
Abstract
Purpose
The purpose of this study was to determine the cut-off values of triglycerides and glucose (TyG) index as one of the indirect indices for metabolic syndrome (MetS) in a pediatric population.
Methods
This national study was conducted in 2015 on 14400 students, aged 7–18 years. They were selected by random cluster sampling from 30 provinces of our country during the fifth survey of a national school-based surveillance program. MetS was defined based on the Adult Treatment Panel III (ATP III) criteria modified for the pediatric age group. The cut-off values of TyG index for MetS were obtained using the receiver operation characteristic (ROC) curve analysis by gender and age groups.
Results
Totally, 3843 students (52.3% boys) with mean (SD) age of 12.45 (3.04) years were assessed. The area under the ROC curve of TyG index for MetS was 0.83 in total participants. According to the ATP III criteria the cut-off values of the TyG index were 8.33 (8.21–8.45) in total students, 8.47 (8.36–8.58) in boys, and 8.33 (8.18–8.48) in girls. In the 7–12 and 13–18 years’ age groups, these values were 8.47 (8.32–8.63) and 8.34 (8.22–8.45) in total, 8.39 (8.26–8.52) and 8.47 (8.33–8.61) in boys, 8.33 (8.11–8.55) and 8.35 (8.22–8.47) in girls, respectively.
Conclusion
The findings of this study can be clinically helpful for screening MetS in children and adolescents but the effectiveness of these criteria needs to be evaluated by further longitudinal surveys.
Level of evidence
Level V, cross-sectional descriptive study (National surveillance study).
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Metabolic syndrome (MetS), a major risk factor in diabetes and cardiovascular disease, is rising in the adolescents due to the worldwide increased prevalence of obesity in this age population group [1]. Since MetS at young age is so closely related to metabolic disorders in adulthood, early recognition and treatment of at risk groups is very important [2]. Population-based studies show that higher anthropometric indices including weight, waist and hip circumferences as well as higher epicardial adipose tissue are associated with elevated risk of MetS in pediatrics [3, 4]. One of the possible methods for screening at-risk groups for MetS is insulin resistance measurements by the pancreatic suppression test or the hyperinsulinemic–euglycemic clamp technique [5]. However, these tests are invasive, expensive and complicated, so they are not suitable for clinical and epidemiological studies. Regarding the difficulties in fasting insulin measurement, an insulin-free surrogate for evaluating insulin resistance was sought and developed. Studies have shown that increased serum triglyceride (TG) can compromise muscle glucose metabolism and leads to a decrease in insulin sensitivity [6]. Therefore, fasting levels of triglycerides and glucose, the so-called triglycerides and glucose index (TyG index), seems to be an appropriate substitute marker of insulin resistance among adolescents [7]. The TyG index is a convenient, cost-effective and logical method for evaluating of insulin resistance, which is based on fasting TG and glucose instead of fasting insulin and glucose [8]. However, there are limited pediatric data regarding this index, and a valid cut-off value has not been established in Iran. Therefore, we conducted this study with the aim of determining of TyG index and finding valid cut-off values for metabolic abnormalities in a representative sample of Iranian children and adolescents.
