
Abstract
Purpose
Despite current recommendations and guidelines on the treatment of overweight and obesity, little is known about what patterns of energy intake or expenditure are ideal for weight loss. The present study examined patterns in energy intake and expenditure and explored whether those differences were associated with weight loss.
Methods
Self-monitoring data on energy intake and expenditure, along with minutes spent in exercise, were obtained from 90 overweight or obese adults (mean BMI = 38.0) enrolled in two behavioral weight loss programs. Energy intake and minutes of daily exercise were self-reported and energy expenditure was obtained from the Caltrac accelerometers that were provided to participants.
Results
On weekends (Friday through Sunday), participants consumed more calories from breakfast (271 vs. 241 kcals/day; p < .01), dinner (605 vs. 547 kcals/day; p < .001), and alcohol (59 vs. 27 kcals/day; p < .01), as well as total daily calories (1669 vs. 1520 kcals/day; p < .001) and expended fewer total calories (2515 vs. 2614 kcals/day; p < .01) than on weekdays. Higher caloric intake on weekdays was associated with less overall weight loss (r = −.29, p < .01) and was marginally associated on weekends (r = −.19, p = .051).
Conclusion
This investigation found evidence that while eating patterns clearly contribute to daily energy intake on weekdays and weekends, they may not necessarily contribute to weight change. At the end of the day, what may be most important is regular self-monitoring and total caloric intake on both the weekdays and weekends.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The current guidelines on the treatment of overweight and obesity in adults recommends, as an initial treatment goal, about a 10 % reduction in baseline body weight, which can be generally achieved by creating a caloric deficit of 500–1000 kilocalories (kcals) per day [1]. This results in modest weight loss [1] and has been found to reduce the occurrence of obesity-related medical conditions [2, 3]. The most effective way to create this deficit is through a combination of reducing energy intake and increasing energy expenditure [1]. However, despite these guidelines, little is known about which patterns of energy intake or expenditure are ideal for weight loss. And, with only about a fifth of participants enrolled in behavioral weight loss programs (BWLPs) successful in losing and maintaining weight loss for at least a year [4], it is possible that differences in eating and exercise patterns may be impacting treatment success.
While there is limited research on eating and exercise patterns, a number of studies have examined whether breakfast consumption is associated with weight loss [5–7]. For example, these studies suggest that eating breakfast, or earlier meals in the day, is associated with greater weight loss. Eating breakfast has also been found to be inversely associated with weight regain [8] and is one of the characteristics for “successful” weight maintenance [9]. However, less is known about other dietary and exercise patterns, as neither the frequency of meals throughout the day [10], the duration and intensity of exercise [11], nor the length of exercise sessions (smaller bouts versus one continuous bout; [12]) have been associated with more successful weight loss.
Research has also examined whether there is a difference in energy intake and expenditure throughout the week [13–17]. For example, in a nationally representative sample, adults aged 19–50 were found to consume 115 more calories on weekends than on weekdays [14]. Adults also consume more fat and alcohol and spend less time engaging in physical activity on weekends [13, 14, 17]. However, it is unclear how these patterns of eating and exercise relate to weight loss. Confirmation of this pattern may be important, given that adults at risk for obesity are more susceptible to weight gain due to increased caloric intake on weekends [16]. Thus, it is possible that if this pattern is observed among adults enrolled in a BWLP then it could have a significant impact on their treatment success.
The purpose of the current study was to examine patterns in dietary intake and physical activity among treatment-seeking overweight and obese adults and to determine whether these differences were associated with weight loss. While prior research has tended to focus on overall daily caloric intake, this study sought to also examine differences in caloric intake across individual meals, beverages, and snacks. Identifying such differences and their association with weight loss could greatly improve the effectiveness of BWLPs by highlighting daily and weekly eating and exercise patterns and identifying if there is in fact a more beneficial pattern for treatment success. Generally speaking, based on previous research [13, 14, 16, 17], it was hypothesized that adults would consume more calories and exercise less on weekends than weekdays. The association between weekday and weekend eating and activity patterns and weight loss was also examined. It was hypothesized that consuming greater calories on weekdays and weekends would be associated with less weight loss.
