
Abstract
Purpose
Medical students appear to be a high-risk group to develop psychological problems including eating disorders (ED). The prevalence estimates of ED risk vary greatly between studies. This systematic review and meta-analysis was done to estimate the prevalence of ED risk among medical students.
Methods
An electronic search of EMBASE, MEDLINE, ProQuest and Google Scholar was conducted. Studies that reported the prevalence of ED risk among medical students and were published in English peer-reviewed journals between 1982 and 2017 were included. Information about study characteristics and the prevalence of ED risk were extracted by four investigators. Each article was reviewed independently by at least two investigators. Estimates were pooled using random-effects meta-analysis using the DerSimonian–Laird method. The main outcome of interest was the prevalence of ED risk in medical students.
Results
The prevalence of ED risk among medical students was extracted from nineteen cross-sectional studies across nine countries (total participants n = 5722). The overall pooled prevalence rate of ED risk was 10.4% (497/5722 students, 95% CI 7.8–13.0%), with statistically significant evidence between-study heterogeneity (Q = 295, τ2 = 0.003, I2 = 94.0%, P < 0.001). Prevalence estimates between studies ranged from 2.2 to 29.1%.
Conclusion
In this systematic review and meta-analysis, the summary prevalence of ED risk among medical students was 10.4%. Further research is needed to identify and prevent ED in this population. Studies are also needed to investigate concurrent pathologies associated with ED risk.
Level of evidence
Level I, systematic review and meta-analysis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Eating disorders (ED) are disorders of eating behaviors, associated thoughts, attitudes and emotions, and their resulting impairments [1]. ED are becoming an area of concern due to their increasing prevalence in all age, ethnic and socioeconomic cohorts [2, 3]. ED are associated with several physiological impairments, comorbidities, and increased risk for mortality [4]. The mortality rate for persons with ED is the highest among all psychiatric illnesses [5], and is estimated to be twelve times higher than the rate from other causes for women of 15–24 years old [6].
Individuals with ED often do not seek medical help, or only seek help in the later stages after a long period of illness [7]. According to the National Eating Disorders Collaboration of Australia there is a mean delay of 4 years between the start of ED symptomology and first treatment, and this delay can be for 10 or more years [8]. Thus, there is a legitimate need to identify individuals at risk of ED to provide timely treatment.
There are numerous tools available to screen for ED risk; however, only limited ones have been used repeatedly in the literature. The top four screening instruments are: Eating Attitudes Test-26 (EAT-26) [9], Eating Disorder Inventory (EDI) [10], Eating Disorder Examination Questionnaire (EDE-Q) [11], and SCOFF Questionnaire [12].
Previous studies have suggested that medical students can be considered as a high-risk group for developing mental health problems including ED due to academic stress, extremely high workloads, the need for continuous learning, and exposure to illnesses and death during their medical education [13,14,15]. Being a young adult also increases the risk for developing ED due to the transitional nature of this phase of life in term of relationships, self-concept and goals for future [16]. The stigma associated with mental health disorders and ED may lead to denial, self-medication, delayed diagnosis and treatment resulting in more severe and persistent presentation of ED [17].
Estimates of the prevalence of ED risk among medical students vary across studies from 2 to 30% [18, 19]. Conflicting findings in the variation by sex, year of study and ethnicity are reported [19, 20]. Obtaining reliable estimates for ED risk during medical education are crucial to identify, treat and prevent such disorders in this specific population. Accordingly, the following global systematic review and meta-analysis was executed to (1) obtain a stable estimate of ED risk among medical students, and (2) to examine variability between studies and assess the generalizability of the results.
Methods
This systematic review and meta-analysis used the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [21] statement as a guideline for reporting.
Database searches
In November 2017, three reviewers HJ, MS and MF conducted an electronic search using EMBASE, MEDLINE, ProQuest and Google Scholar from 1982 to 2017. The search team developed a list of search strategies, including the following keywords: medical students, eating disorder(s), feeding disorder(s), eating problem(s), eating attitude(s), and eating behavior(s). No limitations were applied during the initial search. Furthermore, the review team manually screened the references of the identified papers for potential inclusion in the review.
