
Abstract
Purpose
To evaluate the long-term effectiveness of a web-based therapist-delivered cognitive behavioral therapy (CBT) for patients with eating disorders (ED).
Methods
We used follow-up data from a randomized controlled trial that evaluated a web-based CBT on ED psychopathology and related health, compared to a waiting list control (WL) condition. As participants of the WL condition started the intervention after their waiting period, follow-up data included participants from both groups. The primary outcome was change from baseline, at 3, 6, and 12-month intervals in ED psychopathology, analyzed using mixed models for repeated measures. Secondary outcomes included body dissatisfaction, BMI, physical health, mental health, self-esteem, quality of life, and social functioning.
Results
The population comprised 212 participants in total, in three subgroups: bulimia nervosa (BN; n = 44), binge eating disorder (BED; n = 83), and ED not otherwise specified (EDNOS; n = 85). Treatment effects were sustained during follow-up, with generally large effect sizes for the reduction of ED psychopathology and body dissatisfaction, and small to moderate effect sizes for physical and mental health, self-esteem, social functioning, and quality of life. Most effects were found for all three subgroups, except for long-term improvements in self-esteem and quality of life among participants with BN and EDNOS.
Conclusion
This study showed long-term sustainability of treatment effects up to 1-year post-treatment of a web-based therapist-delivered CBT for patients with various ED.
Level of evidence
Level IV, evidence obtained from multiple time series analysis, with intervention.
Unique clinical trial number
NTR2415—Dutch Trial Registry (http://www.trialregister.nl/trialreg/admin/rctview.asp?TC=2415).
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Emerging technologies offer opportunities for accessible and low-threshold psychological interventions for patients with psychiatric conditions. Technology-based interventions are especially important for patients with eating disorders (ED) [1, 2] because many individuals with ED avoid regular mental health care, due to barriers as feelings of shame, fear of stigmatization, lack of awareness, and low motivation for treatment [3,4,5]. The health risks of ED are potentially serious, resulting in severe psychological, physical, and social issues [6,7,8,9]. According to a meta-analysis, only 23% of those suffering from ED sought eating disorder-specific treatment [10]. Moreover, participation rates were even smaller due to a limited availability of specialized institutions, long waiting times, and high costs [5, 11, 12]. These issues might be resolved by the use of computer- and internet-based interventions (CBIs), as they provide immediate accessibility and relative anonymity to their users.
In eating disorder treatment, CBIs are superior to waiting lists in reducing ED psychopathology and the core symptoms of binging and purging [1, 2]. However, results of these studies should be considered with caution given the limited number of high-quality studies, especially regarding long-term sustainability of treatment effects [1, 2, 13]. This is an important knowledge gap, given the substantial relapse rates in eating disorders and prolonged vulnerability of patients to relapse [14, 15]. Studies on CBIs with a longer follow-up and studies comparing CBIs to face-to-face treatment are rather scarce. Wagner et al. [16] compared online CBT with conventional-guided bibliotherapy in females with bulimia nervosa (BN) in a study with a follow-up of 18 months. Significant improvements in eating disorder symptomatology were found in both groups, which remain stable in long term, but online CBT was not superior to bibliotherapy, both at post-treatment and 18-month follow-up. A 20-week web-based CBT with 25 scheduled therapist feedback moments also showed to be effective in reducing bulimic symptoms, with results sustaining up to 1-year follow-up [17]. In that study, the web-based CBT was superior to no treatment (waiting list group) and unsupported bibliotherapy at post-treatment, but the differences between online CBT and bibliotherapy were no longer significant at 1-year follow-up, due to improvements in the bibliotherapy group. Compared to face-to-face therapy, a telemedicine-delivered CBT including 20 sessions of videoconferencing with a trained therapist was roughly equivalent in outcome among patients with BN and bulimic symptoms at 12-month follow-up [18]. Comparable results were found for a 20-week therapeutic chat group therapy for patients with BN at 12-month follow-up, although this online therapy was inferior to the same treatment conducted via face-to-face group therapy at post-treatment [19]. The study of de Zwaan et al. [20] showed similar outcomes for patients with full or subsyndromal binge eating disorder (BED), with internet-based guided self-help to be less efficacious compared to face-to-face CBT at post-treatment and at 6-month follow-up, while these differences disappeared at 1.5-year follow-up.
