
Abstract
Purpose
Given the range of negative correlates associated with orthorexia nervosa (ON), it is important to identify factors that might contribute to the elevated ON tendencies. Based on the tripartite model of influence, we tested whether sociocultural attitudes towards appearance (i.e., thin and muscular internalization as well as family, peer and media pressure) could contribute to ON. We hypothesized that these attitudes could exert their effect through the intervening processes basic psychological need fulfillment and health anxiety.
Methods
The hypotheses were tested on a sample of 710 young adults (Mage = 21.79, SDage = 2.31). Participants completed validated questionnaires measuring the constructs of interest.
Results
According to the structural equation modeling results, ON was predicted by thinness and muscular internalization as well as media pressure. Need fulfillment and health anxiety partially mediated these relationships. Family and peer pressure were not related to ON.
Discussion
The present results suggest that internalization of appearance ideas and media pressure contribute to ON through need fulfillment and health anxiety. These findings also provide novel insight into the nature of ON.
Level of evidence
Level V (descriptive cross-sectional study.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Despite currently not being present in the various diagnostic manuals, orthorexia nervosa (ON) is an emerging and discussed topic in the public media and in the scientific literature as well [1, 2]. ON has been described as a condition characterized by excessive preoccupation and fixation with healthy food and proper nutrition without any specific focus on managing body weight [3]. People with ON usually have self-defined dietary restrictions that they strictly follow and they only consume food that is considered to be healthy. While it is still questionable to interpret the excessive preoccupation with healthy food itself as a pathology or problematic behavior (whose context and magnitude might also be important), ON-related studies have shown that it could have pathological implications such as being related to other eating disturbances or obsessive–compulsive signs [4]. As with other behaviors, ON tends to first manifest as a normal and harmonious health concern that might slowly turn into an obsessive one [5].
So far, studies have mostly focused on identifying prevalence rates which ranged from 6% to more than 80% [6] with some providing more conservative estimates [7]. The accuracy of these results might be questionable due to the fact that the items used in the ORTO-15 (one of the most popular measures of ON that was inspired by Bratman’s Orthorexia Self-Test) have not been officially validated and were not created with the aim of assessing prevalence. As a result of these psychometric issues and inaccuracies, the definition and diagnostic criteria of ON is still an ongoing discussion [8]. Still, some individual factors have been identified that might be related to ON. For instance, ON has been associated with perfectionism and negative body attitudes [9], vegetarian/vegan diet [10], educational level [11], harm avoidance, self-directedness and transcendence personality factors [12], obsessive-compulsive tendencies [13], motivations for healthy eating [14], psychological distress [15], and so on. At the same time, the recent review of McComb and Mills [16] highlighted that positive reinforcement for clean eating from others might be an important social determinant of ON. In the present study, positive reinforcement was interpreted in the form of sociocultural pressure towards appearance.
Social environment and eating behaviors
According to the well-established tripartite influence model of body image disturbance [17], the social environment consists of agents (e.g., family, peers, and media) who aim to influence and control the perception of appearance ideals. Indeed, these social agents are thought to show favor towards particular appearance ideals and body images (e.g., thin for women, muscular for men) and pressure the individual to attain a certain desired body type. As a result, people often need to rely on specific weight control and dietary methods to reach these ideals. Perceived sociocultural pressure towards appearance and ideal internalization (i.e., the cognitive endorsement of appearance ideals) has already been linked with eating disturbances [18]. As awareness of healthy eating and lifestyle increased in recent years and has become a major message for health organizations [19, 20], it appears to be relevant to investigate how the sociocultural pressure towards a healthy diet/healthy lifestyle might be related to ON. On the other hand, sociocultural pressure towards appearance might also be a relevant predictor of ON tendencies. As per its definition, being healthy is considered to be one of the main motivations of ON; still, studies showed that body image dissatisfaction [9] and weight control might [14] also have a relevant role.
While the role of the media has always been substantial in forming people’s perceptions, particularly with respect to their health and body image [21, 22], studies showed that the more proximal social agents of family and peers also have an influence on one’s body image and subsequent eating behavior [23, 24]. It is reasonable to hypothesize that the sociocultural pressures towards appearance and the internalization of appearance ideals might orient one towards focusing more on the specific ingredients of food as well as on adhering to a stricter diet to achieve these ideals (i.e., the characteristics of ON). Overall, the tripartite model appears to be well suited for the present investigation in exploring the role of the social environment on ON. Some direct evidence has been provided about the positive association between media pressure towards losing weight and ON tendencies [25] as well as social media use (i.e., Instagram) and ON [26]. Moreover, higher internalization of sociocultural attitudes towards appearance was also associated with ON [27]. To deepen our understanding of how sociocultural attitudes towards appearance might be related to ON, we tested the role of psychological need fulfillment and health anxiety as explanatory mechanisms.
