diet (28.0%) among marathon finishers who followed a specific diet over the past year [30]. In terms of orthorexia and veganism/vegetarianism, a study that particularly examined this relationship found that the vegans/vegetarians' attitudes towards eating did not have a tendency towards orthorexia as adopting veganism/vegetarianism is predominantly due to ethical reasons and is not associated with an obsession of healthy eating [31]. Another study also reported the highest (less pathological) mean ORTO-15 score among those who followed a vegan diet [32].
Whether there are any sex differences in orthorexia nervosa has not yet been fully revealed. Several studies reported no difference between sexes [32,33,34,35,36,37] while some others have stated males to be under higher risk [38]. In fact, one study reported that ON rate of females was higher than males when the cut-off value of 35 is applied and vice versa when the cut-off value of 40 is applied [39]. Our study results showed no significant difference between sexes regarding ORTO-R scores. In contrast to other eating disorders, in terms of ON, men seem to be at risk as much as women.
There are several limitations to this study. First of all, the number of competitive athletes is smaller than the number of recreationally active and sedentary participants. Second, distribution of gender and education level of participants is not even. Although the study aimed only to compare participants’ ORTO,-R scores across different activity levels, we have compared between sexes and education levels as well. As we have found out that latent mean differences between male and female, or high and low education levels were nonsignificant, we believe that the uneven distribution of these parameters doesn’t affect the reliability of our findings. ORTO-15 scale is translated into several languages and unfortunately different versions contain different set of items. This makes cross-cultural comparisons very difficult. The fact that participants completed different scales should be kept in mind when comparing the results of two countries such as the United Kingdom and Italy as we have mentioned in the introduction and discussion [8, 11]. Also, there are criticisms in the literature that ORTO-15 is not very sensitive when distinguishing between healthy eating behavior and healthy eating obsession [8, 40]. This criticism is based on very high rates of ON reported in the literature, when evaluated with ORTO-15. In the current study, we utilized ORTO-R instead of ORTO-15, we did not apply any cut-off values and did not define any participants as ON according to their ORTO-R scores. Therefore, we do not report a prevalence rate either. Instead, the scores were used only for comparisons between groups. We are in the opinion that by using ORTO-R in such a way, our study stays more on the safe side regarding the discussions on the validity and diagnostic value of the scale. Finally, we have added a method factor when analyzing the model fit of ORTO-R, the same way it was done in the original article [17]. Although we also report the results of the model without the method factor, latent means of groups were not compared as the model did not have configural invariance.
Conclusion
In conclusion, people who compete at sports events, exercise regularly at a recreational level, or lead a sedentary life have similar scores in ORTO-R. Also, in terms of ON, females are not much different when compared to males.
What is already known on this subject?
Orthorexia nervosa is characterized by pathological fixation on healthy eating. Athletes are under higher risk for other eating disorders. Findings regarding orthorexia nervosa among athletes are contradictory.
What this study adds?
Athletes, be it recreational or competitive, are not more prone to orthorexia nervosa than sedentary people. Also, females do not score differently in ORTO-R than males.
Availability of data and material
Dataset is available under https://doi.org/10.17632/4cdprfmv95.3.
Notes
When model 1 was tested for measurement invariance across groups, configural invariance was rejected (χ2 = 91.85, df = 27, AIC = 12,622, BIC = 12,880, CFI = 0.893, RMSEA = 0.091). Later, measurement invariance of model 1 was tested across genders and configural invariance was rejected (χ2 = 105.15, df = 18, AIC = 12,608, BIC = 12,780, CFI = 0.862, RMSEA = 0.105). Finally, configural invariance of model 1 across different education levels was also rejected (χ2 = 84.168, df = 18, AIC = 11,348, BIC = 11,516, CFI = 0.880, RMSEA = 0.097). We finalized the analysis here. Therefore, metric and scalar invariances were not tested and comparing latent means was not possible.