Inclusion criteria
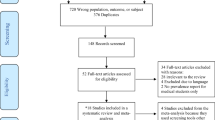
We included all observational studies that aimed to study the prevalence of ED risk among medical students. The studies should have satisfied the following criteria: (1) published in the English language; (2) date of publication was between January 1982 and November 2017; (3) assessed medical students as a target population and (4) reported the prevalence of disordered eating risk. ED risk was defined in this review as significant changes in eating patterns with associated psychological changes. Disordered eating risk in previous studies is often measured using the most common screening tools of EAT-26, SCOFF and EDI (Fig. 1).

Flow diagram of study inclusion
Exclusion criteria
Exclusion criteria were: (1) studies that included medical students with non-medical students in the same group, without providing a subgroup analysis; (2) studies in which the prevalence of ED was not the main focus of the research, e.g., studying “mental health problems” in general; (3) lack of availability of the study, and inability to obtain the full text after contacting the authors (Fig. 1).
Main outcomes and measures
The principal outcome of this review is to report the prevalence of ED risk among medical students using pre-established cut-off scores of continuous measures of eating pathology risk. These cut-off scores were established by the developers of measurement scales for example a score of ≥ 20 points on EAT26 or a score of ≥ 2 points on SCOFF indicate risk of ED. The secondary outcomes were comparisons of the variability between studies reporting the prevalence of ED risk according to the: sex of participants, country of the study, and used research tool.
The five review team members independently screened titles and abstracts and assessed studies for eligibility criteria. Authors AA, MS, AB performed initial data extraction, which was later confirmed by another review member HJ or MF. Any conflicts in study appropriateness for inclusion in the review were resolved through dialogue with the senior reviewer/expert clinician AA and panel consensus. To standardize data extraction, the review team agreed to collect the following variables: study characteristic, e.g., name, year, sample size, country, participants characteristics, e.g., age, sex, body mass index (BMI) (kg/m2) and the main findings of the prevalence of ED risk. Missing data from the included studies were requested from the original authors as necessary using email correspondence.
Data synthesis and statistical analyses
The data were pooled in this meta-analysis using random-effects model according to the DerSimonian–Laird method, reporting the pooled prevalence and the corresponding 95% confidence interval. Data were presented graphically using the Forest plot. When two or more studies reported the same dataset, the first publication was included in the meta-analysis. Three studies reported the prevalence of ED risk using two different screening tools [19, 22, 23]; EAT-26 and SCOFF (Table 2). For these three studies, the results of the prevalence estimates of EAT-26 entered the initial meta-analysis, whereby each study contributed with only one prevalence rate. The decision to include EAT-26 scores in the initial analysis was based on the fact that it was the most common tool used among all studies. However, to avoid any reporting bias and to enable comparison between screening tools all reported prevalence rates per study were made available for secondary analysis.
An assessment of studies heterogeneity using the I2 statistic was performed; the value of 75–100% was considered to represent high heterogeneity. Between-study heterogeneity was also assessed in this review by the Quoran (Q) statistic test and tau2 (τ2).
A leave-one-out sensitivity analysis was performed by iteratively removing one study at a time to confirm that our findings were not driven by any single study.
Meta-analyses were performed using OpenMetaAnalyst software [24, 25] provided by the Centre for Evidence Synthesis in Health/Center for Evidence-Based Medicine, the School of Public Health at Brown University. Other descriptive statistical analyses were performed using STATA 13.1.
Ethical considerations
As this review assessed data from publications that are indexed and available in the public domain, no ethical approval nor informed consent was applicable.