The current paper reports on a 1-year follow-up study into a web-based CBT for female patients with ED. A randomized controlled trial (RCT) with pre–post design already proved this intervention to be superior to a waiting list control (WL) group in reducing ED psychopathology and body dissatisfaction, and in improving ED-related health, self-esteem en social functioning at post-treatment [21]. Since participants of the WL group also started the web-based CBT after the 15-week waiting period, follow-up analyses were conducted for participants from both groups. The aim of this paper is to evaluate the long-term sustainability of treatment effects, also for the specific ED subgroups BN, BED, and eating disorders not otherwise specified (EDNOS). Furthermore, we will examine treatment outcomes in relation to patients’ treatment adherence.
Materials and methods
Procedure
The study was registered in the Dutch Trial Registry (NTR2415) and details of the protocol have been published previously [22]. It was approved by the Ethics Committee of Medical Spectrum Twente in March 2011 (reference number NL31717.044.010, P10-31).
Participants (n = 214) were recruited via the Dutch website www.etendebaas.nl (“Look at your eating”) from March 2011 until December 2013. All female patients who met DSM-IV criteria for BN, BED or EDNOS, had access to the Internet, were fluent in Dutch, and had a referral from their general practitioner (GP) were eligible to participate in this study. Exclusion criteria included severe underweight, suicidal ideation, receiving psychological or pharmaceutical treatment for any eating disorder in the prior 6 months, pregnancy, and expected absence for 4 weeks or longer during the web-based CBT. Eligible participants provided written informed consent and were randomly assigned to start the web-based CBT immediately (n = 108) or after a waiting period of 15 weeks (n = 106). Two participants withdrew before the completion of the baseline questionnaire, thus 212 participants were included in this study. Outcome measures were assessed before and after the web-based CBT, and at 3, 6, and 12 months after the completion (or premature termination) of the treatment.
Web-based CBT
The intervention consisted of 16 treatment modules with at least 21 online contact moments, with asynchronous communication with a personal therapist bi-weekly, and 10 assignments, based on the principles of CBT and motivational interviewing (MI) [23, 24]. The first part of the treatment focused on analyzing participants’ eating behaviors and the function of the ED. The second part aimed to change eating attitudes and behaviors. Therapists’ support included a comprehensive response to participants’ messages, completed assignments or questionnaires, and registrations in the online eating diary. Therapists had a bachelor’s degree in nursing or social work or a master’s degree in psychology. They completed extensive training and were supported by a multidisciplinary team throughout the web-based treatment. A detailed overview of the web-based intervention has been published previously [21].
Participants were considered treatment completers when they had attended all 16 treatment modules with at least 21 times of contact with their therapist and completion of all ten assignments. Participants who dropped out of treatment before the completion of the first part were considered early treatment dropouts. Participants who stopped the treatment afterwards were considered late treatment dropouts. Details about participants’ treatment adherence, including their reasons for dropout, treatment experiences, and predictors for dropout, have been published previously [25].
Measures
Eating disorder psychopathology
ED psychopathology, our primary outcome, was assessed with the Dutch version of the Eating Disorder Examination-Questionnaire (EDE-Q) [26, 27]. The EDE-Q is a self-report questionnaire that assesses the frequency of eating disordered symptoms in a 28-day period. EDE-Q generates a global scale, as well as four subscales (restraint, eating concern, shape concern, weight concern). The items were scored on a 7-point Likert scale (0–6), with a higher score reflecting greater psychopathology. The EDE-Q also measures the key behavioral features of EDs (e.g., number of binge eating episodes, purging, laxative use). Although addressing these behaviors was one of the main goals of the web-based CBT, we did not include them as outcome measures, given the limited reliability of measuring them with the EDE-Q according to prior studies [28,29,30,31].
Body dissatisfaction
The 20-item body attitude test (BAT) [32, 33] measures the level of body dissatisfaction. The items were scored on a 6-point Likert scale (0–5), with a cut-off score of 36 and a higher score representing a more disordered body experience.
Body mass index (BMI)
Participants’ BMI (kg/m2) was calculated with their self-reported height and weight.
Physical health
Physical health was assessed with the 10-item Maudsley Addiction Profile-Health Symptom Scale (MAP-HSS) [34] and 15 ED-specific physical complaints. All items were scored on a 5-point Likert scale (0–4), with a higher score representing more physical complaints in the past 30 days.
