
Abstract
Purpose
Digital interventions that consider end-user needs, preferences, and concerns may address suboptimal rates of e-health uptake, usage, and engagement. We explored target-user perspectives of e-health treatment and prevention programs for eating disorders (EDs), with a focus on investigating (1) perceived advantages and barriers of e-health; (2) help-seeking intentions; and (3) preferences for different digital functionality, device types, and content-delivery formats.
Methods
Survey data were analysed from 722 community-based participants. Participants were categorized into one of four groups based on symptom presentation and severity, ranging from low risk to probable bulimia nervosa or binge-eating disorder.
Results
e-health advantages that received the highest endorsement (~ 84%) were “always there in times of need” and “travel not required”. e-health barriers that received the highest endorsement (~ 50%) were concerns about data privacy and the accuracy of content presented. Nearly three-quarters reported an intention to use an e-health platform for preventing or treating EDs. Preference ratings were highest for programs to be available on all digital devices (relative to restricting the program to one type of device) and for content to be presented via graphics and video tutorials (rather than audio-based). e-health functionality that received highest preference ratings (~ 80%) were added clinician support, tailored feedback, strategies to change unhelpful ED thoughts, screening scales to assess symptoms, ED psychoeducation, and just-in-time intervention prompts. Preference and intention ratings were strikingly similar across all subgroups.
Conclusion
Findings may inform the development and design of e-health platforms that meet the needs of people at different stages of an ED.
Level of evidence
Level V, cross-sectional descriptive study.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Eating disorders (EDs) are serious psychiatric conditions that are associated with high rates of mortality, comorbidity, and relapse [1]. Although empirically-validated ED treatment and prevention programs are available [2, 3], the reality remains that less than one-quarter of people with – or at risk of – an ED seek or receive help [4]. Many factors are proposed to contribute to this existing treatment gap, including limited therapist availability, the cost of treatment, geographic isolation from available services, long wait-lists, privacy concerns, and stigma associated with help-seeking [5].
Prevention or treatment programs delivered via computers, smartphones, or other digital means have been touted as a suitable solution to the barriers of ED treatment. The format of digital interventions vary, but can range from standard therapist-led sessions that are transmitted electronically via online chat or video conferencing (i.e., “e-therapy”), to modular-based, unguided or guided programs delivered through a website or smartphone app (i.e., “e-health”). Proponents of the latter e-health approach highlight their scalability, tailored delivery, and cost advantages over traditional face-to-face treatment [6]. A strong body of research supports the acceptability, efficacy, and cost-effectiveness of e-health interventions for numerous common and costly mental health problems [7], and accumulating evidence shows that e-health interventions may be an accepted and effective approach for treating and preventing EDs [8, 9]. However, the optimism of e-health has been tempered by recognition that these interventions are associated with relatively low rates of uptake, engagement, and adherence [10]. Indeed, a recent review identified that ~ 41% of people enrolled in clinical trials of mental health apps did not even download their prescribed app, while only one-third completed all required modules [11]. This is problematic in light of earlier findings highlighting a dose–response relationship between online intervention usage and therapeutic outcomes [10].
Developing a digital intervention that takes into account end-user needs, preferences, and concerns may be one way to address the suboptimal rates of e-health uptake, adherence, and engagement. Indeed, prior work has shown that involving the target population in the conception, design, and implementation of an e-health intervention produced strong satisfaction ratings and a 97% retention rate in a feasibility trial [12]. Although numerous studies have sought to better understand and identify participant preferences and concerns related to e-health interventions for population mental health e.g., [13, 14], there is a dearth of research investigating e-health perspectives among people with or at risk of an ED.
To our knowledge, only two quantitative studies have investigated participant perspectives of e-health interventions in the context of EDs. First, McClay et al. [15] recruited people with elevated ED symptoms to participate in a randomized trial of an e-health intervention. Prior to the delivery of treatment, participants’ impressions of e-health were assessed; 98% of participants viewed e-health positively, with 74% expressing a desire for added clinician support, primarily via email. The authors also assessed for any anticipated problems associated with e-health interventions, with confidentiality (24%; n = 55) and privacy (17%; n = 38) being the only cited concerns. In the second study, Linardon et al. [16] assessed e-health attitudes, preferences, and intentions in 713 participants spanning the full spectrum of ED pathology. We found that although the majority of participants preferred face-to-face ED treatment, attitudes towards e-health were largely positive, and half of the sample reported an intention to use an online program if it was available to them. Taken together, nascent data indicate that digitally delivered interventions are viewed favourably and have the potential to broaden the reach of evidence-based ED interventions.
