
Abstract
Background
Impulsivity has been shown to be associated with obesity through links to pathological eating behavior such as binge eating. The recent literature suggests that impulsivity is linked to poorer outcomes post-bariatric surgery. Impulsivity can be measured in various ways and comprises of three broad domains: impulsive choice, impulsive action, and impulsive personality traits. The aim of this systematic review is to synthesize the current evidence on the impact of impulsivity on post-bariatric surgery weight loss.
Methods
A literature review was performed in February 2020. Original studies investigating the relationship between impulsivity and weight loss post-bariatric surgery were evaluated.
Results
Ten studies with a total of 1246 patients were analyzed. There were four case–control, four prospective observational and two retrospective observational studies. The postoperative follow-up ranged from 0.5 to 12 years. Eight studies measuring trait impulsivity did not show any association with weight loss post-bariatric surgery, although two studies reported an indirect effect of impulsivity on weight loss mediated via pathological eating behavior. Assessment of impulsive action by two studies showed that post-bariatric surgery weight loss is affected by impulsive action.
Conclusion
Impulsivity may adversely affect postoperative outcomes after bariatric surgery. However, this may be specific to state impulsivity or impulsive action rather than trait impulsivity. Patients with a higher state impulsivity may benefit from closer follow-up post-bariatric surgery, as well as cognitive behavioral therapies targeting cognitive control over food.
Level of evidence
Level I, systematic review.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Impulsivity and its effect on obesity are incredibly complex, and both impulsivity and obesity are multidimensional and multifactorial in nature. The International Society for Research on Impulsivity defined impulsivity as ‘behavior without adequate thought, the tendency to act with less forethought than do most individuals of equal ability and knowledge or a predisposition toward rapid, unplanned reactions to internal or external stimulus without regard to the negative consequences of these reactions’ [1]. Impulsivity has been shown to be associated with obesity through links to pathological eating behavior such as binge eating and various other maladaptive eating styles [2,3,4]. Impulsivity has also been postulated to result in obesity through uncontrolled and excessive food intake [2]. Based on the above definition of impulsivity, an impulsive person, who is obese and overeats, is more likely to continue this same behavior after bariatric surgery, leading to weight regain and failure of intervention. However, efforts to draw a direct relationship between impulsivity and weight regain after bariatric surgery are often hampered by the complex nature of both impulsivity and obesity.
The simple definition of impulsivity by the International Society for Research on Impulsivity belies its multidimensional construct. Impulsivity can be measured in various ways and comprises of three broad domains: impulsive choice, impulsive action, and impulsive personality traits [5]. Impulsive choice is characterized by a preference for more immediate but smaller rewards, over delayed but larger rewards. One measure of impulsive choice is the delay discounting task (DDT) [6]. Impulsive action refers to the capacity or failure to inhibit an inappropriate motor response to prepotent stimuli and can be assessed using go/no-go and stop-signal tasks [7]. Impulsive choice and impulsive action are often collectively known as ‘state impulsivity.’ The third domain of impulsivity is that of impulsivity as a personality trait, or also referred to as ‘trait impulsivity.’ Personality traits are persisting underlying tendencies to behave in particular ways in particular situations, and trait impulsivity can be assessed using the Barratt Impulsiveness Scale [8] and the UPPS-P impulsive behavior scale.
Bariatric surgery is currently the most effective treatment for severe obesity and other obesity-related comorbidities, with mean postoperative excess body weight loss ranging from 65.1–83.4% within the first 2–3 years [9]. The maintenance of weight loss post-surgery has been variable, with weight regain observed in up to 50% of patients 2 years after surgery [10]. The factors for a successful bariatric surgery are multi-fold, ranging from metabolic to psychological variables [11, 12]. In recent years, multiple studies have shown that the bariatric surgery population have an increased incidence of psychiatric conditions [13, 14], and that psychopathology is associated with poorer outcomes following surgery [15, 16].