Mental health
The Depression Anxiety Stress Scale (DASS-21) [35] was used to measure participant’s mental health. The DASS-21 is a 21-item self-report questionnaire assessing levels of depression, anxiety, and stress in the past week. Each item was scored on a 4-point Likert scale (0–3), with a higher score representing greater levels of depression, anxiety, and stress.
Self-esteem
Self-esteem was evaluated with the 10-item Rosenberg Self-Esteem Scale (RSES) [36], with a higher score representing a higher level of self-esteem.
Quality of life
The EuroQol visual analogue scale (EQ-5D VAS) [37] was used as indicator of participant’s quality of life. The EQ-5D VAS records participant’s self-rated health on a scale ranging from 0 (‘worst imaginable health state’) to 100 (‘best imaginable health state’).
Social functioning
Social functioning was assessed with nine items of the Measurements in the Addictions for Triage and Evaluation—International Classification of Functioning, Disability and Health (MATE-ICN) [38]. All items were scored on a 5-point Likert scale (1–5), with a higher score representing more problems in social function.
Statistical analyses
The long-term results of the web-based CBT were measured using Mixed Models for Repeated Measures. Time effects were assessed for all participants, for all three ED subgroups (BN, BED, EDNOS), and for completers, early dropouts, and late dropouts. Effect sizes were calculated by subtracting the average score at the 12-month post-treatment follow-up from the average score at baseline, and dividing the result by the standard deviation of the baseline. Effect sizes of 0.8 were considered large, effect sizes of 0.5 were moderate, and effect sizes of 0.2 were seen as small [39]. All analyses were conducted using SPSS version 21.
Results
Participants
Participants were 212 women with BN (n = 44), BED (n = 83), or EDNOS (n = 85) and a mean age of 39.5 (SD 11.6) years. Most participants lived with others (n = 158; 75%), were employed (n = 168; 79%), and had completed higher education (n = 108; 51%). Less than half of the participants (n = 94; 44%) had received prior care for their ED, although many had a long history of disordered eating behavior (13% < 5 years; 13% 5–10 years; 30% 11–20 years; 39% > 20 years).
Treatment dropouts
Sixty percent of the 212 participants (n = 128) completed the web-based CBT. Of the other 84 participants, half completed the first part of the program and dropped out afterwards (n = 42; 20%; late dropouts). The other participants (n = 42; 20%; early dropouts) stopped the treatment during the first part (n = 29) or never started (n = 13). Treatment adherence did not differ significantly between the three ED subgroups.
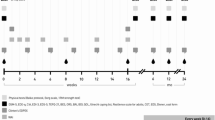
Post-treatment data were available for 180 participants (85%) and at follow-up at 3, 6, and 12 months, for 159 (75%), 157 (74%), and 153 (72%), respectively (Fig. 1). As shown in Fig. 1, the study dropout rates of the three ED subgroups were similar.

CONSORT flow diagram for a randomized controlled trial in patients with eating disorders receiving web-based CBT
Long-term effects of web-based CBT on eating disorder psychopathology
The significant improvement in ED psychopathology during treatment was sustained up to 1 year after treatment (Table 1). The effect size was large (d = 0.97) with a decrease of the mean EDE-Q total score from 3.26 (baseline) to 2.19 (12-month follow-up) (difference − 1.07). No significant differences were found between the effect achieved at post-treatment and the scores at 3, 6, and 12 months of follow-up (data not shown). Similar results were found for the four EDE-Q subscales, with generally large effect sizes for eating concern, shape concern and weight concern, and a moderate effect size for restraint.
Long-term effects of web-based CBT on eating disorder-related health
For all secondary outcomes (except BMI) significant improvements were found between baseline and post-treatment with effect sizes between d = 0.32 and d = 0.70 (Table 1). These effects were maintained up to 1 year after treatment. For body dissatisfaction, the improvement from baseline to post-treatment further progressed at 6- and 12-month follow-up. For participants with a baseline BMI >25, the BMI improved gradually over time and the improvement was significant at all follow-ups. However, effect sizes were small (between d = 0.09 and d = 0.18).
Additional treatment during follow-up
Of all participants, 23% (n = 49) received professional treatment from a GP, therapist or dietician, or completed a web-based treatment elsewhere during the 1-year follow-up period. Most other participants (n = 121; 57%) received no professional treatment during this period. For the remaining participants (n = 42; 20%), information about additional treatment during follow-up was missing.