Potential mediating processes: basic psychological need fulfillment and health anxiety
To better understand the associations between sociocultural attitudes towards appearance and healthy eating, the present study relied on the global and specific explanatory mechanisms of basic psychological need fulfillment and health anxiety, respectively, that might account for the association between sociocultural attitudes and ON. The theory of need fulfillment is one of the fundamental tenets of the well-articulated self-determination theory (SDT; [28]) and maintains that there exist three basic psychological needs (autonomy: being the origin of personal control and choice; competence: feeling effective in life; relatedness: having reciprocal relationships with others) whose fulfillment is conductive of psychological health, growth, and optimal functioning. Need fulfillment so far has been associated with a diverse range of positive outcomes [e.g., 29, 30] across different life domains [31, 32], making it ideal in understanding one’s experiences.
Although not directly examined in relation to ON, indirect evidence underscores the importance of need fulfillment in relation to binge eating and other eating-related disorders. Specifically, cross-sectional studies showed that unfulfilled needs are related to binge eating as well as unhealthy weight control behaviors [33,34,35]. Moreover, decreases in need fulfillment were related to increases in binge eating symptoms among adolescents over a 6-month period [36] as well as on a daily basis [37]. The available literature discussed above suggests that people might have increased tendencies of ON in a need unfulfilled state. From this perspective, ON might be interpreted as a potential compensatory mechanism for the need deficit state. One’s need fulfillment is greatly impacted by the social environment [38, 39], and experiencing social pressure towards appearance as well as a high expectation about one’s appearance could undermine the fulfillment of all three needs, thus contributing to ON tendencies.
Apart from need fulfillment, health anxiety could be a specific, eating-related mediating mechanism. Worrying about one’s health might be adaptive to a certain degree [40], but an overly cautious attitude might bias the interpretation of normal body signals [41]. It is reasonable to assume that sociocultural attitudes towards appearance might encourage people to pay more attention to their bodies to achieve the desired ideal, which, in turn, could increase people’s ON tendencies. As far as the authors know, only one study examined and reported positive associations between ON and health anxiety [14], and indirect results are also scarce [42], suggesting that there might be a relevant gap in the literature in general.
Research questions and hypotheses
The primary purpose of this study was to examine the associations between sociocultural attitudes towards appearance and ON and whether need fulfillment and health anxiety could represent explanatory mechanisms in this relation in a sample of young adults. Based on above-mentioned scientific literature, we expected sociocultural attitudes towards appearance (both internalization and pressure) to be directly related to ON. We also expected both need fulfillment and health anxiety to mediate this relationship by being negatively and positively related to sociocultural attitudes, respectively. Finally, ON was expected to be negatively related to need fulfillment, but positively to health anxiety.
Our decision to focus on young adults was rooted in two reasons. First, eating disorders are thought to start developing in early adulthood [43] and are thought to be the most prevalent in this age group [44]. This life period might also be critical as young adults gradually become more and more independent of their parents and start making their own decision with respect to their eating behaviors. Second, several studies [45, 46] reported negative associations between age an ON and showed that ON was more prevalent among younger adults.
Methods
Procedure and participants
This cross-sectional quantitative study was conducted in accordance with the Declaration of Helsinki and with the explicit approval of the University Research Ethics Committee of the Eötvös Loránd University (Hungary). Young adults were recruited from the corresponding university and through different online forums, groups, and websites specialized in healthy lifestyle and eating (e.g., vegetarian, vegan, fitness groups) with the data gathering occurring between September 2018 and February 2019 using an online questionnaire system. They did not receive any compensation for participation. First, they were informed about the aims of the study and were ensured about their anonymity. If they were willing to participate, they had to check a box to provide explicit consent; otherwise, they were excluded. Participants filled out self-reported questionnaires assessing ON, sociocultural attitudes, health anxiety, and need fulfillment as well as demographic data.
A total of 765 respondents were recruited; since this study focused on young adults, we filtered out those participants (n = 55) who did not correspond to this category (i.e., not being aged between 18 and 30). As a result, 710 individuals remained in the sample (80.7% female; M = 21.79, SD= 2.31). They reportedly lived in the capital city (52.7%), non-capital cities (34.8%), or country towns (12.5%). The average BMI of the participants was 22.13 (SD = 4.01), with 13.4% of the participants being underweight, 70.3% having normal weight, 12% being overweight, and 3.2% being obese. The majority (89.3%) did not have any illnesses at the time of the data gathering, 9.3% were diagnosed with an illness (e.g., diabetes, hypertension, hyperlipidemia, colitis ulcerosa, peptic ulcer, Chron’s disease, etc.), while the rest did not have knowledge of such diagnoses. In addition, 34.4% of the participants followed a diet in the preceding year, and 23.5% followed a diet at the time of the data gathering.
Materials
Orthorexia nervosa
The tendency to ON and people’s attitudes towards healthy eating was measured with the 11-item (e.g., “When eating, do you pay attention to the calories of the food?”; α = 0.82) Ortho-11-Hu [47] which is the Hungarian version of the ORTO-15 [48]. Respondents were able to answer on a four-point scale (1 = always, 4 = never). For ease of interpretation, items were reverse-scored, such that higher values on these ORTO-11-Hu items represent higher levels of ON symptomatology. Previous validation studies [e.g., 47] supported the factorial validity and internal consistency of the Hungarian version.
