
Abstract
Purpose
The purpose of this study was to examine the influence of mother–daughter communication about their bodies on adolescent girls’ and mothers’ body shame.
Methods
The Actor–Partner Interdependence Model was utilized to estimate relationships between individuals’ body surveillance and their own body shame (actor effect), individuals’ body surveillance and the other member’s body shame (partner effect), and negative body talk and both members’ body shame (relationship effect) in a sample of 100 mother–daughter dyads.
Results
For both mothers and daughters, individuals who had higher body surveillance reported higher body shame. Negative body talk emerged as a significant moderator: girls with higher body surveillance experienced greater body shame when they engaged in more negative body talk with their mothers.
Conclusion
The findings highlight the need for clinicians to address mothers’ own surveillance and body shame, as well as negative body talk between mothers and daughters, in interventions that seek to reduce the impact of objectification on body shame in adolescents.
Level of evidence
Level V, cross-sectional descriptive study.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Objectification of women is pervasive in American society. Across multiple levels of a young person’s socialization, adolescents learn that women are judged and valued on their appearance and their appeal to the male gaze [1, 2]. It is not surprising, then, that girls at a young age already experience the consequences of living in a society that consistently and persistently objectifies women [3, 4]. Although some research has examined these consequences of experiencing objectification (e.g., heightened body surveillance, or frequent self-monitoring of appearance and ensuring that one meets cultural ideals, [5]) in adolescent samples, we still know little about social or relational risk factors that may be modifiable to reduce the risks associated with objectification. Identifying these exacerbating influences is critical for clinical interventions seeking to buffer young women from experiencing body shame. As such, the purpose of this study is to examine the influence of mother–daughter communication about their bodies on adolescent girls’ and their mothers’ body shame in a sample of 100 mother–daughter dyads.
Mother–adolescent relationship and objectification
Although the primary mechanisms by which experiencing objectification affects adolescent girls have been supported (e.g., [3, 4, 6, 7]), we know little about how relational factors, particularly mother–daughter interactions, may buffer or put at greater risk, young girls living in our society. Based on the Social Learning Theory [8], models in children’s lives (particularly same gender models, [9]) influence gender-related behaviors and attitudes. Although boys and men also experience objectification, the prevalence of objectification of girls and women is high [10]. Women and girls continue to experience higher rates of objectification compared to men [11] and mass and social media continue to present idealized and objectified images of women and girls at great rates [12]. Further, evidence suggests that adolescent females may be more susceptible to the negative effects of objectification on their body image, compared to boys [13]. Thus, the focus on this study is limited to adolescent females and their mothers. Prior research has suggested that mothers’ modeling of gender-related behaviors and attitudes influences their daughters’ internalization of objectification. For example, one study examined the links between media consumption and young girls’ self-sexualization and found that mothers’ own self-objectification moderated the relation between media consumption and young girls’ self-sexualization [14]. In other words, mothers’ modeling of self-objectification may increase young girls’ risk of internalizing gendered behaviors and attitudes.
To our knowledge, only one study with young adolescent–mother dyads examined protective factors related to body surveillance and body shame. Katz-Wise et al. [15] investigated the influence of mother–adolescent relationship quality and mothers’ own body surveillance and body shame as predictors of adolescents’ body surveillance and body image. Katz-Wise et al. [15] reported mixed findings: on the one hand, mothers’ body shame did associate with greater body surveillance in adolescents; however, greater body surveillance in mothers did not predict body shame in adolescents. The authors propose that individuation in the adolescents may lead adolescents to not model mothers’ self-objectifying attitudes and behaviors. However, it could also be that other moderating factors may be playing a role. For example, how mothers and daughters communicate about body size may be a factor contributing to daughters’ body surveillance and body shame.