Receiving additional professional treatment during the 1-year follow-up period resulted in changes in long-term outcomes of similar magnitude: in those receiving additional professional treatment, the mean of the EDE-Q total score changed from 3.43 (baseline) to 2.47 (12-month follow-up) (difference − 0.97), while for those not receiving additional professional treatment, the mean changed from 3.30 (baseline) to 2.12 (12-month follow-up) (difference − 1.18).
Treatment outcomes for subgroups BN, BED, and EDNOS
For all three subgroups (BN, BED, and EDNOS), the improvement in ED psychopathology was significant at post-treatment and remained so at follow-up 1 year later (ESM Appendix 1). Effect sizes were large for all three subgroups both after treatment (between d = 0.75 and d = 0.99) and 1 year later (between d = 0.94 and d = 1.12). All EDE-Q subscales improved between baseline and post-treatment in all subgroups (data not shown), except for the subscale restraint in the EDNOS subgroup. At follow-up, positive results remained and restraint in the EDNOS subgroup had improved significantly compared to baseline. However, restraint in the BN subgroup proved no longer significantly different from baseline.
Regarding secondary outcomes, participants with BN, BED, and EDNOS all improved significantly on physical and mental health, body dissatisfaction, and social functioning during treatment (ESM Appendix 1). These effects were also sustained up to 1-year post treatment with, generally, moderate to large effect sizes for body dissatisfaction, moderate effect sizes for mental health, and small to moderate effect sizes for physical health and social functioning. The BED and EDNOS subgroup also showed significant improvements for self-esteem and quality of life at post-treatment, but those improvements were only sustained at 1-year follow-up for the BED subgroup. Moreover, the improvement in BMI was also significant at 1-year follow-up for participants in the EDNOS subgroup with a BMI >25 at baseline.
Treatment adherence in relation to treatment outcomes
The significant and lasting improvements in ED psychopathology and related health outcomes were applicable for treatment completers, but often not for treatment dropouts (ESM Appendix 2). Late dropouts showed significant improvements in ED psychopathology (at 1-year follow-up) and body dissatisfaction (both, at post-treatment and at 1-year follow-up). For early dropouts, significant improvements were found in physical health (both, at post-treatment and at 1-year follow-up), body dissatisfaction (at 1-year follow-up), and mental health (at post-treatment).
Discussion
This study demonstrated that the reduction of ED psychopathology among women with eating disorders who participated in the web-based CBT sustained up to 1-year post-treatment for all ED subgroups (BN, BED, EDNOS). Improvements in patients’ physical and mental health, body satisfaction, and social functioning also sustained at 1-year follow-up for all ED subgroups. Furthermore, long-term improvements in self-esteem and quality of life were found for patients with BED. The EDNOS subgroup with a BMI >25 at baseline showed additional long-term improvements in body mass index.
Although our dropout rate of 40% is not uncommon in ED treatment [40], this study highlights the importance of treatment completion as positive long-term improvements in ED psychopathology were found primarily in participants who completed the web-based CBT. Regarding ED-related health, also less improvement over time was found for patients who dropped out of the web-based treatment. These results are consistent with results found in other studies [1]. Therefore, improving treatment adherence and compliance should receive more attention to enhance the effectiveness of the web-based treatment.
The improvement in ED psychopathology found in this study is comparable to other studies, although effect sizes in this study were somewhat lower than in previous studies [16,17,18]. This may be explained by differences in treatment adherence, handling of missing data, eating disorder subgroups, type of intervention, or measurements to assess the primary and secondary treatment outcomes. For example, in the study of Ruwaard et al. [17], an effect size of d = 1.5 at post-treatment and d = 1.4 at 1-year follow-up was found for the improvement of ED psychopathology among patients with bulimic symptoms (versus d = 0.8 and d = 1.0, respectively, in our study). Here the percentage of treatment completers was higher and missing data were handled using last-observation-carried-forward (LOCF) data imputation, which is an inferior method compared to mixed models for repeated measures. The study of Wagner et al. [16] also used LOCF data imputation, and different measurements were used to assess ED psychopathology and related health, making a valid comparison of the results of both studies nearly impossible. The study of Mitchell et al. [18] comprised the effects of CBT delivered via videoconferencing compared to CBT delivered face-to-face for patients with BN and bulimic symptoms. It would be interesting to further study the effectiveness of the web-based CBT in comparison to other active CBIs or to traditional face-to-face treatments.