Results
Study characteristics
Eighteen studies, involving a total of 5722 respondents in nine countries were included in the analysis (Table 1). The median number of respondents per study was 223 (range 75–1107). All of the eighteen studies used a cross-sectional research design to report the prevalence of ED risk among medical students. Approximately 73% of the respondents were females. The median age of the respondents was 21 years (range 18.5–25 years), and the median BMI was 21 kg/m2 (range 20–23 kg/m2).
Prevalence of ED risk in medical students
Meta-analytic pooling of the point prevalence estimates of ED risk yielded a prevalence rate of 10.4% (497/5722 students, 95% CI 7.8–13.0%), with statistically significant evidence of between-study heterogeneity (Q = 295, τ2 = 0.003, I2 = 94.0%, P < 0.001) (Fig. 2). The details of the systematic review findings are presented in Table 2. The raw prevalence estimates reported by individual studies ranged from 2.2 to 29.1%. Sensitivity analysis demonstrated that individual study affected the overall pooled point prevalence estimate by < 1% (Fig. 3).

Summarized prevalence rates of ED risk in medical students

Summarized prevalence rates of ED risk in medical students if one study is deleted
Prevalence of ED among female medical students
Out of the eighteen studies, seven studies only included female medical students. To control for the confounding effect of sex, the meta-analysis was repeated for studies that only included female students. The meta-analytic pooling of the point prevalence estimates of ED risk reported by female medical students yielded a prevalence rate of 13.7% (144/1849 students, 95% CI 6.6–20.7%), with statistically significant evidence of between-study heterogeneity (Q = 104.5, τ2 = 0.008, I2 = 94.3%, P < 0.001).
The raw prevalence estimates reported by individual studies focused on female medical students ranged from 2.2 to 29.1%. Sensitivity analysis demonstrated that individual study affected the overall pooled point prevalence estimate by ≤ 2%.
Prevalence of ED by country
When there were three or more studies from the same country, a pooled prevalence estimate of ED risk among medical students was calculated. The following countries had three or more publications: India (n = 4), Pakistan (n = 3) and China (n = 3).
Studies from India yielded a prevalence rate of 11% (81/775 students, 95% CI 4.2–17.8%), with statistically significant evidence of study heterogeneity (Q = 38, τ2 = 0.004, I2 = 92.1%, P < 0.001). Studies from Pakistan yielded a prevalence rate of 17.1% (122/604 students, 95% CI 5.1–29.0%), with evidence of between study heterogeneity (Q = 27.3, τ2 = 0.01, I2 = 92.7%, P < 0.001). Finally, studies from China yielded a prevalence rate of 2.2% (47/2091 students, 95% CI 1.6–2.9%), with no evidence of between study heterogeneity (Q = 0.54, τ2 = 0.001, I2 = 0%, P < 0.77).
Heterogeneity within ED screening instruments
To identify potential sources of heterogeneity of the screening instruments used within the studies; results from surveys with the same instrument only were meta-analyzed.
Fourteen out of the eighteen studies (78%) used the EAT-26 [17,18,19, 22, 23, 26, 27, 29, 30, 33,34,35,36,37]. The meta-analytic pooling of the prevalence estimates of ED risk yielded a prevalence rate of 10.5% (345/3520 students, 95% CI 8.7–16.4%), with statistically significant evidence of between-study heterogeneity (Q = 204.8, τ2 = 0.003, I2 = 93.6%, P < 0.001).
Three out of the eighteen studies (17%) used the SCOFF [19, 22, 23]. The meta-analytic pooling of the prevalence estimates of ED yielded a prevalence rate of 21.9% (174/810 students, 95% CI 12.6–31.2%), with statistically significant evidence of between-study heterogeneity (Q = 19.3, τ2 = 0.006, I2 = 89.7%, P < 0.001). In addition to SCOFF, these three studies also used the EAT-26, thus a repeat meta-analytic pooling of the prevalence estimates of ED risk was conducted. Results showed a prevalence rate of 20.1% (161/810 students, 95% CI 9–31.3%), with statistically significant evidence of between-study heterogeneity (Q = 33.3, τ2 = 0.009, I2 = 94%, P < 0.001).