Sociocultural attitudes towards appearance
The 22-item Sociocultural Attitudes Towards Appearance Questionnaire-4 (SATAQ-4; [18]) was administered to assess sociocultural attitudes along five factors: thin (5 items, e.g., “I want my body to look very lean”; α = 0.88) and muscular (5 items, e.g., “I think a lot about looking muscular”; α = 0.89) internalization as well as family (4 items, e.g., “I feel pressure from family members to improve my appearance”; α = 0.84), media (4 items, e.g., “I feel pressure from the media to improve my appearance”; α = 0.92) and peer pressures (4 items, e.g., “I feel pressure from my peers to look in better shape”; α = 0.85). Responses were provided on a five-point scale (1 = definitely disagree, 5 = definitely agree). Previous studies [e.g., 18] using U.S. and international samples supported the factor structure, reliability, and convergent validity of the scale.
Basic psychological need fulfillment
The Hungarian version [49, 50] of the 24-item Basic Psychological Need Satisfaction and Frustration Scale [51] was administered to measure need fulfillment. The instrument contains six factors with four items per factor representing need satisfaction and need frustration × autonomy (e.g., “I feel a sense of choice and freedom in the things I undertake” or “I feel forced to do many things I wouldn’t choose to do”), competence (e.g., “I feel capable at what I do” or “I feel like a failure because of the mistakes I make”), and relatedness (e.g., “I feel that the people I care about also care about me” or “I feel the relationships I have are just superficial”; α = 0.93 for the total score). Items were rated on a five-point scale (1 = Not true at all for me; 5 = Very true for me). Tóth-Király et al. [49, 50] reported that the scale had adequate factorial validity, generalizability over gender groups, scale score reliability, and criterion validity.
Health anxiety
Participants’ concerns with their health and their body vigilance were measured with the Hungarian version [52] of the Short Health Anxiety Inventory [53]. Four statements are provided for each item from which participants can select one that best reflects their experiences. The instrument includes two subscales: a 14-item health anxiety (e.g., “I spend most of my time worrying about my health”; α = 0.87) and a 4-item negative consequences (e.g., “A serious illness would ruin every aspect of my life”; α = 0.77) subscale; the present study only focused on the health anxiety subscale. Responses are rated on a four-point scale (1 = no symptoms, 4 = very severe symptoms). The Hungarian validation [52] found that the scale had satisfactory factor structure and internal consistency as well as adequate convergent validity.
Statistical analyses
All analyses were performed with Mplus 8 [54] and the robust maximum-likelihood estimator. Prior to the main analyses, we conducted separate factor analyses for the individual instruments to ascertain their psychometric properties. Given the complexity of the hypothesized model, we opted to save these preliminary measurement models as factor scores and use those as input for the main analyses. Factor scores have the advantage, compared to manifest scale scores, of providing partial control for measurement error by allocating more weight to the items with lower error variances [55]. The use of factor scores is becoming increasingly popular [56, 57], further supporting our decision. The main analyses involved the construction of the hypothesized path model [58] in which sociocultural attitudes towards appearance predicted need fulfillment and health anxiety, which, in turn, predicted ON; sociocultural attitudes towards appearance also predicted ON directly. Model evaluation was based on several goodness-of-fit indices along their excellent or adequate cut-off values [59]: the Comparative Fit Index (CFI ≥ 0.95 excellent ≥ 0.90 adequate), the Tucker–Lewis index (TLI ≥ 0.95 excellent, ≥ 0.90 adequate), the root-mean-square error of approximation (RMSEA ≤ 0.06 excellent, ≤ 0.08 adequate) with its 90% CI, and the standardized root mean square residual (SRMR ≤ 0.05 for excellent, ≤ 0.10 for adequate).
Results
Preliminary analyses
To make this part concise and relevant to the overarching goal of the investigation, detailed results about the preliminary measurement models are reported in Appendix 1 of the online supplements. Overall, all measurement models had adequate fit (see the upper part of Table 1), and the factors were highly reliable in terms of Cronbach alpha and model-based omega composite reliability. With respect to need fulfillment, we were interested in the general factor that accounts for the highest amount of variance in participants’ ratings; therefore, only the general factor was included in the subsequent analyses.
Main analyses
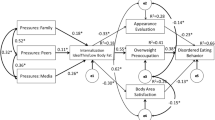
The fit of the model (see Fig. 1) was perfect according to the goodness-of-fit indices given that the model was fully saturated with zero degrees of freedom (i.e., all structural paths were estimated; see the bottom part of Table 1). Our results provided support for the proposed model: ON was predicted by need fulfillment, health anxiety, thinness, and muscular internalization as well as media pressure. Need fulfillment was only predicted by thinness and muscular internalization, while health anxiety was predicted by thinness internalization and media pressure. In the final model, the non-significant (p > 0.05) paths were trimmed, and only the significant ones were estimated (see Fig. 2). The final model also had adequate fit to the data, and the removal of the non-associated variables did not impact the regression coefficients substantially. The proportion of explained variance for ON was 47.4%. Mediation analyses are reported in Table 2 and show that both need fulfillment and health anxiety mediated the relationship between the predictors and the outcome as apparent by the 95% bias-corrected confidence interval not reaching zero for any of the indirect effects.

