
Abstract
Purpose of Review
To provide an updated summary on the field of immunopsychiatry as it pertains to clinical and therapeutic translation in mood disorders (major depressive disorder [MDD] and bipolar disorder [BD]).
Recent Findings
An updated scoping review of a previous publication by Jones et al. identified five recently published RCTs that continue to explore the anti-depressive efficacy of established immunomodulating agents (minocycline, celecoxib, and aspirin). Consistent with our earlier scoping review, study results remain conflicting, and there is still insufficient support for the clinical utility of any anti-inflammatory agent for the treatment of mood disorders.
Summary
Despite extensive evidence supporting a pathophysiological association between inflammatory activation and depressive symptoms, the repurposing of anti-inflammatory agents as novel antidepressant treatments is still an unrealized goal. As highlighted across scoping reviews, published clinical trials remain insensitive to the inherent heterogeneity of patients with mood disorders. We suggest that more nuanced methodological approaches, such as stratification of participants by inflammatory tone or clinical presentation, are required before real translational advances can be made.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Major depressive disorder (MDD) is the single most prevalent mental illness worldwide, affecting 4.4% of the global population and remaining the leading cause of non-fatal disease burden [1, 2]. The consequences of depression are significant, manifesting as a global strain on healthcare systems, workplace productivity, and mortality rates [3, 4]. Though standard treatments have lessened the burden, the clinical heterogeneity across mood disorders is often underemphasized, with key implications for treatment efficacy. Contemporary diagnostic tools such as the ICD-10 and DSM-5 necessitate only one of low mood or anhedonia to diagnose a depressive episode. The remaining seven symptoms, spanning disparate emotional, somatic, and cognitive domains, may be present in any combination, provided there is a minimum of five symptoms overall [5, 6]. Conventional antidepressant treatments for MDD and bipolar disorder (BD) tend to be non-sensitive to this spectrum of clinical presentation, targeting the core symptoms and frequently leaving patients with clinically significant residual symptoms [7]. Large-scale studies demonstrate that, while standard antidepressant treatments are effective for the majority, a substantial subset of patients with so-called treatment-resistant depression (TRD) are unlikely to respond to conventional treatments, embodying a profound clinical need [8, 9]. Pharmacological treatments for depression have remained largely unchanged since the serendipitous discovery of the antidepressant effect of action on the monoamine neurotransmitters in the mid-1990s [10•]. In recent years, researchers have focused on developing and repurposing agents that target alternative pathophysiological mechanisms of depression for those with TRD. One of these pathophysiological mechanisms targeted by novel treatment approaches includes the inflammatory response system [10•].
Inflammation represents the immune system’s defensive response to internal or external injury, elicited by the damage-recognition affinities of host immune cells [11]. With respect to depression, an endemic inflammatory response is thought to arise in part from psychosocial stress, whereby stress-induced monocytes are released from the bone marrow into the bloodstream, where they become quickly activated via their pre-programmed affinity for general microbial- or danger-associated molecular patterns (MAMPs and DAMPs) [12,13,14]. This initially peripheral inflammatory response is relayed to the central immune system via parallel neural, humoral, and cellular pathways (entailing blood–brain-barrier conduction, leukocyte migration, and vagal nerve transmission, respectively) [15,16,17,18]. An association between heightened inflammation and depressive symptoms was first hypothesized in Smith’s 1990 ‘macrophage theory’ of depression, positing that the macrophageal secretion of pro-inflammatory cytokines may cause or worsen a mood episode [19]. This hypothesis has since been strengthened by extensive evidence supporting an epidemiological link between depressive and immune-related disorders, such that diagnosis of conditions including arthritis, multiple sclerosis, and certain cancers infers an increased likelihood of concomitant depression, with the reciprocal risk of comorbid inflammatory disorders in patients with depression similarly demonstrated [20,21,22,23]. Approximated by elevations in peripheral inflammatory markers, most notably C-reactive protein (CRP) and pro-inflammatory cytokines IL-1β, IL-6, and TNF- α, large-scale meta-analyses have consolidated in vivo and post-mortem evidence for inflammatory elevation in depressed patients [24,25,26,27]. Treatment with certain antidepressants both successfully alleviated and pre-emptively inhibited induction of depressive symptoms in complementary trials [28,29,30]. Furthermore, several standard antidepressant medications have demonstrated contingent anti-inflammatory effects in MDD patients, suggesting that these compounds’ antidepressant effects may in part arise from their effects on the immune response [31]. Accordingly, this has led to the exploration of the inflammatory system as a novel treatment target in depression.