Given that end-user needs may influence [re]design choices for the development of online interventions, it is necessary to gather more detailed information about perspectives and preferences for e-health among a target population. Thus, we aimed to extend from the two prior studies in this context and further explore perspectives of, and preferences for, e-health interventions directed at treating and preventing EDs. Specifically, we uniquely focused on investigating participant: (1) perceived advantages and barriers of e-health, (2) help-seeking intentions, and (3) preferences for different digital functionality, devices, modes of content delivery. It is our overall objective that these findings will inform the design and development of tailored online programs that meet the needs of individuals presenting at different stages of an ED.
Method
Participants and procedure
A total of 1,185 participants from the general population were recruited to participate in this online survey. As the creation of study subgroups of ED risk level was based on Eating Disorder Examination Questionnaire (EDE-Q) scores (see below for more detail), we excluded participants who did not complete this measure (the last measure) from subsequent analyses (n = 463). There were no statistically significant differences between completers and drop-outs on any demographic variable (ps > 0.05). The final sample comprised 722 adults. Given that this is a descriptive study, no a priori power analysis was conducted. The sample size of 722 was sufficient to achieve the aims of this study, and we note that the present sample size is substantially larger than prior descriptive studies on e-health attitudes and preferences in the general population [17, 18].
Participants were recruited mostly through the authors’ open access ED-related psychoeducational website (https://breakbingeeating.com/) and associated social media accounts (i.e., Instagram and Facebook). Readers may refer to Linardon et al. [19] for a detailed description of this website platform and the corresponding demographic and mental health profile of website visitors. We briefly note that website and social media visitors are more symptomatic than what is expected from the general population, with more than 80% having reported engaging in at least one ED behaviour in the past month and around 50% exhibiting clinically significant ED symptoms [19]. The only inclusion criteria to participate in this survey were that participants were required to be aged 18 years or over and were able to understand the survey questions presented in English. The survey was not restricted to specific countries. This survey was advertised on the authors’ website and social media pages. The study advertisement stated that the researchers were interested in understanding peoples’ attitudes, perspectives, and opinions related to psychological interventions for problem eating patterns delivered through technology. Respondents to study advertisements clicked on a web link that took them to the online questionnaire. The questionnaire was presented in a fixed order and took approximately 15 min to complete. Informed consent was provided by all participants. Ethics approval was obtained from Deakin University.
Study variables
Sociodemographic and background variables
Sociodemographic characteristics included sex, age, ethnicity, country of residence, and employment status. We also assessed whether participants were receiving any form of face-to-face psychological therapy, had prior experience with an e-health intervention, or had heard or read about e-health interventions.
e-health advantages and barriers
Participants were presented with eight proposed advantages and barriers of e-health interventions and were asked to indicate which advantages and barriers they agreed with. Participants could also select “none of these” as an option or select “other” and specify an additional advantage or barrier. An example advantage includes “I wouldn't have to travel anywhere to receive help with an e-therapy intervention”. An example barrier includes “I would be concerned about the privacy of my data I shared within the e-therapy intervention”. These proposed advantages and barriers were based off prior research [20].
Intervention delivery preference
We assessed preferences for e-health interventions by first providing a description of three types of psychological interventions: face-to-face treatment; unguided e-health programs; therapist-guided e-health programs. After being presented with these descriptions, participants were asked to indicate which of the three they would prefer to use if they were to seek help to address or prevent ED behaviours.
Intended help-seeking
Participants were asked to indicate their intentions for seeking out or using a (1) psychologist/psychiatrist and (2) a guided or unguided e-health program if they were to experience any ED behaviours, now or in the future. Intention ratings were based on a 5-point scale, ranging from extremely unlikely to extremely likely. Responses were later dichotomized as yes (intentions) or no (no intentions) for analyses: ratings of 1 (extremely unlikely), 2 (somewhat unlikely), or 3 (neither unlikely nor unlikely) were categorized as “no,” whereas ratings of 4 (somewhat likely) and 5 (extremely likely) were categorized as “yes.”
Preference and usefulness ratings for different e-health functions
Participants were presented with 14 different functions, strategies, or features commonly implemented in e-health programs aimed at treating or preventing EDs. An example function includes “screening scales to assess the nature and severity of my ED behaviours”. Participants were first asked whether they would personally like to have that function available if they were to use an e-health program for addressing or preventing ED behaviours. Response options were either “yes”, “no”, or “undecided”. Participants also rated how helpful they perceived each of those functions to be, ranging from very unhelpful (1) to very helpful (5).
e-health preference type
Participants were asked to indicate, if they were to use an e-health platform for addressing or preventing ED behaviours, whether they would prefer a tailored (modified to address their unique needs) or generic (delivered in the same way to everyone) online program.
e-health content delivery
Participants were asked to indicate their level of preference for four different e-health content delivery formats: written text; audio recordings; graphics/images; video presentations and tutorials. Responses to each delivery format were rated on a 5-point scale, ranging from strongly avoid (0) to strongly prefer (4).