Despite the emerging literature since 2015 linking impulsivity to poorer outcomes post-bariatric surgery [12, 16,17,18,19,20], the assessment of impulsivity is problematic due to its multidimensional nature. This is further complicated by the fact that the processes may repeatedly change over the course of addiction [21] as well as the lifespan of the patient [22]. This paper aims to synthesize the available literature on the effect of impulsivity on weight loss after bariatric surgery and to tease apart the relationship between the different domains of impulsivity and weight regain after bariatric surgery.
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were adhered to in performing and reporting of this systematic review [23].
Data sources
A comprehensive literature search was conducted in February 2020 using PubMed/MEDLINE, Embase, and the Cochrane Database of Systematic Reviews. The search was performed using medical subject headings (MeSH) and keywords, as well as all possible combination of terms from the following two groups: (1) ‘bariatric surgery,’ ‘metabolic surgery,’ ‘sleeve gastrectomy,’ ‘gastric bypass,’ ‘RYGB,’ ‘gastric band,’ ‘gastroplasty,’ ‘biliopancreatic diversion,’ and ‘duodenal switch’; and (2) ‘impulsivity,’ ‘impulsiveness,’ ‘impulsive choice,’ ‘impulsive action,’ ‘impulsive trait,’ ‘delay discounting task,’ ‘go/no-go,’ ‘stop-signal task,’ ‘Barratt impulsiveness scale,’ ‘Minnesota multiphase personality inventory,’ ‘behavioral/externalizing dysfunction,’ ‘temporal discounting task,’ ‘stop-signal reaction time,’ ‘stroop task,’ ‘Karolinska Scales of personality,’ ‘urgency premeditation perseverance sensation seeking positive urgency impulsive behavior scale,’ and ‘UPPS-P.’ All titles and abstracts of the articles identified through the search were screened against the study selection criteria. The full texts of potentially relevant articles were assessed. A reference list search was conducted based on the extracted full-text articles as well as relevant review articles. The study selection criteria were also applied to articles identified from the reference search. Two reviewers, LG and YJZ, independently conducted title and abstract screening. Any disagreement over study selection was resolved by discussion among the three authors in face-to-face discussions (LG, YJZ, AT).
Inclusion/exclusion criteria
Studies that met all the following criteria were included in the review: (1) cross-sectional or longitudinal studies in which the study population underwent bariatric surgery, (2) measured any domain of impulsivity, and (3) assessment of the impact of impulsivity on postsurgical weight loss/weight regain.
Studies that met any of the follow criteria were excluded from the study: (1) abstract, review articles, clinical practice guidelines, (2) any languages other than English.
Assessment of study quality
The authors analyzed ten articles that met the above criteria. Table 1 details the assessment of quality of the studies using the Newcastle–Ottawa Scale [24]. Each study is judged on eight items, categorized into three groups: the selection of the study groups, the comparability of the cohorts, and the ascertainment of either the exposure or outcome of interest. Each item on the scale is scored from one point, except for comparability which can be scored up to two points. The maximum points for each study is nine, and studies with less than five points were identified as having a high risk of bias [25].
Results
Study selection
Figure 1 shows the study selection flowchart. Using the above keywords, a total of 229 articles were obtained and reviewed, comprising of 108 articles from PubMed, 121 articles from Embase, and 0 from Cochrane database of Systematic Reviews. The title and abstract of 97 unique articles were screened after duplicate articles were removed. 53 articles were excluded after title and abstract screening, and full texts of the 44 remaining articles were reviewed against the study selection criteria. Reasons for exclusion included the following: (1) patient population did not include post-bariatric surgery patients, (2) impulsivity was not assessed (3) article in non-English language, and 4) theoretical, meta-analysis, review article or opinion paper.

PRISMA diagram
Overview of studies
A total of ten studies with a total of 1246 patients were analyzed. The ten articles are summarized in Table 2, and the results of the ten studies are further summarized in Tables 3 and 4. Funnel plots were not performed in view of the small number of studies. Four studies [17, 20, 26, 27] were case–control studies, four studies [16, 19, 28, 29] were prospective observational studies, and two studies [12, 18] were retrospective observational studies.