Materials and methods
Study design and population
The data of current study were obtained from the fifth phase of a national school-based surveillance survey entitled “Childhood and Adolescence Surveillance and Prevention of Adult Non-communicable Disease” (CASPIAN) in 2015. The CASPIAN study is a large nationwide survey in Iran which was conducted on children and adolescents. There are vast data about this pediatrics study which are analyzed with different hypotheses, questions and approaches. Considering this article, the triglyceride–glucose index has not been analyzed in the CASPIAN study, so far. It is for the first time this index has been calculated and analyzed for predicting metabolic syndrome. However, the prevalence of metabolic syndrome and its association with other indices have been published in other articles. The study population was 14,400 individuals aged 7–18 years from urban and rural areas of 30 provinces in Iran. They were selected using multistage, stratified cluster sampling method. Sampling within each province was performed based on the student’s place of residence (urban or rural) and level of education (primary and secondary) using the proportional to size method and with equal sex ratio. This means that the number of boys and girls was the same in each province, and their ratio in urban and rural areas was proportional to the number of students in urban and rural areas. Similarly, the number of samples between different grades in urban and rural areas was divided according to the number of students in each grade. Achieving the desired number of samples was obtained using cluster sampling in each province with equal cluster sizes. Clusters were determined at school levels. The size of each cluster was 10 students, which means that a total of 10 statistical units (including 10 students and their parents) would be considered in each cluster. The sample size was 480 students in each province (48 clusters of 10 students), i.e., a total of 14,400 students at the national level. This was the maximum sample size that helped in achieving a good estimate of all risk factors of interest. In each province, 14 clusters out of 48 clusters were randomly selected for the biochemical test, i.e., a total of 4200 students. There were no significant differences in demographic data and physical measurements between randomly selected and non-selected pediatrics. Protocol details of the study have been explained previously [9].
Ethics
The study protocol was approved by the Research and Ethics Council of Isfahan University of Medical Sciences (code: 194049) and a written informed consent and a verbal consent were obtained from all the parents and students, respectively.
Anthropometric and biochemical measurements
Weight was measured on a scale placed on a flat ground to the nearest 0.1 kg while the subjects were minimally clothed. Height was measured in a standing position to the nearest 0.5 cm, without shoes [10]. Body mass index (BMI) was calculated as weight (kg) divided by square of height (m2). Waist circumference (WC) was measured using non-stretchable plastic tape between the uppermost lateral border of right ilium and that of left ilium to the nearest 0.1 cm. Hip circumference (HC) was measured using non-stretchable plastic tape at the widest part of the hip at the level of the greater trochanter to the nearest 0.1 cm [11]. Neck circumference was measured in the midway of the neck, between mid-cervical spine and mid anterior neck, to the nearest 0.1 cm, using a non-stretchable plastic tape with the subjects standing upright [12]. Wrist circumference was measured to the nearest 0.1 cm with subjects in a seated position using a non-stretchable plastic tape over the Lister tubercle of the distal radius and over the distal ulna [13]. World Health Organization (WHO) growth curves were used for categorizing of BMI; overweight as sex-specific BMI for age of 85th–95th, and obesity as sex-specific BMI for > 95th. Abdominal obesity was defined as waist-to-height ratio (WHtR) equal to or more than 0.5 [10].
Blood pressure (BP) was measured two times in the sitting position after 15 min of rest using a standardized mercury sphygmomanometer on the right arm. The first and fifth Korotkoff sounds were recorded as systolic blood pressure (SBP) and diastolic blood pressure (DBP), respectively. The average of the two recorded values was used in the analyses. Fasting blood samples were taken after 12–14 h of overnight fast. Fasting blood glucose (FBG), total cholesterol (TC), low density lipoprotein-cholesterol (LDL-C), high density lipoprotein-cholesterol (HDL-C), and triglycerides (TG) were measured enzymatically by Hitachi auto-analyzer (Tokyo, Japan) [14].
Definition
In this study, MetS was defined according to Adult Treatment Panel III (ATP III) criteria modified for the pediatric age group. Participants who had at least three of the following criteria were classified as having MetS: TG concentration of 150 mg/dL or greater; HDL-C concentration of 40 mg/dL or less; FBG concentration of 100 mg/dL or greater; abdominal obesity: waist-to-height ratio > 0.5; and either SBP or DBP greater than the 90th percentile for age, sex, and height [15]. The TyG index was calculated as follows: TyG index = Ln [triglyceride (mg/dL) × fasting glucose (mg/dL)/2] [16].