Numerous studies have examined the ways that mothers communicate about weight with their children, and have generally found that talk about weight confers negative outcomes for youth, such as symptoms of depression, lower self-worth, and disordered eating behaviors (e.g., [16, 17]). A distinct type of weight-related talk that has been studied of late is “fat talk,” or communication between two individuals that consists of disparaging comments about one’s own weight or body size [18]. A recent meta-analysis on fat talk and its correlates indicated that fat talk (typically between peers or friends) is associated with and likely precedes components of body image disturbance, such as body surveillance and body shame [19]. Although most research on fat talk, also termed “negative body talk,” has been examined between individuals and their friends (e.g., [20,21,22]), recent investigations have considered other socializing agents, such as mothers. Given the role that mothers play in implicitly influencing daughters’ gendered behaviors and attitudes via modeling, it is likely that more explicit communication about weight and appearance could also impact aspects of young women’s body image.
Mother–daughter negative body talk
To date, two studies [23, 24] have investigated mother–daughter negative body talk and how this type of weight communication associates with outcomes, such as body surveillance and body dissatisfaction. This seminal research found that, consistent with Social Learning Theory [8], there was a positive direct effect of mothers’ levels of self-objectification on their adult daughters’ reported self-objectification [23]. They also found that co-rumination about weight explained the association between mothers’ and daughters’ self-objectification [23]. In other words, the way that mothers may pass on self-objectification is through overt discussions about weight. Related to the outcomes of self-objectification, Arroyo and Andersen [24] found in the same sample of young adult women and mothers, that fat talk predicted bulimic tendencies in the adult daughters, again supporting that mother–daughter negative body talk may be a risk factor for the consequences of self-objectification, at least in adult women. To our knowledge, only one study [25] has examined the impact of negative body talk between mothers and their younger adolescent daughters. Chow and Tan (2017) found that daughters reported greater disordered eating when they and their mothers had higher levels of negative body talk [25]. Given the interactive effect that mother–daughter negative body talk has on disordered eating in younger adolescents [25], and that it is a contributing factor to body surveillance and body dissatisfaction in adult daughters, it is likely that mother–daughter negative body talk likewise accounts for experiences of body surveillance and body shame in younger adolescents.
Current study
Based on the Social Learning Theory, we hypothesize the following to be examined in our cross-sectional study:
Hypothesis 1
Mothers’ body surveillance and body shame will positively associate with adolescents’ body surveillance and body shame, respectively.
Hypothesis 2
Negative body talk will moderate the associations between body surveillance and body shame for both adolescents and mothers, such that stronger associations between body surveillance and body shame will occur for mothers and adolescents higher in negative body talk.
Method
Participants and procedures
Mother–daughter dyads were recruited from a Midwestern metropolitan area in the USA. Electronic flyers posted on webpages (e.g., Facebook, Craigslist) and physical flyers posted at community centers (e.g., colleges and schools) were employed to recruit adolescent girls (11–18 years old) and their mothers. Mother–daughter dyads interested in the study would contact the researchers through emails or phone calls for scheduling a study session. On their scheduled dates, the mother–daughter dyads were invited to the psychology department’s laboratory for the study’s procedures. The participants were told that the purpose of the study was to examine adolescent girls’ social relationships and how they are important for psychological and physical health. During the laboratory sessions, the researchers first provided the mother–daughter dyads an overview of the study (e.g., goals, benefits, participant rights). Both adolescents and their mothers were required to provide written informed consent before participating. Adolescents and their mothers were then assigned to separate rooms to complete a computer-administered survey. Although not reported in this study, adolescents and their mothers also completed two video-recorded interactions. To compensate for their participation, each mother–daughter dyad received a $40 grocery gift card. This study was approved by the authors’ institutional review board.
The current sample included 100 adolescent girls (Mage = 14.34 years, SD 2.31) and their mothers (Mage = 44.06 years, SD 7.23). According to mother report, about 48% of the adolescents were Caucasian, followed by African American (30%), Mixed race/Other (15%), Asian (4%), Hispanic (2%), and Middle Eastern (1%). Furthermore, the majority of the mothers reported a household income of $35,000 or above (79%) and had at least some college education (90%). The median income for the country in which the data were collected was around $41,000; and the current study’s sample was quite representative of the residence in the area. About 60% of the mothers reported that they were married, 14% were single, 17% were divorced, and 9% were either widowed or other relationship status that is not listed above. Mothers’ and daughters’ body mass index (BMI; kg/m2) was computed based on their self-reported weight and height. For this study, mothers’ mean BMI was 30.27 (SD 7.54), falling within the obese category. The mean daughters’ BMI was 23.01 (SD 6.54) and with a percentile of 56%, representing a healthy weight status.
