
Abstract
Purpose
Abnormal feeding has been linked to disruptions in brain dopaminergic activity and recent studies have assessed the role of catechol-O-methyltransferase (COMT) in eating disorders. This is the first study to quantify the soluble catechol-O-methyltransferase (S-COMT) activity in erythrocytes from patients with anorexia nervosa (AN), bulimia nervosa (BN) and binge-eating disorder (BED) and the first study at all to evaluate the COMT on patients with BED.
Methods
Forty blood samples from patients with AN, BN and BED and healthy controls were drawn to evaluate S-COMT activity in erythrocytes by high-performance liquid chromatography and mass spectrometry. Since several patients were being treated with fluoxetine 20 mg, they were included in a different group (BN MED and BED MED). Liver homogenates from rats were used to evaluate baseline S-COMT activity in the presence of fluoxetine by the same in vitro procedures and assays.
Results
Erythrocyte S-COMT activity (pmol/mg prt/h) was significantly increased in patients with BN and BED (41.3 ± 6.8 and 41.4 ± 14, respectively) compared to control group (25.3 ± 9.7). In fluoxetine-treated patients with BN, S-COMT activity (15.9 ± 8.8) was decreased compared to the other BN group; however, in BED group, the difference between BED MED and BED was not observed. In patients with AN, no significant difference was found compared to controls.
Conclusion
Patients with BN and BED presented higher S-COMT activity in erythrocytes, which is in agreement with previous studies on the literature addressing the high-activity COMT allele, Val158, as risk factor for eating disorders. Although in fluoxetine-treated patients with BN the activity of S-COMT was similar to the controls, this is not explained by a direct interaction between fluoxetine and S-COMT as verified in in vitro assays.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Eating disorders (ED) like anorexia nervosa (AN), bulimia nervosa (BN) and binge-eating disorder (BED) are chronic and disabling conditions with complex psychopathological manifestation and multifactor aetiology [1].
In the last years, serotonin attracted most of the attention in the studies about eating behaviour and psychopathological features coupled with ED. However, growing evidence suggests that dopaminergic neuronal functions may play a relevant role [1, 2]. Dopamine released in the dorsal striatum regulates feeding behaviour and correlates with the degree of pleasure experienced whilst eating as well as others motivated and emotional behaviours [3]. Thus, striatal dopaminergic dysfunction might contribute to altered reward and affect, decision making, and executive control in ED [4].
Although widely expressed, catechol-O-methyltransferase (COMT) appears to be of minor relevance in dopamine clearance when compared with neuronal synaptic uptake by the dopamine transporter and subsequent monoamine oxidase metabolism [5]. However, in prefrontal cortex (PFC), where dopamine transporter expression is low, the COMT appears to be of greater importance [5]. In striatum, COMT levels are lower than in PFC [6], although this does not necessarily mean that COMT has no impact on the function of this region [7]. An indirect effect mediated by COMT on PFC strongly regulates dopaminergic activity in striatum [8].
The COMT gene encodes distinct COMT allozymes (membrane bound (MB-) and soluble (S-) COMT). MB-COMT has 50 hydrophobic amino acids, containing the membrane-spanning region, that are not present in the 221 amino acid-soluble catechol-O-methyltransferase (S-COMT) [8]. Most human tissues express both COMT mRNA transcripts, but in brain, only the MB-COMT is readily detectable. The human COMT gene also contains a functional polymorphism in its sequence (Val158Met) which alters enzyme activity: individuals homozygous for the valine allele (Val158) have activity approximately 40 % higher, which may result in faster breakdown of the catecholamines, potentially leading to lower levels of dopamine in the synaptic cleft, than those homozygous for the methionine allele (Met158), whilst heterozygotes have intermediate activity [7].
In the last 15 years, several studies were published about the association between COMT polymorphism, particularly Val158Met, and AN and BN. The results were controversial: some studies appointed the higher activity allele as risk factor for AN [9, 10] or BN [1, 11, 12], whereas other group of studies pointed out the lower activity COMT allele [13, 14]. Some studies did not find association between this polymorphism and AN [1, 2, 15–18] and BN [10].
