
Abstract
Background and purpose
Recent research demonstrates a significant relationship between weight status and impaired reaction time in young, adult, and elderly individuals. However, most such studies were performed on small samples, used only body mass index as the body obesity index, used simple reaction time, and oftentimes did not consider some potential confounders such as age, socioeconomic status, or physical activity in their studies. The present study explored the relationship between various reaction time tasks and various obesity indices in a sample of youth.
Methods
Two hundred and thirty-four young males (19–24 years) underwent standard anthropometry, various information processing tasks (e.g., clinical reaction time, simple audio and visual reaction time, and choice reaction time), as well as an inhibitory control task (congruent and incongruent Simon reaction time).
Results
Results revealed no significant relationship between any of the information processing tests and body mass index, nor for fat percentage, waist circumference, and waist-to-height ratio after adjustment for potential confounders. A weak positive association was observed only between congruent Simon reaction time (but not incongruent Simon reaction time) and waist circumference in participants (t value = 0.199; Std error = 0.0014; p = 0.047; Cohen’s f2 = 0.09).
Conclusion
Inhibitory control, but not information processing speed, was associated only with waist circumference in apparently healthy young men.
Level of evidence
Level I, experimental study.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The increasing prevalence of obesity is a significant public health concern, especially as recent research demonstrates a significant relationship between obesity and cognitive impairment [1]. However, there is little, and what is considered controversial evidence, for the association between weight status and some cognitive tasks, especially in young people.
Information processing speed, which is assessed using time tests such as reaction time (RT), is one of the oldest diagnostic methods used in modern psychology, and the first examinations of this parameter date back to the nineteenth century [2]. RT is the time interval between the application of a stimulus and the appearance of appropriate voluntary response by a subject, and which challenges relatively simple cognitive operations [3]. It has been shown that RT is associated with health and general cognitive ability [4] and can be used as a sensitive cognitive test in both healthy individuals and patients [3,4,5,6,7,8]. While there is evidence which suggests an obesity–impaired cognition relationship [9,10,11,12,13,14,15], the relationship between weight status and information processing speed remains ambiguous [16,17,18].
Skurvydas et al. [10] observed that young males from a group with greater body mass index (BMI) (≥ 25) reacted significantly slower in simple RT than their peers with normal BMI. Nene et al. [13] compared audio and visual RT among a sample of young females with lower BMI (< 18.5), normal BMI, and greater BMI (≥ 25), and observed that subjects with lower BMI (but not subjects with greater BMI) performed worse at visual RT than their normal weight peers. Deore et al. [11] found that both underweight and overweight young females were inferior while performing simple visual RT in comparison to their normal weight peers. Esmaeilzadeh [16] found no association between simple clinical RT (RTclin) and various obesity indices (either central or overall) in a sample of 7–11-year-old boys. In another study, Moradi and Esmaeilzadeh [17] observed a significant association only between fat percentage and visual RT in a sample of 9–11-year-old boys. They concluded that information processing speed impairment due to greater adiposity, which has been reported in the literature, may not be observed for some types of obesity indices or RT tasks during childhood.
Regarding the recently reported relationship between weight status and information processing speed tests some points should be stated. First, most of the previous studies investigating the relationship between weight status and information processing speed included a small sample of participants [9,10,11, 13,14,15] and used only overall obesity indices such as BMI [9,10,11, 13,14,15]. BMI can be influenced by several factors and indices, such as central obesity, which is more closely linked to some adverse health outcomes than BMI [19], and subcutaneous fat skinfold has been suggested as a more reliable general obesity index than BMI [20]. Therefore, obesity indices may relate differentially to changes in cognitive function over time. In addition, some previous studies did not consider potential confounders such as age, socioeconomic status, and physical activity (PA) lifestyle patterns [9,10,11, 13,14,15,16, 21], while socioeconomic status is strongly associated with cognitive ability and achievement during childhood and beyond [22, 23]. Furthermore, it has been shown that athletes are better able to respond quickly to a presented stimulus [24] while physically active individuals are capable of allocating more attentional resources toward the environment [25, 26]. A person’s information processing speed and quality can be evaluated using one (e.g., simple RT) or more (e.g., choice RT) stimuli, with more stimuli causing greater stress on decision making and leading to prolonged RT [27]. However, most of the studies underlying the association between information processing tasks and weight status have used only simple RT [10, 11, 13, 16,17,18, 21] and reported controversial results especially in young people [16,17,18, 21]. However, it should be noted that information processing tasks with more stimuli such as choice RT have rarely been used [15], and it may be possible that the results for cognitive tasks by greater stimuli are different in relation to weight status in young people [12, 15]. Therefore, it would be interesting to explore not only simple RT but also choice RT in relation to weight status in young people.
