
Abstract
Introduction
The present study aimed to investigate the relationship between ORTO-15 score and obsessive-compulsive symptoms, disordered eating patterns and body uneasiness among female and male university students and to examine the predictive model of ORTO-15 in both groups.
Methods
One hundred and twenty students participated in the present study (mean age 22.74 years, SD 7.31). The ORTO-15 test, the Maudsley Obsessive-Compulsive Questionnaire, the Eating Attitudes Test-26 and the Body Uneasiness Test were used for the present study.
Results
Our results revealed no gender differences in ORTO-15 score. Our results show, rather unexpectedly, that in female students lower scores, corresponding to greater severity, were related to less pathological body image discomfort and obsessive-compulsive signs, while in male students, lower ORTO-15 scores were related to less pathological eating patterns, as behaviors and symptoms.
Conclusion
Further studies regarding the relationship between ON and anorexia nervosa, as well as obsessive-compulsive symptoms, are needed to better understand the causality.
Level of Evidence Level V, descriptive study.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The discussion on the relationship between diet and health is widespread and people respond strongly to warnings about dangers caused by unhealthy diets searching food and dietary behaviors promising health. Awareness about healthful eating has increased markedly in recent years [1] and has become one of the primary concerns of Western societies [2]. To maintain a healthy lifestyle, the World Health Organization [3] recommends eating lots of fruit and vegetables, reducing fats, sugars and salt intake and exercising. However, among some people, interest in healthy eating may show obsessive signs. This psychological obsession involves concern and fixation about healthy eating and is known as “orthorexia nervosa” [4]. Orthorexia nervosa (ON) is characterized by accurate food selection, aimed especially at food quality and purity, origin, artificial preservatives or additives free [4,5,6].
At present, ON is not classified as a separate nosological entity neither in DSM-5 [7] nor in ICD-10 [8] and is far from being well known and fully understood. However, an examination of diagnostic boundaries reveals important points of symptom overlap between orthorexia nervosa and typical or atypical eating disorders [9], obsessive-compulsive disorder or somatic symptom disorder [10]. Some studies indeed suggest common clinical features between ON and other typical eating disorders, particularly anorexia nervosa [11,12,13], while other ones underline the association between ON and obsessive-compulsive disorder [14,15,16,17,18,19].
ON usually starts as a health concern followed by efforts to achieve optimum health through diet but it leads to significant damages up to malnutrition, impaired social life, and quality of life deterioration [10]. Diet becomes the main part of people’s thoughts and concerns [2] leading to distress about eating with significant dietary restrictions and consequent loss of food enjoyment, co-occurrence of anxiety with the need of control over food intake [12], rigid/inflexible eating behaviors and ritual meal preparation [11, 20] desiring to achieve self-esteem and self-realization through control of food intake [21]. Sometimes this may be associated with unintentional weight loss, apparently with no desire to lose weight rather subordinated to ideation about healthy food.
At present, there is not sufficient evidence to categorize ON as a distinct nosological entity because the relationship between ON and anorexia nervosa is still little known. Moroze et al. [22] first suggested formal diagnostic criteria, subsequently Dunn and Bratman [23] proposed more recent ones, recommended for future directions for research, reported in Table 1. The proposed ON criteria should be considered as “working criteria”, with expected revisions and modifications in the near future, rather than the proof of ON being clearly distinguishable from anorexia nervosa.
Dunn and Bratman’s criteria [23] do not include body uneasiness, defined as multifaceted construct, including general body/weight dissatisfaction, avoidance and compulsive self-monitoring behavior, feelings of disconnection from one’s own body, and concerns about specific body parts [24]. However, as the authors stated, there is a paucity of research in this area, although interesting results are reported on the relationship between body image disturbance and ON [25, 26]. The study by Varga and Máté [25] showed a positive relationship between ON and body image disturbance; when orthorexia features were expressed, body image disturbances were more severe. The study by Brytek-Matera et al. [26] suggested that orthorexic behaviors were associated with an unhealthy or negative body image among students although their strong concern about healthy and appropriate food choices. The most recent diagnostic criteria acknowledge obsessive-compulsive behavior, as previously reviewed by Koven and Abry [10] and demonstrated by Koven and Senbonmatsu [20]. As for obsessive-compulsive disorder, even orthorexia nervosa is characterized by the occurrence of persistent obsession (e.g. thinking about planning meals), repeating tasks (e.g. ritual meal preparation, weighing products) [19], social functioning disturbances and lack of perceived quality of life as a consequence of cognitive intrusions [20, 27]. Noteworthy that despite most obsessive-compulsive disorder symptoms (intrusive obsessive thoughts and repetitive, compulsive behaviors) are perceived as ego dystonic (person’s thought, behaviors, values, and feelings that are felt to be acceptable and consistent with the needs and goals of the ego), in orthorexia they are perceived as ego syntonic (person’s thought, behaviors, values, and feelings that are felt to be unacceptable, dissonant and inconsistent with the needs and goals of the ego) [5, 20].