Of the four case–control studies, Hogenkamp et al. [17] compared < 50% excess weight loss (EWL) versus > 50% EWL post-Roux-en-Y gastric bypass (RYGB) surgery, O. Ryden et al. [26] compared < 50%EWL and > 50% EWL post-vertical-banded gastroplasty, while Testa et al. [27] compared < 50% EWL versus > 50% EWL in patients who have undergone laparoscopic sleeve gastrectomy. Legenbauer et al. [20] compared obese individuals not receiving treatment versus those undergoing active management for their obesity (either in the form of bariatric surgery or conventional weight loss program).
Of the 1246 patients from ten studies, 747 underwent Roux-en-Y gastric bypass (RYGB), 212 underwent sleeve gastrectomy (SG), 126 underwent gastric banding (LAGB), 28 underwent biliopancreatic diversion with duodenal switch, and 10 underwent laparoscopic gastric plication. The type of surgery was not indicated for the remaining 123 patients from the study by Legenbauer et al. [20]. Nine hundred forty-four (75.8%) of the patients were female. The mean preoperative BMI was 43.3. The postoperative follow-up ranged from 0.5 to 12 years.
Four studies [19, 20, 26, 28] looked at postoperative BMI, three studies [12, 16, 18] reported the weight loss/percentage of excess weight loss (%EWL), and two studies [17, 28] reported both postoperative BMI and weight loss. All the studies demonstrated an overall decrease in weight post-bariatric surgery at varying postoperative timeframes.
Impulsivity was measured at different time points in relation to the surgery. Five studies [16, 19, 20, 27, 28] performed psychometric assessment pre-surgery, four studies [12, 17, 18, 29] performed psychometric assessment post-surgery, while one study by O. Ryden et al. [26] performed psychometric assessment both before and after surgery. Two studies [18, 20] additionally utilized mediation models to investigate the impact of pathological eating behavior as a mediator between impulsivity and weight loss.
Measures of impulsivity: impulsive choice
Only one study by Kulendran et al. [19] assessed impulsive choice using the temporal discounting task. In this study, a monetary temporal discounting task was presented to patients. Patients could choose either an earlier but smaller monetary reward, or a delayed but larger monetary reward. Changes in pre- and post-temporal discounting task score pre- and post-bariatric surgery did not predict weight loss.
Measures of impulsivity: impulsive action
Assessment of impulsive action was performed by two studies. Kulendran et al. [19] measured the stop-signal reaction time in patients performing the go/no-go task, while Hogenkamp et al. [17] used Stroop Task and go/no-go task, with the go/no-go association task testing response to food versus non-food words. Individuals who were slower to respond to the stop signal were classified as ‘impulsive.’ Kulendran et al. [19] found that postoperative reduction in impulsive action based on stop-signal reaction time predicts reduction in BMI. Patients who had the most change in stop-signal reaction time scores also had the most weight loss 6 months after bariatric surgery. Hogenkamp et al. [17] found that patients who responded well to surgery (defined as excess weight loss > 75% and BMI < 30 kg/m2) had significantly faster response times in the go/no-go task tests and performed better in the Stroop task performance. These results suggest that post-bariatric surgery weight loss is affected by impulsive action, and food cues may be a distracting factor in patients who have poor weight loss after bariatric surgery.
Measures of impulsivity: impulsive trait
Measures of impulsive trait used by studies include Barratt Impulsiveness scale, Minnesota Multiphasic Personality Inventory, UPPS-P impulsive behavior scale, and Karolinska Scales of Personality.