Statistical analysis
All variables were checked for normality and presented as the mean ± standard deviation, or number (percentage). The independent sample t test was used to compare continuous variables and the Chi-square test was used to compare proportions according to age and sex groups. TyG index is presented in deciles by age and sex groups. To estimate valid cut-off values of TyG index for predicting metabolic syndrome, the receiver operation characteristic (ROC) curve analysis was used with an estimation of the sensitivity and specificity. Data were analyzed separately for sex and age groups. The estimated cut-off values were determined using the minimum value of which represents the maximum sum of sensitivity and specificity. The area under curve (AUC) shows the ability of TyG index cut-off points to discriminate students with and without metabolic syndrome. Analyses were performed using STATA version 11.0 (STATA Statistical Software: Release 11. STATA Corp LP. Package, College Station, TX, USA); P values less than 0.05 were considered as statistically significant.
Results
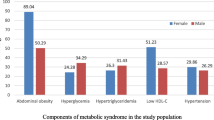
Totally, 3843 students (52.3% boys) with mean (SD) age of 12.45 (3.04) years were assessed. According to WHO criteria, 9.4% of participants (8.7% of boys and 10.2% of girls) were overweight and 11.4% (12.5% of boys and 10.3% of girls) were obese. Abdominal obesity was documented in 21.1% of students (21.6% of boys and 20.5% of girls). Mean of TyG index in normal-weight, overweight and obese pediatrics was 8.19, 8.25, 8.21 in the 7–12 years’ age group and 8.20, 8.23, 8.20 in the 13–18 years’ age group, respectively, and there was no significant difference in the mean values of TyG index among different weight status (P > 0.05). The general characteristics of participants including anthropometric, clinical, and biochemical measurements according to age and gender are presented in Table 1. In the 7–12 years’ age group, no significant differences were observed between boys and girls except for the mean values of waist, wrist and neck circumferences which were significantly lower in girls (P < 0.01). In the 13–18 years’ age group, the mean values of waist, wrist and neck circumferences, weight, SBP, DBP, total cholesterol and LDL-C were significantly higher in boys compared to girls (P < 0.01). There were no significant differences in the mean values of TyG index and the prevalence of MetS between male and female participants in both age groups.
The distribution of the TyG index by age and gender is summarized in Table 2. In the 7–12 years’ age group, the 5th percentile of TyG index was 7.49 in both boys and girls. In the 13–18 years’ age group, the 5th percentile of TyG index was 7.49 and 7.48 in boys and girls, respectively. In the 7–12 years’ age group, the 95th percentile of TyG index was 9.03 and 8.99 in boys and girls, respectively, and in the 13–18 years’ age group, it was 9.02 and 9.04 in boys and girls, respectively.
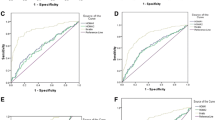
The ROC curves of the TyG index for MetS according to ATP III criteria are displayed in Fig. 1, stratified by age groups. The area under the curve (AUC) revealed values of 0.83 for the 7–18 years’ age group, 0.82 for the 7–12 years’ age group and 0.83 for the 13–18 years’ age group (Fig. 1).

ROC curves for metabolic syndrome by age. a ROC curves for metabolic syndrome in the 7–18 years’ age group. b ROC curves for metabolic syndrome in the 7–12 years’ age group. c ROC curves for metabolic syndrome in the 13–18 years’ age group. ROC receiver operating characteristic
The cut-off values of the TyG index with their corresponding sensitivity, specificity and AUC for metabolic syndrome by gender and age groups were tabulated in Table 3. The cut-off values of the TyG index were 8.33 (sensitivity: 87% and specificity: 68%) in total participants, 8.47 (sensitivity: 77% and specificity: 78%) in boys, and 8.33 (sensitivity: 90% and specificity: 67%) in girls. In the 7–12 and 13–18 years’ age groups, these values were 8.47 (sensitivity: 75% and specificity: 78%) and 8.34 (sensitivity: 89% and specificity: 68%) in total, 8.39 (sensitivity: 80% and specificity: 73%) and 8.47 (sensitivity: 81% and specificity: 78%) in boys, 8.33 (sensitivity: 91% and specificity: 68%) and 8.35 (sensitivity: 88% and specificity: 68%) in girls, respectively.