Diverse interactions between serotonergic, noradrenergic and dopaminergic systems occur in the central nervous system, which makes clinical response to pharmacological treatment a complex phenomenon [19]. Through these years, the hypothesis of modulating COMT activity by selective serotonin reuptake inhibitor (SSRI) [20] and COMT inhibitors [21, 22] as potential treatments for these disorders was also studied.
In the present study, we aim to evaluate the S-COMT activity in erythrocytes from patients with AN, BN and BED, and fluoxetine-treated patients with BN and BED.
Methods
Patients and blood samples
A total of 30 patients with diagnosis of AN, BN and BED (n = 10 each group) made by a senior psychiatrist using the SCID-I (Structured Clinical Interview for DSM-IV Axis I disorders) [23] and EDE-Q (Eating Disorder Examination Questionnaire) [24] were selected. Patients were recruited from the outpatient clinic of the department of Psychiatry of Hospital São João (Porto, Portugal). A number of 10 control subjects matched for age and gender, among medical and nursing students/fellowships in mental health courses were enrolled. Since several patients diagnosed with BN and BED were being treated with anti-depressive for more than 6 weeks, namely a stable dose of a SSRI, fluoxetine 20 mg, they were included in different groups (BN MED and BED MED, respectively). Participants with history of tabagism and drug consumption were not included. Data regarding height, weight and body mass index (BMI) were collected. Body composition was evaluated with a bioelectrical impedance analyser (Bodystat® QuadScan 4000). Bicipital, tricipital, subscapular and suprailiac skinfold thickness using a Harpenden compass were measured. Venous blood samples were drawn, between 08.00 and 09.00 a.m., after an overnight fast and kept on ice in K3EDTA tubes until processing. During the study, by decision of the authors, since the big majority of the participants were females and some participants had a prior history of no therapeutic compliance, total of 10 patients and 1 control were excluded.
Animals
Four male Wistar rats (Interfauna Ibérica, Barcelona, Spain) aged 60 days old were used. Rats were kept under controlled environmental conditions (12-h light/dark cycle and room temperature (22 ± 1 °C) with food and tap water allowed ad libitum. Rats were anesthetized with sodium pentobarbital (60 mg/kg) and perfused through the left ventricle with 0.9 % (w/v) NaCl. Livers were excised and homogenized in 5 mM sodium phosphate buffer, pH 7.8, at 4 °C with a Teflon homogenizer (Heidolph).
Preparation of erythrocyte and liver S-COMT
The liver S-COMT was obtained as previously described by Vieira-Coelho and Soares-da-Silva [25]. In brief, the liver homogenates were centrifuged at 15,000g for 20 min at 4 °C and the supernatants at 100,000g for 60 min at 4 °C. The high-speed supernatants were used for determination of the liver S-COMT. Erythrocyte S-COMT was obtained from washed erythrocytes submitted to haemolysis as previously described by Schultz et al. [26]. Blood samples were centrifuged at 1500g for 10 min at 4 °C and plasma and the uppermost cell layer were removed. Then, to the tubes was added a volume of cold 0.9 % NaCl solution and both fractions were mixed by gentle vortex. Thereafter, the tubes were centrifuged (at 1500g, 10 min, 4 °C) and the supernatant discarded. The erythrocyte washing process was repeated twice. Washed erythrocytes were stored at −70 °C, until the enzyme assay. On the day of the experiment, the frozen erythrocytes were thawed on ice. Haemolysis was conducted at a ratio of 4:1 (water:erythrocytes; V:V). After vigorous mixing, the tubes stood on ice for 10 min. Then, the tubes were centrifuged at 20,000g for 20 min at 4 °C and the supernatant collected for the assay of erythrocyte S-COMT. The protein content in the homogenates and supernatants was determined by the method of Bradford [27] with human serum albumin as standard.