The strengths of this study include a relatively large sample size, rather low study dropout, long-term follow-up, and better way of handling missing data. Furthermore, this study, contrary to previous studies, included participants of all ED subgroups (BN, BED, EDNOS). On the other hand, the lack of reliable information on number of binge eating episodes and purging (due to the limited reliability of the EDE-Q in measuring those behaviors) was an important limitation of our study. Another limitation was the assessment of ED diagnoses using the online self-report questionnaire EDQ-O and additional online questions [41], rather than the gold standard structured in-person clinical interview. However, we considered such a face-to-face interview to be incompatible with the goals of using CBT to reduce barriers to access treatment. The absence of information on the occurrence of comorbidities with other clinically relevant disorders is also a limitation of our study. Furthermore, our sample had a relatively high mean age. Based on the information about the history of the disordered eating behavior, we could determine that participants did not have a late onset of the ED but a long history of disordered eating behavior. In addition, we did not verify whether the ED diagnoses were still applicable during follow-up.
In conclusion, this study shows that web-based treatment can result in long-term improvements in ED psychopathology, body dissatisfaction, physical and mental health, and social functioning in patients with various eating disorders. The main challenge is, however, to minimize dropout and to enhance treatment compliance to achieve optimal treatment outcomes.
What is already known on this subject?
Studies on long-term effectiveness of interned-based interventions for EDs are scarce. More research is needed, given substantial relapse rates and prolonged vulnerability of ED patients to relapse.
What does this study add?
This study showed that the web-based CBT results in long-term improvements in ED psychopathology, body dissatisfaction, physical and mental health, and social functioning in patients with various EDs.
References
Aardoom JJ, Dingemans AE, Spinhoven P, Van Furth EF (2013) Treating eating disorders over the internet: a systematic review and future research directions. Int J Eat Disord 46(6):539–552. https://doi.org/10.1002/eat.22135
Schlegl S, Burger C, Schmidt L, Herbst N, Voderholzer U (2015) The potential of technology-based psychological interventions for anorexia and bulimia nervosa: a systematic review and recommendations for future research. J Med Int Res 17(3):e85. https://doi.org/10.2196/jmir.3554
Becker AE, Hadley Arrindell A, Perloe A, Fay K, Striegel-Moore RH (2010) A qualitative study of perceived social barriers to care for eating disorders: perspectives from ethnically diverse health care consumers. Int J Eat Disord 43(7):633–647. https://doi.org/10.1002/eat.20755
Evans EJ, Hay PJ, Mond J, Paxton SJ, Quirk F, Rodgers B, Jhajj AK, Sawoniewska MA (2011) Barriers to help-seeking in young women with eating disorders: a qualitative exploration in a longitudinal community survey. Eat Disord 19(3):270–285. https://doi.org/10.1080/10640266.2011.566152
Cachelin FM, Striegel-Moore RH (2006) Help seeking and barriers to treatment in a community sample of Mexican American and European American women with eating disorders. Int J Eat Disord 39(2):154–161. https://doi.org/10.1002/eat.20213
Agh T, Kovacs G, Pawaskar M, Supina D, Inotai A, Voko Z (2015) Epidemiology, health-related quality of life and economic burden of binge eating disorder: a systematic literature review. Eat Weight Disord 20(1):1–12. https://doi.org/10.1007/s40519-014-0173-9
Arcelus J, Mitchell AJ, Wales J, Nielsen S (2011) Mortality rates in patients with anorexia nervosa and other eating disorders. A meta-analysis of 36 studies. Arch Gen Psychiatry 68(7):724–731. https://doi.org/10.1001/archgenpsychiatry.2011.74
DeJong H, Oldershaw A, Sternheim L, Samarawickrema N, Kenyon MD, Broadbent H, Lavender A, Startup H, Treasure J, Schmidt U (2013) Quality of life in anorexia nervosa, bulimia nervosa and eating disorder not-otherwise-specified. J Eat Disord 1:43. https://doi.org/10.1186/2050-2974-1-43