Another issue, not fully investigated in literature, regards the gender differences and the gender role in ON development and manifestation. Findings regarding sex- related prevalence of preoccupation with healthy eating, are inconsistent: some studies found that males were more likely to have higher scores on the ORTO-15 test than females [12, 16, 27], while other results reported that the criteria for strong preoccupation with healthy eating were met predominantly by female individuals [14, 28], highlighting once again the gap in the literature on the relationship between gender and ON.
The aim of the present study was to investigate the relationship between ON and obsessive-compulsive symptoms, disordered eating patterns and body uneasiness detecting differences between women and men, and to examine the predictive model of ON in both groups. To our knowledge, this is the first single Italian center study to further investigate this relationship taking into account body image disturbances and gender differences.
Based on the existing research findings, we put forward the following hypotheses:
- H1::
-
There is no difference in ORTO-15 score between female and male students
- H2::
-
As suggested by others [29] reporting associations between obsessive control of food and eating behavior, we anticipate less pathological ORTO-15 scores will be associated with less pathological eating disturbances among both female and male students.
- H3::
-
Since the association between ORTO-15 scores and body image disturbance has been suggested by previous findings [25] we anticipate that ORTO-15 scores will be associated with body uneasiness in females.
Materials and methods
Sample
Students enrolled during the first year of the degree course in Medicine and the graduate program in Literature and Philosophy at the University of Pavia were invited to participate. Participants were enrolled during their day free time, in different locations of the University of Pavia (Italy), after posting volunteers recruitment brochures in the appropriate University message boards. Inclusion criteria were: (1) age range 19–30 years (2) in good health, (3) both genders.
Informed consent was obtained from all participants after providing them with the information on the purpose of the study and the self-administered questionnaires that would then be compiled. Anonymous data processing was guaranteed.
Institutional Review Board (IRB) approval was obtained per institutional guidelines. All procedures performed in our study were in accordance with The Code of Ethics of the World Medical Association (Declaration of Helsinki) for experiments involving humans.
Measures
The ORTO-15 test
The ORTO-15 test [16] is a self-report questionnaire with a 4-point Likert-type scale (Always, Often, Sometimes, Never), including 15 multiple-choice items. It is the first validated instrument proposed for the assessment/evaluation of ON and the estimate of its prevalence [16]. The items address the selection, preparation, consumption, and effect of, and attitude towards presumed to be healthy food. Items receiving a score of 1 reflect an orthorexic tendency, while those with 4 points score indicate normal eating behavior (lower scores refer to more ON features). It is worth pointing out that the ORTO-15 is a reverse-scoring test; therefore, lower scores correspond to a more pathological behavior.
The results of one study [27] confirmed the substantial validity of the ORTO-15 test only for 40 points threshold score; the ORTO-15 test has a sensitivity value of 100%, a specificity value of 73.6%, a positive predictive value of 17.6% and a negative predictive value of 100%, while, at 35 points threshold score, the test has an efficacy of 86.5%, with a high specificity (94.2%) and a high negative predictive value (91.1%).
Although Donini et al. [27] proposed different cut-offs (<35, <40), an ORTO-15 score <35 has been found to ensure the best predictive capability to correctly identify orthorexic symptoms among the tested cut-offs [30, 31]. In the present study the most restrictive threshold has been adopted (<35) to guarantee the highest specificity for orthorexic behaviors in a population of university students.
In the present study the Italian version of the ORTO-15 test has been used.
The Maudsley Obsessive-Compulsive Questionnaire (MOCQ-R)
For the present study we used the Italian revised form of the MOCQ [32], included as Schedule 9 in the Cognitive Behavioral Assessment 2.0 battery [33]. The Maudsley Obsessive-Compulsive Questionnaire was developed by Hodgson and Rachman [34]. The MOCQ-R, resulted from a laborious revision and reduction of the MOCQ English version; it consists of 21 dichotomous items (true–false). Scores can range from 0 to 21, with a high score indicating more obsessive-compulsive tendency. It has three subscales investigating the main characteristics of obsessive-compulsive disorder: checking, cleaning and doubting-ruminating. It represents a reliable and valid tool for detection of obsessive-compulsive traits and characteristic of ON and can be applied for assessing obsessive and compulsive symptoms not only in patients, but also as a screening tool for nonclinical populations [35].