Abbreviations
- AIC:
-
Akaike information criterion
- BIC:
-
Bayesian information criterion
- CFA:
-
Confirmatory factor analysis (CFA)
- CFI:
-
Comparative fit index
- CI:
-
Confidence interval
- Df:
-
Degree of freedom
- DSM:
-
Diagnostic and Statistical Manual of Mental Disorders
- ICD:
-
International Classification of Disease
- IQR:
-
Interquartile range
- ON:
-
Orthorexia nervosa
- RMSEA:
-
Root mean square error of approximation
- RNI:
-
Relative non-centrality index
- SRMR:
-
Standardized root mean square residual
- TLI:
-
Tucker–Lewis index
- WRMR:
-
Weighted root mean square residual
References
American Psychiatric Association (2013) Diagnostic and statistical manual of mental disorders. American Psychiatric Association, New York
Fairburn CG, Cooper Z (2011) Eating disorders, DSM-5 and clinical reality. Br J Psychiatry 198:8–10
Bratman S (1997) Health Food Junkie. Yoga J 136:42–50
Dunn TM, Bratman S (2016) On orthorexia nervosa: a review of the literature and proposed diagnostic criteria. Eat Behav 21:11–17
Cena H et al (2019) Definition and diagnostic criteria for orthorexia nervosa: a narrative review of the literature. Eating Weight Disord 24:209–246
Costa CB, Hardan-Khalil K, Gibbs K (2017) Orthorexia nervosa: a review of the literature. Issues Mental Health Nurs 38:980–988
Sundgot-Borgen J, Torstveit MK (2004) Prevalence of eating disorders in elite athletes is higher than in the general population. Clin J Sport Med 14:25–32
Segura-García C et al (2012) Orthorexia nervosa: a frequent eating disordered behavior in athletes. Eat Weight Disord 17:e226–e233
Malmborg J, Bremander A, Olsson MC, Bergman S (2017) Health status, physical activity, and orthorexia nervosa: a comparison between exercise science students and business students. Appetite 109:137–143
Eriksson L, Baigi A, Marklund B, Lindgren EC (2008) Social physique anxiety and sociocultural attitudes toward appearance impact on orthorexia test in fitness participants. Scand J Med Sci Sports 18:389–394
Clifford T, Blyth C (2019) A pilot study comparing the prevalence of orthorexia nervosa in regular students and those in University sports teams. Eat Weight Disord 24:473–480
Oberle CD, Watkins RS, Burkot AJ (2018) Orthorexic eating behaviors related to exercise addiction and internal motivations in a sample of university students. Eat Weight Disord 23:67–74
Varga M, Thege BK, Dukay-Szabó S, Túry F, van Furth EF (2014) When eating healthy is not healthy: Orthorexia nervosa and its measurement with the ORTO-15 in Hungary. BMC Psychiatry 14:1–11
Yargıç M (2020) Orthorexia nervosa risk assessment of athletes vs sedentary. Mendeley Data V3. https://doi.org/10.17632/4cdprfmv95.3
Donini LM, Marsili D, Graziani MP, Imbriale M, Cannella C (2005) Orthorexia nervosa: validation of a diagnosis questionnaire. Eat Weight Disord 10:e28–e32
Arusoğlu G, Kabakçı E, Köksal G, Merdol TK (2008) Orthorexia Nervosa and Adaptation of ORTO-11 into Turkish. Türk Psikiyatr Derg 19:283–291
Rogoza R, Donini LM (2020) Introducing ORTO-R: a revision of ORTO-15: based on the re-assessment of original data. Eat Weight Disord 1:3
Hu LT, Bentler PM (1998) Fit indices in covariance structure modeling: sensitivity to underparameterized model misspecification. Psychol Methods 3:424–453
Byrne BM (1994) Structural equation modeling with EQS and EQS-Windows: Basic Concepts, Applications, and Programming. Sage Publications, Inc., USA
Distefano C, Liu J, Jiang N, Shi D (2017) Structural equation modeling: a multidisciplinary journal examination of the weighted root mean square residual: evidence for trustworthiness? Taylor Fr 25:453–466
McDonald R (2012) Test theory: a unified treatment
R Core Team (2013) R: a language and environment for statistical computing
Kenny DA, Kaniskan B, McCoach DB (2015) The performance of RMSEA in models with small degrees of freedom. Soc Methods Res 44:486–507
Segura-García C et al (2012) Orthorexia nervosa: a frequent eating disordered behavior in athletes. Eat Weight Disord 17:226