Measures
Body surveillance
Mothers and daugthers completed the Objectified Body Consciousness Scale [5] to capture their body surveillance (8 items). The body surveillance subscale captured individuals’ tendency to monitor and think about their appearance (e.g., “During the day, I think about how I look many times.”). The items were on a 7-point Likert scale, ranging from 1 (strongly disagree) to 7 (strongly agree). Composite scores were computed by averaging the corresponding items, such that higher scores reflect higher body surveillance. The alpha coefficients for both mothers’ and daugthers’ body surveillance were satisfactory (Cronbach’s alphas = 0.78 and 0.79, respectively). Reliability and validity of the OBC scale have been demosntrated in various age groups (e.g., adult, adolescent) and ethnicities (e.g., White, Black women [5, 26, 27]).
Body shame
Mothers and daughters completed the Objectified Body Consciousness Scale [5] to capture their body shame (8 items). The body shame subscale captured individuals’ tendency to feel shame and guilt when they do not meet the cultural expectations for their appearance (e.g., “I feel ashamed of myself when I haven’t made the effort to look my best.”). The items were on a 7-point Likert scale, ranging from 1 (strongly disagree) to 7 (strongly agree). Composite scores were computed by averaging the corresponding items, such that higher scores reflect higher body shame. The alpha coefficients for both mothers’ and daughters’ body shame were satisfactory (Cronbach’s alphas = 0.80 and 0.80, respectively).
Negative body talk
To capture negative body talk, mothers and daughters were asked to complete the Body Talk Scale [28]. They were asked to first imagine a scenario in which they say negative things about their own bodies with each other (for example, “My stomach is too big” or “I need to tone up my abs”). They then answered a series of 3 items, including: (1) How often would this [negative body talk] occur between you and your mother/daughter?, (2) How often do you say negative things about your physical appearance in front of your mother/daughter?, and (3) How often does your mother/daughter say negative things about her physical appearance in front of you?. Participants rated the items on a scale ranging from 1 (never) to 5 (very frequently). A composite score was computed by averaging the corresponding items. The alpha coefficients for both mothers’ and daugthers’ body talk were acceptable, with Cronbach’s alphas 0.70 and 0.74, respectively. Reliability and validity of the negative body talk subscale have been demonstrated in the previous research [21, 22, 28] showing that negative body talk was related to depressive symptoms, body dissatisfaction, disordered eating behaviors, and lower self-esteem. Mothers’ and daughters’ reports of negative body talk were significantly related, r = 0.38, p < 0.01. Because body talk reflects a dyadic construct, both mothers’ and daughters’ reports were averaged to form a composite score of overall body talk in the relationship. Previous research shows this method of measuring negative body talk with a composite score to be valid [21, 22].
Analysis plan
Preliminary analyses were first conducted to examine descriptive statistics and correlations for the target variables. Then, the Actor–Partner Interdependence Model (APIM) was used to examine the main hypotheses [29, 30]. As depicted in Fig. 1, the APIM estimated the actor effects of individuals’ body surveillance on their own body shame, and the partner effects of individuals’ body surveillance on other member’s body shame (Hypothesis 1). This model also estimated the direct association between negative body talk and both members’ body shame, along with two interaction terms: (1) negative body talk with mothers’ body surveillance and (2) negative body talk with daughters’ body surveillance. These interaction effects examined whether body talk would moderate the actor and partner effects of body surveillance and body shame, for both mothers and daughters (Hypothesis 2). The model accounted for the degree of interdependence between mothers and daughters in the predictor and outcome variables (reflected as covariances). In this model, age and BMI of mothers and their daughters were included as covariates; these variables have been shown to be related to body image disturbance [31]. All predictors were standardized to the mean, and the interaction terms were computed based on the standardized predictors [32]. The APIM was estimated with Structural Equation Modeling (SEM) implemented by R’s lavaan package [33].