Methods
Participants
Self-monitoring data were obtained from 89 participants enrolled in two similar BWLPs (Study 1: N = 45; [18]; Study 2: N = 44; [19]). Data were used from two similar studies to increase statistical power.Footnote 1 Participants’ mean age was 46.4 years (SD = 12.8) and mean BMI was 38.0 (SD = 8.1; range = 26.5–63.4). Participants were primarily Caucasian (85 %), female (75 %), and married or living with a partner (80 %). Most participants (55 %) reported an annual income of over $45,000 and 58 % had at least a bachelor’s degree. There were no significant differences between the two weight loss program participants in baseline demographics. Eighty-two percent of participants completed the programFootnote 2 with an average weight loss of 7.0 % (SD = 5.0). The two programs did not differ in overall percent weight loss (Study 1: 6.9 ± 4.3 %; Study 2: 7.0 ± 5.7 %). However, because of the longer duration but less intensive nature of the intervention in study two, weekly percent weight loss was lower than study one (Study 1: 0.6 ± 0.4 %; Study 2: 0.4 ± 0.3 %, p < .01).
For both studies, participants were recruited through advertisements on community bulletin boards, newspapers, and emails sent to faculty and staff at a large Midwestern university. Participants were included if they were overweight or obese (BMI > 25 kg/m2), received medical clearance from their primary care physician, and were free from major medical conditions (e.g., insulin-dependent diabetes, uncontrolled hypertension, etc.). Additionally, participants were excluded if they: (1) were pregnant or currently nursing, (2) had undergone bariatric surgery, or (3) had a serious mental illness (i.e., schizophrenia and bipolar disorder) or an eating disorder. The procedures used in both weight loss studies were approved by the university’s human subject review board and all participants provided informed consent.
Weight loss programs
Both studies received similar program orientations and instructions to self-monitor energy intake and total daily energy expenditure (see “Self-monitoring”), and included weekly weight assessments and a combination of didactic instruction, group and individual in-class activities, and take home assignments. In each study, small groups of 10–15 people met weekly for approximately 90 min. Groups were led by a licensed clinical health psychologist or graduate students specializing in health psychology. Study one was 12 weeks in duration and study two was 18 weeks. However, both studies emphasized the modification of participants’ relationships with food, their bodies, and their weight, as well as healthy habit formation and disruption of unhealthy habits.
Participants in both studies were instructed on how to create a caloric deficit of 500–1000 kcals per day based on their total daily energy expenditure, which was obtained from the Caltrac accelerometers that were provided to participants. While participants were not explicitly told which foods and beverages they should or should not consume, they were educated on topics, such as nutrition, food choice, and portion control, which emphasized making healthier choices. In addition, in-class activities, such as “taste tests”, which involved trying healthier food options, and doing a “recipe makeover” (i.e., taking a recipe used at home and making it healthier), were done in class to further reinforce concepts discussed. The current recommended federal guidelines of at least 30 min of moderate-intensity aerobic activity for at least 5 days per week were provided as a target goal [1, 20]. Participants were also advised to increase lifestyle activity, such as taking the stairs instead of the elevator.
Measures
Self-monitoring
Participants were instructed on how to self-monitor dietary intake. They were provided with demonstrations of common food measurement procedures, as well as instructions for estimating food portion sizes, and were instructed on how to use reputable online calorie databases, such as the USDA’s SuperTracker and CalorieKing.com. Participants were further instructed on how to electronically (or by paper and pencil) submit daily records of energy intake from breakfast, lunch, dinner, snacks, nonalcoholic beverages, alcoholic beverages, and total energy intake. Meals and snacks were defined by the participants based on their own common practices.
Participants were also instructed to self-monitor time spent in physical activity (minutes) and total daily energy expenditure, based on the Caltrac accelerometer readings. As with dietary intake, participants were encouraged to submit daily records throughout the duration of treatment.