Digital device preference
Participants indicated which technology device they would prefer an e-health program to be available on if they were to use an online program for addressing or preventing ED behaviours. Response options included computer only, smartphone only, tablet only, or all of these devices.
Creation of study subgroups
Four subgroups were created to capture the spectrum of EDs based on responses to the EDE-Q. The EDE-Q is a 28-item, psychometrically sound measure that assesses the core symptoms of EDs experienced over the past month [21]. There are four subscales each with items rated along a 7-point scale. There are also specific items that assess the frequency of ED behaviours. The four subgroup definitions, which were based off prior research (Linardon et al., 2020), are as follows:
-
Binge-eating disorder symptomatology. At least two objective binge-eating episodes in the past 28 days; and the absence of persistent extreme weight control behaviour in the past 28 days (< 2 episodes). The threshold of ≥ two binge episodes (rather than ≥ four episodes) was used because we wanted to capture individuals who met criteria for either threshold or subthreshold BED, according to existing diagnostic criteria [22]. We combined subthreshold and threshold cases, because there is evidence to suggest that individuals with subthreshold symptoms closely resemble those who meet full diagnostic criteria on a range of eating disorder, psychiatric, and impairment measures [23].
-
Bulimia nervosa symptomatology. At least two objective binge eating episodes in the past 28 days; and at least two extreme weight-control behaviours (fasting, self-induced vomiting, laxative misuse, or driven exercise) in the past 28 days; and overvaluation of weight and shape. The threshold of ≥ two episodes was used for the same reason listed above.
-
At risk. Reporting at least one episode of an ED behaviour (binge eating, self-induced vomiting, laxative misuse, driven exercise); and/or exhibiting elevated weight or shape concerns (a key ED risk factor), which we defined as scoring 1 SD above population norms on the shape (M = 2.23, SD = 1.65 for women and M = 1.59, SD = 1.38 for men) and weight concern (M = 1.79, SD = 1.51 and M = 1.29, SD = 1.27 for men) subscale [24, 25]; and not meeting criteria for BN or BED.
-
Low risk. No ED behaviour episodes; and low-normal levels of shape and weight concerns (subscale scores within or below 1 SD of the same population norms listed for the at risk group). Low risk participants were defined on the basis of weight and shape concern scores because of prior research showing that these variables are the most established risk factors for the development of an ED [26].
Data analysis
Given the descriptive nature of this study, data are presented in terms of frequencies and percentages, and means and standard deviations. Frequencies and percentages are presented for the following variables: perceived advantages and barriers to e-health; intervention delivery mode preference; intentions to use e-health and face-to-face therapy; preference ratings for different digital functionality; and preference for digital device type and tailoring. Means and standard deviations are presented for perceived usefulness ratings for different digital functionality and content delivery preferences. All data are presented for the whole sample as well as for the four distinct subgroups.
Results
Participant characteristics
Sample characteristics are presented in Table 1. The mean age of the total sample was 30.25 (SD = 8.29). The majority of participants were female, White/Caucasian, were working full-time, and resided in either the US or Australia/New Zealand. Most participants had heard about e-health, while few participants were currently receiving psychotherapy or had any experience with e-health.
The breakdown of the four subgroups is as follows: most participants met criteria for the at risk subgroup (n = 257; 36%), followed by the BN symptomatology (n = 176; 24%), BED symptomatology (n = 165; 23%), and low risk subgroup (n = 124; 17%).
Perceived e-health advantages and barriers
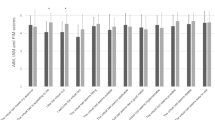
Figures 1 and 2 present the percentage of participants overall and across each subgroup who agreed with or endorsed each of the eight proposed advantages and barriers of e-health interventions, respectively. e-health advantages that received substantial agreement among participants (> 75% endorsed) were the statements “e-health interventions are always there in times of need”, “e-health interventions do not require travel”, and “e-health interventions are cost-effective”. e-health advantages that received the lowest agreement ratings were “e-health interventions would not require me to write things down on paper (like my thoughts and feelings)” “e-health interventions are more compatible with my life” and “e- health interventions are more private”. No participant selected “none of these are advantages to me”. The mean number of e-health advantages participants endorsed was 5.14 (SD = 1.65; range = 1–8).

