
Abstract
Purpose
Theory suggests that binge eating symptoms may develop in an attempt to avoid distressing states that arise in the context of negative affect. In light of its theoretical significance, including the “escape from awareness” model of binge eating, surprisingly few empirical evaluations have examined the empirical evidence for this variable in relation to anxiety and binge eating symptoms. In addition, although it is understood that anxiety is more prevalent among women than men, empirical investigations of gender differences in cognitive avoidance in binge eating are thus far absent from the published literature.
Methods
Participants (N = 436) were recruited from diverse geographic regions across the United States to take part in an online study. Cognitive avoidance, anxiety, and binge eating measures were collected.
Results
Cognitive avoidance partially mediated the relation between anxiety and binge eating in the full sample; however, results differed across genders. Specifically, cognitive avoidance was a mediator for women, but not for men.
Conclusions
Findings support the “escape from awareness” model of binge eating among women, and suggest that targeting cognitive avoidance in binge eating treatment may be a promising clinical avenue. Future research may benefit from exploring the broader construct of experiential avoidance to determine if the gender differences in cognitive avoidance observed in this study are indicative of a larger pattern of avoidance behavior, and if factors other than cognitive avoidance may have greater relevance for men.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Does cognitive avoidance mediate the relation of anxiety and binge eating
Binge eating is a prevalent and impairing condition marked by psychological distress [1]. Now recognized within the DSM-5 as a psychological disorder, binge eating disorder (BED) is defined as consuming a larger than average amount of food while experiencing a loss of control, along with three or more of the following associated features: eating until uncomfortably full, eating much more rapidly than normal, consuming large amounts of food in the absence of physical hunger, eating alone due to embarrassment over the amount eaten, feeling disgusted, depressed, or guilty afterward [2]. Although BED may be more common among women, binge eating is the most prevalent form of eating disturbance among men [1]. In addition to full BED, subclinical binge eating is also associated with a host of impairments, including psychological dysfunction [3–5], and may occur at higher rates among men than women [6]. Therefore, dimensional examinations of binge eating symptoms may be an important component to better understand factors that may impact the development and maintenance of binge eating across genders.
Theoretical models of binge eating help to contextualize the symptoms of this deleterious behavior and its correlates. Cognitive avoidance theory posits that distressing emotional states, such as anxiety, creates vulnerability for binge eating, and that binge eating serves as a process through which the salience of negative thoughts is mitigated. In turn, the avoidance of negative thoughts also limits the salience of negative emotions [7], with binge eating functioning as an anxiety reduction strategy [8]. Heatherton and Baumeister coined the phrase “escape from awareness,” [7] to describe the process through which binge eating reduces the salience of negative emotions. They described that cognitive narrowing, a state in which thinking and interaction with the environment occur on a more basic level, is achieved for individuals during in binge eating. For example, thoughts are limited in scope to the direct experiences of binge eating (e.g., sensory experiences) rather than more abstract concepts and beliefs (e.g., self-concept). As such, this theory suggests that because the scope of awareness is limited, the adverse consequences of binge eating are not salient during the act itself [7]. There is some support in the literature thus far for binge eating functioning, in part, as an attempt to reduce negative emotions through cognitive avoidance. Negative affect has been identified as a trigger of binge eating episodes [9, 10], and binge eating has been shown to serve the function of coping with negative affect in empirical evaluations of the “escape from awareness” model [11]. Additionally, there is evidence that reductions in binge eating may occur for individuals following participation in programs to reduce experiential avoidance [12], and that suppression of thoughts related to food (e.g., strong agreement with statements such as “there are foods that I try not to think about” and “I always try to put eating problems out of my mind”) is associated with higher levels of disordered eating pathology among individuals seeking treatment for BED [13]. Empirical evidence supports the notion that binge eating provides relief from negative affect, on at least a temporary, momentary level [14].
To better understand the process through which binge eating may occur, it is also important to consider the particular components of negative affect that could prompt the perceived need for avoidance. The literature has demonstrated an association between high levels of anxiety symptoms and binge eating symptoms [15, 16]. Additionally, previous research has found that anxiety is uniquely important, after considering other components of negative affect, in understanding the severity of binge eating symptoms [6]. This is supported by evidence that binge eating is associated with a reduction in anxiety [17], particularly among individuals with BED [18]. Despite the promising developments in the literature thus far, to our knowledge, there have not been empirical evaluations that have examined cognitive avoidance as a mediator in the relation between the anxiety and binge eating symptoms.