Inhibitory control is the ability to prevent planned or ongoing, although inappropriate actions, in a given situation and plays an important role in choosing proper behaviours in daily life [7, 8]. Like information processing speed, inhibitory control task has different levels of difficulty. Inhibitory control task is the difference in RT between the trials in which response and stimuli are relevant (congruent), and trials in which response and stimuli are irrelevant (incongruent). In general, responses are slower and less accurate when the response and stimuli are irrelevant [7, 8]. A few studies have reported the negative effect of adiposity on inhibitory control in young people [12, 28, 29], but a few measured both central and overall obesity indices [29] or included possible covariates such as socioeconomic status and PA [12].
Therefore, based on the mentioned literature above, there is needed for further research regarding the association between weight status for not only simple cognitive tasks (i.e., simple RT), but also tasks with greater stimuli (i.e., choice RT, congruent RT, and incongruent RT) among young people.
Following this context, the purpose of the present study was to examine whether there are associations between various cognitive tasks (simple or complex) and obesity indices (central or overall), while controlling for potential confounders such as age, socioeconomic status, and PA among a sample of apparently healthy youth.
Methods
Participants and procedure
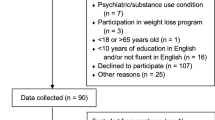
This cross-sectional study was conducted with students, 19–24-year-old, studying at the University of Mohaghegh Ardabili in the centre of Ardabil Province, North West Iran, during 2015 and 2016. Due to sociocultural problems, only male volunteers were considered. The procedure of the study was explained to the students (n = 481) and they were invited to participate in the study. 154 students were not included in the study due to exclusion criteria such as: not being 19–24-year-old, daily smoking, alcohol abuse, heavy caffeine use, medication intake, drug abuse, reported medical illness, history of endocrine disorder, or cardiovascular disease. Therefore, 327 eligible students who signed the written consent participated in the study. As 93 students did not complete all the measurements, or left the study, the statistical analyses were done using only complete data (n = 234). On the days of the experiments, participants were instructed to avoid caffeine drinks [30] and PA [27]. After anthropometric (e.g., height, weight, waist and hip circumference, and fat percentage) and sociodemographic data collection (e.g., age and socioeconomic status), participants were familiarized with the procedure of the RT tests. RT Tasks were performed in a quiet room. Experimental sessions were conducted between 14:30 and 18:00, and consisted of 5 RT tasks performed in the same order for all participants as follows: clinical RT (RTclin), simple visual RT, simple audio RT, 4-choice reaction time, and Simon task. To prevent fatigue, after each task participants rested for 5 min [31]. Response accuracy was recorded for each trial and error trials were excluded from the analysis.
The study design was approved by the Human Ethics Committee of the University of Mohaghegh Ardabili, and the experiment was performed in accordance with the ethical standards of the committee and the Helsinki Declaration.
Anthropometric variables
Subjects’ weight was measured in underwear and without shoes on an electronic scale (Type SECA 861) to the nearest 0.1 kg, and height was measured barefoot in the Frankfurt horizontal plane using a telescopic height measuring instrument (Type SECA 225) to the nearest 1 mm. Four obesity indices were measured:
-
indices indicating overall obesity: BMI and fat percentage
-
indices indicating central obesity: waist circumference and waist to height.
BMI was calculated as body weight in kilograms divided by the square of height in meters.