Percentage of participants who endorse each e-health advantage

Percentage of participants who endorse each e-health barrier
e-health barriers that received the highest level of agreement (> 50% endorsed) were “concern about the accuracy of information in an e-health intervention” and “concern about the privacy of the data that I share”. Barriers that were rarely endorsed (< 15%) were “I would not trust an e-health intervention”, “concern that I would not know how to use the e-health program properly”, “using an e-health intervention would be too much work and take up too much time”, and “none of these”. The mean number of e-health barriers participants endorsed was 2.41 (SD = 1.49; range = 1–8).
Mode of intervention delivery preference
The majority of participants expressed a desire for face-to-face therapy (n = 418; 57.9%), followed by a therapist-guided e-health program (n = 243; 33.7%), and then an unguided e-health program (n = 61; 8.4%). This pattern of results remained the same across the four subgroups (Table 2).
We examined whether participants who selected a preference for e-health (guided or unguided) differed on the number of advantages and barriers endorsed than participants who selected a preference for face-to-face therapy. T-tests revealed that participants who selected a preference for e-health endorsed significantly more advantages (M = 5.69, SD = 1.50) and fewer barriers (M = 1.99, SD = 1.29) than participants who selected a preference for face-to-face therapy (M = 4.74, SD = 1.64; t = − 7.96, p < 0.001; M = 2.72, SD = 1.55; t = − 6.83, p < 0.001, respectively).
We also examined whether those who selected a preference for e-health differed to those who selected a preference for face-to-face therapy on prior e-health experience and current therapy usage. Chi square test of independence revealed that those who preferred e-health were significantly less likely to be receiving current face-to-face therapy than those who preferred face-to-face therapy (25% vs 73%; χ2 = 20.48, p < 0.001). No difference between those who preferred e-health to those who preferred face-to-face therapy was observed on prior e-health experience (40% vs 59%; χ2 = 0.08, p = 0.770).
Intention to use face-to-face and e-health interventions
Table 2 reports the percentage of participants who intend on seeking out or using an e-health intervention (guided or unguided) and face-to-face therapy for addressing or preventing ED behaviours. Across the total sample more than half of the participants reported an intention to seek out or use an e-health intervention, and more than half reported an intention to seek out or use face-to-face therapy. A total of 289 participants reported an intention to seek out both e-health and face-to-face intervention, while 158 and 177 participants reported an intention to seek out only e-health and face-to-face treatment, respectively.
Preference and usefulness ratings for e-health functions
Perceived usefulness ratings and a preference to use 14 different e-health functions are presented in Table 3. Across all subgroups, there was a strong preference (> 80% endorsed) to use (or to have available) the following features: screening scales to assess the nature and severity of ED symptoms; tailored automated and professional feedback; psychoeducation about EDs; cognitive restructuring strategies to change unhelpful thoughts related to food; mood-boosting strategies; links to other support services; and just-in-time intervention prompts. These features also received high perceived usefulness ratings.
e-health features that received lower preference (< 65% endorsed) and usefulness ratings across subgroups included: motivational pop-ups; reminder text messages or emails to engage in the intervention; gratitude journals; and the ability to connect with others who are also using the e-therapy program (Table 3).
Generic vs tailored e-health program
The vast majority expressed a preference for a tailored (96%) over a generic (4%) e-health program. The same pattern occurred across all four subgroups (see Table 4).
Digital device preference
The vast majority indicated that they would like the e-health program to be available on all digital devices, followed by smartphones only, computers only, and then tablets only. The same pattern occurred across all four subgroups (see Table 4).
Content delivery preferences
Mean preference ratings were highest for graphics/images, followed by video tutorials, written text, and audio recordings. The same pattern occurred across all four subgroups (see Table 4).
Discussion
Summary of findings
Several important findings emerged. First, e-health interventions were viewed relatively favourably, with majority of participants endorsing many of the proposed advantages of digital interventions, including their cost-effectiveness, availability in times of need, and their ability to potentially address the stigma associated with help-seeking. However, most participants expressed concern about the accuracy of information presented in an e-health program as well as the privacy of data shared. Second, despite the fact that most participants preferred face-to-face interventions, a significant percentage of participants (~ 68%) reported an intention to seek out and use an e-health program. Third, participants expressed a strong preference for content to be delivered via video or graphic format (relative to audio), to be tailored rather than generic, and to be available on a range of different digital devices (rather than restricted to one device). Finally, e-health functionalities that received highest preference and perceived usefulness ratings were tailored feedback on progress, clinician support, cognitive restructuring strategies, symptom monitoring, mood-boosting strategies, and just-in-time intervention prompts. By contrast, e-health functionalities that received lowest preference and usefulness ratings were motivational pop-ups, reminders messages to engage, and gratitude exercises. Importantly, each of these four broad findings were largely similar across the subgroups, suggesting that e-health perspectives may not vary as a function of different symptom profiles or severities.