Energy expenditure
The Caltrac accelerometers were used to assess total daily energy expenditure (i.e., total energy expenditure from physical activity and rest). The Caltrac accelerometer measures vertical acceleration as the individual moves about and converts the measurement into an expenditure value (kcals/day) based on their age, sex, height, and weight, which are entered by the participants into the accelerometer. Although accelerometers have been shown to mildly overestimate the absolute energy cost (i.e., measured VO2) of selected activities, they provide a reliable assessment of total energy expenditure [21, 22]. Participants were instructed on the proper use of the accelerometer (e.g., wear over belt or waistband) and were reminded to record and reset it at the same time each day (every 24 h), as the accelerometers did not have a memory function.
Weight and body mass index (BMI)
Participants’ weights were measured to the nearest 0.1 pounds at baseline and post-treatment using a digital scale (BF-350e; Tanita, Arlington Heights, IL). Height was measured at baseline to the nearest 0.5 inch using a steel height rod on a standard spring scale. Height and weight were converted to meters and kilograms, respectively, before calculating BMI as kg/m2.
Statistical analyses
Self-monitoring data were aggregated by participant and day of the week by taking the average of each response over the course of treatment (i.e., calories consumed from each meal for each day of the week). All self-monitoring entries that were submitted over the treatment period in both studies were included in the analyses. We chose to be conservative and not remove any data, since there is no clear, consistent criterion used in the extant literature and information on how adherence is measured is lacking [23]. Further, our dataset contained no consistent pattern of missing or incomplete data. Consistent with prior research [14], weekday was defined as Monday through Thursday and weekend as Friday through Sunday.
Repeated measures ANOVAs were conducted to determine whether there was significant variability across the week in energy intake and expenditure. If there were any significant differences then paired samples t tests were utilized to examine if there were differences on weekdays and weekends. When the assumption of sphericity was violated, Huynh–Feldt or Greenhouse–Geisser corrections were applied. The effect of treatment type was used as a covariate (i.e., differences in each studies’ treatment groups) to examine differences in overall percent weight loss across weekdays and weekends. Missing data were handled using pairwise deletion to allow for maximum power to detect relationships between explanatory variables. The Benjamini and Hochberg procedure [24] was applied to tests involving multiple comparisons.
Results
Preliminary analyses
This investigation used 4830 days of self-monitoring entries submitted over the course of both studies. The mean number of entries that were submitted per person in study one was 48.7 (SD = 31.4; total possible entries = 83) and in study two was 60.0 (SD = 46.3; total possible entries = 139Footnote 3). In study one, participants self-monitored on 59 % of weekdays and 58 % of weekends, while in study two it was 44 and 42 %, respectively.Footnote 4 Participants submitted significantly more entries on weekdays than on weekends in study two (p < .01). A positive correlation was found between age and number of entries (r = .39, p < .001). No other significant differences emerged.
Differences in dietary intake and physical activity
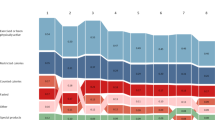
Figure 1 shows daily energy intake and expenditure throughout the week. Prior to examining differences in eating and activity patterns between weekdays and weekends, repeated measures ANOVAs were conducted to determine whether there was significant variability throughout the week.

Mean differences and 95 % confidence intervals for energy intake and exercise patterns across the week. M Monday, T Tuesday, W Wednesday, Th Thursday, F Friday, Sa Saturday, Su Sunday, WD weekday (Monday through Thursday), WE weekend (Friday through Sunday). Significance is indicated only for weekday and weekend comparisons. **p < .01; ***p < .001. aSelf-report. bAccelerometer readings
Significant differences were found across the week in calories consumed from breakfast, F(4.7, 356.9) = 3.4, p < .01, lunch, F(5.5, 412.1) = 3.7, p < .01, dinner, F(5.5, 425.0) = 6.2, p < .001, and alcoholic beverages, F(2.7, 178.4) = 4.6, p < .01, as well as total caloric intake, F(5.1, 389.5) = 14.6, p < .001 and total daily energy expenditure, F(2.7, 204.1) = 6.4, p < .01. There were no significant differences in calories consumed from snacks and nonalcoholic beverages, or minutes exercised. Therefore, comparisons between calories consumed from snacks and nonalcoholic beverages, as well as minutes exercised on weekdays and weekends were not examined further. To avoid running an excessive number of statistical comparisons with the attendant risk of Type I error, we chose to limit statistical analyses between weekdays and weekends.