There is reason to suspect that anxiety and cognitive avoidance may have differential relations to binge eating symptoms between women and men. It is well established in the literature that anxiety is more prevalent among women [19], and as previously mentioned, BED rates are higher among women than men [1]; therefore, it may be the case that cognitive avoidance is more salient in the context of anxiety and BED for women as well. While there are few investigations of gender differences of cognitive avoidance in the weight and eating literature, at least one study has found that suppression of food-related thoughts mediates the relation between stress and weight cycling for women, but not for men [20]. In sum, examination of gender differences in the relation of cognitive avoidance, anxiety, and binge eating is a meaningful, yet underexplored area of the literature.
The primary aim of this study was to empirically examine the role of cognitive avoidance as the pathway through which anxiety relates to binge eating symptoms, consistent with the “escape from awareness” model [7]. This study is novel in that it was the first, to our knowledge, to examine the role of cognitive avoidance as a mediator of the relation between anxiety and binge eating symptoms for women and men. We hypothesized that (1) cognitive avoidance would be significantly positively related to binge eating symptoms, and (2) the relation between anxiety and binge eating symptoms would be mediated by cognitive avoidance. We also conducted analyses to determine whether the effect of cognitive avoidance would differ by gender in subsamples of men and women.
Methods
Participants and measures
Participants (N = 436; 62 % female) were recruited nation-wide across the United States, and ranged from 18 to 72 years old (M = 33.4, SD = 13.5). Individuals with psychosis (e.g., self-reported schizophrenia) were excluded. Responses from participants were excluded if they were determined to be invalid or random per validity screening questions.
Assessment included self-reported demographic variables and questionnaires pertaining to anxiety, cognitive avoidance, and binge eating. Anxiety was measured using the depression anxiety stress scales [21]. The DASS is a 21-item self-report questionnaire with a 7-item subscale measuring anxiety. The Likert-type scale is scored such that higher values indicate greater anxiety. Psychometrics for the anxiety subscale are strong [22], including test–retest reliability (r = 0.79 [21, 23]), concurrent validity with the Beck Anxiety Inventory (r = 0.84 [24]) and internal consistency (α = 0.82 in the current sample).
Cognitive avoidance was measured using the 15-item white bear suppression inventory (WBSI) [25]. Item-level scores range from 1 (strongly agree) to 5 (strongly disagree), with items including statements such as “There are things I prefer not to think about.” Good internal consistency (0.87–0.89) and test–retest reliability (0.69–0.92) have been shown in previous samples [25], and internal consistency (α = 0.95) was strong for the current sample.
Binge eating symptoms were measured using the 22-item eating disorder diagnostic scale (EDDS) [26]. This measure has demonstrated good psychometrics with both men and women [26–28]. For this study, the symptom composite of the EDDS was used as it allows for dimensional interpretation of symptoms rather than dichotomous categorization of symptoms [29]. Higher symptom composite scores indicate greater pathology.
Test–retest reliability (r = 0.87), internal consistency (Cronbach’s α = 0.89), and convergent validity have been established for the symptom composite [26]. Consistent with the previous literature [28], a binge eating-specific symptom composite was computed for this study. Internal consistency analyses from previous research [28] (α = 0.84) and the current sample consistency (α = 0.76) indicate adequate reliability for the binge eating-specific symptom composite.
Procedure
The Institutional Review Board at The University of Missouri–St. Louis approved this research. Because we were interested in examining binge eating across a spectrum of severity, a broad-based community sample was targeted. Recruitment occurred through postings to online community sites (e.g., “volunteers” section of Craigslist.org), not targeted toward overweight, obese or eating disordered populations. An example of one of our ads reads as follows: “Please consider visiting the site below to take part in an online study of eating patterns and feelings.” Questionnaires were administered through a secure website accessed by an encrypted link that allowed the data to be collected anonymously. An opportunity to be included in a raffle drawing for one of seven $100 gift cards was provided as incentive for providing data. Participants were asked to complete the questionnaire battery one time only.