In pursuit of effective therapeutic translation, there has also been a significant focus on the biological mechanisms by which inflammation induces depressive symptomatology. Converging evidence from pre-clinical, in vivo, and post-mortem studies points to the role of microglial activation, and the resultant profusion of central pro-inflammatory cytokines, in dysregulating neurotransmitter systems [32••, 33, 34, 35•, 36]. In particular, the inflammation-induced enzyme indoleamine-2, 3-dioxygenase (IDO) disrupts tryptophan catabolism, such that instead of serotonin, it breaks down into kyneurine and thus the NMDA agonist quinolinic acid, resulting in both serotonin depletion and glutamate surplus [37, 38]. Altered glutamate metabolism reduces synaptic plasticity and neurogenesis via downregulation of growth factors [39]. Pro-inflammatory cytokines have additionally demonstrated inhibitory effects on dopamine, disrupting reward circuits and manifesting as key symptoms of depression such as anhedonia and motor retardation [40]. Understanding exactly how inflammatory elevations mediate depressive pathophysiology is key to the successful adaptation of anti-inflammatory agents as a targeted treatment for mood disorders.
In the last two decades, there have been an increasing number of randomized clinical trials (RCTs) investigating the antidepressant efficacy of immunomodulatory agents [10•]. Despite the extensive evidence demonstrating the clinical relevance of inflammation in depression, the utility of anti-inflammatory agents has yet to translate to therapeutic practice. In this review, we will build upon an earlier scoping review in which we synthesized evidence from published RCTs, which investigated the efficacy of anti-inflammatory agents in the treatment of mood disorders. Our aim is to provide an update on the evidence in the field as it applies to clinical and therapeutic translation. In addition, we will highlight studies where researchers have attempted to explore mechanisms of action as it pertains to anti-inflammatory drugs and mood disorders.
Methods and Analysis
The following is an updated scoping review of a previously published review synthesizing the evidence of immunomodulatory agents for the treatment of mood disorders [10•]. The literature was reviewed by searching Medline for clinical trials of immunomodulating agents as monotherapy or as adjunctive treatments for depressive symptoms in both MDD and BD, published from December 2019 to March 2022. Included trials were randomized controlled studies or cross-over trials of an immunomodulating agent which had a placebo or an active comparator arm. Included investigational immunomodulating agents were consistent with those included in the previous review [10•]. Participants in the included trials had to have a diagnosis of MDD or BD as defined by the current DSM or ICD version at the time of publication (i.e. DSM-IV or DSM-V, ICD-10), and only studies reporting depression-rating scales in each treatment arm were included. All studies collected from the searches were independently evaluated against inclusion criteria by two of the review authors (MEK and BDMJ). Data was extracted independently by the two review authors and included a description of participants, intervention and control groups, psychometric data, and outcomes.
Results
The search strategy results yielded five additional clinical trials of anti-inflammatory agents for the treatment of depressive symptoms in MDD and BD. These RCTs are described in detail in Table 1. The trials investigated the utility of the following medications: minocycline, celecoxib (CXB), and aspirin (acetylsalicylic acid; ASA). A summary table of 16 previously reviewed studies, some of which included these agents, is included as supplementary material (see Supplementary Table 1).
Minocycline
Minocycline is a tetracycline antibiotic with known anti-inflammatory properties [41]. At the time of our previous review, there were four published RCTs of minocycline for the treatment of MDD and BD [10•]. Since 2019, there have been an additional three published RCTs investigating the effectiveness of minocycline: two in MDD and one in BD.