Discussion
In this study we determined the cut-off values of the TyG index, 8.33 in total participants, 8.47 in boys, and 8.33 in girls. The area under the ROC curve (AUC) of TyG index for MetS was 0.83.
MetS is growing in the pediatric age group especially in Middle East countries [17]. The prevalence of MetS in Iranian children and adolescents has been increased [18]. However, no study has examined the cut-off values of surrogate measures of MetS in Iranian pediatrics. Several population-based studies have demonstrated the clinical advantages of the TyG index as a surrogate measure for insulin resistance [19,20,21,22], but since the range of triglyceride and MetS is diverse in different populations, it is essential to validate the new indices in each population. Therefore, in this study, for the first time we tried to indicate the percentile distribution of TyG index, as one of the indirect indices for MetS, and its cut-off values in Iranian children and adolescents with the aim of screening at-risk groups of MetS.
Insulin resistance is strongly associated with MetS, so several population-based studies have used MetS as the indicator of insulin resistance and proposed cut-off values using ROC curves for MetS [23,24,25,26,27]. In this study we conducted ROC curve analysis of the TyG index for MetS according to ATP III criteria for children and adolescents to determine a valid cut-off value. The ROC curve is an appropriate method for determination of an ideal cut-off value by considering both sensitivity (true positives) and specificity (true negatives). It propose a graphical illustration of each cut-off value for any diagnostic test that uses a continuous variable [28]. Therefore, it is a suitable tool for MetS diagnosis. The area under the ROC curve (AUC) is widely realized as the measure of a diagnostic test’s discriminative power. The maximum value for the AUC is 1.0, but, in general, ROC curves with an AUC more than 0.75 are clinically useful [29]. In current study, the AUC of TyG index for MetS was 0.83 which demonstrating a suitable discriminative power and potential utility for diagnosis of MetS.
The cut-off value of TyG index was 8.33 in total participants which was somehow similar to previous studies [30, 31]. In a study performed on different ethnics of American and Korean adolescents, the cut-off values for TyG index was evaluated according to three metabolic syndrome definitions commonly used in adolescents and ranged from 8.45 to 8.65 in Mexican American, Non-Hispanic White, from 8.35 to 8.55 in Korean adolescents and from 8.15 to 8.35 in Non-Hispanic Black adolescents [32]. Kim et al. compared the cut-off values of two methods of insulin resistance measurements for MetS in 10- to 18-year-old Korean subjects. The cut-off values of the homeostasis model assessment (HOMA-IR) and TyG index were 3.29 and 8.48, respectively, according to the criteria of Cook et al.; 2.96 and 8.41, respectively, according to the criteria of de Ferranti et al.; and 3.54 and 8.66, respectively, according to the criteria of the IDF [33].
It has been demonstrated that TyG index is associated with several parameters of insulin resistance and totally contributes better performance in comparison with the HOMA-IR for screening of insulin resistance [34,35,36]. These results can be justified by the fact that the TyG index consists of two main parts of MetS including fasting level of TG and glucose in its equations; however, HOMA-IR consists of only one component of fasting glucose in MetS.
In the present study for the first time we contribute cut-off values of TyG index for MetS in Iranian children and adolescents by age and gender groups. However, this study has some limitations. First of all, we used only one definition for MetS, but since there is no outcome about the determining of MetS in children and adolescents, it was better to use different definitions for MetS. Moreover, in our survey TyG index was not compared with other direct or indirect methods of insulin resistance measurements.