Actor–partner interdependence model depicting actor and partner effects of body surveillance and body shame. Double-headed arrows represent the covariance between two members. Body talk is conceptualized as a dyadic construct that moderates the actor and partner effects. Although not shown in the figure, BMI and age of both members were included as control variables. R2s for daughter’s body shame was 0.51 and for mother’s body shame was 0.34. Unstandardized beta coefficients along with standard errors (in parentheses) are presented. *p < 0.05
Results
Preliminary analyses
Due to a small amount of missing data across the observed variables, we employed the Full Information Maximum Likelihood (FIML) estimator for handling the missing observations [34]. This approach was used to estimate the descriptive statistics, correlations, and APIM. Descriptive statistics and correlations of all variables are presented in Table 1. Negative body talk was related to self- and other- body surveillance. Negative body talk was related to mothers’ body shame, but not daughters’ body shame. Mothers’ and daughters’ body surveillance was related to their own body shame, but not each other’s body shame.
Actor–partner interdependence model
Figure 1 presents the APIM findings. The APIM was a saturated model and thus, no fit indices were reported.
Actor effects
Actor effect showed that mothers who had higher body surveillance reported higher body shame. Similarly, actor effect showed that daughters who had higher body surveillance also reported higher body shame.
Partner effects
Partner effect showed that mothers’ body surveillance was not significantly related to their daughters’ body shame. Similarly, partner effect showed that daughters’ body surveillance was not significantly related to their mothers’ body shame.
Actor–partner interaction effects
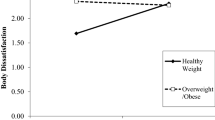
The direct association between negative body talk was not related to mothers’ and daughters’ reports of body shame. The association between daughters’ body surveillance and their own body shame was significantly moderated by negative body talk (moderated actor effect; Hypothesis 2). Simple slopes analyses were conducted to examine the actor effect of daughters’ body surveillance on body shame, depending on high (1 SD above mean) and low (1 SD below mean) levels of negative body talk [32]. The simple slopes are plotted in Fig. 2. Specifically, the results showed that the association between adolescent girls’ body surveillance and body shame was stronger among mother–daughter dyads with more negative body talk (b = 0.83, SE 0.14, p < 0.01), compared to mother–daughter dyads who engaged in less negative body talk (b = 0.40, SE 0.13, p < 0.01). No other moderating effects of body talk emerged as significant.

Interaction between daughters’ body surveillance and body shame, moderated by body talk
Discussion
This study extended previous work using a dyadic design by examining the relational risk factors, particularly negative body talk in mothers and their daughters, in moderating the link between mothers’ and adolescents’ body surveillance and body shame. The strength of the dyadic design is that it allows the examination of which individuals within a dyadic system (i.e., mother–daughter) are more influential in one’s body shame when engaging in negative body talk. Given that most extant work focuses only on mothers’ influence on daughters’ body image issues, despite the possibility that mothers and daughters may jointly influence and regulate each other’s body dissatisfaction, using the dyadic design allowed us to consider the interdependence between mother–daughter dyad’s characteristics on their outcomes simultaneously [35].
We found actor effects such that greater body surveillance was associated with body shame for both mothers and adolescents. However, contrary to our expectations that mothers’ modeling of body surveillance may increase adolescents’ body shame, the partner effects of body surveillance on body shame were not significant for either mothers or daughters. It appears that exposure to each other’s body surveillance, as examined in the partner effects, has a relatively weaker association with body shame compared to individuals’ own internalization of body surveillance. The hierarchical nature of the mother–child relationship may explain for the lack of partner effect of adolescents’ body surveillance on mothers’ body shame, such that adults may be less susceptible to change in response to children’s behaviors and attitudes. In addition, our finding is also consistent with prior work that found that mothers’ body surveillance was not associated adolescents’ body shame [15]. This may be due to the individuation process, where adolescents may behave independently from their parents to achieve positive well-being and self-esteem (e.g., identity formation; [36]). Hence, the individuation in adolescents may lead adolescents to not model their mothers’ behaviors and attitudes.