In vitro studies
Aliquots of 0.5 ml of erythrocyte and liver S-COMT were pre-incubated for 20 min with 0.4 ml of phosphate buffer in the presence of a saturating concentration of the methyl donor, S-adenosyl-l-methionine (500 mM). The incubation medium also contained pargyline (100 mM), MgCl2 (100 mM) and EGTA (1 mM). The reaction mixture was incubated with a saturating concentration of adrenaline (5, 50, 250, 500, 1000, 2000 µM). The pre-incubation and incubation were carried out at 37 °C under conditions of light protection with continuous shaking. At the end of the incubation period (5 min), the tubes were transferred to ice and the reaction was stopped by the addition of 200 ml of 2 M perchloric acid. In liver experiments carried out to evaluate the effect of fluoxetine, this inhibitor was present since the pre-incubation time in six concentrations (3, 10, 30, 100, 300, 1000 µM).
Assay of COMT
COMT activity was determined by the ability of enzyme preparations to methylate adrenaline to metanephrine as previously described in crude homogenates and S-COMT [25]. The reaction was stopped with perchloric acid, the samples were kept at 4 °C for two hours and then centrifuged (5400g, 10 min, 4 °C); 500 ml aliquots of the supernatant, filtered on 0.22 mm pore size Spin-X filter tubes (Costar), were used for the assay of metanephrine.
Assay of catechol derivatives
Adrenaline and metanephrine samples were assayed by HPLC (high-performance liquid chromatography) with electrochemical detection, as previously described by Soares-da-Silva et al. [28]. Aliquots of samples from the COMT assay were assayed for metanephrine by HPLC with electrochemical detection, as previously described by Vieira-Coelho and Soares-da-Silva [25]. In brief, aliquots of 20 or 50 ml were injected into the chromatograph. The chromatographic system consisted of a pump (Gilson 307) and a stainless steel 5 mm ODS2 column (Biophase; Bioanalytical Systems, West Lafayette, IN, USA) of 25 cm length and 4.6 mm diameter; samples were injected by means of an automatic sample injector (Gilson 231) connected to a Gilson dilutor (Gilson 401). The mobile phase was a degassed solution of citric acid 0.1 mM; sodium octylsulphate 0.5 mM; sodium acetate 0.1 M; Na2EDTA 0.17 mM; dibutylamine 1 mM and methanol (10 % v/v), adjusted to pH 3.5 with PCA 2 M and pumped at a rate of 1.0 ml/min. The detection was carried out electrochemically with a glassy carbon electrode, an Ag/AgCl reference electrode and an amperometric detector (Gilson 142); the detector cell was operated at 0.75 V. The current produced was monitored using the Gilson Unipoint HPLC software. The lower limit of detection of metanephrine ranges from 350 to 1000 fmol.
Drugs
S-adenosyl-l-methionine, fluoxetine, DL-metanephrine and adrenaline (bitartrate salt) were purchased from Sigma Chemical Co. (St Louis, MO).
Kinetic analysis
Michaelis–Menten constant (Km) and maximum velocity (Vmax) values for COMT activity were calculated by nonlinear regression analysis using GraphPad Prism version 6.0 for Windows (GraphPad Software, La Jolla, CA, USA).
Statistical analysis
Statistical analysis was performed by one-way (ANOVA) with Dunnett’s for multiple comparisons or Student’s t test using GraphPad Prism version 6.0 for Windows (GraphPad Software, La Jolla, CA, USA). A p value less than 0.05 was assumed to denote a significant difference.
Results
Concerning about anthropometric parameters, significant differences in BMI and body fat percentage were found in AN and BED groups compared to control group. As expected, patients with AN had lower BMI (15.6 ± 0.5 kg/m2, p < 0.05) than controls (22.5 ± 0.9 kg/m2). On the other hand, patients with BED and fluoxetine-treated BED presented higher BMI (39.3 ± 1.4 and 44.3 ± 4.0 kg/m2, respectively, p < 0.05), and body fat percentage (46.0 ± 1.1 and 49.3 ± 1.4 %, respectively, p < 0.05) compared to control group (BMI: 22.5 ± 0.9 kg/m2 and body fat percentage: 30.1 ± 2.3 %). No statistical differences were found in patients with BN when compared with control group. In line with the clinical diagnosis, results from EDE-Q assessment (restraint, shape, eating and weight concerns) were significantly higher (p < 0.05) in all groups compared to control group.
S-COMT activity in erythrocytes was time and adrenaline concentration dependent as shown in Fig. 1a, b. Km and Vmax values were 362 ± 193 μM and 40 ± 7 pmol/mg prt/h, respectively. From these results, an incubation time of 60 min and a saturating concentration of 1000 µM of adrenaline were chosen in all further assays.