Conclusion
The area under the ROC curve (AUC) of TyG index for MetS was 0.83 in total participants. The cut-off values of the TyG index according to ATP III criteria were 8.33 (8.21–8.45) in total participants, 8.47 (8.36–8.58) in boys, and 8.33 (8.18–8.48) in girls. These outcomes are clinically helpful for diagnosing MetS in children and adolescents. However, for obtaining more valid cut-off values, further studies with stratification of at-risk groups using the different criteria for MetS and also correlation studies between the TyG index and the gold standard methods for insulin resistance are suggested.
References
Day C (2007) Metabolic syndrome, or what you will: definitions and epidemiology. Diabetes Vasc Dis Res 4:32–38. https://doi.org/10.3132/dvdr.2007.003
Morrison JA, Friedman LA, Wang P, Glueck CJ (2008) Metabolic syndrome in childhood predicts adult metabolic syndrome and type 2 diabetes mellitus 25 to 30 years later. J Pediatr 152:201–206. https://doi.org/10.1016/j.jpeds.2007.09.010
Ejtahed HS, Qorbani M, Motlagh ME, Angoorani P, Hasani-Ranjbar S, Ziaodini H et al (2017) Association of anthropometric indices with continuous metabolic syndrome in children and adolescents: the CASPIAN-V study. Eat Weight Disord. https://doi.org/10.1007/s40519-017-0455-0 (online)
Barbaro G, Piedimonte A, Podagrosi M, Mercurio R, Mosca A, D’Avanzo M et al (2016) Epicardial adipose tissue and signs of metabolic syndrome in children. Eat Weight Disord 21:269–286. https://doi.org/10.1007/s40519-015-0221-0
Bergman RN, Phillips LS, Cobelli C (1981) Physiologic evaluation of factors controlling glucose tolerance in man: measurement of insulin sensitivity and beta-cell glucose sensitivity from the response to intravenous glucose. J Clin Investig 68:1456–1467. https://doi.org/10.1172/JCI110398
Kelley DE, Goodpaster BH (2001) Skeletal muscle triglyceride. An aspect of regional adiposity and insulin resistance. Diabetes Care 24:933–941. https://doi.org/10.2337/diacare.24.5.933
Guerrero-Romero F, Simental-Mendia LE, Gonzalez-Ortiz M, Martinez-Abundis E, Ramos-Zavala MG, Hernandez-Gonzalez SO et al (2010) The product of triglycerides and glucose, a simple measure of insulin sensitivity. Comparison with the euglycemic–hyperinsulinemic clamp. J Clin Endocrinol Metab 95:3347–3351. https://doi.org/10.1210/jc.2010-0288
Kang B, Yang Y, Lee EY, Yang HK, Kim HS, Lim SY et al (2017) Triglycerides/glucose index is a useful surrogate marker of insulin resistance among adolescents. Int J Obes 41:789–792. https://doi.org/10.1038/ijo.2017.14
Motlagh ME, Ziaodini H, Qorbani M, Taheri M, Aminaei T, Goodarzi A et al (2017) Methodology and early findings of the fifth survey of childhood and adolescence surveillance and prevention of adult noncommunicable disease: the CASPIAN-V study. Int J Prev Med 8:4. https://doi.org/10.4103/2008-7802.198915
Organization WH (1995) Physical status: the use of and interpretation of anthropometry, Report of a WHO Expert Committee
Knowles K, Paiva L, Sanchez S, Revilla L, Lopez T, Yasuda M et al (2011) Waist circumference, body mass index, and other measures of adiposity in predicting cardiovascular disease risk factors among Peruvian adults. Int J Hypertens. https://doi.org/10.4061/2011/931402
Aswathappa J, Garg S, Kutty K, Shankar V (2013) Neck circumference as an anthropometric measure of obesity in diabetics. N Am J Med Sci 5:28. https://doi.org/10.4103/1947-2714.106188