Dickstein LP, Franco KN, Rome ES, Auron M (2014) Recognizing, managing medical consequences of eating disorders in primary care. Cleve Clin J Med 81(4):255–263. https://doi.org/10.3949/ccjm.81a.12132
Hart LM, Granillo MT, Jorm AF, Paxton SJ (2011) Unmet need for treatment in the eating disorders: a systematic review of eating disorder specific treatment seeking among community cases. Clin Psychol Rev 31(5):727–735. https://doi.org/10.1016/j.cpr.2011.03.004
de la Rie S, Noordenbos G, Donker M, van Furth E (2006) Evaluating the treatment of eating disorders from the patient’s perspective. Int J Eat Disord 39(8):667–676. https://doi.org/10.1002/eat.20317
Escobar-Koch T, Banker JD, Crow S, Cullis J, Ringwood S, Smith G, van Furth E, Westin K, Schmidt U (2010) Service users’ views of eating disorder services: an international comparison. Int J Eat Disord 43(6):549–559. https://doi.org/10.1002/eat.20741
Loucas CE, Fairburn CG, Whittington C, Pennant ME, Stockton S, Kendall T (2014) E-therapy in the treatment and prevention of eating disorders: a systematic review and meta-analysis. Behav Res Ther 63C:122–131. https://doi.org/10.1016/j.brat.2014.09.011
Grilo CM, Pagano ME, Stout RL, Markowitz JC, Ansell EB, Pinto A, Zanarini MC, Yen S, Skodol AE (2012) Stressful life events predict eating disorder relapse following remission: six-year prospective outcomes. Int J Eat Disord 45(2):185–192. https://doi.org/10.1002/eat.20909
Herzog DB, Dorer DJ, Keel PK, Selwyn SE, Ekeblad ER, Flores AT, Greenwood DN, Burwell RA, Keller MB (1999) Recovery and relapse in anorexia and bulimia nervosa: a 7.5-year follow-up study. J Am Acad Child Adolesc Psychiatry 38(7):829–837. https://doi.org/10.1097/00004583-199907000-00012
Wagner G, Penelo E, Wanner C, Gwinner P, Trofaier ML, Imgart H, Waldherr K, Wober-Bingol C, Karwautz AF (2013) Internet-delivered cognitive-behavioural therapy v. conventional guided self-help for bulimia nervosa: long-term evaluation of a randomised controlled trial. Br J Psychiatry 202:135–141. https://doi.org/10.1192/bjp.bp.111.098582
Ruwaard J, Lange A, Broeksteeg J, Renteria-Agirre A, Schrieken B, Dolan CV, Emmelkamp P (2013) Online cognitive-behavioural treatment of bulimic symptoms: a randomized controlled trial. Clin Psychol Psychother 20(4):308–318. https://doi.org/10.1002/cpp.1767
Mitchell JE, Crosby RD, Wonderlich SA, Crow S, Lancaster K, Simonich H, Swan-Kremeier L, Lysne C, Myers TC (2008) A randomized trial comparing the efficacy of cognitive-behavioral therapy for bulimia nervosa delivered via telemedicine versus face-to-face. Behav Res Ther 46(5):581–592. https://doi.org/10.1016/j.brat.2008.02.004
Zerwas SC, Watson HJ, Hofmeier SM, Levine MD, Hamer RM, Crosby RD, Runfola CD, Peat CM, Shapiro JR, Zimmer B, Moessner M, Kordy H, Marcus MD, Bulik CM (2017) CBT4BN: a randomized controlled trial of online chat and face-to-face group therapy for Bulimia nervosa. Psychother Psychosom 86(1):47–53. https://doi.org/10.1159/000449025
de Zwaan M, Herpertz S, Zipfel S, Svaldi J, Friederich HC, Schmidt F, Mayr A, Lam T, Schade-Brittinger C, Hilbert A (2017) Effect of internet-based guided self-help vs individual face-to-face treatment on full or subsyndromal binge eating disorder in overweight or obese patients: the INTERBED Randomized Clinical Trial. JAMA Psychiatry 74(10):987–995. https://doi.org/10.1001/jamapsychiatry.2017.2150
ter Huurne ED, de Haan HA, Postel MG, van der Palen J, Van Der Nagel JEL, De Jong CAJ (2015) Web-based cognitive behavioral therapy for female patients with eating disorders: randomized controlled trial. J Med Internet Res 17(6):e152. https://doi.org/10.2196/jmir.3946
ter Huurne ED, Postel MG, de Haan HA, DeJong CA (2013) Effectiveness of a web-based treatment program using intensive therapeutic support for female patients with bulimia nervosa, binge eating disorder and eating disorders not otherwise specified: study protocol of a randomized controlled trial. BMC Psychiatry 13:310. https://doi.org/10.1186/1471-244X-13-310