Two out of the eighteen studies (11%) used the EDI-1 only [28, 32]. The meta-analytic pooling of the prevalence estimates of ED risk yielded a prevalence rate of 10% (42/1203 students, 95% CI 0–2.6%), with statistically significant evidence of between-study heterogeneity (Q = 17.2, τ2 = 0.01, I2 = 94.2%, P < 0.001).
Discussion
This systematic review and meta-analysis of eighteen research studies involved 5722 medical students in nine countries and demonstrated that 10.4% of the students screened were positive/at risk for ED. The prevalence rate of ED risk among medical students obtained by this meta-analysis was higher than that reported in the general population which is estimated to be about 5% [38]. It must be acknowledged here that none of the studies included in this meta-analysis actually presented data about diagnosed ED. Rather, each of the eighteen studies presented descriptive statistics based on pre-established cut-off scores of screening instruments. As these continuous measures of eating pathology were not meant to be used as diagnostic tools, but rather as indicators of ED risk, results from this study cannot be interpreted as providing prevalence rates of ED.
Nevertheless, a comparison between the pooled prevalence rate of ED risk among medical students with the reported estimates of ED among university students reveals that both groups have comparable ED risk of approximately 10% [16, 39, 40]. This finding highlights that ED risk are pervasive among university age students with some variation across student characteristics.
The prevalence rate finding of 10.4% is alarming given the fact that ED have the potential to lead to other serious physical or mental health problems. Previous research shows that more than 80% of individuals with ED risk have at least one comorbid psychiatric disorder including anxiety disorders (> 50%), affective disorders (> 40%), deliberate self-harm (> 20%), and substance use (> 10%) [41,42,43]. Individuals with diagnosed ED may develop physical health issues including skeletal complications [44], edema [1], cardiac failure [45], pancreatitis [46], and infertility [47]. Thus, it is clearly evident that ED have severe and persistent health consequences; and therefore, early identification and treatment is important.
The median age of the respondents was 21 years (range 18.5–25 years). This finding related to the peak age at onset; late adolescence and young adulthood have been identified as important developmental periods for the development of ED risk and related conditions [16]. During the transitions to adulthood, young individuals face many stressors to become independent, and begin to look at the future in terms of relationships, schooling, career, etc. The first year as an undergraduate university student can be significantly stressful [39, 48]. The major stressors among university students are changes in environment, academic workload, new relationships and time management issues [49].
Female medical students appeared to be at more risk for ED with a prevalence rate of 13.7% (95% CI 6.6–20.7%) compared to the prevalence rate of eating disorders among medical students. No data were available to analyze prevalence among male medical students only and this perhaps an area for future research to address. Nonetheless, given the prevalence rate for ED risk and the females only prevalence rate of ED risk, it appears that there is a difference between men and women when it comes to ED. Eating disorders have been predominantly presenting in young females [50]. Young women have specific attitudes toward food and body weight, aiming to achieve and maintain a slim body shape; great importance is given to thinness as requisite for self-esteem [16, 42]. Recent research suggests that the prevalence and manifestations of ED among young men is increasing in community samples [51]. The male body image; the great importance given to low body fat and pronounced muscles to achieve muscular physique, has emerged as an important factor for increasing the prevalence of ED among men [18].
Three countries had a significant number of publications. Pooling the results of the same country showed mixed results. Studies from India and Pakistan showed evidence of between-study heterogeneity with prevalence of 11.0% (I2 = 92.1%, P < 0.001) and 17.1% (I2 = 92.3%, P < 0.001) for India and Pakistan, respectively.
However, studies from China showed no significant evidence of between-study heterogeneity (I2 = 0%, P < 0.77). This may be due to the different ethnic and cultural contexts in defining and measuring ED. Culture has been documented as significant to the cause and presentation of ED [52]. The large variety within the same country might be also explained by socio-economic factors and difference in sample characteristics.