Barratt Impulsiveness Scale (BIS) [8] is the most commonly used assessment, reported in seven out of ten studies. Six studies [12, 17, 19, 20, 27, 28] used the BIS-11 30-item questionnaire, and all but Testa et al. [27] reported that higher BIS scores (impulsivity) are not associated with %EWL post-bariatric surgery. Testa et al. [27] reported three subscales of the BIS-11 score; attentional impulsiveness (tendency to fast shift in attention), motor impulsiveness (tendency to rush), and non-planning impulsiveness (tendency not to plan ahead), as well as the total BIS-11 score. While poor EWL % was associated with lower scores in the BIS-11 non-planning and attentional impulsiveness scales, logistic regression adjusting for sex/age/BMI/metabolic diseases shows that a higher score in the BIS-11 attentional scale was a significant predictor for good weight loss (> 50% %EWL) [27].
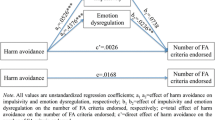
Schag et al. [18] used the short version BIS-15 (15 items) questionnaire, and reported that mediation analyses showed impulsivity had an indirect effect on %EWL through depression and pathological eating behavior, a finding that was mirrored by Legenbauer et al. [20] who noted that impulsivity had an indirect effect on weight loss, mediated by disinhibited eating.
Marek et al. [16] used the Minnesota Multiphasic Personality Inventory-2-Restructured Form (MMPI-2-RF), which assessed impulsivity under the behavioral/externalizing dysfunction (BXD) scale. Ryd et al. [26] assessed impulsivity as part of the Karolinska Scales of Personality (KSP) assessment, while Lavender et al. [29] assessed impulsivity using the UPPS-P impulsive behavior scale.
Higher BXD scores are associated with impulsivity, and such patients were likely to have less weight loss post-surgery. Impulsivity assessed as part of the KSP assessment and the UPPS-P impulsive behavior scale did not predict post-surgery weight loss.
Measures of other psychopathology
All the studies reported the incidences of formally diagnosed psychiatric conditions in their patient populations, and two studies [19, 20] excluded them from further analysis. Six studies [12, 17, 18, 20, 27, 28] analyzed eating disorders in addition to impulsivity. Six studies [12, 16, 18, 20, 26, 28] looked at other psychopathology as well, the most common being depression. Poor weight loss after bariatric surgery is associated with depression [12, 18, 28], anxiety [28], and pathological eating behavior [12, 18, 20].
Discussion
The most commonly used score to measure impulsivity was the Barratt Impulsiveness Scale (BIS) [8], which is a self-report questionnaire designed to assess both personality and behavioral aspects of impulsivity. It encompasses three main domains: attentional aspect of impulsivity, motor impulsivity, and non-planning impulsivity. There are several versions available, and the most commonly used version among the selected studies was the BIS-11. The BIS-11 has an internal consistency of 0.83 (Cronbach’s) for the total score and test–retest reliability at 1 month of 0.83 (Spearman’s Rho) [19]. Six studies [12, 17,18,19,20, 28] using the BIS score did not find any direct association between higher BIS scores and poorer weight loss outcomes after bariatric surgery. In comparison, the two studies [17, 19] that utilized behavioral measures of impulsivity (or state impulsivity) found a significant association between impulsive action and postsurgical weight loss. This could be attributed to the trait versus state dichotomy of impulsivity.
Psychopathology has described impulsivity as both a trait and a state. A trait is a stable characteristic that influences an individual’s thoughts, feelings, and behaviors, whereas a state is a temporary emotional condition. State impulsivity encompasses both impulsive choice and impulsive action. Previous studies have demonstrated low correlations between trait (personality) and state (behavioral) measures of impulsivity [30]. This has been postulated to be secondary to complex interactions with other external factors (e.g., independent subcortical systems, emotion regulatory mechanisms, environmental factors), which result in varying behaviors along the externalizing spectrum [31]. The low correlation between trait impulsivity (BIS scores) and postsurgical weight loss may be explained by other mitigating factors, either endogenous or exogenous. Kulendran et al. [19] hypothesize that the biological and psychological changes post-bariatric surgery may affect state impulsivity measures, such as response inhibition and reward processing [19]. Other studies have also suggested that neural activity in the brain cortices related to food reward may be altered by bariatric surgery, through various pathways such as altered dopamine receptor availability [32,33,34].