Analytic plan
Data were analyzed using SPSS [30]. Participants who responded incorrectly to more than one random response pattern detection item were excluded from analyses. Data were also excluded from two individuals following a review of outliers due to the likelihood of an invalid response pattern. Mean imputation was performed for questionnaires that were at least 80 % complete.
Results
Descriptive analyses
Approximately 62 % of participants were women, 38 % were men, and three individuals (<1 % of sample) identified as transgendered. Over half (54 %) of the sample worked full-time or part-time, 20 % were full-time undergraduate or graduate students, and 25 % were unemployed, full-time homemakers, on disability, or retired. Participants’ age ranged from 18 to 72 years (M = 33.4, SD = 13.5). Race and ethnicity are as follows: 64.7 % White, 15.1 % African American/Black, 7.4 % Asian American, 6.5 % Hispanic/Latino, 4.9 % Biracial or Multiracial, 1.2 % American Indian/Alaska Native, 0.2 % Native Hawaiian/Pacific Islander. Participants’ average BMI was 27.5 kg/m2 (SD = 7.7), and ranged from 16.46 to 68.41 kg/m2, based upon self-reported weight and height. Although the full sample included 436 participants, 261 participants provided analyzable data for all of the measures of interest.
Women had significantly higher anxiety (M = 8.79, SD = 8.56), and binge eating symptoms (M = 8.33, SD = 5.78), than men (M = 6.64, SD = 7.58; M = 7.02, SD = 5.59, respectively), although overall anxiety was in the mild range. We also found that cognitive avoidance was also significantly greater among women (t=-3.43, p < 0.01, M = 50.06, SD = 15.06) than men (M = 42.62, SD = 17.56). The cognitive avoidance reported in this sample was similar to levels reported among a normative comparison group of undergraduates (M men = 43.4, M women = 47.6, SD = 10.18) [25]. Approximately 6.8 % of participants who responded to the EDDS reported symptoms of binge eating that were consistent with DSM-IV-TR diagnostic criteria for BED, and approximately 6.5 % endorsed symptoms at a subclinical level.
Primary analyses
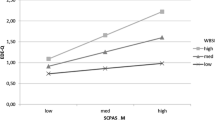
Cognitive avoidance was significantly positively correlated with binge eating symptoms (r = 0.30, p = 0.000) and anxiety (r = 0.46, p = 0.000), with correlation coefficients consistent with medium effect size. Mediation analyses were performed using Hayes’ Process Macro [31]. The overall model was significant F (1262) = 17.43, p < 0.001. Anxiety was significantly associated with cognitive avoidance (B = 1.82, SE = 0.23, p < 0.001). Cognitive avoidance was significantly associated with binge eating symptoms (B = 0.07, SE = 0.02, p < 0.01). The total effect of anxiety on binge eating symptoms was significant (B = 0.44, SE = 0.11, p < 0.001), and there was a significant direct effect of anxiety on binge eating (B = 0.32, SE = 0.12, p < 0.01). The indirect effect was tested using bootstrapping with 5000 resamples. There was a significant indirect effect via cognitive avoidance (B = 0.12, SE = 0.05, 95 % CI 0.03–0.22), with evidence of mediation from a significant Sobel test (test statistic = 2.24, p = 0.03). Cognitive avoidance partially mediated the relation of anxiety and binge eating symptoms.
A set of secondary analyses was conducted to contextualize and better understand the possibility of a gender effect on these results and study variables. The mediation analysis was performed separately for men and women to examine the possibility of a gender effect. For the subsample of men (n = 89), the overall model was significant F (1, 87) = 21.60, p < 0.001. Anxiety was significantly associated with cognitive avoidance (B = 2.14, SE = 0.46, p < 0.001); however, cognitive avoidance was not significantly associated with binge eating symptoms (B = −0.004, SE = 0.04, p = 0.92). The confidence interval for the indirect effect (B = −0.01, SE = 0.02, 95 % CI −0.03 to 0. 03) crossed zero, indicating that there was not a significant result for this analysis. There was no support for mediation for the subsample of men.