The fully saturated model of sociocultural attitudes, need fulfillment, health anxiety and orthorexia nervosa. Correlations are not shown for the sake of simplicity. Coefficients represent standardized regression weights.; Gray arrows represent non-significant paths. *p < 0.05; **p < 0.01

The final trimmed model of sociocultural attitudes, need fulfillment, health anxiety and orthorexia nervosa. Correlations are not shown for the sake of simplicity. Coefficients represent standardized regression weights. *p < 0.05; **p < 0.01
Discussion
The aim of the present study was to contribute to the scientific literature about ON by examining the role of sociocultural attitudes towards appearance (i.e., thin and muscular internalization as well as social pressure from the family, peers and media) as predictors of ON via two potential mediating processes, namely basic psychological need fulfillment and health anxiety. Both internalization factors predicted ON directly; in addition, thinness indirectly through both mediators, while muscular internalization only through need fulfillment. Out of the three pressure dimensions, contrary to our expectations, only media pressure was a significant predictor, while family and peer pressures were not. These findings lead to a number of important implications.
Sociocultural sources of ON tendencies
Our first key findings complement prior studies in the field of eating behaviors, which showed that sociocultural risk factors are related to eating-related pathologies and problematic eating behaviors. For instance, disturbed eating has been related to elevated scores on all five sociocultural factors [18]. Higher degrees of internalization of thinness and muscularity suggest that people adopted the ideals of either thinness (i.e., having a slim body with low body fat) or muscularity (i.e., having a well-developed athletic body) to a higher degree and that they wish to attain these ideals. One potential way to achieve such goals is to regulate one’s eating behaviors. By establishing a strict rule about what can or cannot be eaten (e.g., more vegetables or full grains instead of sugar), people might be able to achieve these appearance ideals more easily compared to those cases when they do not regulate their diet. Additionally, these appearance ideals might also be understood as reflections of an ideal yet unrealistic lifestyle [60], which should be achieved for happiness. Although the definition of ON mostly refers to the internalization of being healthy and healthy eating being a value, it is possible that the internalization of appearance ideas is also present, only to a smaller extent.
As for social pressures towards appearance, studies highlighted the importance of examining multiple sources of social appearance pressure as these sources might have different effects. Based on our findings, only pressure from the media was associated with ON tendencies. This aligns well with previous theoretical [22] and empirical [61] works showing that even brief exposure to manipulated media images could have an effect on one’s body (dis)satisfaction and, in turn, eating behavior. In most cases, the social pressures towards appearance are likely to be unrealistic, potentially leading to a higher degree of body dissatisfaction and, as a consequence, a more radical diet that could undermine one’s health. Again, similar to internalization, regulating eating behavior could be one of the tools that one has to reach a certain body type. While the zero-order correlations were statistically significant between ON and the other pressure sources (i.e., family and peers), these associations disappeared in the more complex model in which other factors were also taken into account. These results might be attributed to the fact that the participants were young adults who might not live with their families; thus, these pressures might have less influence on them. Still, future studies are needed to more thoroughly test the relative effect of these sources of social pressure.
The relation of ON with need fulfillment and health anxiety
A second key finding relates to the examination of need fulfillment and health anxiety as predictors of ON. Need fulfillment was negatively related to ON, indicating that the higher one’s basic psychological needs of autonomy, competence, and relatedness are satisfied, the lower the ON tendencies are likely to be. This finding is in line with prior studies focusing on need satisfaction and various eating behaviors [33]. Overall, it is probable that when one’s needs are satisfied, they might not feel the pressure to engage in problematic/exaggerated eating behaviors, which have been suggested as a potential compensatory mechanism against unfulfilled needs [36]. Similarly, high need fulfillment is associated with more autonomous regulation forms that are, in turn, conductive of fewer compensatory behaviors [62]. Conversely, having unfulfilled needs might orient people to overengage in eating-related behaviors to cope with their need deficit state [62]. However, this compensatory behavior is likely to be ephemeral.
Health anxiety was positively related to ON, suggesting that the more people worry about their health and bodily functions, the more they are likely to focus on establishing and following a strict diet as well as on doing more physical activity. The heightened self-awareness is positive only to a certain extent, and people with health anxiety might be more likely to misinterpret bodily information even if no pathology is present. Although no study investigated their temporal directions, it is possible that ON manifests as a coping mechanism for health anxious people.