Although negative body talk was found to be directly related to body image issues in previous research [23, 24], the current expanded prior work using a dyadic design to identify which individuals within a dyadic system (i.e., mother–daughter) are more influential in one’s body shame when engaging in negative body talk. Consistent with the Social Learning Theory that postulates that learning involves behavioral (e.g., reinforcement) and cognitive factors (e.g., motivation) [8], we found that negative body talk interacted with body surveillance to predict body shame in adolescent girls. Specifically, higher body surveillance predicted greater body shame for girls who engaged in more negative body talk with their mothers, but not for those who engaged in low levels of negative body talk with their mothers. First, it is likely that during weight communication between mothers and daughters, adolescent girls may experience the reinforcement of how our society values thinness (behavioral factor), hence adolescent girls may feel pressure to be thin. As a result, adolescent girls may be motivated to live up to the society expectations of thin body ideal (cognitive factor), thus experiencing an increase in body shame. Indeed, this is supported in previous experimental research (i.e., exposure to social pressure to be thin increased young women’s body dissatisfaction [37]). Second, it is also possible that during weight communication, girls with heightened body surveillance may be reminded of their own body dissatisfaction thus experiencing more body shame. Indeed, prior work has shown that engagement in body talk was associated with greater body dissatisfaction (see review conducted by [38]).
However, negative body talk did not moderate the associations between body surveillance and body shame for mothers. One possible reason is that mothers may already have body shame from years of socialization; thus, they may not be influenced by their daughters’ own body surveillance. Indeed, research suggests that adults’ body image disturbances are rather stable after adolescence [39]. In addition, it is important to consider the hierarchical structure within the family, especially in the mother–daughter relationship. Although parent–child relationships become more egalitarian over the course of development [40], the hierarchical structure may not be fully dismissed until adulthood [41].
Limitation and future directions
It is important to note that this study was cross-sectional in nature and did not allow us to draw causal explanations among the variables. For instance, although the current model predicted that body surveillance preceded body shame, the reverse causality is also possible [42]. Interestingly, the line of research on body checking suggests that although negative body image may increase the frequency of body checking, the frequent checking of body size may also serve to reinforce body dissatisfaction [43, 44]. Indeed, a recent experimental study found that participants who were allowed to retake and retouch their selfies (self-taken photos) experienced more negative body image than participants who were asked to upload an untouched selfies or the control group [45]. Nonetheless, future research could adopt a longitudinal design that addresses the directional linkages among body surveillance, body shame, and body talk.
Another limitation was that this study only focused on the negative aspect of body talk but did not consider the content of this talk. Thus, we do not know, for certain, what physical attributes were most negatively discussed (i.e., some individuals may be concerned about appearing too skinny or not curvy enough, or mothers may have made comments about appearing older). Future research should clarify the content of this negative body talk (thin-ideal related versus age-related). Similarly, we did not measure positive body talk. It is likely that mother–daughter dyads may engage in supportive and encouraging forms of discussion about weight. A recent study showed that positive body talk was not associated with negative outcomes, and that this type of weight communication is protective against pathological eating, especially among individuals with lower weight status [46]. Thus, future research could investigate the differential influence of types of body talk on adolescent health and mental health outcomes.
This current sample only consisted of mothers and their daughters because of the prevalence of body image issues among females. Nonetheless, future work should consider examining similar research questions with male participants, as some work suggests that adolescent boys also experience similar body image issues, although it could manifest differently (e.g., men/boys are being pressured to be masculine or muscular [47]). Finally, although we had 100 mother–daughter dyads (i.e., 200 participants), the sample is relatively small. Future research should seek to include a larger sample size, with a greater diversity of participants.