Rogoza R (2019) Investigating the structure of ORTO-15: a meta-analytical simulation study. Eat Weight Disord 24:363–365
Rudolph S (2018) The connection between exercise addiction and orthorexia nervosa in German fitness sports. Eat Weight Disord 23:581–586
Kiss-Leizer M, Tóth-Király I, Rigó A (2019) How the obsession to eat healthy food meets with the willingness to do sports: the motivational background of orthorexia nervosa. Eat Weight Disord 24:465–472
Martinsen M, Sundgot-Borgen J (2013) Higher prevalence of eating disorders among adolescent elite athletes than controls. Med Sci Sports Exerc 45:1188–1197
Pelly FE, Burkhart SJ (2014) Dietary regimens of athletes competing at the Delhi 2010 commonwealth games. Int J Sport Nutr Exerc Metab 24:28–36
Wilson PB (2016) Nutrition behaviors, perceptions, and beliefs of recent marathon finishers. Phys Sportsmed 44:242–251
Çiçekoğlu P, Tunçay GY (2018) A comparison of eating attitudes between vegans/vegetarians and nonvegans/nonvegetarians in terms of orthorexia nervosa. Arch Psychiatr Nurs 32:200–205
Dunn TM, Gibbs J, Whitney N, Starosta A (2017) Prevalence of orthorexia nervosa is less than 1%: data from a US sample. Eat Weight Disord 22:185–192
Brytek-Matera A, Donini LM, Krupa M, Poggiogalle E, Hay P (2015) Orthorexia nervosa and self-attitudinal aspects of body image in female and male university students. J Eat Disord 3:2
Baǧci-Bosi AT, Çamur D, Güler Ç (2007) Prevalence of orthorexia nervosa in resident medical doctors in the faculty of medicine (Ankara, Turkey). Appetite 49:661–666
Hyrnik J et al (2016) The assessment of orthorexia nervosa among 1899 Polish adolescents using the ORTO-15 questionnaire. Int J Psychiatry Clin Pract 20:199–203
Bundros J, Clifford D, Silliman K, Neyman-Morris M (2016) Prevalence of Orthorexia nervosa among college students based on Bratman’s test and associated tendencies. Appetite 101:86–94
Tremelling K, Sandon L, Vega GL, McAdams CJ (2017) Orthorexia nervosa and eating disorder symptoms in registered dietitian nutritionists in the United States. J Acad Nutr Diet 117:1612–1617
Fidan T, Ertekin V, Işikay S, Kirpinar I (2010) Prevalence of orthorexia among medical students in Erzurum, Turkey. Compr Psychiatry 51:49–54
Herranz-Valera J, Acuña-Ruiz P, Romero-Valdespino B, Visioli F (2014) Prevalence of orthorexia nervosa among ashtanga yoga practitioners: a pilot study. Eat Weight Disord 19:469–472
Missbach B et al (2015) When eating right, is measured wrong! A validation and critical examination of the ORTO-15 questionnaire in German. PLoS ONE 10:e0135772
Acknowledgements
We would like to thank M. Sinan İyisoy for his valuable contributions to the data analysis.
Funding
None.
Author information
Authors and Affiliations
Contributions
FÖ conceptualization of the study, data collection, interpretation of the data, writing, supervising. MPY conceptualization of the study, data collection, data analysis, interpretation of the data, writing. RS, OY, and GBK conceptualization of the study, data collection, interpretation of the data, and writing. All authors reviewed the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethics approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Medical Ethics Committee of Necmettin Erbakan University. (2020/2374).
Informed consent
All participants were informed about the study and informed consent was obtained online prior to initiation of the questionnaire from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The article is part of the Topical Collection on Orthorexia Nervosa.
Rights and permissions
About this article

Cite this article
Özdengül, F., Yargic, M.P., Solak, R. et al. Assessment of orthorexia nervosa via ORTO-R scores of Turkish recreational and competitive athletes and sedentary individuals: a cross-sectional questionnaire study. Eat Weight Disord 26, 1111–1118 (2021). https://doi.org/10.1007/s40519-020-01006-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40519-020-01006-2