Implications and future directions
Important implications and future directions emerged related to the design, implementation, and evaluation of e-health interventions for EDs. First, present findings suggest that individual preferences for intervention delivery formats may need to be considered before prescribing an intervention for individuals at different stages of an ED. That only a very small percentage of participants preferred a purely unguided e-health program indicates that, where feasible, some level of face-to-face or virtual professional support should be incorporated within an intervention to potentially maximize engagement and therapeutic outcomes. Such low preference rates for purely unguided e-health interventions have been reported previously [17], and it could explain why this modality is associated with poorer outcomes than guided e-health programs and standard treatment [7]. However, whether individual differences in intervention delivery preference predict therapeutic outcomes has yet to be demonstrated empirically. Thus, future RCTs may benefit from assessing intervention delivery preference at baseline, and then investigating whether preference rates account for variance in adherence, drop-out, and symptom reduction. If preferences ratings do emerge as robust predictors of outcome, then subsequent research should consider conducting a modified matched care design, in which a group of individuals are given an intervention that matches their delivery preference and are then compared against a group of individuals who are given a generic, unmatched intervention [27]. This sequence of events may help accelerate the delivery of personalized care among individuals at all stages of an ED, and may consequently help reduce the strain on the already limited healthcare resources.
A second implication concerns the use of peer or automated support systems. Even though most preferred an intervention that had some element of professional guidance, it is important to point out that the involvement of a professional can be costly and may restrict the capacity of e-health interventions to reach the millions of people worldwide in need of help. Finding other, more novel methods of support may instead be needed. For example, automated supported systems may be particularly useful, as these systems can be guided by sophisticated machine learning principles, meaning that end-users could receive personalized guidance, prompts, or help in real time and in moments of need [28]. Automated support has been shown to produce equivalent outcomes to human support in the field of depression [29], suggesting that ED research may benefit from developing, testing, and implementing automated support systems for those wanting guidance. Further to this, automated support systems may be particularly suited to a blended care approach, in which a person uses an e-health program in between their face-to-face sessions to help facilitate skill acquisition (i.e., the ability to successfully perform a learned skill) and utilization (i.e., the frequency with which a skill is practiced) [30]. Automated support systems that prompt clients to engage in and practice relevant skills taught by their therapist in high risk situations may be necessary for enhancing outcomes.
Third, even though intentions to seek out e-health were relatively high, whether this corresponds to subsequent e-health usage remains unclear. Although Protection Motivation Theory suggests that intentions are strongly predictive of behaviour [31], there is reason to suspect that few people who expressed such intentions will go on to use an e-health platform, particularly since e-health uptake in the “real-world” is relatively low [32] and a minority of study participants reported having previously used e-health. Our findings point towards possible reasons for this potential discrepancy. First, results suggest that concern about the accuracy of information presented in an e-health platform may be an important deterrent. Indeed, previous research identified that, of the 40 or so different apps for EDs freely available in iTunes, most do not resemble the programs evaluated in rigorous research trials and some contain non-evidence-based elements that are potentially harmful [33]. A standardized rating system that can appraise each e-health program, in terms of its usability, content quality, and evidence-base, is needed to inform the end-user on what platform may or may not be helpful. An easy-to-understand rating system may guide end-users towards the specific programs that contain scientifically sound content, which could thus increase e-health uptake. Although such quality systems are available [34, 35], they are yet to be applied to ED-related interventions. A second reason why intention ratings may not translate to e-health uptake may have to do with concerns about the privacy of data shared. Indeed, earlier research has showed that fewer than 10% of a surveyed population were willing to share their health data with a technology company due to privacy concerns [36]. It may thus be important for e-health developers to ensure that an explicit privacy policy statement is provided in the platform so that users are well-informed of how their data will be managed. Without this, people may be reluctant to download a potentially effective online program.