A recent 8-week RCT (n = 21) incorporated positron emission tomography (PET) into their investigation of the effects of adjunctive minocycline on depressive symptoms [42]. In addition to their primary outcome measure, reduction of depressive symptoms as measured by the 17-item Hamilton Depression Rating Scale (HDRS-17), the authors concurrently assessed the reduction of translocator protein distribution volume (TSPO VT), a reliable index of microglial activation, in three regions of interest: the prefrontal cortex (PCC), anterior cingulate cortex (ACC), and insula [42]. After the treatment period, there was no significant difference in depressive symptom reduction between the minocycline and placebo groups, and no significant effect of minocycline on TSPO VT in the three regions of interest [42].
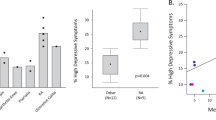
Another RCT-randomized 39 MDD patients with biochemical evidence of low-grade inflammation (baseline CRP ≥ 1 mg/L) to standard antidepressant treatment augmented with either minocycline (200 mg/day) or placebo [43••]. The primary outcome (reduction in HDRS-17) did not show a significant difference between the minocycline and placebo groups. However, after stratification of patients into high-grade or low-grade inflammation (CRP levels < 3 mg/L or ≥ 3 mg/L), there was a significant difference in HDRS-17 reduction in patients with high-grade baseline inflammation (CRP ≥ 3 mg/L) who received minocycline compared with all other groups [43••].
Husain et al. (2020) conducted a 4 × 4 factorial design RCT in adult BD patients with a current major depressive episode. Participants were randomized to one of four arms: minocycline and CXB; minocycline and placebo; CXB and placebo; or placebo and placebo [44]. Assessed on the HDRS-17, there was no significant difference in depressive symptom reduction between the four groups, nor was there a significant treatment effect of either agent alone, or in combination [44]. The study did not recruit based upon inflammatory status but did assess for changes in inflammatory markers throughout the treatment period; post hoc analyses showed that the sample had high rates of inflammation overall (median CRP = 4 mg/L). No treatment arm had a significant effect on CRP or white blood cell level [45].
Celecoxib
Celecoxib (CXB) is a nonsteroidal anti-inflammatory drug that has been extensively investigated for the treatment of mood disorders [10•]. In our previous review, we synthesized four studies of CXB in MDD and none in BD (Supplemental Table 1). In the present updated search, we identified one additional published RCT of CXB in BD. This 10-week trial randomized 47 adults with BD I or II to treatment with either escitalopram and CXB or escitalopram and placebo [46]. Results demonstrated significantly higher treatment response rates (defined as a 50% reduction in HDRS-17 score from baseline) and significantly higher remission rates (final HDRS-17 score ≤ 7) in the CXB group compared to placebo. HDRS-17 scores were significantly lower in the CXB group compared to those in the placebo as early as 1 week into the 10-week trial [46]. Edberg et al. (2020) conducted a secondary analysis of the same RCT, assessing levels of the inflammatory mediator monocyte chemoattractant protein-1 (MCP-1) throughout the treatment period, and found that baseline inflammatory status did not predict response to CXB in this sample [47]. There were no significant differences in MCP-1 levels between the CXB and placebo groups at baseline or at week 8 (p = 0.209, p = 0.054). However, the authors did find some evidence for a negative correlation between MCP-1 elevation and depression, as week 8 MCP-1 was significantly lower in treatment non-responders across the entire sample (p = 0.014) [47].
Aspirin
Aspirin, commonly known as acetylsalicylic acid (ASA), is frequently used to treat inflammatory physical health conditions [48]. In our previous review, we identified two RCTs that investigated the efficacy of ASA in BD (Supplemental Table 1). Since our group’s 2020 review, there has been one additional published RCT investigating ASA for depression. This moderate-size trial (n = 130) randomized 15–25-year-olds with MDD to receive either ASA, the anti-inflammatory rosuvastatin, or placebo, in addition to their treatment as usual (TAU) [49, 50]. As measured by the Montgomery Asberg Depression Rating Scale (MADRS), there was no significant difference in response and remission rates, nor in depressive symptom reduction, in either treatment arm compared to placebo [50]. There was some evidence for the superiority of rosuvastatin vs. ASA, with a significantly greater MADRS reduction observed at both week 12 (p = 0.017) and 26-week follow-up (p = 0.035). Compared to the ASA group, participants in the rosuvastatin group also demonstrated better outcomes on secondary scales at week 12 (Clinical Global Impressions scale; CGI-S, Negative problems Orientation Questionnaire; NPOQ).