Results from paired samples t tests indicated significant differences in eating and exercise on weekdays and weekends (Table 1). Specifically, on weekends, adults consumed a greater percentage of calories from breakfast, dinner, and alcoholic beverages, consumed more total calories, and expended fewer total daily calories.
Association between dietary intake and weight loss
There was a significant correlation between overall percent weight loss and total caloric intake on weekdays (r = −.29, p < .01). This relationship was marginally significant for total caloric intake on weekends (r = −.19, p = .051). Greater caloric intake on both weekdays and weekends combined was associated with less weight loss (r = −.25, p < .05). No significant differences emerged from calories consumed from breakfast, dinner, or alcoholic beverages, or total daily calories expended. However, a significant association was found between the percentage of days self-monitored and overall percent weight loss (weekdays: r = .47, p < .001; weekends: r = .49, p < .001).
Association between weekday and weekend calorie consumption
Given that all participants were trying to lose weight and caloric intake was associated with weight loss, we were curious if those who consumed more calories on the weekends compensated for this by lowering their intake on the weekdays or vice versa. Therefore, post hoc analyses examining for compensation between calorie consumption on weekends and weekdays were conducted. We ran a one-sample t test using serial correlation z-scores for overall energy intake from one period to the next (e.g., weekdays of week 1 to weekend days of week 1, etc.) and found no evidence for compensation occurring in the overall sample, t(75) = −1.23, p = .223. However, a marginally significant finding was found among successful weight losers (i.e., those who lost ≥5 % of their baseline weightFootnote 5), t(45) = −1.99, p = .053.
Discussion
There is no shortage of advice on eating patterns that will lead to weight loss. Nevertheless, few studies have examined patterns in dietary intake and physical activity across the week, with the goal of determining whether these patterns are associated with weight loss. Consistent with previous research [14], the current investigation’s overweight and obese sample consumed approximately 150 more calories per day on weekends (Friday through Sunday) than weekdays. While modest, an extra 450 kcals on the weekend could result in an extra 23,400 kcals over the course of a year and likely contribute to significant weight gain. The greater consumption during weekends was distributed primarily among breakfast (20 % of increased caloric consumption), dinner (39 %), and alcoholic beverages (21 %), suggesting that it is overall consumption and not one particular area. Although it was not assessed whether meals were eaten in or out, anecdotally, weight loss participants often report consuming more food and alcohol on the weekends because of social gatherings, celebrations, etc. These findings are summarized in Fig. 1 and are consistent with previous research on alcohol consumption [14, 25]. Therefore, even among weight loss participants who are closely monitoring their energy intake, weekends appear to be a time of lower adherence.
Total daily energy expenditure was significantly lower on weekends, however, minutes spent in physical activity was not significantly different. It is possible that this discrepancy is due to differences in the types of physical activity that participants engaged in. In other words, while formal exercise minutes is similar, participants may have engaged in less unstructured exercise (e.g., walking) during the weekend. This is consistent with prior research indicating that adults take fewer steps on weekends (10,479 vs. 9091 steps/day; [13, 17]). Given that these patterns observed in the general population were replicated among weight loss participants suggests that it may be challenging to modify existing activity habits or patterns.
In this investigation, all participants were actively attempting to lose weight. Nevertheless, eating and activity patterns between the weekdays and weekends were significantly different and distinct (Fig. 1). Despite this, differences in individual meals and beverages on weekdays and weekends were not associated with overall weight loss. Thus, it appears that having a little more alcohol and some larger meals on the weekend may not completely sabotage a diet. While total daily calories on weekdays were more strongly associated with weight loss than on weekends, this is not to say that the weekend is not important, as greater caloric intake on both weekdays and weekends combined was associated with less weight loss. Additionally, the frequency of self-monitoring on weekdays and weekends was associated with weight loss; though, this finding was not too surprising, given that the importance of regular self-monitoring to successful weight loss has been well established [26].