Nyland J, Fried A, Maitra R, Johnson DL, Caborn DN (2006) Wrist circumference is related to patellar tendon thickness in healthy men and women. Clin Imaging 30:335–338. https://doi.org/10.1016/j.clinimag.2006.02.004
McNamara JR, Schaefer EJ (1987) Automated enzymatic standardized lipid analyses for plasma and lipoprotein fractions. Clin Chim Acta 166:1–8. https://doi.org/10.1016/0009-8981(87)90188-4
Zimmet P, Alberti G, Kaufman F, Tajima N, Silink M, Arslanian S et al (2007) The metabolic syndrome in children and adolescents. Lancet 369(9579):2059–2061. https://doi.org/10.1016/s0140-6736(07)60958-1
Du T, Yuan G, Zhang M, Zhou X, Sun X, Yu X (2014) Clinical usefulness of lipid ratios, visceral adiposity indicators, and the triglycerides and glucose index as risk markers of insulin resistance. Cardiovasc Diabetol 13:146. https://doi.org/10.1186/s12933-014-0146-3
Delavari A, Forouzanfar MH, Alikhani S, Sharifian A, Kelishadi R (2009) First nationwide study of the prevalence of the metabolic syndrome and optimal cutoff points of waist circumference in the Middle East. Diabetes Care 32:1092–1097. https://doi.org/10.2337/dc08-1800
Kelishadi R, Gouya MM, Adeli K, Ardalan G, Gheiratmand R, Majdzadeh R et al (2008) Factors associated with the metabolic syndrome in a national sample of youths: CASPIAN study. Nutr Metab Cardiovasc Dis 18:461–470. https://doi.org/10.1016/j.numecd.2007.02.014
Unger G, Benozzi SF, Perruzza F, Pennacchiotti GL (2014) Triglycerides and glucose index: a useful indicator of insulin resistance. Endocrinol Nutr 61:533–540. https://doi.org/10.1016/j.endonu.2014.06.009
Lee SH, Han K, Yang HK, Kim MK, Yoon KH, Kwon HS et al (2015) Identifying subgroups of obesity using the product of triglycerides and glucose: the Korea National Health and Nutrition Examination Survey, 2008–2010. Clin Endocrinol 82:213–220. https://doi.org/10.1111/cen.12502
Lee S-H, Kwon H-S, Park Y-M, Ha H-S, Jeong SH, Yang HK et al (2014) Predicting the development of diabetes using the product of triglycerides and glucose: the Chungju Metabolic Disease Cohort (CMC) study. PLoS One 9:e90430. https://doi.org/10.1371/journal.pone.0090430
Mohd Nor NS, Lee S, Bacha F, Tfayli H, Arslanian S (2016) Triglyceride glucose index as a surrogate measure of insulin sensitivity in obese adolescents with normoglycemia, prediabetes, and type 2 diabetes mellitus: comparison with the hyperinsulinemic–euglycemic clamp. Pediatr Diabetes 17:458–465. https://doi.org/10.1111/pedi.12303
Gayoso-Diz P, Otero-González A, Rodriguez-Alvarez MX, Gude F, García F, De Francisco A et al (2013) Insulin resistance (HOMA-IR) cut-off values and the metabolic syndrome in a general adult population: effect of gender and age: EPIRCE cross-sectional study. BMC Endocr Disord 13:47. https://doi.org/10.1186/1472-6823-13-47
Tomé M, Botana M, Cadarso-Suárez C, Rego-Iraeta A, Fernández-Mariño A, Mato J et al (2009) Prevalence of metabolic syndrome in Galicia (NW Spain) on four alternative definitions and association with insulin resistance. J Eendocrinol Investig 32:505. https://doi.org/10.1007/BF03346497
Esteghamati A, Ashraf H, Esteghamati A-R, Meysamie A, Khalilzadeh O, Nakhjavani M et al (2009) Optimal threshold of homeostasis model assessment for insulin resistance in an Iranian population: the implication of metabolic syndrome to detect insulin resistance. Diabetes Res Clin Pract 84:279–287. https://doi.org/10.1016/j.diabres.2009.03.005