For the subsample of women (n = 172), a robust mediation effect was observed. The overall model was significant F(1, 170) = 34.88, p < 0.001. Anxiety was significantly associated with cognitive avoidance (B = 1.58, SE = 0.27, p < 0.001). Cognitive avoidance was significantly associated with binge eating symptoms (B = 0.11, SE = 0.03, p < 0.001). The total effect of anxiety on binge eating symptoms was significant (B = 0.30, SE = 0.13, p = 0.03); however, there was not a significant direct of anxiety on binge eating (B = 0.13, SE = 0.15, p = 0.37). The indirect effect was tested using bootstrapping with 5000 resamples. There was a significant indirect effect via cognitive avoidance (B = 0.16, SE = 0.06, 95 % CI 0.07–0.31), and a significant Sobel test (test statistic = 3.14, p = 0.002). These analyses supported full mediation.
Discussion
Our study evaluated whether avoidance of distressing thoughts mediated the relation between anxiety and binge eating symptoms, consistent with the escape from awareness model of binge eating [7]. Moreover, we aimed to evaluate whether the importance of cognitive avoidance, in relation to anxiety and binge eating symptoms, differs for men and women.
Consistent with previous empirical evidence that supports the conceptualization of binge eating as a method of coping with negative emotional states [32–34]; our study found that for the sample overall, there was both a direct effect of anxiety and an indirect effect of cognitive avoidance, supporting an interpretation of partial mediation. The results from this study are novel, given that to date, many of the studies supporting this theory have extrapolated support for the role of avoidance in their examination of negative emotionality and binge eating behavior [10, 27, 35, 36]; direct tests of the association of cognitive avoidance and binge eating have been less common [37, 38].
Our finding supports a cognitive avoidance model of binge eating [7], and suggests that binge eating may be more likely to occur in as part of a maladaptive coping process when individuals are faced with distressing thoughts. Further, if the above-mentioned process is in fact occurring, this suggests that individuals may have difficulty appreciating the negative proximal and distal consequences of this behavior as they are focused on the perceived positive consequences of binge eating (i.e., temporary blunting of anxiety).
The current study furthers the understanding of the role of cognitive avoidance in the relation of anxiety and binge eating in the context of BED. Although the association between anxiety, cognitive avoidance, and binge eating has been previously studied, these evaluations have not occurred within the context of BED [39, 40]. Our data also extend these findings to a broader clinical context of individuals with subclinical binge eating disorder symptoms, and may be more generalizable than previous studies given that we utilized a diverse community-based sample.
This study examined the novel question of whether an individual’s gender impacted the relations between their emotional experiences and binge eating. Our results showed men and women differed in their degree of cognitive avoidance—and, for men and women, cognitive avoidance functioned differently in the anxiety–binge eating relationship. This study was also the first of which we are aware to explore gender effects to further the understanding of the relation of cognitive avoidance, anxiety, and binge eating behavior. We conducted separate analyses for men and women, given that women reported higher levels of cognitive avoidance than men, and found evidence that the role of cognitive avoidance differed by gender in relation to anxiety and binge eating. Specifically, cognitive avoidance completely mediated the relation between anxiety and binge eating for women, but was not significantly associated with binge eating for men. The results found in the overall sample should be interpreted in light of the differing follow-up analyses by gender.
There are several potential factors that may help to understand why cognitive avoidance was shown to be a mediator of the relation of anxiety and binge eating for women, but not for men. First, women may be more likely to experience a perceived need to push away uncomfortable thoughts due to a greater exposure to stressors, including gender-salient stressors such as sexual harassment, assault and discrimination. Similarly, men may have fewer anxious thoughts given the higher rates of anxiety disorders among women than men [41]. Second, women may be more likely to endorse cognitive avoidance although the true level of this construct may be similar across genders. Third, men may be more likely to engage in another form of experiential avoidance that we did not evaluate in the current study. For instance, they may have responded differently to items assessing avoidance of emotions rather than avoidance of thoughts. Finally, it may be possible that using an experimental technique to evaluate avoidance may have yielded different results than self-report, particularly given social norms emphasizing masculinity among men and the impact this may have on endorsement of psychological concerns [42].
There are some limitations of this study. The study design precludes causal conclusions among the study variables, and future work will be required to draw temporal conclusions among these constructs. These data were collected among a community-based sample and, therefore, may not fully generalize to clinical populations. The results found within this study warrant replication and extension in other samples, in particular, in patients with clinician-diagnosed disorders. Future research employing a longitudinal and experimental design may yield additional understanding of the relation among the factors we examined. As previously mentioned, our measures focused on one domain of psychological avoidance, specifically, cognitive avoidance. It may be possible that a broader assessment of experiential avoidance may yield different results.