The Eating Attitudes Test-26 (EAT-26)
The EAT-26 [36] is the most common self-report measure of symptoms and concerns characteristic of eating disorders [36]. The scale includes three basic dimensions: dieting, bulimia and food preoccupation, plus oral control. The EAT-26 Italian version [37] has been proved to be more sensitive to the presence of an eating disorder than to a specific clinical entity. Item analysis performed on the EAT-26 variables showed satisfactory reliability coefficients. Factor analysis using an oblique rotation was similar to that obtained by Garner et al. [36]. The authors suggested overall that the EAT-26 isolates cases at risk of clinical spectrum eating disorders. A score of 20 or above on the EAT-26 indicates a high level of concern about dieting, body weight or problematic eating behaviors.
The Body Uneasiness Test (BUT)
The BUT [24] is a valuable multidimensional tool for the clinical assessment of abnormal body image attitudes. A 71-item self-report questionnaire that consists of two parts. (1) BUT-A (34 items) exploring weight phobia, body image concerns, avoidance, compulsive self-monitoring, detachment and estrangement feelings towards one’s own body (depersonalization; examples of items: I avoid mirrors; If I begin to look at myself, I find it difficult to stop). This first part (BUT-A) consists of 34 items whose average total score identifies the degree of severity related to body image (GSI—Global Severity Index). The severity rating is expressed on a scale from 0 to 5, where 0 corresponds to no problems in that area and 5 to maximum severity. The higher the indexes of each group higher then the discomfort.
(2) BUT-B (37 items) investigating specific worries about particular body parts, shapes or functions (examples of items: the shape of my face; buttocks; blushing). This part focuses attention towards a specific part of the body and toward some sensory manifestations (responses) derived from it, such as sweating, reddening, the smell and noise. There are two evaluations resulting from this second part of the questionnaire:-result overall (PST—Positive Symptom Total)-index of discomfort (PSDI—Positive Symptom Distress Index). The severity rating is expressed in this case on a scale of 0 to 37, where 0 corresponds to the absence of the symptom and 37 maximally body discomfort. BUT higher scores indicate greater body uneasiness.
The authors reported a satisfactory internal consistency, highly significant test–retest correlation coefficients and a concurrent validity with other tests (Eating Disorder Inventory, EDI-2; Eating Attitudes Test, EAT-26; Symptom Check List, SCL-90R and Coopersmith Self-Esteem Inventory, SEI).
Design and analysis
This was a cross-sectional study aimed at investigating ORTO-15 scores’ differences between gender and relation with obsessive-compulsive behavior and body image dissatisfaction on a sample of volunteering university students. Data were collected from November 2011 to December 2012. Data were analyzed using SPSS Statistic version 24.0 software (SPSS Inc., Chicago, IL). Descriptive statistics are presented as means, standard deviations (SD) and percentages. An independent t test was used to compare measured variables between males and females. p values less than 0.05 were considered significant. In order to assess the pattern of relationships among ORTO-15, obsessive-compulsive symptoms, eating disorders pathology and body uneasiness, we used two-tailed Pearson’s r correlation coefficient and additionally we regressed each criterion variable on ORTO-15 score in males and females separately in a simple linear regression model.
Results
Sample characteristics
The study sample consisted of 83 females and 37 males (mean age 22.74 ± 7.31 years, age range 19–29); 52 of them were students at the Medical School and 68 at the graduate program in Literature and Philosophy.
No gender related differences were found for age (22.83 ± 8.66 and 22.54 ± 2.42 years, respectively, for female and male students) and body mass index (BMI), calculated with self-reported measures for height and weight. The average BMI was 22.87 kg/m2 (SD 12.42) in female students and 23.87 kg/m2 (SD 3.38) in male ones. In both groups, these mean values indicate normal weight (normal weight ranging from BMI 18.5–24.9 kg/m2).
Gender differences between measured variables
The results in Table 2 show that significant differences between males and females were found only in body image discomfort (weight phobia, body image concerns, avoidance, compulsive self-monitoring, detachment, depersonalization and specific worries about particular body parts or functions). Based on descriptive statistics (Table 2) it can be concluded that female students’ scores were significantly higher both on the BUT-A and BUT-B compared to male students.
We found no significant differences between females and males regarding ORTO-15 and EAT-26 scores.