When interpreting the findings from this systematic review and meta-analysis, it is very important to acknowledge that these were primarily self-reported. Self-report questionnaires measure symptoms and risk behaviors for ED and do not provide a specific clinical diagnosis. Although these self-report tools of ED have limitations, they are very important to screen subclinical or threshold symptoms for ED risk. They will identify subjects with eating behaviors that are not considered normal, but they may not yet have disordered enough to qualify for a formal diagnosis. Furthermore, it must also be acknowledged that from a research perspective the use of self-report tools is the only way to protect the anonymity of the medical students during data collection.
To control for the possible differences between the different screening tools, a decision was taken to meta-analyses studies using the EAT-26. Results of this analysis showed a point prevalence rate of ED risk 10.5% (95% CI 7.3–13.7%), with statistically significant evidence of between-study heterogeneity (I2 = 93.6%, P < 0.001). A similar point prevalence rate of ED risk 10% (95% CI 0–2.6%), with statistically significant evidence of between-study heterogeneity (I2 = 94.2%, P < 0.001) was obtained using EDI-1.
Three studies used both EAT-26 and SCOFF and yielded a prevalence rate of eating disorders 20.1% (95% CI 9–31.3%) and of 21.9% (95% CI 12.6–31.2%) for EAT-26 and SCOFF, respectively.
These findings are perhaps suggestive that EAT-26 can adequately screen ED at risk cases.
Limitations
This review has two main limitations. First, the data were collated from studies that had different screening instruments and with some variations in the quality of design, specifically sample size and the reliance on one study site. This perhaps can explain the heterogeneity between studies and therefore pooled estimates must be interpreted with caution. Second, the prevalence rates are based on self-report instruments using cross-sectional designs without interviews to determine congruence with ED diagnostic criteria. Nonetheless, these questionnaires are cost-effective, specific and demonstrate good psychometric properties. Results from this study cannot be interpreted as providing prevalence rates of ED, however, these results are very useful as an indicator of ED risk.
Implications and future research directions
The high prevalence of ED risk among medical students requires ongoing monitoring, accurate diagnosis and management interventions to reduce these disorders. There is a legitimate need for further research in the field particularly in parts of the world where the prevalence of ED is under investigated among medical students, e.g., the Middle East and North Africa. Future epidemiological studies are encouraged to follow a prospective study design so that the same students can be assessed over time. Multiple tools to measure ED risk will provide information on superiority in detecting cases and will allow specificity and sensitivity comparisons. The use of additional tools to screen for comorbidities such as anxiety or depressive symptoms will provide an opportunity to understand the association between ED risk and other pathologies. The association between stress and ED risk needs to receive more attention. Epidemiological research is also urged to follow the Strengthening the Reporting of Observational Studies in Epidemiology guidelines to completely and accurately report data. Related comparison groups, e.g. medical interns or residents, can be also used to determine if medical students will carry the ED risk after transition to residency. Finally, future reviews are encouraged to utilize meta-regression techniques to analyze the moderating effect of some covariates on ED risk among medical students.
Conclusion
In this systematic review and meta-analysis, the summary estimate of the prevalence of ED risk among medical students was 10.4%. Future studies are needed to identify and prevent ED in this population.