Finally, increasing e-health uptake, engagement and preferences may depend on the extent to which the design of the online platform has taken into account end-user needs. This study was able to identify which e-health devices, content delivery formats, and functionalities were preferred by the target population, suggesting that developers may need to incorporate these preferences into the design of the platform if it is to be downloaded or used over a sustained period. For example, most participants preferred the e-health program to be available on all digital device types (rather than restricted to one device), suggesting that researchers may benefit from collaborating with various software designers to allow for this flexibility in device usage. Different digital devices serve unique functions (e.g., large screen computers enable for completion of written homework tasks better, while smartphone apps enable users to receive instantaneous alerts in high-risk situations) that may be necessary for improving treatment outcomes [11]. Moreover, preference findings suggest that certain e-health components for EDs should be prioritized over others when creating the intervention package. For example, mood-boosting, cognitive restructuring, and symptom monitoring strategies should be prioritized over gratitude and motivational exercises not only because of their relative preference and perceived usefulness ratings, but also because they have a much larger evidence base [37, 38]. Even though it is reasonable to hypothesize that an e-health platform that has taken into account these individual preferences will result in greater engagement and consequently better outcomes than a generic platform, this needs to be tested and confirmed in a head-to-head randomized trial [39]. Present findings are important insofar as they may inform the design of such an RCT, in terms of what the e-health experimental group may entail (i.e., the preferred functionality, layout, device flexibility etc.).
Limitations
This study has important limitations First, participants were recruited mostly from a psychoeducational ED-related website and associated social media account. Thus, participants self-selected into this study which could have introduced some biases, such that only those who report elevated symptoms, more motivation, or who are already active online completed the survey.
Second, given that we only sampled adults, our results cannot be generalized to younger populations. Exploring e-health perspectives in younger populations is important because younger people may be more receptive to and benefit from early interventions delivered through technology [40].
Third, there were several variables that we did not assess (e.g., prior experience with face-to-face treatment, perceived advantages and disadvantages of other intervention modalities) that could have furthered our understanding of perspectives of e-health. For example, for those that had prior experience with e-health, assessing reasons for discontinuation may have shed light towards possible strategies that may have enhanced sustained user engagement [11]. Moreover, preferences for other distinct and common digital functionality, including gamification strategies, virtual reality components, and peer feedback, were not assessed in this study but are worthy of future consideration.
Fourth, present findings cannot be generalized to people with anorexia nervosa (AN). We did not create an AN subgroup due to inherent limitations with relying on self-reported height and weight [41]. At present, few digital interventions have been trialled in individuals with AN, in part because this diagnostic subgroup usually requires more intensive face-to-face services. However, accumulating evidence suggests that e-health after-care interventions that include self-monitoring components, therapist guidance, and personalized coping strategies produce modest improvements in core AN symptoms [42]. Such findings shed light towards potentially effective and tolerated digital components. However, surveying the needs and preferences in this population is needed to better understand what role technology may play in interventions for AN.
What is already known on this subject?
Little is known about preferences for different e-health functionality and content delivery formats for EDs. This study addressed this gap.
What this study adds?
This is the first study to have generated data on participant e-health device, content delivery format, and functionality preferences. Findings will inform the design of tailored e-health programs for EDs.
Code availability
Syntax can be provided upon request.
References
Klump KL, Bulik CM, Kaye WH, Treasure J, Tyson E (2009) Academy for eating disorders position paper: eating disorders are serious mental illnesses. Int J Eat Disord 42(2):97–103