Relationships between ORTO-15 and measured variables
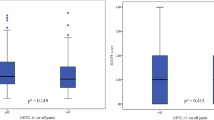
Analyzing the relationship among the ORTO-15 and obsessive-compulsive symptoms (the MOCQ-R), eating disorders pathology (the EAT-26) and body discomfort (the BUT), we observed different patterns in males and females. In female students a statistically significant positive, although weak, correlation was observed between ORTO-15 and body image discomfort (r = 0.39 and r = 0.32; p = 0.001 and p = 0.003) as well as obsessive-compulsive symptoms (r = 0.28; p = 0.12), whereas in male students there was a positive, although weak, relationship between ORTO-15 and disordered eating patterns (r = 0.35; p = 0.39). Results are presented in Table 3.
It is quite noteworthy that the sample means for the EAT-26 were 5.56 and 4.22, respectively, for females and males indicating that the sample was quite “healthy” when considering eating attitude, indeed their mean BMI scores were higher than 22 kg/m2, considered the midpoint of the normal range (M BMI for women = 22.87 kg/m2, M BMI for men = 23.87 kg/m2). It should therefore be acknowledged that this sample, despite their ORTO-15 scores, is to be considered “healthy”; nevertheless, in females, body uneasiness is associated with stronger healthy eating concerns.
Discussion
This study aims at contributing to the literature in the field of ON investigating differences between gender and relation with obsessive-compulsive behavior, disordered eating patterns and body image dissatisfaction in a sample of Italian female and male university students and by examining the predictive model of ORTO-15 in both groups.
Since the real impact of gender-related differences on ON is still unclear, we supposed comparable rates across gender. Healthy eating behavior was observed in both groups. Nonetheless, there was no significant difference between female and male students in ORTO-15 (H1 was confirmed). This would suggest that women and men presented the same attitudes related to the selection, purchase, preparation and consumption of food considered to be healthy. It may also suggest that both females and males have interest on proper nutrition since they worry about their health, physical appearance (drive to thinness in females versus drive to muscularity in males) and weight control (desire of adiposity reduction in females and increase of muscles in males). In our opinion, similarities between female and male university ORTO-15 scores underline the potential need to address these issues in females as well as in males. Nevertheless, comparing females and males in such a homogeneous population (University Students), may hide important characteristics of the differences between genders. This is consistent with ON literature because many university studies often tested ON among non-equivalent groups, in which differences might not have been biased by participants with a particular inclination or interest in health such as dietetics students. On the other hand the concern of healthy eating has increased today both in females and males, due to healthism, related to good health public objectives and health and well-being subjective desire [38]. Our results propose both women and men of our sample embrace health-beliefs and behavior and pursue healthy lifestyle patterns. Our results, however, should be interpreted with caution because of the unequal number of female and male participants (with female predominance). Furthermore, regrettably data about precise number of female and male students in Medicine, Literature and Philosophy were not available.
We found a statistically significant difference between males and females in body uneasiness, with higher scores in the female subgroup, confirming literature data [24] for body dissatisfaction which is more common and more strongly perceived in women [39,40,41,42]. Women are more concerned about their body weight status and this may interfere with the quality of life and even become a predictor of depressed mood independently of body mass index, age and gender [39, 43].
Body dissatisfaction appears to be so prevalent in women that it has been coined “normative discontent” [44], but as recently underlined by others [45] it should be kept distinct from the eating disorders and other adverse psychological phenomena for which body dissatisfaction is commonly discussed as a risk factor. This may be one of the reasons we have not observed differences in ORTO-15 between genders despite a higher body dissatisfaction in females. Nevertheless, it should be noted that mean ORTO-15 scores were very low for both women and men, suggesting that our student population was more likely to engage in extreme dieting practices. According to Dunn and Bratman [23] the ORTO-15 is likely to measure healthy eating, but it is not feasible to more accurately and fully capture pathology.
Interestingly, contrary to our expectations, we found that in the male students group, as the scores on the ORTO-15 decreased (more pathological), the EAT-26 scores indicated healthier eating attitudes (H2 was not confirmed). It may suggest that male students may be more at increased risk for ON than for ED. Our results do not confirm those of other researchers reporting a significant relationship between less orthorexic traits and less level of eating pathology among American students (r = −0.26, p < 0.01) [18] and Turkish students (r = −0.40, p < 0.001) [45]. It is worth pointing out that there is one previous study supporting our results [46], although the authors used the Orthorexia Self-Test, commonly named as the Bratman Orthorexia Test (BOT). The authors report a significant positive correlation between total BOT and EAT-26 scores (r = 0.47, p < 0.01) [46]. Segura-Garcia et al. [21], and Herranz Valera et al. [47] showed an association between ON and its increased prevalence following eating disorders (ED) improvement, besides they indicated that in ED patients the frequency of orthorexic behaviors increases alongside with the decrease of ED pathology [48].