References
Sachs K, Andersen D, Sommer J et al (2015) Avoiding medical complications during the refeeding of patients with anorexia nervosa. Eat Disord 23:411–421. https://doi.org/10.1080/10640266.2014.1000111
Smink FRE, van Hoeken D, Hoek HW (2012) Epidemiology of eating disorders: incidence, prevalence and mortality rates. Curr Psychiatry Rep 14:406–414. https://doi.org/10.1007/s11920-012-0282-y
Sweeting H, Walker L, MacLean A et al (2015) Prevalence of eating disorders in males: a review of rates reported in academic research and UK mass media. Int J Mens Health. https://doi.org/10.3149/jmh.1402.86
Sim LA, McAlpine DE, Grothe KB et al (2010) Identification and treatment of eating disorders in the primary care setting. Mayo Clin Proc 85:746–751. https://doi.org/10.4065/mcp.2010.0070
Arcelus J, Mitchell AJ, Wales J, Nielsen S (2011) Mortality rates in patients with anorexia nervosa and other eating disorders. A meta-analysis of 36 studies. Arch Gen Psychiatry 68:724–731. https://doi.org/10.1001/archgenpsychiatry.2011.74
Franko DL, Keshaviah A, Eddy KT et al (2013) Do mortality rates in eating disorders change over time? A longitudinal look at anorexia nervosa and bulimia nervosa. Am J Psychiatry 170:917–925. https://doi.org/10.1176/appi.ajp.2013.12070868
Evans EJ, Hay PJ, Mond J et al (2011) Barriers to help-seeking in young women with eating disorders: a qualitative exploration in a longitudinal community survey. Eat Disord 19:270–285. https://doi.org/10.1080/10640266.2011.566152
Identifying people at risk. http://www.nedc.com.au/identifying-people-at-risk. Accessed 4 Apr 2018
Garner DM, Olmsted MP, Bohr Y, Garfinkel PE (1982) The eating attitudes test: psychometric features and clinical correlates. Psychol Med 12:871–878
Garner DM, Olmstead MP, Polivy J (1983) Development and validation of a multidimensional eating disorder inventory for anorexia nervosa and bulimia. Int J Eat Disord 2:15–34. https://doi.org/10.1002/1098-108X(198321)2:2<15::AID-EAT2260020203>3.0.CO;2-6
Mond JM, Hay PJ, Rodgers B, Owen C (2006) Eating Disorder Examination Questionnaire (EDE-Q): norms for young adult women. Behav Res Ther 44:53–62. https://doi.org/10.1016/j.brat.2004.12.003
Morgan JF, Reid F, Lacey JH (2000) The SCOFF questionnaire: a new screening tool for eating disorders. West J Med 172:164–165
Rotenstein LS, Ramos MA, Torre M et al (2016) Prevalence of depression, depressive symptoms, and suicidal ideation among medical students: a systematic review and meta-analysis. JAMA 316:2214–2236. https://doi.org/10.1001/jama.2016.17324
Puthran R, Zhang MWB, Tam WW, Ho RC (2016) Prevalence of depression amongst medical students: a meta-analysis. Med Educ 50:456–468. https://doi.org/10.1111/medu.12962
Pacheco JP, Giacomin HT, Tam WW et al (2017) Mental health problems among medical students in Brazil: a systematic review and meta-analysis. Rev Bras Psiquiatr Sao Paulo Braz 1999 39:369–378. https://doi.org/10.1590/1516-4446-2017-2223
Tavolacci MP, Grigioni S, Richard L et al (2015) Eating disorders and associated health risks among university students. J Nutr Educ Behav 47:412–420.e1. https://doi.org/10.1016/j.jneb.2015.06.009
Bosi MLM, Nogueira JAD, Alencar CH, Moreira JA (2016) Body image and eating behavior among medical students: eating disorders among medical students. Epidemiol Open Access 6:1–4. https://doi.org/10.4172/2161-1165.1000256
Liao Y, Knoesen NP, Castle DJ et al (2010) Symptoms of disordered eating, body shape, and mood concerns in male and female Chinese medical students. Compr Psychiatry 51:516–523. https://doi.org/10.1016/j.comppsych.2009.11.007
Shashank J, Praveen G, Chethan T (2016) A crosssectional study to asses the eating disorder among female medical students in a Rural Medical College of Karnataka State. Natl J Community Med 7:524–527