A Lange skinfold caliper was used to assess body fat percentage. Fat percentage was determined from the average of three measures of the thickness of three sites on the right side of the body (chest, abdomen, and thigh) and calculated according to the Jackson–Pollock method [32].
Waist circumference was measured at a point immediately above the iliac crest on the midaxillary line, at minimal respiration to the nearest 0.1 cm [33]. Waist circumference was divided by height to determine the waist-to-height ratio (WHtR).
Possible confounders
Physical activity (PA) was measured using the 12-month recall Baecke PA questionnaire [34] as a valid and reliable PA inventory [35]. The questionnaire consisted of 16 questions organized in three sections: PA at work, PA during leisure excluding sport (PADLES) and sport during leisure time (SDLT). Since almost all students were not working, the work section was excluded. Questions in each section were scored on the 5-point Likert scale (always, often, sometimes, seldom, and never).
Socioeconomic status was computed from parents’ education and occupational status [36, 37]. Monthly household income was separated into the following income categories, counted in Iranian Rial (note 1 USD equals approximately 37,000 Iranian Rial): 1 ≤ 4,000,000 Rial; 2 = 4,000,000–8,000,000 Rial; 3 = 8,000,000–12,000,000 Rial; 4 = 12,000,000–16,000,000 Rial; 5 = 16,000,000–20,000,000 Rial; 6 = 20,000,000–25,000,000 Rial; 7 = 25,000,000–30,000,000 Rial; 8 = 30,000,000–40,000,000 Rial; 9 = 40,000,000–50,000,000 Rial; 10 ≥ 50,000,000 Rial.
The highest educational level attained by either parent was collapsed into the following categories: 0 = no education; 1 = elementary; 2 = secondary 3 = incomplete high school 4 = completed high school; 5 = bachelor’s degree 6 = Master of Science/Arts; 7 = PhD, Doctoral, etc.
Reaction time (RT)
Simple visual RT and 4-choice RT
Participants performed the Deary–Liewald computer-based RT which included simple visual RT and 4-choice RT tasks [4]. The simple visual RT task involved 8 practice trials and 20 test trials. The participants were requested to respond (press space bar) to a single stimulus as quickly as possible (response range from 150 to 1500 ms; inter-stimulus interval from 1000 to 3000 ms). The 4-choice RT task involved 8 practice trials followed by 40 test trials. For the 4-choice RT, the participant was requested to press the key that corresponded to the correct response to four different stimuli (response range from 200 to 1500 ms; inter-stimulus interval from 1000 to 3000 ms). Response accuracy for the 4-choice RT task was 0.93.
Simple audio RT
Each subject completed 8 practice trials and 20 data acquisition trials using RT software installed on a laptop [17]. When performing simple audio RT (response range from 150 to 1500 ms; inter-stimulus interval from 1000 to 3000 ms), the participants were requested to press a default key (space bar) as soon as possible, using the index finger, which was in contact with the key, every time the subject heard a “beep” sound. Headphones were provided for clarity of sound.
Clinical reaction time (RTclin)
In addition to the above-computerized simple visual RT and simple audio RT tests we took a new clinical measure of RT (RTclin) which has been recently developed and validated [38]. Each subject participated in simple RTclin testing using an RTclin apparatus [16, 17]. The apparatus for measuring RTclin is a measuring stick, coated in high-friction tape and marked by 5 mm increments, 0.8 m long, which is embedded in a weighted rubber disk. The distance that the apparatus fell before being caught by the subject was recorded in meters (m). The formula for a body falling under the influence of gravity \((t=0.45 \times \surd d)\) for each trial was used to calculate RTclin in seconds (s), where “d” is for distance (meters) and “t” is for time (seconds). Each participant executed four practice trials followed by ten trials for data acquisition. For each participant, mean (SD) baseline RTclin values were calculated.