Our findings suggest that most people “let loose” on the weekend. However, it may be that those who consume more calories on the weekends compensate for this by lowering their intake on the weekdays. Post hoc analyses examining for compensation between calorie consumption on weekends and weekdays found that, while there was no evidence for compensation in the overall sample, there was a marginally significant finding among successful weight losers. This may suggest that successful weight losers are able to offset days characterized by higher energy intake by cutting back on successive days. If so, then this could prove to be beneficial for long-term weight control, as adhering to a strict eating routine every day may be tiring and lead to issues with long-term compliance. In which case, having some flexibility on the weekends may allow them to not feel as psychologically deprived.
Interestingly, total daily calories expended were not associated with weight loss. This finding is consistent with previous research suggesting that regular exercise may have only a modest ability to influence weight [11, 27]. To illustrate, an individual who engages in 30 min of moderate-intensity physical activity on five or more days each week is likely to expend the equivalent of approximately 1000 kcal per week. However, one large meal can easily exceed this, essentially offsetting a week’s worth of exercise-related calories. Therefore, in the end, caloric intake may have a larger influence on weight loss than caloric expenditure.
This investigation has several limitations that should be noted. First, individuals’ reports of dietary intake and physical activity can be inaccurate, particularly among overweight individuals [28]. However, we are not familiar with any research indicating systematic distortion by particular meals or days of the week and all participants in this investigation were treatment-seeking overweight or obese adults. Therefore, systematic weight-related differences between subjects were likely minimized. Additionally, consistent with observations from other BWLPs, many individuals did not maintain consistent food records. These inconsistencies likely reflect noncompliance with self-monitoring instructions, secondary to sickness, motivation, or time constraints. However, this study’s use of self-report data does make it subject to social desirability bias and misrepresentation. For example, when compared to direct measurements (e.g., doubly labeled water technique, indirect calorimetry), individuals tend to underestimate energy intake and overestimate physical activity [29, 30]. Nevertheless, despite this, self-report measures continue to be used, as they are a cost-effective, time-efficient method that can provide an estimate of caloric intake and expenditure. Further, while individuals were instructed on how to use various reputable online calorie databases, it was not made explicit to use a specific database. Nevertheless, programs such as these primarily use the USDA’s National Nutrient Database for Standard Reference. As such, the energy values for foods and beverages across databases should be relatively consistent. Finally, the sample is largely homogeneous (Caucasian, female, treatment-seeking), indicating that generalizability of these findings may be limited.
Conclusion
Obesity continues to be a leading public health concern in the United States, with over two-thirds of the population either overweight or obese [31]. The current obesity epidemic has heightened interest in identifying consumption patterns that might contribute to weight gain or poor health. Individuals are commonly inundated with competing, and often, contradictory messages about eating patterns and weight loss. This investigation found evidence that while eating patterns clearly contribute to daily energy intake on weekdays and weekends, they may not necessarily contribute to weight change. At the end of the day, what may be most important to weight loss is regular self-monitoring and total caloric intake on both the weekdays and weekends.
Notes
The statistical power for the main analyses ranged from 0.66 to 0.99, with effect sizes ranging from 0.2 to 0.7.
The total possible number of self-monitoring entries that could be submitted in study one was 12 weeks and in study two was 20 weeks, as both studies also included an orientation and/or a screening visit. The last week of each study’s weight loss program was not required, as the final class took place on the first day of that week and no entries were required to be submitted after the final class. There was also an additional week included in study two due to a break that occurred during the treatment period.
Study two’s compliance was lower than study one’s due to the longer duration of treatment, as self-monitoring frequency has been shown to decrease over the course of treatment [34].
We used a 5 % cutoff because it is commonly included in the range for “successful” weight loss due to its demonstrated health benefits [2].