Conclusions
This study revealed the importance of investigating relational risk factors to better understand the body surveillance-body shame link in mother–daughter dyads. We demonstrated that when girls have high body surveillance, negative body talk between them and their mothers increases the level of body shame. To reduce body shame among girls with high body surveillance, mothers may be encouraged to minimize their expression of body dissatisfaction with their daughters. Hence, these results have practical implications for clinicians and practitioners who work with adolescents with body image issues. Specifically, clinicians and practitioners may consider the role of mothers’ own surveillance and body shame, as well as the existence of negative body talk within dyads when designing interventions.
What is already known on this subject?
Prior research has examined consequences of experiencing objectification (e.g., heightened body surveillance, or frequent self-monitoring of appearance) in adolescent samples. However, little is known about social or relational risk factors that may be modifiable to reduce the risks associated with objectification. Identifying these exacerbating influences is critical for clinical interventions seeking to buffer young women from experiencing body shame.
What your study adds?
We demonstrated that when girls have high body surveillance, negative body talk between mothers and daughters increases the level of body shame. To reduce body shame among girls with high body surveillance, mothers may be encouraged to minimize their expression of body dissatisfaction with their daughters. Hence, these results have practical implications for clinicians and practitioners who work with adolescents with body image issues.
References
Fredrickson BL, Roberts T-A (1997) Objectification theory: toward understanding women’s lived experiences and mental health risks. Psychol Women Q 21:173–206. https://doi.org/10.1111/j.1471-6402.1997.tb00108.x
Moradi B, Huang YP (2008) Objectification theory and psychology of women: a decade of advances and future directions. Psychol Women Q 32:377–398. https://doi.org/10.1111/j.1471-6402.2008.00452.x
Slater A, Tiggemann M (2010) Body image and disordered eating in adolescent girls and boys: a test of objectification theory. Sex Roles 63:42–49. https://doi.org/10.1007/s11199-010-9794-2
Slater A, Tiggemann M (2002) A test of objectification theory in adolescent girls. Sex Roles 46:343–349. https://doi.org/10.1023/A:1020232714705
McKinley NM, Hyde JS (1996) The objectified body consciousness scale development and validation. Psychol Women Q 20:181–215. https://doi.org/10.1111/j.1471-6402.1996.tb00467.x
Grabe S, Hyde JS, Lindberg SM (2007) Body objectification and depression in adolescents: the role of gender, shame, and rumination. Psychol Women Q 31:164–175. https://doi.org/10.1111/j.1471-6402.2007.00350.x
Grabe S, Hyde JS (2009) Body objectification, MTV, and psychological outcomes among female adolescents. J Appl Soc Psychol 39:2840–2858. https://doi.org/10.1111/j.1559-1816.2009.00552.x
Bussey K, Bandura A (1999) Social cognitive theory of gender development and differentiation. Psychol Rev 106:676
Perry DG, Bussey K (1979) The social learning theory of sex differences: imitation is alive and well. J Pers Soc Psychol 37:1699. https://doi.org/10.1037/0022-3514.37.10.1699
Holland E, Koval P, Stratemeyer M, Thomson F, Haslam N (2017) Sexual objectification in women’s daily lives: a smartphone ecological momentary assessment study. Br J Soc Psychol 56:314–333. https://doi.org/10.1111/bjso.12152
Hatton E, Trautner MN (2011) Equal opportunity objectification? The sexualization of men and women on the cover of rolling stone. Sex Cult 15:256–278. https://doi.org/10.1007/s12119-011-9093-2