Fidan T, Ertekin V, Işikay S, Kirpinar I (2010) Prevalence of orthorexia among medical students in Erzurum, Turkey. Compr Psychiatry 51:49–54. https://doi.org/10.1016/j.comppsych.2009.03.001
Liberati A, Altman DG, Tetzlaff J et al (2009) The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med 6:e1000100. https://doi.org/10.1371/journal.pmed.1000100
Vijayalakshmi P, Thimmaiah R, Reddy SSN et al (2017) Gender differences in body mass index, body weight perception, weight satisfaction, disordered eating and weight control strategies among Indian Medical and Nursing Undergraduates. Investig Educ Enferm 35:276–284. https://doi.org/10.17533/udea.iee.v35n3a04
Memon AA, Adil SE-E-R., Siddiqui EU et al (2012) Eating disorders in medical students of Karachi, Pakistan-a cross-sectional study. BMC Res Notes 5:84. https://doi.org/10.1186/1756-0500-5-84
Wallace BC, Schmid CH, Lau J, Trikalinos TA (2009) Meta-analyst: software for meta-analysis of binary, continuous and diagnostic data. BMC Med Res Methodol 9:80. https://doi.org/10.1186/1471-2288-9-80
OpenMeta[Analyst]—CEBM @ Brown. http://www.cebm.brown.edu/openmeta/index.html. Accessed 26 Jan 2018
Gupta N, Bhargava R, Chavan BS, Sharan P (2017) Eating attitudes and body shape concerns among medical students in Chandigarh. Indian J Soc Psychiatry 33:219. https://doi.org/10.4103/0971-9962.214605
Szweda S, Thorne P (2002) The prevalence of eating disorders in female health care students. Occup Med Oxf Engl 52:113–119
Chang W-W, Nie M, Kang Y-W et al (2015) Subclinical eating disorders in female medical students in Anhui, China: a cross-sectional study. Nutr Hosp 31:1771–1777. https://doi.org/10.3305/nh.2015.31.4.8456
Ngan SW, Chern BCK, Rajarathnam DD et al (2017) The relationship between eating disorders and stress among medical undergraduate: a cross-sectional study. Open J Epidemiol 07:85. https://doi.org/10.4236/ojepi.2017.72008
Babar N, Alam M, Ali SS et al (2002) Anorexic behaviour and attitudes among female medical and nursing students at a private university hospital. JPMA J Pak Med Assoc 52:272–276
Hamburg P, Herzog DB (1985) Studying reports of women medical students on their eating disorders. Acad Med 60:644
Futch LS, Wingard DL, Felice ME (1988) Eating pattern disturbances among women medical and graduate students. J Adolesc Health Care Off Publ Soc Adolesc Med 9:378–383
Liao Y, Liu T, Cheng Y et al (2013) Changes in eating attitudes, eating disorders and body weight in Chinese medical university students. Int J Soc Psychiatry 59:578–585. https://doi.org/10.1177/0020764012445862
Manaf NA, Saravanan C, Zuhrah B (2016) The prevalence and inter-relationship of negative body image perception, depression and susceptibility to eating disorders among female medical undergraduate students. J Clin Diagn Res JCDR 10:VC01-VC04. https://doi.org/10.7860/JCDR/2016/16678.7341
Alberton VC, Dal-Bó MJ, Piovezan AP, Silva RM da (2013) Abnormal eating behaviors among medical students at a university in southern Santa Catarina, Brazil. Rev Bras Educ Méd 37:15–20. https://doi.org/10.1590/S0100-55022013000100003
Panchami P, Samuel T (2016) A cross-sectional study of disturbed eating attitudes and behaviours in medical students. Int J Res Med Sci 4:2830–2833. https://doi.org/10.18203/2320-6012.ijrms20161959
Haroon S, Usman M, Hafeez M (2016) Eating disorders in medical students of Islamabad Pakistan—a cross-sectional study. Ophthalmol Update ISSN 1993–2863:89–92
Treasure J, Claudino AM, Zucker N (2010) Eating disorders. Lancet Lond Engl 375:583–593. https://doi.org/10.1016/S0140-6736(09)61748-7