References
National Heart Lung and Blood Institute (1998) Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults: The Evidence Report. http://www.nhlbi.nih.gov/files/docs/guidelines/ob_gdlns.pdf
Hamman RF, Wing RR, Edelstein SL et al (2006) Effect of weight loss with lifestyle intervention on risk of diabetes. Diabetes Care 29:2102–2107. doi:10.2337/dc06-0560
Wing R, Lang W, Wadden T et al (2011) Benefits of modest weight loss in improving cardiovascular risk factors in overweight and obese individuals with Type 2 diabetes. Diabetes Care 34:1481–1486. doi:10.2337/dc10-2415
McGuire MT, Wing RR, Hill JO (1999) The prevalence of weight loss maintenance among American adults. Int J Obes 23:1314–1319. doi:10.1038/sj.ijo.0801075
Garaulet M, Gómez-Abellán P, Alburquerque-Béjar JJ et al (2013) Timing of food intake predicts weight loss effectiveness. Int J Obes 37:604–611. doi:10.1038/ijo.2012.229
Jakubowicz D, Barnea M, Wainstein J, Froy O (2013) High Caloric intake at breakfast vs. dinner differentially influences weight loss of overweight and obese women. Obesity 21:2504–2512. doi:10.1002/oby.20460
Keim NL, Van Loan MD, Horn WF et al (1997) Weight loss is greater with consumption of large morning meals and fat-free mass is preserved with large evening meals in women on a controlled weight reduction regimen. J Nutr 127:75–82
Van der Heijden, AAWA, Hu FB, Rimm EB, van Dam RM (2007) A prospective study of breakfast consumption and weight gain among U.S. men. Obesity 15:2463–2469. doi:10.1038/oby.2007.292
Wyatt HR, Grunwald GK, Mosca CL et al (2002) Long-term weight loss and breakfast in subjects in the National Weight Control Registry. Obes Res 10:78–82. doi:10.1038/oby.2002.13
Cameron JD, Cyr M-J, Doucet E (2010) Increased meal frequency does not promote greater weight loss in subjects who were prescribed an 8-week equi-energetic energy-restricted diet. Br J Nutr 103:1098–1101. doi:10.1017/S0007114509992984
Jakicic J, Clark K, Coleman E et al (2001) American College of Sports Medicine position stand. Appropriate intervention strategies for weight loss and prevention of weight regain for adults. Med Sci Sports Exerc 33:2145–2156. doi:10.1097/00005768-200112000-00026
Schmidt WD, Biwer CJ, Kalscheuer LK (2001) Effects of long versus short bout exercise on fitness and weight loss in overweight females. J Am Coll Nutr 20:494–501. doi:10.1080/07315724.2001.10719058
Clemes S, Griffiths P, Hamilton S (2007) Four-week pedometer-determined activity patterns in normal weight and overweight UK adults. Int J Obes 31:261–266. doi:10.1038/sj.ijo.0803420
Haines PS, Hama MY, Guilkey DK, Popkin BM (2003) Weekend eating in the United States is linked with greater energy, fat, and alcohol intake. Obes Res 11:945–949. doi:10.1038/oby.2003.130
Hart CN, Raynor HA, Osterholt KM et al (2011) Eating and activity habits of overweight children on weekdays and weekends. Int J Pediatr Obes 6:467–472. doi:10.3109/17477166.2011.590204
Racette SB, Weiss EP, Schechtman KB et al (2008) Influence of weekend lifestyle patterns on body weight. Obesity 16:1826–1830. doi:10.1038/oby.2008.320
Tudor-Locke C, Burkett L, Reis J et al (2005) How many days of pedometer monitoring predict weekly physical activity in adults? Prev Med (Baltim) 40:293–298. doi:10.1016/j.ypmed.2004.06.003
Carels RA, Burmeister JM, Koball AM et al (2014) A randomized trial comparing two approaches to weight loss: differences in weight loss maintenance. J Health Psychol 19:296–311. doi:10.1177/1359105312470156
Carels RA, Hoffmann DA, Hinman N et al (2013) Step-down approach to behavioural weight loss treatment: a pilot of a randomised clinical trial. Psychol Health 28:1121–1134. doi:10.1080/08870446.2013.789875