An overarching model of the relations between on and sociocultural attitudes
As a third key finding, the hypothesized model provides novel insights into the nature of ON. Psychological need fulfillment partly accounted for the relationship between ON and internalization of thinness as well as ON and internalization of muscularity, though the directions of these associations were opposing: while need fulfillment was negatively predicted by the internalization of thinness, it was positively predicted by muscular internalization. Therefore, having internalized the ideals of thinness is likely to decrease people’s need fulfillment, possibly because they feel that they are not efficient in maintaining their lifestyle (i.e., need for competence) or because they feel pressured to look and behave in a certain way and live up to the societal expectations (i.e., need for autonomy). However, these expectations might not be self-endorsed, eliciting need unfulfillment and a subsequent compensatory behavior that might be ON. By the same token, the internalization of thinness and the societal expectations might also be so high that anxiety about one’s health and life could manifest not just due to the fear of not being able to match these expectations, but also because of seeing oneself and unattractive or unhealthy. As opposed to thinness internalization, muscle internalization appears to have a positive association with need fulfillment. Being firm, athletic, and muscular could increase one’s basic psychological needs, and doing physical activities on a regular basis might lead to feelings of success (i.e., need for competence) or free activity selection (i.e., need for autonomy).
Overall, the findings of the present study contribute to the existing knowledge in three ways. First, similar to other problematic eating behaviors, the present study reinforced the important role appearance ideals, and body attitudes might have in relation to ON. While body image disturbance is not part of the definition of ON, future studies should examine the importance of the attitude towards one’s body in the differential diagnosis. It is possible that various subgroups could be identified based on a combination of motivations among which body weight control and body image dissatisfaction might play a role. Second, our results suggest that lower levels of basic psychological need fulfillment, as a potential risk factor, might increase the risk of ON tendencies. Third, the heightened self-perception that is health anxiety might also be considered as a risk factor for ON as eating is one of the health-related behaviors that is the easiest to control for the individual (relative to, for instance, exercising) which might lead to an increased sense of control.
Limitations and future directions
Despite the strengths of the present study (i.e., solid theoretical basis, relatively large sample size, sophisticated analyses), it had limitations as well, which should be addressed. A cross-sectional design was used, which does not allow for causal inferences. Future studies should, in the next step, use longitudinal designs to test the temporal ordering of the variables or experimental designs to establish causality. Daily diary studies might also be useful in examining the above-tested model in a more nuanced way. This study used self-reported questionnaires which could potentially be biased (e.g., social desirability or self-selection bias). More objective indicators of health and lifestyle could shed more light on the manifestation of ON (e.g., actual food intake, body-fat percentage, measured fitness level). The instrument to measure ON was derived from the ORTO-15, which is known to have psychometric issues; thus, conclusions should be drawn with caution. While the sample was relatively large, it was not representative; thus, generalizations to other groups should be made tentatively. Further replications are needed in different cultural and socioeconomic countries. Although the included correlates had theoretical foundations, other potential moderators and mediators might also have an important role, such as perfectionism, self-esteem, body dissatisfaction, or pressure towards healthy eating. The need to include other variables in future studies is also underscored by the fact that the indirect effects were small. Although the criteria for and the field of ON are still evolving [63], the present study might enhance our understanding of the nature of ON.
In conclusion, the current study suggests that various sociocultural attitudes towards appearance are differentially related to ON. Thinness and muscular internalization as well as media pressure predicted ON, while family and peer pressure did not. In addition, these associations were mediated by health anxiety and basic psychological need fulfillment. These results highlight the importance that the social environment and the appearance ideals might play in the development and maintenance of ON as well as two of its potential risk factors.
What is already known on this subject?
So far, most empirical studies on orthorexia nervosa focused on how it is predicted by individual factors (e.g., perfectionism or motivations for healthy eating). However, less research focused on the potential social determinants of orthorexia nervosa, namely sociocultural attitudes towards appearance and the possible mediating processes (e.g., basic psychological need fulfillment and health anxiety) between sociocultural attitudes and orthorexia nervosa.
What this study adds?
Thinness internalization, muscular internalization, and media pressure appear to predict orthorexia nervosa. Additionally, need fulfillment and health anxiety might be two potential mediators that could explain how sociocultural attitudes might relate to orthorexia nervosa. These findings suggest that more attention should be paid to these factors by researchers and practitioners alike to better understand and address the development and maintenance of orthorexia nervosa.