Lee S, Choi S, Kim HJ, Chung Y-S, Lee KW, Lee HC et al (2006) Cutoff values of surrogate measures of insulin resistance for metabolic syndrome in Korean non-diabetic adults. J Korean Med Sci 21:695–700. https://doi.org/10.3346/jkms.2006.21.4.695
Kwon HC, Woo SI, Kim YK, Ahn SM, Song KE, Jung SH et al (2005) Cutoff values of surrogate measures of insulin resistance for metabolic syndrome in Korean non-diabetic adults. Korean J Obes 14:69–75. https://doi.org/10.3346/jkms.2006.21.4.695
Grzybowski M, Younger JG (1997) Statistical methodology: III. Receiver operating characteristic (ROC) curves. Acad Emerg Med 4:818–826
Faraggi D, Reiser B (2002) Estimation of the area under the ROC curve. Stat Med 21:3093–3106. https://doi.org/10.1002/sim.1228
Simental-Mendía LE, Rodríguez-Morán M, Guerrero-Romero F (2008) The product of fasting glucose and triglycerides as surrogate for identifying insulin resistance in apparently healthy subjects. Metab Syndr Relat Disord 6:299–304. https://doi.org/10.1089/met.2008.0034
Guerrero-Romero F, Simental-Mendía LE, González-Ortiz M, Martínez-Abundis E, Ramos-Zavala MG, Hernández-González SO et al (2010) The product of triglycerides and glucose, a simple measure of insulin sensitivity. Comparison with the euglycemic–hyperinsulinemic clamp. J Clin Endocrinol Metab 95:3347–3351. https://doi.org/10.1210/jc.2010-0288
Moon S, Park J-S, Ahn Y (2017) The cut-off values of triglycerides and glucose index for metabolic syndrome in American and Korean adolescents. J Korean Med Sci 32:427–433. https://doi.org/10.3346/jkms.2017.32.3.427
Kim JW, Park SH, Kim Y, Im M, Han H-S (2016) The cutoff values of indirect indices for measuring insulin resistance for metabolic syndrome in Korean children and adolescents. Ann Pediatr Endocrinol Metab 21:143–148. https://doi.org/10.6065/apem.2016.21.3.143
Vasques ACJ, Novaes FS, de Oliveira MdS, Souza JRM, Yamanaka A, Pareja JC et al (2011) TyG index performs better than HOMA in a Brazilian population: a hyperglycemic clamp validated study. Diabetes Res Clin Pract 93:e98–e100. https://doi.org/10.1016/j.diabres.2011.05.030
Mohd Nor NS, Lee S, Arslanian SA (2015) Triglyceride Glucose (TyG) Index As a surrogate measure of insulin sensitivity in obese adolescents. Nucl Pept Regul Glucose Metab Endocr Soc. https://doi.org/10.1111/pedi.12303
Rodríguez-Morán M, Simental-Mendía L, Guerrero-Romero F (2017) The triglyceride and glucose index is useful for recognising insulin resistance in children. Acta Paediatr 106:979–983. https://doi.org/10.1111/apa.13789
Acknowledgements
This study was supported by the Ministry of Health and Medical education, Ministry of Education and Training, Isfahan University of Medical Sciences, and Endocrinology and Metabolism Research Institute of Tehran University of Medical Sciences. We are indebted to the participating schools, families and students in the study for their cooperation.
Funding
This study was funded by the Ministry of Health and Medical education, Ministry of Education and Training, Isfahan University of Medical Sciences, and Endocrinology and Metabolism Research Institute of Tehran University of Medical Sciences (Grant no. 194049).
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Angoorani, P., Heshmat, R., Ejtahed, HS. et al. Validity of triglyceride–glucose index as an indicator for metabolic syndrome in children and adolescents: the CASPIAN-V study. Eat Weight Disord 23, 877–883 (2018). https://doi.org/10.1007/s40519-018-0488-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40519-018-0488-z