Simon task
A small, white square was posited in the center of the display which remained throughout the trials (n = 100) as a gaze-fixation point [39]. The subjects were requested to respond as accurately and quickly as possible to the color of an oval (delivered either to the right or to the left of the white gaze-fixation square) by pressing the appropriate response key. The task included two equiprobable trial types as follows: congruent trials in which the spatial location of the stimulus corresponded to the task-relevant aspect of the stimulus (for example: right stimulus/right response) and the incongruent trials in which the spatial location of the stimulus corresponded to the opposite spatial location of the response (for example: right stimulus/left response). The program [39] had been designed to save only true responses; therefore, response accuracy for the Simon task was 1.0.
Statistical analysis
Before further analysis, all data were checked for outliers using graphical models such as boxplot, and normality was cheeked using the Kolmogorov–Smirnov test and graphical models such as histograms and Q–Q plots. The initial Pearson product–moment correlations were conducted on RT tasks, demographic variables (age and socioeconomic status), and PA (SDLT and PADLES). Any variable which exhibited a significant correlation with the dependent variable (cognitive tasks) was included as a covariate in the regression analyses. For exploring the association between the obesity indices and the RT tasks, four regression models were conducted as follows: (1) ordinary multiple linear regression analyses with non-transformed data; (2) ordinary multiple linear regression with transformed data (according to the results of Table 1) using the natural logarithm (transformation by exponential value); (3) a generalized gamma regression with a link to a non-normal distribution; (4) robust regression with non-transformed data. All calculations were performed using R-3.5.1 program or SPSS v.21.0 software for Windows. Package “robust” and “rsq” were installed in the R program for conducting robust regression analysis and r-squared for gamma regression, respectively. The significance level was set at p ≤ 0.05.
Results
General characteristics of the participants are shown in Table 1. According to the results of Kolmogorov–Smirnov test (Table 1), simple visual RT, simple audio RT, 4-choice RT, congruent RT, incongruent RT, SDLT, and also socioeconomic status were transformed using natural logarithm for using in the parametric statistics (i.e., Pearson moment correlation and multiple linear regression analysis).
Pearson product moment correlation (Table 2) indicated a significant relationship between simple visual RT and SDLT, while 4-choice RT was significantly correlated with socioeconomic status, and congruent RT was significantly correlated with SDLT. Incongruent RT was significantly associated with age, socioeconomic status, and SDLT.
Multiple linear regression analysis by including non-transformed data and after adjustment for possible confounders showed no significant relationship between any of the obesity indices and RT tasks except for a positive association between waist circumference and congruent RT (standardized β = 0.196; p = 0.025; Table 3).
Multiple linear regression analysis by including transformed data and after adjustment for possible confounders revealed no significant relationship between any of the obesity indices and RT tasks except for a positive association between waist circumference and congruent RT (standardized β = 0.193; p = 0.03; Table 4).
Generalized gamma regression analysis after adjustment for possible confounders indicated no significant relationship between any of the obesity indices and RT tasks except for a positive association between waist circumference and congruent RT (t value = 0.199; Std error = 0.0014; p = 0.047; Table 5). For interpreting the observed significant association between waist circumference and congruent RT, Cohen’s f2 [40] was used (i.e., 0.02 = small, 0.15 = medium, 0.35 = large). For this mean, we calculated r square for the association between waist circumference and congruent RT using “rsq” package in the R program and then calculated effect size using the following formula: r2/(1 − r2). Since the calculated effect size value for the association between waist circumference and congruent RT was 0.09, so there is a weak association between waist circumference and congruent RT and this means that small part of variance is explained by these data.
Robust regression analysis after adjustment for possible confounders revealed no significant relationship between any of the obesity indices and RT tasks (Table 6).
For further exploring the association between waist circumference and congruent RT, we explored the distribution of both waist circumference and congruent RT. For this mean, we used two-sample Kolmogorov–Smirnov test to observe the distribution of both waist circumference and congruent RT in comparison to the simulated gamma distribution generated by R program (Fig. 1). The two-sample Kolmogorov–Smirnov test showed gamma distribution for both waist circumference (p = .62) and congruent RT (p = .23) in comparison to the simulated gamma distribution. Therefore, the results of this test affirm that the results of generalized gamma regression observed for the association between waist circumference and congruent RT are acceptable in comparison to the results of robust regression.