References
Cuzzolaro M, Donini LM (2016) Orthorexia nervosa by proxy? Eat Weight Disord 21(4):549–551. https://doi.org/10.1007/s40519-016-0310-8
Reynolds R, McMahon S (2019) Views of health professionals on the clinical recognition of orthorexia nervosa: a pilot study. Eat Weight Disord. https://doi.org/10.1007/s40519-019-00701-z
Bratman S (1997) Healthy Food Junkie: obsession with dietary perfection can sometimes do more harm than good, says one who has been there. Yoga J 136:42–46
Brytek-Matera A, Fonte ML, Poggiogalle E, Donini LM, Cena H (2017) Orthorexia nervosa: relationship with obsessive-compulsive symptoms, disordered eating patterns and body uneasiness among Italian university students. Eat Weight Disord 22:609–617. https://doi.org/10.1007/s40519-017-0427-4
Koven NS, Abry AW (2015) The clinical basis of orthorexia nervosa: emerging perspectives. Neuropsychiatr Dis Treat 11:385–394. https://doi.org/10.2147/NDT.S61665
Dunn TM, Bratman S (2016) On orthorexia nervosa: a review of the literature and proposed diagnostic criteria. Eat Behav 21:11–17. https://doi.org/10.1016/j.eatbeh.2015.12.006
Dunn TM, Gibbs J, Whitney N, Starosta A (2017) Prevalence of orthorexia nervosa is less than 1%: data from a US sample. Eat Weight Disord 22(1):185–192. https://doi.org/10.1007/s40519-016-0258-8
Cena H, Barthels F, Cuzzolaro M, Bratman S, Brytek-Matera A, Dunn T, Donini LM (2019) Definition and diagnostic criteria for orthorexia nervosa: a narrative review of the literature. Eat Weight Disord 24(2):209–246. https://doi.org/10.1007/s40519-018-0606-y
Barnes MA, Caltabiano ML (2017) The interrelationship between orthorexia nervosa, perfectionism, body image and attachment style. Eat Weight Disord 22(1):177–184. https://doi.org/10.1007/s40519-016-0280-x
Dell’Osso L, Carpita B, Muti D, Cremone IM, Massimetti G, Diadema E, Carmassi C (2018) Prevalence and characteristics of orthorexia nervosa in a sample of university students in Italy. Eat Weight Disord 23(1):55–65. https://doi.org/10.1007/s40519-017-0460-3
Donini LM, Marsili D, Graziani MP, Imbriale M, Cannella C (2004) Orthorexia nervosa: a preliminary study with a proposal for diagnosis and an attempt to measure the dimension of the phenomenon. Eat Weight Disord 9(2):151–157. https://doi.org/10.1007/BF03325060
Kiss-Leizer M, Rigó A (2019) People behind unhealthy obsession to healthy food: the personality profile of tendency to orthorexia nervosa. Eat Weight Disord 24(1):29–35. https://doi.org/10.1007/s40519-018-0527-9
Poyraz CA, Tüfekçioğlu EY, Özdemir A, Baş A, Kani AS, Erginöz E, Duran A (2015) Relationship between orthorexia and obsessive-compulsive symptoms in patients with generalised anxiety disorder, panic disorder and obsessive compulsive disorder. Yeni Symp 53(4):22–26. https://doi.org/10.5455/NYS.20160324065040
Kiss-Leizer M, Tóth-Király I, Rigó A (2019) How the obsession to eat healthy food meets with the willingness to do sports: the motivational background of orthorexia nervosa. Eat Weight Disord 24(3):465–472. https://doi.org/10.1007/s40519-019-00642-7
Luck-Sikorski C, Jung F, Schlosser K, Riedel-Heller SG (2019) Is orthorexic behavior common in the general public? A large representative study in Germany. Eat Weight Disord 24(2):267–273. https://doi.org/10.1007/s40519-018-0502-5
McComb SE, Mills JS (2019) Orthorexia nervosa: a review of psychosocial risk factors. Appetite 140:50–75. https://doi.org/10.1016/j.appet.2019.05.005
Thompson JK, Heinberg LJ, Altabe M, Tantleff-Dunn S (1999) Exacting beauty: theory, assessment, and treatment of body image disturbance. American Psychological Association, Washington
Schaefer LM, Burke NL, Thompson JK, Dedrick RF, Heinberg LJ, Calogero RM, Anderson DA (2015) Development and validation of the Sociocultural Attitudes Towards Appearance Questionnaire-4 (SATAQ-4). Psychol Assess 27(1):54–67. https://doi.org/10.1037/a0037917
Gorski MT, Roberto CA (2015) Public health policies to encourage healthy eating habits: recent perspectives. J Healthc Leadersh 7:81–90. https://doi.org/10.2147/JHL.S69188
World Health Organization (2002) Global strategy on diet physical activity and health. World Health Organization, Geneva
Becker AE, Burwell RA, Herzog DB, Hamburg P, Gilman SE (2002) Eating behaviours and attitudes following prolonged exposure to television among ethnic Fijian adolescent girls. Br J Psychiatry 180(6):509–514. https://doi.org/10.1192/bjp.180.6.509
Derenne JL, Beresin EV (2006) Body image, media, and eating disorders. Acad Psychiatry 30(3):257–261. https://doi.org/10.1176/appi.ap.30.3.257
Bearman SK, Presnell K, Martinez E, Stice E (2006) The skinny on body dissatisfaction: a longitudinal study of adolescent girls and boys. J Youth Adolescence 35:217–229. https://doi.org/10.1007/s10964-005-9010-9