Despite the fact that both groups in our sample had essentially the same mean score on both measures (ORTO-15 test and EAT-26 test), it may seem surprising that the EAT-26 score was correlated with ORTO-15 score for men and not for women. We may hypothesize that contrary to the broader eating disorder literature, in which female prevalence exceeds that of male counterpart, ORTO-15 lower scores in males are more likely associated with eating disordered behavior than to body dissatisfaction, while in females the opposite is true. Therefore, ORTO-15 lower scores could be a better indicator of ED in males than in females. One other factor influencing the outcome is that the actual correlation coefficients are quite weak. Nevertheless, important confounders like culture and educational background may have influenced these results and our interpretation.
In our female sample, as the ORTO-15 score decreased, the compulsive–obsessive symptoms’ scores decreased. This may suggest that ON should not be considered as a subset of obsessive-compulsive disorder. In the American study, Bundros et al. [49] have obtained the same results (r = 0.19, p < 0.01). In contrast with our results, the Turkish study [14] showed that subjects, who displayed pathological eating attitudes (β = −0.25) and symptoms of obsessive-compulsive disorder (β = −0.17), were more likely to display orthorexic behaviors. However, Asil and Saip Sürücüoğlua [50] observed no relationship between obsessive-compulsive disorder and ON among female sample.
In addition, in our female sample, as ORTO-15 score lowered, abnormal body image attitudes, general body/weight dissatisfaction, avoidance and compulsive self-monitoring behavior, feelings of disconnection from one’s own body, and concerns about specific body parts decreased (H3 was not confirmed). This result is consistent with the newly proposed diagnostic criteria [23] that identify ON as an independent pathological entity, in which a relevant clinic aspect is that “weight loss may ensue as a result of dietary choices, but this is not the primary goal”, as stated in criterion A. This characteristic (body image discomfort) could be noteworthy able to differentiate ON from others eating disorders, but further research will be needed to confirm this finding. At present, some studies [9, 26, 50] revealed that there is a correlation between ON and body image concerns in females (in contrast to previous case studies [6, 22, 51,52,53] reporting no body image concerns or issues regarding weight in ON subjects). In addition, one study has shown the positive association between ON (measured by BOT) and body dysmorphic disorder (measured by BDDQ) among college students [49].
At present, atypical EDs represent a concerning health issue being more common in youth [54] and likely to slip into a chronic condition with serious repercussions on the quality of life, nutritional and mental state of the subject. For these reasons, it is important to detect early symptoms that may reliably identify subjects at risk for ON in order to design specific prevention interventions.
Several limitations encountered in the present study should be acknowledged. Firstly, our sample included predominantly female students (69.2% women versus 30.8% men). Secondly this sample cannot be considered representative for all the university students; it would be desirable to replicate and extend the present findings in future. Forthcoming research should include larger sample sizes and simple random sampling across the general population. Besides, the current results are based on self-reporting that could be subject to potential bias. Moreover, the current study was a cross-sectional one and could not assess causality of relationships. Future studies should determine causal relationships between measurable variables. Lastly, the study only used the ORTO-15 test to assess ON. Although, the preliminary validation shows that the test has good predictive validity [27] the internal consistency of the ORTO-15 has been criticized [10] and a low reliability has been ascribed [14, 18]. There are many possible objection on the ORTO-15 test reliability [23, 55], e.g. high prevalence rates of ON among different research populations (which could be explained by the absence of items on disruption in everyday functioning, interpersonal distress, or health problems because of diet), lack of clearly articulated development of construct validity, lack of discussion about the creation of an item pool, lack of standardization methods and lack the basic psychometric properties [23], suggesting caution in the ORTO-15 test use to reliably measure prevalence of ON. Dunn et al. [56] consider that the ORTO-15 likely cannot distinguish between healthy eating and pathologically healthful eating.
Notwithstanding those limitations, we showed that more pathological ORTO-15 scores are associated with less pathological body image discomfort as well as pathological obsessive-compulsive signs among Italian female university students. Whereas, in Italian male students more pathological ORTO-15 lower scores were related to less disordered eating attitudes. On the basis of the present results we recommend considering ON neither obsessive-compulsive disorder nor anorexia nervosa.