While this study provides some empirical evidence to support the “escape from awareness” model, continued investigation of the process through which facets of negative affect trigger binge eating episodes is needed. Some have suggested that a dual pathway model, which posits negative affect and dietary restraint may serve as precipitants to binge eating episodes, may better explain the link between binge eating episodes and triggers such as body dissatisfaction [43]. One potential avenue to increase understanding of the moment-to-moment changes in affect and psychological processes that occur before, during, and after binge eating episodes is increased use of ecological momentary assessment and objective measurements collected through laboratory studies. While outside the scope of this national community-based study, future research utilizing these tools may provide compelling evidence to inform conceptual models of binge eating and potentially improve clinical interventions. Additionally, future study examining the differences between men and women regarding the function of binge eating and cognitive avoidance is needed.
This study has several clinical implications. Although we focused on binge eating symptoms through the lens of BED, the current study utilized dimensional measurement that included individuals at varying levels of clinical severity. As such, the results found in this study have relevance for newer clinical research perspectives that embrace the full range of functioning and behavior and minimize reliance on diagnostic cut points, such as transdiagnostic models and the NIMH Research Domain Criteria Initiative. Our finding that cognitive avoidance may be a more important factor for women than men suggests that interventions that utilize mindfulness and address avoidance of internal experiences, such as Dialectical Behavior Therapy and acceptance-based treatments, may be particularly useful for women with binge eating concerns. There is some empirical support for mindfulness as an effective strategy for reducing binge eating symptoms, as highlighted by studies that have found mindfulness training is associated with a decrease in binge eating episodes [44–46]. Our data also suggest that mindfulness and acceptance-based intervention strategies may potentially have less utility for men, and men may have differential responses to other treatment modalities. Alternatively, it may be important to consider individualized treatment matching or tailoring for men and women with binge eating concerns depending on the importance of cognitive avoidance in their presentations.
In conclusion, this study supports the importance of cognitive avoidance as a mediating factor in the relation between anxiety and binge eating symptoms, particularly among women. Additional research is needed to further explore gender differences in conceptual models of binge eating, including the “escape from awareness” model [7] and whether these gender differences indicate different treatment approaches for men and women.
References
Hudson JI, Hiripi E, Pope HG Jr, Kessler RC (2007) The prevalence and correlates of eating disorders in the national comorbidity survey replication. Biol Psychiatry 61(3):348–358. doi:10.1016/j.biopsych.2006.03.040
American Psychiatric Association (2013) Diagnostic and statistical manual of mental disorders, fifth edition (DSM-5). American Psychiatric Association, Arlington
Striegel-Moore RH, Wilfley D, Pike KM, Dohm F, Fairburn CG (2000) Recurrent binge eating in black american women. Arch Fam Med 9:83–87. doi:10.1001/archfami.9.1.83
Javaras KN, Pope HG Jr, Lalonde JK, Roberts JL, Nillni YI, Laird NM, Bulik CM, Crow SJ, McElroy SL, Walsh BT, Tsuang MT, Rosenthal NR, Hudson JI (2008) Co-occurrence of binge eating disorder with psychiatric and medical disorders. J Clin Psychiatry 69:266–273
Reichborn-Kjennerud T, Bulik CM, Sullivan PF, Tambs K, Harris JR (2004) Psychiatric and medical symptoms in binge eating in the absence of compensatory behaviors. Obes Res 12(9):1445–1454. doi:10.1038/oby.2004.181