Menzel JE, Schaefer LM, Burke NB, Mayhew LL, Brannick MT, Thompson JK (2010) Appearance-related teasing, body dissatisfaction, and disordered eating: a meta-analysis. Body Image 7:261–270. https://doi.org/10.1016/j.bodyim.2010.05.004
Haddad C, Obeid S, Akel M, Honein K, Akiki M, Azar J, Hallit S (2019) Correlates of orthorexia nervosa among a representative sample of the Lebanese population. Eat Weight Disord 24(3):481–493. https://doi.org/10.1007/s40519-018-0631-x
Turner PG, Lefevre CE (2017) Instagram use is linked to increased symptoms of orthorexia nervosa. Eat Weight Disord 22(2):277–284. https://doi.org/10.1007/s40519-017-0364-2
Eriksson L, Baigi A, Marklund B, Lindgren EC (2008) Social physique anxiety and sociocultural attitudes toward appearance impact on orthorexia test in fitness participants. Scand J Med Sci Spor 18(3):389–394. https://doi.org/10.1111/j.1600-0838.2007.00723.x
Ryan RM, Deci EL (2017) Self-determination theory. Basic psychological needs in motivation, development, and wellness. Guildford Press, New York
Gillet N, Morin AJS, Huyghebaert T, Burger L, Maillot A, Poulin A, Tricard E (2019) University students’ need satisfaction trajectories: a growth mixture analysis. Learn Instr 60:275–285. https://doi.org/10.1016/j.learninstruc.2017.11.003
Krijgsman C, Vansteenkiste M, van Tartwijk J, Maes J, Borghouts L, Cardon G, Haerens L (2017) Performance grading and motivational functioning and fear in physical education: a self-determination theory perspective. Learn Individ Differ 55:202–211. https://doi.org/10.1016/j.lindif.2017.03.017
Cox A, Williams L (2008) The roles of perceived teacher support, motivational climate, and psychological need satisfaction in students’ physical education motivation. J Sport Exerc Psychiatry 30:222–239. https://doi.org/10.1123/jsep.30.2.222
Deci EL, Ryan RM, Gagné M, Leone DR, Usunov J, Kornazheva BP (2001) Need satisfaction, motivation, and well-being in the work organizations of a former eastern bloc country: a cross-cultural study of self-determination. Pers Soc Psychol B 27:930–942. https://doi.org/10.1177/0146167201278002
Froreich FV, Vartanian LR, Zawadzki MJ, Grisham JR, Touyz SW (2017) Psychological need satisfaction, control, and disordered eating. Brit J Clin Psychol 56(1):53–68. https://doi.org/10.1111/bjc.12120
Schüler J, Kuster M (2011) Binge eating as a consequence of unfulfilled basic needs: the moderating role of implicit achievement motivation. Motiv Emotion 35:89–97. https://doi.org/10.1007/s11031-010-9200-y
Thøgersen-Ntoumani C, Ntoumanis N, Nikitaras N (2010) Unhealthy weight control behaviours in adolescent girls: a process model based on self-determination theory. Psychol Health 25:535–550. https://doi.org/10.1080/08870440902783628
Boone L, Vansteenkiste M, Soenens B, der Kaap-Deeder V, Verstuyf J (2014) Self-critical perfectionism and binge eating symptoms: a longitudinal test of the intervening role of psychological need frustration. J Couns Psychol 61(3):363–373. https://doi.org/10.1037/a0036418
Verstuyf J, Vansteenkiste M, Soenens B, Boone L, Mouratidis A (2013) Daily ups and downs in women’s binge eating symptoms: the role of basic psychological needs, general self-control, and emotional eating. J Soc Clin Psychol 32(3):335–361. https://doi.org/10.1521/jscp.2013.32.3.335
Tóth-Király I, Bőthe B, Orosz G, Rigó A (2018) On the importance of balanced need fulfillment: a person-centered perspective. J Happiness Stud. https://doi.org/10.1007/s10902-018-0066-0
Yu S, Chen B, Levesque-Bristol C, Vansteenkiste M (2018) Chinese education examined via the lens of self-determination. Educ Psychol Rev 30(1):177–214. https://doi.org/10.1007/s10648-016-9395-x
Asmundson GJG, Abramowitz JS, Richter AA, Whedon M (2010) Health anxiety: current perspectives and future directions. Curr Psychiatry Rep 12(4):306–312. https://doi.org/10.1007/s11920-010-0123-9
Abramowitz JS, Olatunji BO, Deacon BJ (2007) Health anxiety, hypochondriasis, and the anxiety disorders. Behav Ther 38(1):86–94. https://doi.org/10.1016/j.beth.2006.05.001
Hadjistavropoulos H, Lawrence B (2007) Does anxiety about health influence eating patterns and shape-related body checking among females? Pers Indiv Differ 43(2):319–328. https://doi.org/10.1016/j.paid.2006.11.021
Nagl M, Jacobi C, Paul M, Beesdo-Baum K, Höfler M, Lieb R (2016) Prevalence, incidence, and natural course of anorexia and bulimia nervosa among adolescents and young adults. Eur Child Adoles Psychiatry 25:903–918. https://doi.org/10.1007/s00787-015-0808-z
Hoek HW, van Hoeken D (2003) Review of the prevalence and incidence of eating disorders. Int J Eat Disorder 34(4):383–396. https://doi.org/10.1002/eat.10222
Dell’Osso L, Abelli M, Carpita B, Massimett G, Pini S, Rivett L, Carmassi C (2016) Orthorexia nervosa in a sample of Italian university population. Riv Psichiatr 51:190–196. https://doi.org/10.1708/2476.25888