Human erythrocyte S-COMT activity (pmol/mg prt/h) shown as the rate of formation of metanephrine (MN) with time (a) and increasing concentrations (μM) of adrenaline (AD) (b)
Table 1 summarizes the measurements of S-COMT activity in all groups. At a single concentration of substrate (1000 μM of adrenaline), baseline S-COMT activity of patients with AN was not significantly different from control group. On the other hand, patients with BN showed increased S-COMT activity (41.3 ± 6.8 pmol/mg prt/h, p < 0.05) when compared with controls (25.3 ± 9.7 pmol/mg prt/h). Interestingly, this group presented higher S-COMT activity compared with fluoxetine-treated patients with BN (15.9 ± 8.8 pmol/mg prt/h, p < 0.05). No differences between fluoxetine-treated patients with BN and control participants were observed. Concerned to BED, the patients had also higher values of S-COMT activity (40.9 ± 14.3 pmol/mg prt/h, p < 0.05), but no differences were seen between BED and fluoxetine-treated BED groups.
Since we have found significant differences in baseline S-COMT activity in BN and BED patients, further enzymatic kinetic studies were performed. The results of these studies are presented in Figs. 2, 3 and 4 and Table 1. Regarding Km values, no differences were seen among all the groups; however, in patients with BN and BED, Vmax was significantly higher (60 ± 6 and 61 ± 9 nmol/mg prt/h, p < 0.05, respectively) compared with control group (37 ± 4 nmol/mg prt/h). Vmax of fluoxetine-treated BN patients was lower (23 ± 2 nmol/mg prt/h, p < 0.05) than Vmax of the other BN group.

Erythrocyte S-COMT activity (pmol/mg prt/h) in patients with anorexia nervosa (AN) shown as the rate of formation of metanephrine (MN) with increasing concentrations (μM) of adrenaline (AD)

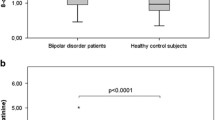
Erythrocyte S-COMT activity (pmol/mg prt/h) in patients with bulimia nervosa (BN) and in fluoxetine-treated patients with bulimia nervosa (BN MED) shown as the rate of formation of metanephrine (MN) with increasing concentrations (μM) of adrenaline (AD). *p < 0.05

Erythrocyte S-COMT activity (pmol/mg prt/h) in patients with binge-eating disorder (BED) and in fluoxetine-treated patients with binge-eating disorder (BED MED) shown as the rate of formation of metanephrine (MN) with increasing concentrations (μM) of adrenaline (AD). *p < 0.05
The differences found on fluoxetine-treated patients with BN compared to the other group of BN patients led us to study the liver baseline S-COMT activity of rats pre-incubated with fluoxetine. The baseline S-COMT activity was not modified, presenting similar values of baseline S-COMT activity as the group without fluoxetine.
Discussion
The contribution of this work for the study of the association of COMT and ED is especially important because it is the first work to do a quantitative evaluation of the COMT activity in erythrocytes of these patients. Furthermore, it is the first study evaluating the association between COMT and BED. In the present study, a statistically significant increase of the S-COMT activity was observed in patients with BN and BED. These findings corroborate the growing evidence about the role of COMT on ED. Moreover, these results are in line with several studies that pointed out the high-activity allele of COMT, Val158, as risk factor for BN [1, 11, 12]. However, as mentioned before, some studies also showed an association between the low activity allele of COMT, Met158 and ED, whereas other studies found no association. To understand this possible association, it is important to keep in mind that ED are complex and multifactorial. This means that the relationship between COMT activity and ED is more complex than ‘low COMT activity is good, high COMT activity is bad’. The exact effect that COMT activity plays on ED most probably depends on an individual given environmental and genetic context. The stress that an individual is subjected to and the complex genetic interactions and background on which the COMT genotype is expressed are known to affect COMT activity [5].