Linardon J, Fairburn CG, Fitzsimmons-Craft EE, Wilfley DE, Brennan L (2017) The empirical status of the third-wave behaviour therapies for the treatment of eating disorders: a systematic review. Clin Psychol Rev 58:125–140. https://doi.org/10.1016/j.cpr.2017.10.005
Linardon J, Wade T, De la Piedad GX, Brennan L (2017) The efficacy of cognitive-behavioral therapy for eating disorders: a systematic review and meta-analysis. J Consult Clin Psychol 85:1080–1094. https://doi.org/10.1037/ccp0000245
Weissman RS, Rosselli F (2017) Reducing the burden of suffering from eating disorders: unmet treatment needs, cost of illness, and the quest for cost-effectiveness. Behav Res Ther 88:49–64. https://doi.org/10.1016/j.brat.2016.09.006
Kazdin AE, Fitzsimmons-Craft EE, Wilfley DE (2017) Addressing critical gaps in the treatment of eating disorders. Int J Eat Disord 50:170–189. https://doi.org/10.1002/eat.22670
Andersson G (2016) Internet-delivered psychological treatments. Annu Rev Clin Psychol 12:157–179. https://doi.org/10.1146/annurev-clinpsy-021815-093006
Linardon J, Cuijpers P, Carlbring P, Messer M, Fuller-Tyszkiewicz M (2019) The efficacy of app-supported smartphone interventions for mental health problems: a meta-analysis of randomized controlled trials. World Psychiatry 18:325–336. https://doi.org/10.1002/wps.20673
Loucas CE, Fairburn CG, Whittington C, Pennant ME, Stockton S, Kendall T (2014) E-therapy in the treatment and prevention of eating disorders: a systematic review and meta-analysis. Behav Res Ther 63:122–131. https://doi.org/10.1016/j.brat.2014.09.011
Linardon J, Shatte A, Messer M, Firth J, Fuller-Tyszkiewicz M (2020) E-mental health interventions for the treatment and prevention of eating disorders: an updated systematic review and meta-analysis. J Consult Clin Psychol. https://doi.org/10.1037/ccp0000575
Donkin L, Christensen H, Naismith SL, Neal B, Hickie IB, Glozier N (2011) A systematic review of the impact of adherence on the effectiveness of e-therapies. J Med Internet Res 13:e52. https://doi.org/10.2196/jmir.1772
Linardon J, Fuller-Tyszkiewicz M (2020) Attrition and adherence in smartphone-delivered interventions for mental health problems: a systematic and meta-analytic review. J Consult Clin Psychol 88:1–13. https://doi.org/10.1037/ccp0000459
Tighe J, Shand F, Ridani R, Mackinnon A, De La Mata N, Christensen H (2017) Ibobbly mobile health intervention for suicide prevention in Australian Indigenous youth: a pilot randomised controlled trial. BMJ Open 7:e013518. https://doi.org/10.1136/bmjopen-2016013518
Apolinário-Hagen J, Kemper J, Stürmer C (2017) Public acceptability of e-mental health treatment services for psychological problems: a scoping review. JMIR Mental Health 4(2):e10
Apolinário-Hagen J, Vehreschild V, Alkoudmani RM (2017) Current views and perspectives on e-mental health: an exploratory survey study for understanding public attitudes toward internet-based psychotherapy in Germany. JMIR Mental Health 4:e8. https://doi.org/10.2196/mental.6375
McClay C-A, Waters L, Schmidt U, Williams C (2016) A survey of attitudes towards computerized self-help for eating disorders within a community-based sample. Behav Cognit Psychother 44:65–78
Linardon J, Shatte A, Tepper H, Fuller-Tyszkiewicz M (2020) A survey study of attitudes toward, and preferences for, e-therapy interventions for eating disorder psychopathology. Int J Eat Disord 53:907–916. https://doi.org/10.1002/eat.23268
Apolinário-Hagen J, Harrer M, Kählke F, Fritsche L, Salewski C, Ebert DD (2018) Public attitudes toward guided internet-based therapies: web-based survey study. JMIR Mental Health 5(2):e10735
March S, Day J, Ritchie G, Rowe A, Gough J, Hall T, Yuen CYJ, Donovan CL, Ireland M (2018) Attitudes toward e-mental health services in a community sample of adults: online survey. J Med Internet Res 20(2):e59. https://doi.org/10.2196/jmir.9109
Linardon J, Rosato J, Messer M (2020) Break binge eating: reach, engagement, and user profile of an internet-based psychoeducational and self-help platform for eating disorders. Int J Eat Disord. https://doi.org/10.1002/eat.23356
Carlbring P, Andersson G (2006) Internet and psychological treatment. How well can they be combined? Comput Hum Behav 22(3):545–553
Fairburn CG, Beglin S (1994) Assessment of eating disorders: interview or self-report questionnaire? Int J Eat Disord 16:363–370. https://doi.org/10.1002/1098-108X
American Psychiatric Association (2013) The Diagnostic and Statistical Manual of Mental Disorders, 5th edn. DSM 5. American Psychiatric Association, Virginia
Crow SJ, Stewart Agras W, Halmi K, Mitchell JE, Kraemer HC (2002) Full syndromal versus subthreshold anorexia nervosa, bulimia nervosa, and binge eating disorder: a multicenter study. Int J Eat Disord 32:309–318. https://doi.org/10.1002/eat.10088