The dichotomy between the trait and state of impulsivity is further substantiated by the mediation analyses performed by Schag et al. [18] and Legenbauer et al. [20]. Although majority of the studies [16,17,18,19,20] concluded that impulsivity affects weight loss after bariatric surgery, the association between the two appears to be indirect. The studies by Schag et al. [18] and Legenbauer et al. [20] demonstrate that the indirect impact of impulsive trait on weight loss is mediated through other psychopathologies such as pathological eating behavior or depression. Our systematic review also demonstrates that when impulsivity is broken down into three broad domains: impulsive choice, impulsive action, and impulsive trait, it becomes clear that only impulsive action has a direct effect on weight loss after bariatric surgery.
The main limitation of this systematic review is the heterogeneity of the studies. Different measures of impulsivity used by various studies make it difficult to do a comprehensive analysis of the impact on impulsivity on post-bariatric surgery weight loss. The studies also measured impulsivity at different time intervals (half measured preoperatively [16, 19, 20], half postoperatively [12, 17, 18], and had varying lengths of follow-up post-surgery). The variation in surgery that the patients underwent may also affect the outcomes, as RYGB is associated with greater weight loss than SG [35]. Despite the majority of studies concluding that impulsivity affects weight loss, this was largely via an indirect association. The most commonly used score, BIS-11, did not show any significant statistical correlation with weight loss in majority of the studies. Instead, authors concluded that there was an indirect effect based on mediation analyses, or through other psychometric scoring systems. Interestingly, the majority of the patients in this review are female (75.8%), with the exception of the study by Kulendran et al. [19] where 31% of the study participants were female. Whether the results of this systematic review are applicable to males should be the subject of future studies.
Bariatric surgery is deemed the most effective method for sustained weight loss and improvement in metabolic conditions in the severely obese. Both the bariatric surgery patient population and healthcare professionals have a vested interest in ensuring successful weight loss after surgery. In light of the above findings, cognitive behavioral therapy strategies targeting cognitive control over food may help patients attain sustained weight loss post-bariatric surgery.
Currently, the most commonly used test is the BIS-11; however, BIS-11 is predominantly a measure of trait impulsivity and does not appear to show significant association with bariatric surgery weight loss. Future studies analyzing the impact of impulsivity on postsurgical weight loss should focus on using alternative psychometric scores that measure state impulsivity or impulsive action instead. Further longitudinal studies are needed to investigate the impact of bariatric surgery weight loss on the food-related neural and hormonal pathways in our bodies.
Conclusion
Impulsive trait may adversely affect postoperative outcomes after bariatric surgery indirectly, while impulsive action is associated with significantly poorer weight loss post-surgery. We would recommend applying alternative psychometric scores that measure state impulsivity or impulsive action instead of the BIS-11 score. Based on current available evidence, impulsivity is not a contraindication to bariatric surgery. However, patients deemed to be impulsive might benefit from closer psychological follow-up and weight monitoring post-surgery, as well as cognitive behavioral therapies targeting cognitive control over food. Further studies into this area and a validated score to measure state impulsivity are warranted.
What is already known on this subject?
Impulsivity has been shown to be associated with obesity through links to pathological eating behavior, and the recent literature suggests that impulsivity is linked to poorer outcomes post-bariatric surgery. An impulsive person, who is obese and overeats, is more likely to continue this same behavior after bariatric surgery, leading to weight regain and failure of intervention. However, efforts to draw a direct relationship between impulsivity and weight regain after bariatric surgery are often hampered by the complex nature of both impulsivity and obesity.
What you study adds?
We now know that impulsivity needs to be assessed as either a trait or state (impulsive action or impulsive choice). Contrary to what was previously believed, impulsive trait does not affect post-bariatric surgery outcomes. Impulsive action is associated with significantly poorer weight loss post-surgery. Based on the results of our study, impulsivity is not a contraindication to bariatric surgery; however, patients deemed to be impulsive might benefit from closer follow-up post-surgery, as well as cognitive behavioral therapies targeting cognitive control over food.