An interesting result was observed in fluoxetine-treated patients with BN, whose S-COMT activity was significantly lower than the other group of BN patients. However, in vitro experiments with livers of rats showed no changes in baseline S-COMT activity, when a pre-incubation with fluoxetine was performed. Liver has a special role in relation to catecholamine metabolism and it has the highest COMT activity in the body. For this reason is expected to play a central role when modulation of COMT has to be tested [29]. However, a recent study [20] suggests that serotonin inhibits COMT activity by actively competing with S-adenosyl methionine (SAM) at the active site; without SAM, COMT is unable to metabolize substrates such as dopamine. Therefore, one of these conditions has to be confirmed or/and other hypotheses have to be suggested to clarify this interaction. SSRI and COMT could be directly or indirectly related when the background of multiple and complex interactions between genes, proteins and environment (including drugs) is taken into account.
The lack of a significant difference between patients with AN and control group is in line with several studies on literature, which also reported no association between COMT polymorphism and AN [1, 2, 15, 16, 18]. However, an association between Val158 and AN was also shown in two studies [9, 10]. Curiously, a study of Michaelovsky et al. [30] showed that Val158 was associated with restricting AN and the Met158 had protective effect. These differences were not found in bingeing/purging AN. As a limitation of our study, the group of patients with AN should be evaluated separately according to restricting and bingeing/purging subtypes, what would be important to verify if this difference between subtypes exists or not. Another limitation is the few participants included in all groups. These results are very promising because they increase our understanding about the modulation of dopaminergic system on ED and can open opportunities to treat these patients. So, it is important to confirm these results with more studies with a more patients.
Curiously, all the studies on literature trying to find an association between COMT and ED were performed on patients with AN and BN, with no studies on BED. Another strong recommendation for future studies on this area is to evaluate genotype and phenotype of COMT in patients with AN, BN and even more on BED. Future studies should also clarify the modulation of COMT activity, using SSRI or even COMT inhibitors.
Conclusion
Patients with BN and BED presented higher soluble COMT activity in erythrocytes. The higher Vmax values in BN and BED compared to controls and the similar Km values in these groups indicate that these patients have more enzymatic functional units with similar affinity. These findings are in line with studies on literature addressing the allele Val158 (higher COMT activity) as risk factor for these disorders. Fluoxetine-treated patients with BN presented lower levels of S-COMT compared to the other group of BN patients, which may not be explained by a direct relationship between S-COMT and fluoxetine as verified in in vitro assays. Despite all the results, it is important to keep in mind the complex psychopathological manifestation and multifactor aetiology of these disorders. To validate these results, more studies should be performed, including on BED, which have not been so studied as AN and BN.
References
Mikolajczyk E, Grzywacz A, Samochowiec J (2010) The association of catechol-O-methyltransferase genotype with the phenotype of women with eating disorders. Brain Res 1307:142–148. doi:10.1016/j.brainres.2009.10.035
Gervasini G, Gordillo I, Garcia-Herraiz A, Flores I, Jimenez M, Monge M, Carrillo JA (2013) Influence of dopamine polymorphisms on the risk for anorexia nervosa and associated psychopathological features. J Clin Psychopharmacol 33(4):551–555. doi:10.1097/JCP.0b013e3182970469