Mond J, Hay PJ, Rodgers B, Owen C (2006) Eating disorder examination questionnaire (EDE-Q): norms for young adult women. Behav Res Ther 44:53–62. https://doi.org/10.1016/j.brat.2004.12.003
Lavender JM, De Young KP, Anderson DA (2010) Eating disorder examination questionnaire (EDE-Q): norms for undergraduate men. Eat Behav 11:119–121
Stice E (2002) Risk and maintenance factors for eating pathology: a meta-analytic review. Psychol Bull 128:825–848. https://doi.org/10.1037/0033-2909.128.5.825
Van Straten A, Tiemens B, Hakkaart L, Nolen W, Donker M (2006) Stepped care vs. matched care for mood and anxiety disorders: a randomized trial in routine practice. Acta Psychiatr Scand 113(6):468–476
Richards D, Richardson T (2012) Computer-based psychological treatments for depression: a systematic review and meta-analysis. Clin Psychol Rev 32:329–342. https://doi.org/10.1016/j.cpr.2012.02.004
Kelders SM, Bohlmeijer ET, Pots WTM, van Gemert-Pijnen JEWC (2015) Comparing human and automated support for depression: fractional factorial randomized controlled trial. Behav Res Ther 72:72–80. https://doi.org/10.1016/j.brat.2015.06.014
Juarascio AS, Parker MN, Lagacey MA, Godfrey KM (2018) Just-in-time adaptive interventions: a novel approach for enhancing skill utilization and acquisition in cognitive behavioral therapy for eating disorders. Int J Eat Disord 51:826–830. https://doi.org/10.1002/eat.22924
Ajzen I (1985) From intentions to actions: a theory of planned behavior. In: Action control. Springer, pp 11–39
Fleming T, Bavin L, Lucassen M, Stasiak K, Hopkins S, Merry S (2018) Beyond the trial: systematic review of real-world uptake and engagement with digital self-help interventions for depression, low mood, or anxiety. J Med Internet Res 20(6):e199
Fairburn CG, Rothwell ER (2015) Apps and eating disorders: a systematic clinical appraisal. Int J Eat Disord 48:1038–1046. https://doi.org/10.1002/eat.22398
Stoyanov SR, Hides L, Kavanagh DJ, Zelenko O, Tjondronegoro D, Mani M (2015) Mobile app rating scale: a new tool for assessing the quality of health mobile apps. JMIR mHealth uHealth 3(1):e27
Torous J, Andersson G, Bertagnoli A, Christensen H, Cuijpers P, Firth J, Haim A, Hsin H, Hollis C, Lewis S (2019) Towards a consensus around standards for smartphone apps and digital mental health. World Psychiatry 18:97–98. https://doi.org/10.1002/wps.20592
Rock Health (2015) Digital health consumer adoption. https://rockhealth.com/reports/digital-health-consumer-adoption-2015/.
Levin ME, Haeger J, An W, Twohig MP (2018) Comparing cognitive defusion and cognitive restructuring delivered through a mobile app for individuals high in self-criticism. Cognit Ther Res. https://doi.org/10.1007/s10608-018-9944-3
Kauer SD, Reid SC, Crooke AH, Khor A, Hearps SJ, Jorm AF, Sanci L, Patton G (2012) Self-monitoring using mobile phones in the early stages of adolescent depression: randomized controlled trial. J Med Internet Res 14(3):e67. https://doi.org/10.2196/jmir.1858
Fairburn CG, Patel V (2017) The impact of digital technology on psychological treatments and their dissemination. Behav Res Ther 88:19–25. https://doi.org/10.1016/j.brat.2016.08.012
Fairburn CG, Harrison PJ (2003) Eating disorders. Lancet 361:407–416
Bowring AL, Peeters A, Freak-Poli R, Lim MS, Gouillou M, Hellard M (2012) Measuring the accuracy of self-reported height and weight in a community-based sample of young people. BMC Med Res Methodol 12(1):175
Neumayr C, Voderholzer U, Tregarthen J, Schlegl S (2019) Improving aftercare with technology for anorexia nervosa after intensive inpatient treatment: a pilot randomized controlled trial with a therapist-guided smartphone app. Int J Eat Disord 52:1191–1201. https://doi.org/10.1002/eat.23152
Funding
No funding was received.
Author information
Authors and Affiliations
Contributions
JL and MM were responsible for conceptualising the research, conducting the statistical analyses and drafting the manuscript. SL and JR were responsible for conceptualising aspects of the research and editing the manuscript. All authors approved the final version of this manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors report no conflict of interest.
Ethical approval
This research was approved by the Ethical Board at Deakin University.
Informed consent
All participants provided informed consent to participate.
Availability of data and material
Data are available from the corresponding author on request.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Linardon, J., Messer, M., Lee, S. et al. Perspectives of e-health interventions for treating and preventing eating disorders: descriptive study of perceived advantages and barriers, help-seeking intentions, and preferred functionality. Eat Weight Disord 26, 1097–1109 (2021). https://doi.org/10.1007/s40519-020-01005-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40519-020-01005-3