References
Evenden JL (1999) Varieties of impulsivity. Psychopharmacology 146(4):348–361. https://doi.org/10.1007/pI00005481
Kulendran M et al (2014) Neuropsychological assessment as a predictor of weight loss in obese adolescents. Int J Obes (Lond) 38(4):507–512. https://doi.org/10.1038/ijo.2013.198
Fields SA, Sabet M, Reynolds B (2013) Dimensions of impulsive behavior in obese, overweight, and healthy-weight adolescents. Appetite 70:60–66. https://doi.org/10.1016/j.appet.2013.06.089
Banos RM et al (2014) Relationship between eating styles and temperament in an Anorexia Nervosa, healthy control, and morbid obesity female sample. Appetite 76:76–83. https://doi.org/10.1016/j.appet.2014.01.012
MacKillop J et al (2016) The latent structure of impulsivity: impulsive choice, impulsive action, and impulsive personality traits. Psychopharmacology 233(18):3361–3370. https://doi.org/10.1007/s00213-016-4372-0
Green L, Myerson J (2004) A discounting framework for choice with delayed and probabilistic rewards. Psychol Bull 130(5):769–792. https://doi.org/10.1037/0033-2909.130.5.769
Weafer J, Baggott MJ, de Wit H (2013) Test-retest reliability of behavioral measures of impulsive choice, impulsive action, and inattention. Exp Clin Psychopharmacol 21(6):475–481. https://doi.org/10.1037/a0033659
Patton JH, Stanford MS, Barratt ES (1995) Factor structure of the Barratt impulsiveness scale. J Clin Psychol 51(6):768–774. https://doi.org/10.1002/1097-4679(199511)51:6%3c768:aid-jclp2270510607%3e3.0.co;2-1
Yeo D (2018) Outcomes after metabolic surgery in asians—a meta-analysis. Obesity Surgery. https://doi.org/10.1007/s11695-018-3484-5
Magro DO et al (2008) Long-term weight regain after gastric bypass: a 5-year prospective study. Obes Surg 18(6):648–651. https://doi.org/10.1007/s11695-007-9265-1
Odom J et al (2010) Behavioral predictors of weight regain after bariatric surgery. Obes Surg 20(3):349–356. https://doi.org/10.1007/s11695-009-9895-6
Brandao I et al (2015) Metabolic profile and psychological variables after bariatric surgery: association with weight outcomes. Eat Weight Disord 20(4):513–518. https://doi.org/10.1007/s40519-015-0199-7
Mitchell JE et al (2012) Psychopathology before surgery in the longitudinal assessment of bariatric surgery-3 (LABS-3) psychosocial study. Surg Obes Relat Dis 8(5):533–541. https://doi.org/10.1016/j.soard.2012.07.001
Jones-Corneille LR et al (2012) Axis I psychopathology in bariatric surgery candidates with and without binge eating disorder: results of structured clinical interviews. Obes Surg 22(3):389–397. https://doi.org/10.1007/s11695-010-0322-9
Spitznagel MB et al (2014) The role of cognitive function in postoperative weight loss outcomes: 36-month follow-up. Obes Surg 24(7):1078–1084. https://doi.org/10.1007/s11695-014-1205-2
Marek RJ et al (2015) Using presurgical psychological testing to predict 1-year appointment adherence and weight loss in bariatric surgery patients: predictive validity and methodological considerations. Surg Obes Relat Dis 11(5):1171–1181. https://doi.org/10.1016/j.soard.2015.03.020
Hogenkamp PS et al (2015) Patients lacking sustainable long-term weight loss after gastric bypass surgery show signs of decreased inhibitory control of prepotent responses. PLoS ONE 10(3):e0119896. https://doi.org/10.1371/journal.pone.0119896
Schag K et al (2016) The impact of impulsivity on weight loss four years after bariatric surgery. Nutrients. https://doi.org/10.3390/nu8110721
Kulendran M et al (2017) Impulsivity predicts weight loss after obesity surgery. Surg Obes Relat Dis 13(6):1033–1040. https://doi.org/10.1016/j.soard.2016.12.031