Davis SE (2018) Objectification, sexualization, and misrepresentation: social media and the college experience. Social Media + Society 4:2056305118786727. https://doi.org/10.1177/2056305118786727
Hargreaves DA, Tiggemann M (2004) Idealized media images and adolescent body image: “comparing” boys and girls. Body Image 1:351–361. https://doi.org/10.1016/j.bodyim.2004.10.002
Starr CR, Ferguson GM (2012) Sexy dolls, sexy grade-schoolers? Media & maternal influences on young girls’ self-sexualization. Sex Roles 67:463–476. https://doi.org/10.1007/s11199-012-0183-x
Katz-Wise SL, Budge SL, Lindberg SM, Hyde JS (2013) Individuation or identification? Self-objectification and the mother–adolescent relationship. Psychol Women Q 37:366–380. https://doi.org/10.1177/0361684312468425
Bauer KW, Bucchianeri MM, Neumark-Sztainer D (2013) Mother-reported parental weight talk and adolescent girls’ emotional health, weight control attempts, and disordered eating behaviors. J Eat Disord 1:45. https://doi.org/10.1186/2050-2974-1-45
Neumark-Sztainer D, Bauer KW, Friend S, Hannan PJ, Story M, Berge JM (2010) Family weight talk and dieting: how much do they matter for body dissatisfaction and disordered eating behaviors in adolescent girls? J Adolesc Health 47:270–276. https://doi.org/10.1016/j.jadohealth.2010.02.001
Nichter M, Vuckovic N (1994) Fat talk: body image among adolescent girls. In Many mirrors: body image and social relations. Rutgers University Press, New Brunswick
Mills J, Fuller-Tyszkiewicz M (2017) Fat talk and body image disturbance: a systematic review and meta-analysis. Psychol Women Q 41:114–129. https://doi.org/10.1177/0361684316675317
Chow CM, Ruhl H, Tan CC, Ellis L: Fear of fat and restrained eating: negative body talk between female friends as a moderator. Eating and Weight Disorders-Studies on Anorexia, Bulimia and Obesity 2017:1-8. https://doi.org/10.1007/s40519-017-0459-9
Tan CC, Chow CM (2014) Weight status and depression: moderating role of fat talk between female friends. Journal of health psychology 19:1320–1328. https://doi.org/10.1177/1359105313488982
Chow CM, Tan CC (2016) Weight status, negative body talk, and body dissatisfaction: a dyadic analysis of male friends. Journal of health psychology 21:1597–1606. https://doi.org/10.1177/1359105314559621
Arroyo A, Andersen KK (2016) Appearance-related communication and body image outcomes: fat talk and old talk among mothers and daughters. Journal of Family Communication 16:95–110. https://doi.org/10.1080/15267431.2016.1144604
Arroyo A, Andersen KK (2016) The relationship between mother–daughter self-objectification: identifying direct, indirect, and conditional direct effects. Sex Roles 74:231–241. https://doi.org/10.1007/s11199-015-0554-1
Chow C, Tan C (2017) The role of fat talk in eating pathology and depressive symptoms among mother–daughter dyads. Body image 24:36–43. https://doi.org/10.1016/j.bodyim.2017.11.003
Dakanalis A, Timko AC, Clerici M, Riva G, Carrà G (2017) Objectified body consciousness (OBC) in eating psychopathology: construct validity, reliability, and measurement invariance of the 24-item OBC scale in clinical and nonclinical adolescent samples. Assessment 24:252–274. https://doi.org/10.1177/1073191115602553
Kelly NR, Mitchell KS, Gow RW, Trace SE, Lydecker JA, Bair CE, Mazzeo S (2012) An evaluation of the reliability and construct validity of eating disorder measures in white and black women. Psychol Assess 24:608. https://doi.org/10.1037/a0026457
Rudiger JA, Winstead BA (2013) Body talk and body-related co-rumination: associations with body image, eating attitudes, and psychological adjustment. Body Image 10:462–471. https://doi.org/10.1016/j.bodyim.2013.07.010
Chow CM, Claxton SE, van Dulmen MH (2015) Testing dyadic mechanisms the right way: a primer into moderated actor–partner interdependence model with latent variable interactions. Emerging adulthood 3:421–433. https://doi.org/10.1177/2167696815605728