Eisenberg D, Nicklett EJ, Roeder K, Kirz NE (2011) Eating disorder symptoms among college students: prevalence, persistence, correlates, and treatment-seeking. J Am Coll Health J ACH 59:700–707. https://doi.org/10.1080/07448481.2010.546461
Varela-Mato V, Cancela JM, Ayan C et al (2012) Lifestyle and health among Spanish university students: differences by gender and academic discipline. Int J Environ Res Public Health 9:2728–2741. https://doi.org/10.3390/ijerph9082728
Keski-Rahkonen A, Mustelin L (2016) Epidemiology of eating disorders in Europe: prevalence, incidence, comorbidity, course, consequences, and risk factors. Curr Opin Psychiatry 29:340–345. https://doi.org/10.1097/YCO.0000000000000278
Tavolacci MP, Ladner J, Grigioni S et al (2013) Prevalence and association of perceived stress, substance use and behavioral addictions: a cross-sectional study among university students in France, 2009–2011. BMC Public Health 13:724. https://doi.org/10.1186/1471-2458-13-724
Fragkos KC, Frangos CC (2013) Assessing eating disorder risk: the pivotal role of achievement anxiety, depression and female gender in non-clinical samples. Nutrients 5:811–828. https://doi.org/10.3390/nu5030811
Donaldson AA, Gordon CM (2015) Skeletal complications of eating disorders. Metabolism 64:943–951. https://doi.org/10.1016/j.metabol.2015.06.007
Jáuregui-Garrido B, Jáuregui-Lobera I (2012) Sudden death in eating disorders. Vasc Health Risk Manag 8:91–98. https://doi.org/10.2147/VHRM.S28652
Tong J, D’Alessio D (2011) Eating disorders and gastrointestinal peptides. Curr Opin Endocrinol Diabetes Obes 18:42–49. https://doi.org/10.1097/MED.0b013e328341e12b
Linna MS, Raevuori A, Haukka J et al (2013) Reproductive health outcomes in eating disorders. Int J Eat Disord 46:826–833. https://doi.org/10.1002/eat.22179
Ansari WE, Clausen SV, Mabhala A, Stock C (2010) How do I look? Body image perceptions among university students from England and Denmark. Int J Environ Res Public Health 7:583–595. https://doi.org/10.3390/ijerph7020583
Britz J, Pappas E (2010) Sources and outlets of stress among university students: correlations between stress and unhealthy habits. Undergrad Res J Hum Sci 9. http://www.kon.org/urc/v9/britz.html
Sharan P, Sundar AS (2015) Eating disorders in women. Indian J Psychiatry 57:S286–S295. https://doi.org/10.4103/0019-5545.161493
Blond A (2008) Impacts of exposure to images of ideal bodies on male body dissatisfaction: a review. Body Image 5:244–250. https://doi.org/10.1016/j.bodyim.2008.02.003
Pike KM, Hoek HW, Dunne PE (2014) Cultural trends and eating disorders. Curr Opin Psychiatry 27:436–442. https://doi.org/10.1097/YCO.0000000000000100
Funding
No funds were received towards the study at any stage.
Author information
Authors and Affiliations
Contributions
HJ and AA designed the study. MS, MF, HJ, AB coordinated data search, data entry and data cleaning. HJ performed statistical analyses and wrote the first draft. AA and MF provided intellectual contributions to strengthening the manuscript and suggested additional data analyses. All authors provided critical revisions of manuscript and approved the final version.
Corresponding author
Ethics declarations
Conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Ethical approval
This article does not contain any studies with human participants performed by any of the authors.
Informed consent
For this type of study formal consent is not required.
Rights and permissions
About this article

Cite this article
Jahrami, H., Sater, M., Abdulla, A. et al. Eating disorders risk among medical students: a global systematic review and meta-analysis. Eat Weight Disord 24, 397–410 (2019). https://doi.org/10.1007/s40519-018-0516-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40519-018-0516-z