Legenbauer T et al (2018) The impact of self-reported impulsivity on the course of weight is mediated by disinhibited eating. Eur Eat Disord Rev 26(1):38–45. https://doi.org/10.1002/erv.2563
Elkins IJ et al (2006) Personality traits and the development of nicotine, alcohol, and illicit drug disorders: prospective links from adolescence to young adulthood. J Abnorm Psychol 115(1):26–39. https://doi.org/10.1037/0021-843X.115.1.26
Green L (1999) Discounting of delayed rewards across the life span: age differences in individual discounting functions. Bhav Process 46:86–96. https://doi.org/10.1016/s0376-6357(99)00021-2
Moher D et al (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ 339:b2535. https://doi.org/10.1136/bmj.b2535
Stang A (2010) Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol 25(9):603–605. https://doi.org/10.1007/s10654-010-9491-z
Luchini C (2017) Assessing the quality of studies in meta-analyses: advantages and limitations of the Newcastle Ottawa Scale. World Journal of Meta-Analysis 5(4):80–84. https://doi.org/10.13105/wjma.v5.i4.80
Ryden O, Hedenbro J, Frederiksen S (1996) Weight loss after vertical banded gastroplasty can be predicted: a prospective psychological study. Obes Surg 6(3):237–243. https://doi.org/10.1381/096089296765556827
Testa G et al (2019) Psychological predictors of poor weight loss following LSG: relevance of general psychopathology and impulsivity. Eat Weight Disord. https://doi.org/10.1007/s40519-019-00800-x
Aguera Z et al (2015) Psychological and personality predictors of weight loss and comorbid metabolic changes after bariatric surgery. Eur Eat Disord Rev 23(6):509–516. https://doi.org/10.1002/erv.2404
Lavender JM et al (2020) Examining emotion-, personality-, and reward-related dispositional tendencies in relation to eating pathology and weight change over seven years in the Longitudinal Assessment of Bariatric Surgery (LABS) study. J Psychiatr Res 120:124–130. https://doi.org/10.1016/j.jpsychires.2019.10.014
Wingrove J, Bond AJ (1997) Bond, impulsivity: A state as well as trait variable. Does mood awareness explain low correlations between trait and behavioural measures of impulsivity? Personality and Individual Differences 22(3):333–339. https://doi.org/10.1016/S0191-8869(96)00222-X
Beauchaine TP, Zisner AR, Sauder CL (2017) Trait impulsivity and the externalizing spectrum. Annu Rev Clin Psychol 13:343–368. https://doi.org/10.1146/annurev-clinpsy-021815-093253
Bruce JM et al (2012) Changes in brain activation to food pictures after adjustable gastric banding. Surg Obes Relat Dis 8(5):602–608. https://doi.org/10.1016/j.soard.2011.07.006
Olivo G et al (2017) Resting-state brain connectivity changes in obese women after Roux-en-Y gastric bypass surgery: a longitudinal study. Sci Rep 7(1):6616. https://doi.org/10.1038/s41598-017-06663-5
Frank S et al (2014) Altered brain activity in severely obese women may recover after Roux-en Y gastric bypass surgery. Int J Obes (Lond) 38(3):341–348. https://doi.org/10.1038/ijo.2013.60
Yeo D et al (2018) Outcomes after metabolic surgery in asians-a meta-analysis. Obes Surg. https://doi.org/10.1007/s11695-018-3484-5
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors have no conflicts of interest to declare.
Ethical approval
Not applicable.
Informed consent
The study does not involved participants.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The article is part of the Topical Collection on Personality and Eating and Weight Disorders.
Rights and permissions
About this article

Cite this article
Yeo, D., Toh, A., Yeo, C. et al. The impact of impulsivity on weight loss after bariatric surgery: a systematic review. Eat Weight Disord 26, 425–438 (2021). https://doi.org/10.1007/s40519-020-00890-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40519-020-00890-y