Distribution of WC and Simon congruent RT in comparison with the simulated gamma distributions. Distribution of waist circumference and Simon congruent RT in comparison to simulated gamma distributions using the two-sample Kolmogorov–Smirnov test to explore whether the distributions are gamma or not. WC waist circumference, Congruent RT Simon congruent reaction time
Discussion
The present study aimed to explore the relationship between various reaction time tasks and various obesity indices in a sample of youth. The results revealed no association between various information processing tests (i.e., simple and choice RT) and obesity indices among young male participants. However, we observed a weak positive association between waist circumference and congruent RT (but not incongruent RT) in young men.
It has been proven that different fat compartments carry differential metabolic risks [41], and there is growing evidence that visceral fat and abdominal obesity are more correlated with individuals’ physical and mental health outcomes than global body mass [29, 33, 42, 43]. However, limited data exist regarding these concepts in association with cognitive function, especially in healthy young individuals [29, 42].
Although it has been reported that obesity is negatively related to cognitive function [44], this relationship may not be significant for all tasks and obesity indices [12, 16,17,18, 45, 46] and even a reverse relationship may be observed between adiposity and some simple tasks in healthy people [21, 46]. In 2014, Grantham and Henneberg [21] reported that it is not necessarily appropriate to consider body adiposity as a negative factor influencing neuromuscular RT performance, as body lipid reserves are integral to the development of the nervous system (e.g., the development of myelin nerve sheath) and thus improved RT, even amongst individuals within healthy weight ranges. Gunstad et al. [45] observed no association between elevated BMI and various cognitive functioning tasks in a relatively large number of 6–19-year-old healthy participants and suggested further similar studies to clarify the inconsistent results between adults and younger individuals. However, in another study they observed a significant negative effect of obesity on cognitive function (e.g., inhibitory control) among a sample of adults [28]. Kamijo et al. [12], in a study exploring the association between an inhibitory control task and adiposity, observed that children with greater BMI and fat mass showed worse performance on the incongruent RT. However, they observed no association between congruent RT and adiposity.
According to our knowledge, there are a few studies which explore the association between cognitive function and both central and overall obesity indices among young people and most studies have used overall obesity indices such as BMI and fat percentage [9,10,11,12,13,14,15, 21, 22, 28, 45]. Deng et al. [29] observed that, in comparison to BMI, waist circumference was more closely connected with inhibitory control and suggested waist circumference as a reliable indicator of brain function in young adults. Dore et al. [42] found that both waist circumference and WHtR were significantly associated with cognitive function; however, after adjustment for PA, they observed a significant association only for waist circumference, which is similar to our results. Like Dore et al. [42], we are not aware of the reason that only a significant association was found for waist circumference (but not WHtR) and inhibitory control.
Some biological mechanisms such as impaired insulin regulation, systemic inflammation, and elevated triglycerides by which obesity could impair cognitive function have been suggested by researchers [44] as possible reasons. Unfortunately, the mentioned mechanisms only have been examined in elderly people or in animals and the need for further research in young people has been reported [44]. Therefore, we are unaware of possible mechanisms of why only central obesity was significantly associated with inhibitory control in young men.
According to the published literature [10, 12, 16,17,18, 21, 45, 46] and the results of the present study, there is a need for further research to better understand the relationship between various cognitive functioning tasks requiring a smaller or greater amount of cognitive control and weight status in young individuals.
Although the present study has some strengths, including using linear models to assess the association between the variables and the study including a number of potential confounders that are consistent with the previous literature on the topic, such as socioeconomic status and PA, as well as a homogenous sample of participants; the study has several limitations, and these results should be interpreted with caution. For example, the cross-sectional nature of the study limits the possibility to draw conclusions about causality of any of the observed relationships in the participants. Furthermore, the present study did not include subjects of both sexes, did not include more obese or underweight subjects, did not include samples of various age ranges, and did not measure adiposity of the participants using direct methods (e.g., dual-energy X-ray absorptiometry, etc.). Finally, although we have invited 481 individuals to participate, only 234 met the inclusion criteria and completed all the measurements. This is below the targeted sample of 250 for stable estimates of correlation [47].