Baik JH (2013) Dopamine signaling in reward-related behaviors. Frontiers in neural circuits 7:152. doi:10.3389/fncir.2013.00152
Kaye W (2008) Neurobiology of anorexia and bulimia nervosa. Physiol Behav 94(1):121–135. doi:10.1016/j.physbeh.2007.11.037
Craddock N, Owen MJ, O’Donovan MC (2006) The catechol-O-methyl transferase (COMT) gene as a candidate for psychiatric phenotypes: evidence and lessons. Mol Psychiatry 11(5):446–458. doi:10.1038/sj.mp.4001808
Matsumoto M, Weickert CS, Akil M, Lipska BK, Hyde TM, Herman MM, Kleinman JE, Weinberger DR (2003) Catechol O-methyltransferase mRNA expression in human and rat brain: evidence for a role in cortical neuronal function. Neuroscience 116(1):127–137
Tunbridge EM, Huber A, Farrell SM, Stumpenhorst K, Harrison PJ, Walton ME (2012) The role of catechol-O-methyltransferase in reward processing and addiction. CNS Neurol Disord Drug Targets 11(3):306–323
Tunbridge EM, Harrison PJ, Weinberger DR (2006) Catechol-O-methyltransferase, cognition, and psychosis: Val158Met and beyond. Biol Psychiatry 60(2):141–151. doi:10.1016/j.biopsych.2005.10.024
Frisch A, Laufer N, Danziger Y, Michaelovsky E, Leor S, Carel C, Stein D, Fenig S, Mimouni M, Apter A, Weizman A (2001) Association of anorexia nervosa with the high activity allele of the COMT gene: a family-based study in Israeli patients. Mol Psychiatry 6(2):243–245. doi:10.1038/sj.mp.4000830
Mikolajczyk E, Smiarowska M, Grzywacz A, Samochowiec J (2006) Association of eating disorders with catechol-O-methyltransferase gene functional polymorphism. Neuropsychobiology 54(1):82–86. doi:10.1159/000096043
Groleau P, Steiger H, Joober R, Bruce KR, Israel M, Badawi G, Zeramdini N, Sycz L (2012) Dopamine-system genes, childhood abuse, and clinical manifestations in women with Bulimia-spectrum Disorders. J Psychiatr Res 46(9):1139–1145. doi:10.1016/j.jpsychires.2012.05.018
Thaler L, Groleau P, Badawi G, Sycz L, Zeramdini N, Too A, Israel M, Joober R, Bruce KR, Steiger H (2012) Epistatic interactions implicating dopaminergic genes in bulimia nervosa (BN): relationships to eating- and personality-related psychopathology. Prog Neuropsychopharmacol Biol Psychiatry 39(1):120–128. doi:10.1016/j.pnpbp.2012.05.019
Donofry SD, Roecklein KA, Wildes JE, Miller MA, Flory JD, Manuck SB (2014) COMT met allele differentially predicts risk versus severity of aberrant eating in a large community sample. Psychiatry Res. doi:10.1016/j.psychres.2014.08.037
Yilmaz Z, Kaplan AS, Zai CC, Levitan RD, Kennedy JL (2011) COMT Val158Met variant and functional haplotypes associated with childhood ADHD history in women with bulimia nervosa. Prog Neuropsychopharmacol Biol Psychiatry 35(4):948–952. doi:10.1016/j.pnpbp.2011.01.012
Karwautz A, Rabe-Hesketh S, Hu X, Zhao J, Sham P, Collier DA, Treasure JL (2001) Individual-specific risk factors for anorexia nervosa: a pilot study using a discordant sister-pair design. Psychol Med 31(2):317–329
Gabrovsek M, Brecelj-Anderluh M, Bellodi L, Cellini E, Di Bella D, Estivill X, Fernandez-Aranda F, Freeman B, Geller F, Gratacos M, Haigh R, Hebebrand J, Hinney A, Holliday J, Hu X, Karwautz A, Nacmias B, Ribases M, Remschmidt H, Komel R, Sorbi S, Tomori M, Treasure J, Wagner G, Zhao J, Collier DA (2004) Combined family trio and case-control analysis of the COMT Val158Met polymorphism in European patients with anorexia nervosa. Am J Med Genet Part B Neuropsychiatr Genet Off Publ Int Soc Psychiatr Genet 124B(1):68–72. doi:10.1002/ajmg.b.20085
Pinheiro AP, Bulik CM, Thornton LM, Sullivan PF, Root TL, Bloss CS, Berrettini WH, Schork NJ, Kaye WH, Bergen AW, Magistretti P, Brandt H, Crawford S, Crow S, Fichter MM, Goldman D, Halmi KA, Johnson C, Kaplan AS, Keel PK, Klump KL, La Via M, Mitchell JE, Strober M, Rotondo A, Treasure J, Woodside DB (2010) Association study of 182 candidate genes in anorexia nervosa. Am J Med Genet Part B Neuropsychiatr Genet Off Publ Int Soc Psychiatr Genet 153B(5):1070–1080. doi:10.1002/ajmg.b.31082