Rosenbaum DL, White KS (2015) The relation of anxiety, depression, and stress to binge eating behavior. J Health Psychology 20(6):887–898. doi:10.1177/1359105315580212
Heatherton TF, Baumeister RF (1991) Binge eating as escape from self-awareness. Psychol Bull 110:86–108. doi:10.1037//0033-2909.110.1.86
Pallister E, Waller G (2008) Anxiety in the eating disorders: understanding the overlap. Clin Psychol Rev 28:366–386. doi:10.1016/j.cpr.2007.07.001
Napolitano MA, Himes S (2011) Race, weight, and correlates of binge eating in female college students. Eat Behav 12:29–36. doi:10.1016/j.eatbeh.2010.09.003
Stein RI, Kenardy J, Wiseman CV, Dounchis JZ, Arnow BA, Wilfley DE (2007) What’s driving the binge in binge eating disorder?:a prospective examination of precursors and consequences. Int J Eat Disord 40:195–203. doi:10.1002/eat.20352
Engelberg MJ, Steiger H, Gauvin L, Wonderlich SA (2007) Binge antecedents in bulimic syndromes: an examination of dissociation and negative affect. Int J Eat Disord 40(6):531–536. doi:10.1002/eat.20399
Lillis J, Hayes SC, Levin ME (2011) Binge eating and weight control: the role of experiential avoidance. Behav Modif 35(3):252–264. doi:10.1177/0145445510397178
Barnes RD, Masheb RM, White MA, Grilo CM (2013) Examining the relationship between food thought suppression and binge eating disorder. Compr Psychiatry 54(7):1077–1081. doi:10.1016/j.comppsych.2013.04.017
Deaver CM, Miltenberger RG, Smyth J, Meidinger A, Crosby R (2003) An evaluation of affect and binge eating. Behav Modif 27(4):578–599. doi:10.1177/0145445503255571
Mussell MP, Mitchell JE, De Zwaan M, Crosby RD, Seim HC, Crow SJ (1996) Clinical characteristics associated with binge eating in obese females: a descriptive study. Int J Obes 20(4):324–331
Yanovski SZ, Nelson JE, Dubbert BK, Spitzer RL (1993) Association of binge eating disorder and psychiatric comorbidity in obese subjects. Am J Psychiatry 150(10):1472–1479
Fairburn CG, Cooper Z, Cooper PJ (1986) The clinical features and maintenance of bulimia nervosa. In: Brownell KD, Foreyt JP (eds) Handbook of eating disorders: physiology, psychology and treatment of obesity, anorexia and bulimia. Basic Books, New York, pp 389–404
Mitchell JE, Mussell MP, Peterson CB, Crow S, Wonderlich SA, Crosby RD, Davis T, Weller C (1999) Hedonics of binge eating in women with bulimia nervosa and binge eating disorder. Int J Eat Disord 26:165–170. doi:10.1002/(SICI)1098-108X(199909)26:2<165:AID-EAT5>3.3.CO;2-8
Kessler RC, Berglund PA, Demler O, Jin R, Walters EE (2005) Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication (NCS-R). Arch Gen Psychiatry 62(6):593–602
Barnes RD, Tantleff-Dunn S (2010) Food for thought: examining the relationship between food thought suppression and weight-related outcomes. Eat Behav 11:175–179
Lovibond PF, Lovibond SH (1995) Manual for the depression anxiety stress scales. Psychology Foundation of Australia, Sydney
McDowell I (2006) Measuring health: a guide to rating scales and questionnaires, 3rd edn. Oxford University Press, New York
Henry JD, Crawford JR (2005) The short-form version of the depression anxiety stress scales (DASS-21): construct validity and normative data in a large non-clinical sample. Br J Clin Psychol 44:227–239. doi:10.1348/014466505X29657
Antony MM, Bieling PJ, Cox BJ, Enns MW, Swinson RP (1998) Psychometric properties of the 42-item and 21-item versions of the depression anxiety stress scales in clinical groups and a community sample. Psychol Assess 10:176–181
Wegner DM, Zanakos S (1994) Chronic thought suppression. J Pers 62:615–640
Stice E, Telch CF, Rizvi SL (2000) Development and validation of the eating disorder diagnostic scale: a brief self-report measure of anorexia, bulimia, and binge-eating disorder. Psychol Assess 12:123–131. doi:10.1037//1040-3590.12.2.123