Conclusion
In summary, we observed no association between various obesity indices and information processing tasks or inhibitory control, except for a positive association between central obesity (waist circumference) and congruent RT in young men. It is, therefore, possible that cognitive impairment due to greater adiposity among young, healthy people may not be observed for some simple tasks [16,17,18]. However, according to the study results (i.e., the small effect size), it should be stated that the observed association between central obesity and congruent RT is weak and further studies are needed to establish the findings.
Abbreviations
- BMI:
-
Body mass index
- 4-choice RT:
-
4-Choice reaction time
- PA:
-
Physical activity
- SDLT:
-
Sport during leisure time
- PADLES:
-
Physical activity during leisure excluding sport
- RT:
-
Reaction time
- RTclin :
-
Clinical reaction time
- Simple visual RT:
-
Simple visual reaction time
- Simple audio RT:
-
Simple audio reaction time
- Congruent RT:
-
Simon congruent reaction time
- Incongruent RT:
-
Simon incongruent reaction time
- WHtR:
-
Waist-to-height ratio
References
Prickett C, Brennan L, Stolwyk R (2015) Examining the relationship between obesity and cognitive function: a systematic literature review. Obes Res Clin Pract 9(2):93–113. https://doi.org/10.1016/j.orcp.2014.05.001
Merkel J (1885) Die zeitlichen Verhältnisse der Willensthähigkeit. Philos Stud 2:73–127
Botwinik J, Thompson LW (1966) Premotor and motor components of reaction time. J Exp Psychol 71:9–15. https://doi.org/10.1037/h0022634
Deary IJ, Liewald D, Nissan J (2011) A free, easy-to-use, computerbased simple and four-choice reaction time programme: the Deary-Liewald reaction time task. Behav Res Methods 43:258–268. https://doi.org/10.3758/s13428-010-0024-1
Jakobsen LH, Sorensen JM, Rask IK, Jensen BS, Kondrup J (2011) Validation of reaction time as a measure of cognitive function and quality of life in healthy subjects and patients. Nutrition 27:561–570. https://doi.org/10.1016/j.nut.2010.08.003
Pachana NA, Thompson LW, Marcopulos BA, Yoash-Gantz R (2004) California older adult Stroop test (COAST): development of a Stroop test adapted for geriatric populations. Clin Gerontol 27:3–22. https://doi.org/10.1300/J018v27n03_02
Simon JR (1990) The effects of an irrelevant directional cue on human information processing. In: Proctor RW, Reeve TG (eds) Stimulus-response compatibility: an integrated perspective. North-Holland, Amsterdam, pp 31–86
Simon JR, Rudell AP (1967) Auditory SR compatibility: the effect of an irrelevant cue on information processing. J Appl Psychol 51:300–304. https://doi.org/10.1037/h0020586
Gunstad J, Paul RH, Cohaen RA, Tate DF, Gordon E (2006) Obesity is associated with memory deficits in young and middle aged adults. J Eat Weight Disord 11:15–19. https://doi.org/10.1007/BF03327747
Skurvydas A, Gutnik B, Zuoza AK et al (2009) Relationship between simple reaction time and body mass index. HOMO J Comp Hum Biol 60:77–85. https://doi.org/10.1016/j.jchb.2008.06.006
Deore DN, Surwase SP, Masroor S, Khan ST, Kathore V (2012) A cross sectional study on the relationship between the body mass index (BMI) and the audiovisual reaction time (ART). J Clin Diagn Res 6:1466–1468. https://doi.org/10.7860/JCDR/2012/4440.2534
Kamijo K, Khan NA, Pontifex MB et al (2012) The relation of adiposity to cognitive control and scholastic achievement in preadolescent children. Obesity (Silver Spring) 20:2406–2411. https://doi.org/10.1038/oby.2012.112
Nene AS, Pazare PA, Sharma KD (2011) A study of relation between body mass index and simple reaction time in healthy young females. Indian J Physiol Pharmacol 55:288–291