Brandys MK, Slof-Op’t Landt MC, van Elburg AA, Ophoff R, Verduijn W, Meulenbelt I, Middeldorp CM, Boomsma DI, van Furth EF, Slagboom E, Kas MJ, Adan RA (2012) Anorexia nervosa and the Val158Met polymorphism of the COMT gene: meta-analysis and new data. Psychiatr Genet 22(3):130–136. doi:10.1097/YPG.0b013e328351859e
Illi A, Setala-Soikkeli E, Kampman O, Viikki M, Nuolivirta T, Poutanen O, Huhtala H, Mononen N, Lehtimaki T, Leinonen E (2010) Catechol-O-methyltransferase Val108/158met genotype, major depressive disorder and response to selective serotonin reuptake inhibitors in major depressive disorder. Psychiatry Res 176(1):85–87. doi:10.1016/j.psychres.2009.03.010
Tsao D, Wieskopf JS, Rashid N, Sorge RE, Redler RL, Segall SK, Mogil JS, Maixner W, Dokholyan NV, Diatchenko L (2012) Serotonin-induced hypersensitivity via inhibition of catechol O-methyltransferase activity. Mol Pain 8:25. doi:10.1186/1744-8069-8-25
Schendzielorz N, Mannisto PT, Karayiorgou M, Gogos JA, Raasmaja A (2012) A transient inhibition and permanent lack of catechol-O-methyltransferase have minor effects on feeding pattern of female rodents. Basic Clin Pharmacol Toxicol 110(4):307–313. doi:10.1111/j.1742-7843.2011.00783.x
Lapish CC, Ahn S, Evangelista LM, So K, Seamans JK, Phillips AG (2009) Tolcapone enhances food-evoked dopamine efflux and executive memory processes mediated by the rat prefrontal cortex. Psychopharmacology 202(1–3):521–530. doi:10.1007/s00213-008-1342-1
Gorman LL, O’Hara MW, Figueiredo B, Hayes S, Jacquemain F, Kammerer MH, Klier CM, Rosi S, Seneviratne G, Sutter-Dallay AL, Group T-P (2004) Adaptation of the structured clinical interview for DSM-IV disorders for assessing depression in women during pregnancy and post-partum across countries and cultures. Br J Psychiatry Suppl 46:s17–s23
Fairburn CG, Beglin SJ (1994) Assessment of eating disorders: interview or self-report questionnaire? Int J Eat Disord 16(4):363–370
Vieira-Coelho MA, Soares-da-Silva P (1999) Effects of tolcapone upon soluble and membrane-bound brain and liver catechol-O-methyltransferase. Brain Res 821(1):69–78
Schultz E, Nissinen E, Kaakkola S (1989) Determination of catechol-O-methyltransferase activity in erythrocytes by high performance liquid chromatography with electrochemical detection. Biomed Chromatogr BMC 3(2):64–67. doi:10.1002/bmc.1130030205
Bradford MM (1976) A rapid and sensitive method for the quantitation of microgram quantities of protein utilizing the principle of protein–dye binding. Anal Biochem 72:248–254
Soares-da-Silva P, Parada A, Serrao P (2000) The O-methylated derivative of L-DOPA, 3-O-methyl-L-DOPA, fails to inhibit neuronal and non-neuronal aromatic L-amino acid decarboxylase. Brain Res 863(1–2):293–297
Vieira-Coelho MA, Soares-da-Silva P (1996) Ontogenic aspects of liver and kidney catechol-O-methyltransferase sensitivity to tolcapone. Br J Pharmacol 117(3):516–520
Michaelovsky E, Frisch A, Leor S, Stein D, Danziger Y, Carel C, Fennig S, Mimouni M, Klauck SM, Benner A, Poustka A, Apter A, Weizman A (2005) Haplotype analysis of the COMT–ARVCF gene region in Israeli anorexia nervosa family trios. Am J Med Genet Part B Neuropsychiatr Genet Off Publ Int Soc Psychiatr Genet 139B(1):45–50. doi:10.1002/ajmg.b.30230
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. All applicable international, national, and/or institutional guidelines for the care and use of animals were followed.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Amorim-Barbosa, T., Serrão, M.P., Brandão, I. et al. Catechol-O-methyltransferase activity in erythrocytes from patients with eating disorders. Eat Weight Disord 21, 221–227 (2016). https://doi.org/10.1007/s40519-015-0213-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40519-015-0213-0