Rudolph S (2018) The connection between exercise addiction and orthorexia nervosa in German fitness sports. Eat Weight Disord 23(5):581–586. https://doi.org/10.1007/s40519-017-0437-2
Varga M, Thege BK, Dukay-Szabó S, Túry F, van Furth EF (2014) When eating healthy is not healthy: orthorexia nervosa and its measurement with the ORTO-15 in Hungary. BMC Psychiatry 14(59):1–11. https://doi.org/10.1186/1471-244X-14-59
Donini LM, Marsili D, Graziani MP et al (2005) Orthorexia nervosa: validation of a diagnosis questionnaire. Eat Weight Disord 10:28–32. https://doi.org/10.1007/BF03327537
Tóth-Király I, Bőthe B, Orosz G, Rigó A (2019) A new look on the representation and criterion validity of need fulfillment: application of the Bifactor exploratory structural equation modeling framework. J Happiness Stud 20(5):1609–1626. https://doi.org/10.1007/s10902-018-0015-y
Tóth-Király I, Morin AJS, Bőthe B, Orosz G, Rigó A (2018) Investigating the multidimensionality of need fulfillment: a bifactor exploratory structural equation modeling representation. Struct Equ Model 25(2):267–286. https://doi.org/10.1080/10705511.2017.1374867
Chen B, Vansteenkiste M, Beyers W, Boone L, Deci EL, Van der Kaap-Deeder J, Ryan RM (2015) Basic psychological need satisfaction, need frustration, and need strength across four cultures. Motiv Emotion 39(2):216–236. https://doi.org/10.1007/s11031-014-9450-1
Köteles F, Simor P, Bárdos G (2011) A Rövidített Egészségszorongás- Kérdőív (SHAI) magyar verziójának kérdőíves validálása és pszichometriai értékelése [Validation and psychometric evaluation of the Hungarian version of the Short Health Anxiety Inventory (SHAI)]. Mentálhigiéné és Pszichoszomatika 12(3):191–213. https://doi.org/10.1556/Mental.12.2011.3.1
Salkovskis PM, Rimes KA, Warwick HMC, Clark DM (2002) The Health Anxiety Inventory: development and validation of scales for the measurement of health anxiety and hypochondriasis. Psychol Med 32(5):843–853. https://doi.org/10.1017/S0033291702005822
Muthén LK, Muthén BO (1998) Mplus user’s guide, vol 8. Muthén and Muthén, Los Angeles
Skrondal A, Laake P (2001) Regression among factor scores. Psychometrika 66(4):563–575. https://doi.org/10.1007/BF02296196
Gillet N, Morin AJS, Cougot B, Gagné M (2017) Workaholism profiles: associations with determinants, correlates, and outcomes. J Occup Organ Psych 90(4):559–586. https://doi.org/10.1111/joop.12185
Tóth-Király I, Vallerand RJ, Bőthe B, Rigó A, Orosz G (2019) Examining sexual motivation profiles and their correlates using latent profile analysis. Pers Individ Differ 146:76–86. https://doi.org/10.1016/j.paid.2019.04.002
Tóth-Király I, Bőthe B, Márki AN, Rigó A, Orosz G (2019) Two sides of the same coin: The differentiating role of need satisfaction and frustration in passion for screen-based activities. Eur J Soc Psychol. https://doi.org/10.1002/ejsp.2588
Marsh HW, Hau K-T, Grayson D (2005) Goodness of fit evaluation in structural equation modeling. In: Maydeu-Olivares A, McArdle J (eds) Contemporary psychometrics: a festschrift for Roderick P. McDonald, Erlbaum, pp 275–340
Featherstone M (1991) The body in consumer culture. In: Featherstone M, Hepworth M, Turner SB (eds) The body: social process and cultural theory. Sage Publications, London, pp 170–196
Mask L, Blanchard CM (2011) The protective role of general self-determination against ‘thin ideal’ media exposure on women’s body image and eating-related concerns. J Health Psychol 16(3):489–499. https://doi.org/10.1177/1359105310385367
Vansteenkiste M, Ryan RM (2013) On psychological growth and vulnerability: basic psychological need satisfaction and need frustration as a unifying principle. J Psychother Integr 23(3):263–280. https://doi.org/10.1037/a0032359
Varga M, Dukay-Szabó S, Túry F, van Furth Eric F (2013) Evidence and gaps in the literature on orthorexia nervosa. Eat Weight Disord 18(2):103–111. https://doi.org/10.1007/s40519-013-0026-y
Funding
The first author was supported by a Horizon Postdoctoral Fellowship from Concordia University in the preparation of the manuscript. The project was also supported by a research grant from the Faculty of Education and Psychology of Eötvös Loránd University.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Institutional Review Board of the Eötvös Loránd University and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The article is part of the topical collection on orthorexia nervosa.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Tóth-Király, I., Gajdos, P., Román, N. et al. The associations between orthorexia nervosa and the sociocultural attitudes: the mediating role of basic psychological needs and health anxiety. Eat Weight Disord 26, 125–134 (2021). https://doi.org/10.1007/s40519-019-00826-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40519-019-00826-1