Nikam LH, Gadkari JV (2012) Effect of age, gender and body mass index on visual and auditory reaction times in Indian population. Indian J Physiol Pharmacol 56:94–99
Gentier I, Augustijn M, Deforche B et al (2013) A comparative study of performance in simple and choice reaction time tasks between obese and healthy-weight children. Res Dev Disabil 34:2635–2641. https://doi.org/10.1016/j.ridd.2013.04.016
Esmaeilzadeh S (2014) Reaction time: does it relate to weight status in children? HOMO J Comp Hum Biol 65:171–178. https://doi.org/10.1016/j.jchb.2013.09.007
Moradi A, Esmaeilzadeh S (2017) Simple reaction time and obesity in children: whether there is a relationship? Environ Health Prev Med 22:2. https://doi.org/10.1186/s12199-017-0612-0
Moradi A, Esmaeilzadeh S (2015) Association between reaction time, speed and agility in schoolboys. Sport Sci Health 11:251–256. https://doi.org/10.1007/s11332-015-0230-4
Lindqvist P, Andersson K, Sundh V et al (2006) Concurrent and separate effects of body mass index and waist-to-hip ratio on 24-year mortality in the population study of women in Gothenburg: evidence of age-dependency. Eur J Epidemiol 21:789–794. https://doi.org/10.1007/s10654-006-9074-1
Nooyens AC, Koppes LL, Visscher TL et al (2007) Adolescent skinfold thickness is a better predictor of high body fatness in adults than is body mass index: the Amsterdam Growth and Health Longitudinal Study. Am J Clin Nutr 85:1533–1539
Henneberg M, Brush G, Harrison GA (2001) Growth of specific muscle strength between 6 and 18 years in contrasting socioeconomic conditions. Am J Phys Anthropol 115:62–70. https://doi.org/10.1002/ajpa.1057
Noble KG, Norman MF, Farah MJ (2005) Neurocognitive correlates of socioeconomic status in kindergarten children. Dev Sci 8:74–87. https://doi.org/10.1111/j.1467-7687.2005.00394.x
Montés-Micó R, Bueno I, Candel J, Pons AM (2000) Eye-hand and eye-foot visual reaction times of young soccer players. Optometry 71:775–780
Gomez-Pinilla F, Hillman C (2013) The influence of exercise on cognitive abilities. Compr Physiol 3:403–428. https://doi.org/10.1002/cphy.c110063
Sibley BA, Etnier JL (2003) The relationship between physical activity and cognition in children: a meta-analysis. Pediatr Exerc Sci 15:243–256. https://doi.org/10.1515/ijsl.2000.143.183
Murray NP, Russoniello C (2012) Acute physical activity on cognitive function: a heart rate variability examination. Appl Psychophysiol Biofeedback 37:219–227. https://doi.org/10.1007/s10484-012-9196-z
Grantham J, Henneberg M (2014) Adiposity is associated with improved neuromuscular reaction time. Med Hypotheses 83:593–598. https://doi.org/10.1016/j.mehy.2014.08.012
Gunstad J, Robert H. Paul RH, Cohen RA, Tate DF, Spitznagel MB, Gordon E (2007) Elevated body mass index is associated with executive dysfunction in otherwise healthy adults. Compr Psychiatry 48:57–61. https://doi.org/10.1016/j.comppsych.2006.05.001
Deng Z, Huang Q, Huang J, Zhang W, Qi C, Xu X (2018) Association between central obesity and executive function as assessed by stroop task performance: a functional near-infrared spectroscopy study. J Innov Opt Health Sci 11:1750010. https://doi.org/10.1142/S1793545817500109
Durlach PJ, Edmunds R, Howard L, Tipper SP (2002) A rapid effect of caffeinated beverages on two choice reaction time tasks. Nutr Neurosci 5:433–442. https://doi.org/10.1080/1028415021000039211
Welford AT (1980) Choice reaction time: basic concepts. In: Welford AT (ed) Reaction times. Academic Press, New York, pp 73–128