Whiteside U, Chen E, Neighbors C, Hunter D, Lo T, Larimer M (2007) Difficulties regulating emotions: do binge eaters have fewer strategies to modulate and tolerate negative affect? Eat Behav 8(2):162–169. doi:10.1016/j.eatbeh.2006.04.001
Dunn EC, Neighbors C, Larimer M (2003) Assessing readiness to change binge eating and compensatory behaviors. Eat Behav 4(3):305–314. doi:10.1016/S1471-0153(03)00023-0
Stice E, Fisher M, Martinez E (2004) Eating disorder diagnostic scale: additional evidence of reliability and validity. Psychol Assess 16(1):60–71. doi:10.1037/1040-3590.16.1.60
IBM Corp. (2012) IBM SPSS Statistics for Windows, Version 21.0. IBM Corp., Armonk, NY
Hayes AF (2013) Introduction to mediation, moderation and conditional process analysis. Guilford Press, New York
Binford RB, Mussell MP, Peterson CB, Crow SJ, Mitchell JE (2004) Relation of binge eating age of onset to functional aspects of binge eating in binge eating disorder. Int J Eat Disord 35:286–292. doi:10.1002/eat.10272
Sierra-Baigrie S, Lemos-Giráldez S, Paino M, Fonseca-Pedrero E (2012) Exploring the relationship between coping strategies and binge eating in nonclinical adolescents. Eur Eat Disord Rev 20(1):e63–e69
Sulkowski ML, Dempsey J, Dempsey AG (2011) Effects of stress and coping on binge eating in female college students. Eat Behav 12(3):188–191. doi:10.1016/j.eatbeh.2011.04.006
Stickney MI, Miltenberger RG, Wolff G (1999) A descriptive analysis of factors contributing to binge eating. J Behav Ther Exp Psychiatry 30(3):177–189. doi:10.1016/S0005-7916(99)00019-1
Kaye WH, Gwirtsman HE, George DT, Weiss SR, Jimerson DC (1986) Relationship of mood alterations to bingeing behaviour in bulimia. Br J Psychiatry 149(4):479–485. doi:10.1192/bjp.149.4.479
Blackburn S, Johnston L, Blampied N, Popp D, Kallen R (2006) An application of escape theory to binge eating. Eur Eat Disord Rev 14(1):23–31. doi:10.1002/erv.675
Paxton SJ, Diggens J (1997) Avoidance coping, binge eating, and depression: an examination of the escape theory of binge eating. Int J Eat Disord 22(1):83–87
Lingswiler VM, Crowther JH, Stephens MAP (1989) Affective and cognitive antecedents to eating episodes in bulimia and binge eating. Int J Eat Disord 8:533–539. doi:10.1002/1098-108X(198909)8:5<533:AID-EAT2260080505>3.0.CO;2-O
Meyer C, Serpell L, Waller G, Murphy F, Treasure J, Leung N (2005) Cognitive avoidance in the strategic processing of ego threats among eating-disordered patients. Int J Eat Disord 38(1):30–36. doi:10.1002/eat.20147
McLean CP, Asnaani A, Litz BT, Hofmann SG (2011) Gender differences in anxiety disorders: prevalence, course of illness, comorbidity and burden of illness. J Psychiatr Res 45(8):1027–1035. doi:10.1016/j.jpsychires.2011.03.006
Addis ME, Cohane GH (2005) Social scientific paradigms of masculinity and their implications for research and practice in men’s mental health. J Clin Psychol 61(6):633–647. doi:10.1002/jclp.20099
Holmes M, Fuller-Tyszkiewicz M, Skouteris H, Broadbent J (2015) Understanding the link between body image and binge eating: a model comparison approach. Eat weight disord EWD 20(1):81–89. doi:10.1007/s40519-014-0141-4
Kristeller JL, Wolever RQ (2011) Mindfulness-based eating awareness training for treating binge eating disorder: the conceptual foundation. Eat Disord 19(1):49–61
Courbasson CM, Nishikawa Y, Shapira LB (2011) Mindfulness-action based cognitive behavioral therapy for concurrent binge eating disorder and substance use disorders. Eat Disord 19(1):17–33
Dalen J, Smith BW, Shelley BM, Sloan AL, Leahigh L, Begay D (2010) Pilot study: mindful eating and living (MEAL): weight, eating behavior, and psychological outcomes associated with a mindfulness-based intervention for people with obesity. Complement Ther Med 18(6):260–264. doi:10.1016/j.ctim.2010.09.008
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Rosenbaum, D.L., White, K.S. Does cognitive avoidance mediate the relation of anxiety and binge eating?. Eat Weight Disord 21, 653–659 (2016). https://doi.org/10.1007/s40519-016-0284-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40519-016-0284-6