At present we cannot argue that ON can be classified as ARFID, since it does not fit into the proposed criteria, but we cannot rule out the possible condition of ON as a fourth variant in the Avoidant/Restrictive Food Intake Disorder (ARFID), according to DSM-5 [7]. The ARFID criteria (aversive experience with food causing food avoidance, highly selective eating habits, and avoidance of food based on its sensory properties) could be broadened to include ON. Nevertheless, we must also consider the possibility that ON might be a variant of anorexia nervosa as claimed by some authoritative authors [9]. There are several hints in current research and literature of a strong overlap between anorexia nervosa and orthorexia, which should be kept in mind while talking about possible nosological classifications, for which it is obviously still necessary to deepen the current knowledge.
Undeniably ON is an emergent disorder that stands out from other eating disorders for lack of concern with body weight and shape. Further studies regarding the relationship between ON and officially recognized eating disorders are needed to better understand the risks associated with healthy eating and/or pathologically healthful eating and ED development.
References
Brytek-Matera A (2012) Orthorexia nervosa—an eating disorder, obsessive-compulsive disorder or disturbed eating habit? Arch Psychiatr Psychother 14(1):55–60
Chaki B, Pal S, Bandyopadhyay A (2013) Exploring scientific legitimacy of orthorexia nervosa: a newly emerging eating disorder. J Hum Sport Exerc 8(4):1045–1053. doi:10.4100/jhse.2013.84.14
World Health Organization (2002) Global strategy on diet, physical activity and health. World Health Organization, Geneva
Bratman S (1997) Health food junkie. Yoga J 136:42–50
Bratman S, Knight D (2000) Health food junkies. Orthorexia nervosa: overcoming the obsession with healthful eating. Broadway Books, New York
Catalina Zamora ML, Bote Bonaechea B, García Sánchez F, Ríos Rial B (2005) Ortorexia nerviosa. ¿Un nuevo trastorno de la conducta alimentaria? Actas Esp Psiquiatr 33(1):66–68
American Psychiatric Association (2013) Diagnostic and statistical manual of mental disorders, 5th edn. American Psychiatric Publishing, Arlington
World Health Organization (2010) International statistical classification of diseases and related health problems, tenth revision. World Health Organization, Geneva
Barthels F, Meyer F, Pietrowsky R (2015) Orthorexic eating behavior. A new type of disordered eating. Ernährungs Umschau 62:156–161
Koven NS, Abry AW (2015) The clinical basis of orthorexia nervosa: emerging perspectives. Neuropsychiatr Dis Treat 11:385–394. doi:10.2147/NDT.S61665
Bartrina JA (2007) Ortorexia o la obsesión por la dieta saludable. Arch Latinoam Nutr 57(4):313–315
Fidan T, Ertekin V, Işikay S, Kirpinar I (2010) Prevalence of orthorexia among medical students in Erzurum, Turkey. Compr Psychiatry 51(1):49–54. doi:10.1016/j.comppsych.2009.03.001
Kummer A, Dias FM, Teixeira AL (2008) On the concept of orthorexia nervosa. Scand J Med Sci Sports 18(3):395–396. doi:10.1111/j.1600-0838.2008.00809.x
Arusoğlu G, Kabakçi E, Köksal G, Merdol TK (2008) Orthorexia nervosa and adaptation of ORTO-11 into Turkish. Turk Psikiyatri Derg 19(3):283–291
Bağci Bosi AT, Camur D, Güler C (2007) Prevalence of orthorexia nervosa in resident medical doctors in the faculty of medicine (Ankara, Turkey). Appetite 49(3):661–766. doi:10.1016/j.appet.2007.04.007
Donini LM, Marsili D, Graziani MP, Imbriale M, Cannella C (2004) Orthorexia nervosa: a preliminary study with a proposal for diagnosis and an attempt to measure the dimension of the phenomenon. Eat Weight Disord 9(2):151–157
Mathieu J (2005) What is orthorexia? J Am Diet Assoc 105(10):1510–1512. doi:10.1016/j.jada2005.08.021
McInerney-Ernst EM (2011) Orthorexia nervosa: real construct or newest social trend? Dissertation, University of Missouri-Kansas City
Kinzl JF, Hauer K, Traweger C, Kiefer I (2006) Orthorexia nervosa in dieticians. Psychother Psychosom 75(6):395–396. doi:10.1159/000095447