Jackson AS, Pollock ML (1978) Generalized equations for prediction body density of men. Br J Nutr 40:497–504. https://doi.org/10.1079/BJN19780152
Esmaeilzadeh S, Farzizadeh R, Kalantari HA (2018) Central or overall obesity: which one is a better predictor of depressive symptoms in children, adolescents, and youths? Eat Weight Disord 23(1):117–123. https://doi.org/10.1007/s40519-016-0320-6
Baecke J, Burema J, Frijters J (1982) A short questionnaire for the measurement of habitual physical activity in epidemiological studies. Am J Clin Nutr 36:936–942
Pereira MA, Fitzergerald SJ, Gregg EW et al (1997) A collection of physical activity questionnaires for health-related research. Med Sci Sports Exerc 29:S1–S205
Esmaeilzadeh S (2015) The association between depressive symptoms and physical status including physical activity, aerobic and muscular fitness tests in children. Environ Health Prev Med 20:434–440. https://doi.org/10.1007/s12199-015-0484-0
Kalantari HA, Esmaeilzadeh S (2016) Association between academic achievement and physical status including physical activity, aerobic and muscular fitness tests in adolescent boys. Environ Health Prev Med 21:27–33. https://doi.org/10.1007/s12199-015-0495-x
Eckner JT, Whitacre RD, Kirsch N, Richardson JK (2006) Evaluating a clinical measure of reaction time. Arch Phys Med Rehabil 87:10. https://doi.org/10.2466/pms.108.3.717-720
Francis G, Neath I, VanHorn D (2007) CogLab on a CD, version 2.0. Thomson Wadsworth, Belmont
Cohen J (1988) Statistical power analysis for the behavioral sciences, 2nd edn. Lawrence Erlbaum Associates, Publishers, Hillsdale, NJ. ISBN 0-8058-0283-5
Fox CS, Massaro JM, Hoffmann U et al (2007) Abdominal visceral and subcutaneous adipose tissue compartments: association with metabolic risk factors in the Framingham Heart Study. Circulation 116:39–48. https://doi.org/10.1161/CIRCULATIONAHA.106.675355
Dore GA, Elias MF, Robbins MA, Budge MM, Elias PK (2008) Relation between central adiposity and cognitive function in the Maine–Syracuse Study: attenuation by physical activity. Ann Behav Med 35:341–350. https://doi.org/10.1007/s12160-008-9038-7
Franzosi MG (2006) Should we continue to use BMI as a cardiovascular risk factor? Lancet 368:624–625. https://doi.org/10.1016/S0140-6736(06)69222-2
Smith E, Hay P, Campbell L, Trollor JN (2011) A review of the association between obesity and cognitive function across the lifespan: implications for novel approaches to prevention and treatment. Obes Rev 12:740–755. https://doi.org/10.1111/j.1467-789X.2011.00920.x
Gunstad J, Lhotsky A, Wendell CR, Ferrucci L, Zonderman AB (2010) Longitudinal examination of obesity and cognitive function: results from the Baltimore longitudinal study of aging. Neuroepidemiology 34:222–229. https://doi.org/10.1159/000297742
Gunstad J, Spitznagel MB, Paul RH, Cohen RA, Kohn M, Luyster FS et al (2008) Body mass index and neuropsychological function in healthy children and adolescents. Appetite 50:246–251. https://doi.org/10.1016/j.appet.2007.07.008
Schönbrodt FD, Perugini M (2013) At what sample size do correlations stabilize? J Res Pers 47(5):609–612. https://doi.org/10.1016/j.jrp.2013.05.009
Funding
No funding was received for performing the present study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the Human Ethics Committee of University of Mohaghegh Ardabili and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Esmaeilzadeh, S., Farzizadeh, R., Kalantari, HA. et al. Is obesity associated with impaired reaction time in youth?. Eat Weight Disord 25, 415–425 (2020). https://doi.org/10.1007/s40519-018-0614-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40519-018-0614-y