U.S. Department of Health and Human Services (2008) 2008 Physical Activity Guidelines for Americans. http://www.health.gov/paguidelines/pdf/paguide.pdf
Fehling P, Smith D, Warner S, Dalsky G (1999) Comparison of accelerometers with oxygen consumption in older adults during exercise. Med Sci Sports Exerc 31:171–175. doi:10.1097/00005768-199901000-00026
Pambianco G, Wing R, Robertson R (1990) Accuracy and reliability of the Caltrac accelerometer for estimating energy expenditure. Med Sci Sports Exerc 22:858–862. doi:10.1249/00005768-199012000-00020
Burke LE, Wang J, Sevick MA (2011) Self-monitoring in weight loss: a systematic review of the literature. J Am Diet Assoc 111:92–102. doi:10.1016/j.jada.2010.10.008
Benjamini Y, Hochberg Y (1995) Controlling the false discovery rate: a practical and powerful approach to multiple testing. J R Stat Soc 57:289–300. doi:10.2307/2346101
Thompson FE, Larkin FA, Brown MB (1986) Weekend–weekday differences in reported dietary intake: the nationwide food consumption survey, 1977–78. Nutr Res 6:647–662. doi:10.1016/S0271-5317(86)80006-9
Carels RA, Darby LA, Rydin S et al (2005) The relationship between self-monitoring, outcome expectancies, difficulties with eating and exercise, and physical activity and weight loss treatment outcomes. Ann Behav Med 30:182–190. doi:10.1207/s15324796abm3003_2
Garrow J, Summerbell C (1995) Meta-analysis: effect of exercise, with or without dieting, on the body composition of overweight subjects. Eur J Clin Nutr 49:1–10
Trabulsi J, Schoeller DA (2001) Evaluation of dietary assessment instruments against doubly labeled water, a biomarker of habitual energy intake. Am J Physiol Metab 5:E891–E899
Hill RJ, Davies PS (2001) The validity of self-reported energy intake as determined using the doubly labelled water technique. Br J Nutr 85:415–430. doi:10.1079/BJN2000281
Lichtman SW, Pisarska K, Berman ER et al (1992) Discrepancy between self-reported and actual caloric intake and exercise in obese subjects. N Engl J Med 327:1893–1898. doi:10.1056/NEJM199212313272701
Ogden C, Carroll M, Kit B, Flegal K (2014) Prevalence of childhood and adult obesity in the United States, 2011-2012. J Am Med Assoc 311:806–814. doi:10.1001/jama.2014.732
Williams RL, Wood LG, Collins CE, Callister R (2015) Effectiveness of weight loss interventions - is there a difference between men and women: a systematic review. Obes Rev 16:171–186. doi:10.1111/obr.12241
Mutsaerts MAQ, Kuchenbecker WKH, Mol BW et al (2013) Dropout is a problem in lifestyle intervention programs for overweight and obese infertile women: a systematic review. Hum Reprod 28:979–986. doi:10.1093/humrep/det026
Carels RA, Young KM, Coit C et al (2008) Can following the caloric restriction recommendations from the Dietary Guidelines for Americans help individuals lose weight? Eat Behav 9:328–335. doi:10.1016/j.eatbeh.2007.12.003
Acknowledgments
We would like to thank the anonymous reviewers for helping improve the paper through their insightful and valuable feedback. We would also like to thank Dr. Richard Anderson (Bowling Green State University) for his statistical expertise and assistance with some of our analyses.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Rights and permissions
About this article

Cite this article
Hoffmann, D.A., Carels, R.A. Does when you eat and exercise matter? Differences in eating and physical activity patterns in overweight and obese adults. Eat Weight Disord 21, 91–98 (2016). https://doi.org/10.1007/s40519-015-0214-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40519-015-0214-z