Koven NS, Senbonmatsu N (2013) A neuropsychological evaluation of orthorexia nervosa. Open J Psychiatr 3:214–222. doi:10.4236/ojpsych.2013.32019
Segura-Garcia C, Ramacciotti C, Rania M, Aloi M, Caroleo M, Bruni A, Gazzarrini D, Sinopoli F, De Fazio P (2015) The prevalence of orthorexia nervosa among eating disorder patients after treatment. Eat Weight Disord 20(2):161–166. doi:10.1007/s40519-014-0171-y
Moroze RM, Dunn TM, Holland JC, Yager J, Weintraub P (2015) Microthinking about micronutrients: a case of transition from obsessions about healthy eating to near-fatal “orthorexia nervosa” and proposed diagnostic criteria. Psychosomatics 56(4):397–403. doi:10.1016/j.psym.2014.03.003
Dunn TD, Bratman S (2016) On orthorexia nervosa: a review of the literature and proposed diagnostic criteria. Eat Behav 21:11–17. doi:10.1016/j.eatbeh.2015.12.006
Cuzzolaro M, Vetrone G, Marano G, Garfinkel PE (2006) The Body Uneasiness Test (BUT): development and validation of a new body image assessment scale. Eat Weight Disord 11(1):1–13
Varga M, Máté G (2009) Eating disturbances in orthorexia nervosa. XIII annual meeting of the European Association for Consultation-Liaison Psychiatry and Psychosomatics (EACLPP) XXVIII European Conference on Psychosomatic Research (ECPR): a selection of the best abstracts submitted. J Psychosom Res 68:672–673
Brytek-Matera A, Donini LM, Krupa M, Poggiogalle E, Hay P (2016) Erratum to: Orthorexia nervosa and self-attitudinal aspects of body image in female and male university students. J Eat Disord 4:16. doi:10.1186/s40337-016-0105-3
Donini LM, Marsili D, Graziani MP, Imbriale M, Cannella C (2005) Orthorexia nervosa: validation of a diagnosis questionnaire. Eat Weight Disord 10:e28–e32
Brytek-Matera A, Krupa M, Poggiogalle E, Donini LM (2014) Adaptation of the ORTHO-15 test to Polish women and men. Eat Weight Disord 19(1):69–76. doi:10.1007/s40519-014-0100-0
Tremelling K, Sandon L, Vega GL, McAdams CJ (2017) Orthorexia nervosa and eating disorder symptoms in registered dietitian nutritionists in the United States. J Acad Nutr Diet S2212–2672(17):30448–30453. doi:10.1016/j.jand.2017.05.001
Ramacciotti CE, Perrone P, Coli E, Burgalassi A, Conversano C, Massimetti G, Dell’Osso L (2011) Orthorexia nervosa in the general population: a preliminary screening using a self-administered questionnaire (ORTO-15). Eat Weight Disord 16(2):e127–e130. doi:10.1007/BF03325318
Dell’Osso L, Abelli M, Carpita B, Pini S, Castellini G, Carmassi C, Ricca V (2016) Historical evolution of the concept of anorexia nervosa and relationships with orthorexia nervosa, autism, and obsessive–compulsive spectrum. Neuropsychiatr Dis Treat 12:1651–1660. doi:10.2147/NDT.S108912
Sanavio E, Vidotto G (1985) The components of the Maudsley Obsessional-Compulsive Questionnaire. Behav Res Ther 23(6):659–662. doi:10.1016/0005-7967(85)90061-0
Bertolotti G, Zotti AM, Michielin P, Vidotto G, Sanavio E (1990) A computerized approach to cognitive behavioral assessment: an introduction to CBA-2.0 primary scales. J Behav Ther Exp Psychiatry 21(1):21–27. doi:10.1016/0005-7916(90)90045-M
Hodgson RJ, Rachman S (1977) Obsessional-compulsive complaints. Behav Res Ther 15(5):389–395. doi:10.1016/0005-7967(77)90042-0
Einstein D, Menzies R (2006) Magical thinking in obsessive-compulsive disorder, panic disorder and the general community. Behav Cogn Psychother 34(3):351–357. doi:10.1017/S1352465806002864
Garner DM, Olmsted MP, Bohr Y, Garfinkel PE (1982) The Eating Attitudes Test: psychometric features and clinical correlates. Psychol Med 12(4):871–878
Dotti A, Lazzari R (1998) Validation and reliability of the Italian EAT-26. Eat Weight Disord 3(4):188–194
Rose N (1999) Powers of freedom: reframing political thought. Cambridge University Press, Cambridge
Runfola CD, Von Holle A, Trace SE, Brownley KA, Hofmeier SM, Gagne DA, Bulik CM (2013) Body dissatisfaction in women across the lifespan: results of the UNC-SELF and Gender and Body Image (GABI) studies. Eur Eat Disord Rev 21(1):52–59. doi:10.1002/erv.2201
Carvalheira A, Godinho L, Costa P (2017) The impact of body dissatisfaction on distressing sexual difficulties among men and women: the mediator role of cognitive distraction. J Sex Res 54(3):331–340. doi:10.1080/00224499.2016.1168771