Garcia RL, Kenny DA, Ledermann T (2015) Moderation in the actor–partner interdependence model. Personal Relationships 22:8–29. https://doi.org/10.1111/pere.12060
Bully P, Elosua P (2011) Changes in body dissatisfaction relative to gender and age: the modulating character of BMI. The Spanish journal of psychology 14:313–322. https://doi.org/10.5209/rev_SJOP.2011.v14.n1.28
Aiken LS, West SG, Reno RR (1991) Multiple regression: testing and interpreting interactions. Sage, Thousand Oaks
Rosseel Y (2012) Lavaan: an R package for structural equation modeling and more. Version 0.5–12 (BETA). Ghent University, Ghent
Allison PD (2003) Missing data techniques for structural equation modeling. J Abnorm Psychol 112:545. https://doi.org/10.1037/0021-843X.112.4.545
Cook WL, Kenny DA (2005) The actor–partner interdependence model: a model of bidirectional effects in developmental studies. Int J Behav Dev 29:101–109. https://doi.org/10.1080/01650250444000405
Grotevant HD, Cooper CR (2005) Individuality and connectedness in adolescent development. In: Elisabeth E, Skoe AE (eds) Personality development in adolescence: a cross national and life span perspective. Routledge, London, pp 3–37
Stice E, Maxfield J, Wells T (2003) Adverse effects of social pressure to be thin on young women: an experimental investigation of the effects of “fat talk”. Int J Eat Disord 34:108–117. https://doi.org/10.1002/eat.10171
Shannon A, Mills JS (2015) Correlates, causes, and consequences of fat talk: a review. Body Image 15:158–172. https://doi.org/10.1016/j.bodyim.2015.09.003
Tiggemann M (2004) Body image across the adult life span: stability and change. Body Image 1:29–41. https://doi.org/10.1016/S1740-1445(03)00002-0
De Goede IH, Branje SJ, Meeus WH (2009) Developmental changes in adolescents’ perceptions of relationships with their parents. J Youth Adolesc 38:75–88. https://doi.org/10.1007/s10964-008-9286-7
Galambos N, Kotylak L (2012) Transformations in parent-child relationships from adolescence to adulthood. From adolescence to young adulthood, Relationsh Pathw, pp 23–42
Roberts T-A, Gettman JY (2004) Mere exposure: gender differences in the negative effects of priming a state of self-objectification. Sex Roles 51:17–27. https://doi.org/10.1023/B:SERS.0000032306.20462.22
Reas DL, Whisenhunt BL, Netemeyer R, Williamson DA (2002) Development of the body checking questionnaire: a self-report measure of body checking behaviors. Int J Eat Disord 31:324–333. https://doi.org/10.1002/eat.10012
Walker DC, White EK, Srinivasan VJ (2018) A meta-analysis of the relationships between body checking, body image avoidance, body image dissatisfaction, mood, and disordered eating. Int J Eat Disord 51:745–770. https://doi.org/10.1002/eat.22867
Mills JS, Musto S, Williams L, Tiggemann M (2018) “Selfie” harm: effects on mood and body image in young women. Body image 27:86–92. https://doi.org/10.1016/j.bodyim.2018.08.007
Hart E, Chow CM, Tan CC (2017) Body talk, weight status, and pathological eating behavior in romantic relationships. Appetite 117:135–142. https://doi.org/10.1016/j.appet.2017.06.012
Murray T, Lewis V (2014) Gender-role conflict and men’s body satisfaction: the moderating role of age. Psychol Men Mascul 15:40. https://doi.org/10.1037/a0030959
Funding
No funding to report.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest to report.
Ethical approval
Eastern Michigan University Institutional Review Board approved study.
Informed consent
Obtained informed consent from adult participants and adolescent assent.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Domoff, S.E., Tan, C.C. & Chow, C.M. Mother–daughter negative body talk as a moderator between body surveillance and body shame in adolescent girls. Eat Weight Disord 26, 941–948 (2021). https://doi.org/10.1007/s40519-020-00925-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40519-020-00925-4