Britt E, Hudson SM, Blampied NM (2004) Motivational interviewing in health settings: a review. Patient Educ Couns 53(2):147–155. https://doi.org/10.1016/S0738-3991(03)00141-1S0738399103001411
Miller JH, Moyers T (2002) Motivational interviewing in substance abuse: applications for occupational medicine. Occup Med 17(1):51–65 (iv)
Ter Huurne ED, Postel MG, de Haan HA, van der Palen J, DeJong CA (2017) Treatment dropout in web-based cognitive behavioral therapy for patients with eating disorders. Psychiatry Res 247:182–193. https://doi.org/10.1016/j.psychres.2016.11.034
Fairburn CG, Beglin SJ (1994) Assessment of eating disorders: interview or self-report questionnaire? Int J Eat Disord 16(4):363–370
van Furth EF (2000) Nederlandse vertaling van de EDE-Q. Robert-Fleury Stichting, Leidschendam
Black CM, Wilson GT (1996) Assessment of eating disorders: interview versus questionnaire. Int J Eat Disord 20(1):43–50. https://doi.org/10.1002/(SICI)1098-108X(199607)20:1%3c43:AID-EAT5%3e3.0.CO;2-4
Luce KH, Crowther JH (1999) The reliability of the eating disorder examination-self-report questionnaire version (EDE-Q). Int J Eat Disord 25(3):349–351
Reas DL, Grilo CM, Masheb RM (2006) Reliability of the Eating Disorder Examination-Questionnaire in patients with binge eating disorder. Behav Res Ther 44(1):43–51. https://doi.org/10.1016/j.brat.2005.01.004
Wilfley DE, Schwartz MB, Spurrell EB, Fairburn CG (1997) Assessing the specific psychopathology of binge eating disorder patients: interview or self-report? Behav Res Ther 35(12):1151–1159
Probst M, Van Coppenolle H, Vandereycken W (1997) Further experience with the body attitude test. Eat Weight Disord 2(2):100–104
Probst M, Vandereycken W, Van Coppenolle H, Vanderlinden J (1995) The body attitude test for patients with an eating disorder: psychometric characteristics of a new questionnaire. Eat Disord J Treat Prev 3(2):133–144
Marsden J, Gossop M, Stewart D, Best D, Farrell M, Lehmann P, Edwards C, Strang J (1998) The Maudsley Addiction Profile (MAP): a brief instrument for assessing treatment outcome. Addiction 93(12):1857–1867
Lovibond PF, Lovibond SH (1995) The structure of negative emotional states: comparison of the Depression Anxiety Stress Scales (DASS) with the beck depression and anxiety inventories. Behav Res Ther 33(3):335–343
Rosenberg M (1965) Society and adolescent child. Princeton University Press, Princeton
Lamers LM, Stalmeier PF, McDonnell J, Krabbe PF, van Busschbach JJ (2005) Measuring the quality of life in economic evaluations: the Dutch EQ-5D tariff. Ned Tijdschr Geneeskd 149(28):1574–1578
Schippers GM, Broekman TG, Buchholz A, Koeter MW, van den Brink W (2010) Measurements in the Addictions for Triage and Evaluation (MATE): an instrument based on the World Health Organization family of international classifications. Addiction 105(5):862–871. https://doi.org/10.1111/j.1360-0443.2009.02889.x
Cohen J (1992) A power primer. Psychol Bull 112(1):155–159
Fassino S, Piero A, Tomba E, Abbate-Daga G (2009) Factors associated with dropout from treatment for eating disorders: a comprehensive literature review. BMC Psychiatry 9:67. https://doi.org/10.1186/1471-244X-9-67
Ter Huurne ED, de Haan HA, Ten Napel-Schutz MC, Postel MG, Menting J, van der Palen J, Vroling MS, DeJong CA (2015) Is the Eating Disorder Questionnaire-Online (EDQ-O) a valid diagnostic instrument for the DSM-IV-TR classification of eating disorders? Compr Psychiatry 57:167–176. https://doi.org/10.1016/j.comppsych.2014.10.019
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This study was approved by the Ethics Committee of Medical Spectrum Twente in March 2011 (reference number NL31717.044.010, P10-31) and registered in the Dutch Trial Registry (NTR2415).
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
ter Huurne, E.D., de Haan, H.A., Postel, M.G. et al. Long-term effectiveness of web-based cognitive behavioral therapy for patients with eating disorders. Eat Weight Disord 26, 911–919 (2021). https://doi.org/10.1007/s40519-020-00929-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40519-020-00929-0