Karazsia BT, Murnen SK, Tylka TL (2017) Is body dissatisfaction changing across time? A cross-temporal meta-analysis. Psychol Bull 143(3):293–320. doi:10.1037/bul0000081
del Mar Bibiloni M, Coll JLI, Pich J, Pons A, Tur JA (2017) Body image satisfaction and weight concerns among a Mediterranean adult population. BMC Public Health 17(1):39. doi:10.1186/s12889-016-3919-7
Richard A, Rohrmann S, Lohse T, Eichholzer M (2016) Is body weight dissatisfaction a predictor of depression independent of body mass index, sex and age? Results of a cross-sectional study. BMC Public Health 16(1):863. doi:10.1186/s12889-016-3497-8
Rodin J, Silberstein L, Striegel-Moore R (1984) Women and weight: a normative discontent. Neb Symp Motiv 32:267–307
Griffiths S, Hay P, Mitchison D, Mond JM, McLean SA, Rodgers B, Massey R, Paxton SJ (2016) Sex differences in the relationships between body dissatisfaction, quality of life and psychological distress. Aust N Z J Public Health 40(6):518–522. doi:10.1111/1753-6405.12538
Sanlier N, Yassibas E, Bilici S, Sahin G, Celik B (2016) Does the rise in eating disorders lead to increasing risk of orthorexia nervosa? Correlations with gender, education, and body mass index. Ecol Food Nutr 55(3):266–278. doi:10.1080/03670244.2016
Herranz Valera J, Acuña Ruiz P, Romero Valdespino B, Visioli F (2014) Prevalence of orthorexia nervosa among ashtanga yoga practitioners: a pilot study. Eat Weight Disord 19:469–472. doi:10.1007/s40519-014-0131-6
Brytek-Matera A, Rogoza R, Gramaglia C, Zeppegno P (2015) Predictors of orthorexic behaviours in patients with eating disorders: a preliminary study. BMC Psychiatry 15(1):252. doi:10.1186/s12888-015-0628-1
Bundros J, Clifford D, Silliman K, Neyman Morris M (2016) Prevalence of Orthorexia nervosa among college students based on Bratman’s test and associated tendencies. Appetite 101:86–94. doi:10.1016/j.appet.2016.02.144
Asil E, Saip Sürücüoğlu M (2015) Orthorexia nervosa in Turkish dietitians. Ecol Food Nutr 54(4):303–313. doi:10.1080/03670244.2014.987920
Park SW, Kim JY, Go GJ, Jeon ES, Pyo HJ, Kwon YJ (2011) Orthorexia nervosa with hyponatremia, subcutaneous emphysema, pneumomediastinum, pneumothorax, and pancytopenia. Electrolyte Blood Press 9(1):32–37. doi:10.5049/EBP.2011.9.1.32
Saddichha S, Babu GN, Chandra P (2012) Orthorexia nervosa presenting as prodrome of schizophrenia. Schizophr Res 134(1):110. doi:10.1016/j.schres.2011.10.017
Barnes MA, Caltabiano ML (2016) The interrelationship between orthorexia nervosa, perfectionism, body image and attachment style. Eat Weight Disord 22(1):177–184. doi:10.1007/s40519-016-0280-x
National Collaborating Centre for Mental Health (2004) Eating disorders. Core interventions in the treatment and management of anorexia nervosa, bulimia nervosa and related eating disorders. NICE Clinical Guidelines, No. 9. British Psychological Society, Leicester
Missbach B, Hinterbuchinger B, Dreiseitl V, Zellhofer S, Kurz C, König J (2015) When eating right, is measured wrong! A validation and critical examination of the ORTO-15 Questionnaire in German. PLoS One 10(8):e0135772. doi:10.1371/journal.pone.0135772
Dunn TM, Gibbs J, Whitney N, Starosta A (2017) Prevalence of orthorexia nervosa is less than 1%: data from a US sample. Eat Weight Disord 22:185–192. doi:10.1007/s40519-016-0258-8
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Ethical approval
Institutional Review Board (IRB) approval was obtained per institutional guidelines. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
This article is part of the topical collection on Orthorexia nervosa.
Rights and permissions
About this article

Cite this article
Brytek-Matera, A., Fonte, M.L., Poggiogalle, E. et al. Orthorexia nervosa: relationship with obsessive-compulsive symptoms, disordered eating patterns and body uneasiness among Italian university students. Eat Weight Disord 22, 609–617 (2017). https://doi.org/10.1007/s40519-017-0427-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40519-017-0427-4