Discussion
During the last decade, there has been increasing interest in repurposing immunomodulatory agents for the treatment of mood disorders. We previously synthesized evidence from RCTs of these agents in adults with MDD and BD [10•]. The current scoping review provides an update on evidence from published RCTs and identified five additional RCTs of anti-inflammatory agents that met our predefined inclusion criteria. The findings from these studies were conflicting, highlighting the heterogeneity of mood disorders, and the need for more nuanced approaches in clinical trial design.
It is unlikely that immunomodulatory agents have antidepressant effects for all individuals with depressive symptoms. Though the literature indicates that depressive symptoms may be associated with low-grade inflammation, evidence suggests this might only be applicable to a subgroup of clinically depressed patients. Trials demonstrate that depressed patients with higher inflammatory responses may experience increased symptom severity and chronicity, as well as non-response to standard antidepressant agents [51•, 52,53,54,55,56,57, 58•, 59••, 60, 61]. Pertinent to therapeutic translation, studies indicate that peripheral biomarkers such as CRP, interleukin (IL)-6, and tumour necrosis factor (TNF) may be elevated in treatment-resistant subgroups and that antidepressant effects of anti-inflammatory agents are more likely in individuals exhibiting elevated inflammation pre-treatment [43••, 62,63,64]. This data suggests a distinct pathophysiological basis underlying standard treatment non-response in a subgroup of patients. Interestingly, a significant proportion of this treatment-resistant subgroup of patients exhibit atypical, neurovegetative depressive symptoms such as fatigue, appetite increase, increased pain response, and anhedonia; a phenotypic cluster coined ‘sickness behavior’ due to its high incidence during inflammatory activation [65, 66••, 67]. A recent study found significantly elevated inflammatory markers in a neurovegetative subtype of patients compared to five alternate depressive subtypes (mean CRP 4.2 mg/L), with neurovegetative symptoms mediating the association between CRP and other symptoms of depression such as cognitive or emotional features [68••]. Given the clinical heterogeneity previously referenced, the clustering of inflammation-linked depressive symptoms in a distinct treatment-resistant subgroup suggests the unique utility of anti-inflammatory agents for patients with these specific symptom subsets.
A reliable biomarker for the identification of an ‘inflamed’ subgroup of mood disorder patients remains elusive. For example, in the study by Edberg et al., adjunctive response to CXB in bipolar depression was associated with changes in MCP-1, while Husain et al. found that CXB was not associated with change in CRP or treatment response [44, 47]. The discrepancy may be related to differential associations of inflammatory markers and clinical characteristics in the patient population as previously postulated [45, 61]. Though minocycline has a purported antidepressant and established anti-inflammatory effect, the present review found one study indicating elevated CRP was associated with a favorable antidepressant response while another two failed to show a reduction in sophisticated markers of neuroinflammation [42, 43••, 44, 69]. This evinces a major methodological challenge in stratifying participants to an anti-inflammatory agent on the basis of pre-treatment inflammatory status in future clinical trials. While studies have attempted to recruit and conduct post hoc analyses on patients with biochemical evidence of a reactive immune system, there is currently no reliable way to do so. As previously described, authors have attempted to utilize peripheral inflammatory biomarkers as well as phenotypic indicators of inflammation with mixed success. An approach to mitigate the heterogeneity of inflammatory markers may be to utilize composite scores of inflammatory markers to create an ‘index’ of an inflammatory profile, relying on multiple markers of inflammation, rather than a single measure [70, 71]. Utilization of central biomarkers of inflammation such as positron emission tomography (PET) imaging and cerebrospinal fluid (CSF) markers; or upstream regulators (e.g. regulatory T cells; Tregs) of inflammation may also be more reliable markers of inflammation related to mood disorders [72, 73]. We encourage future research in pursuit of reliable and pragmatic biomarkers that may be used to identify patients who might best respond to immunomodulatory agents.
A further explanation for the conflicting findings from RCTs of anti-inflammatory agents is the prevalent and large placebo response observed in trials recruiting mood disorder patients [74]. Several of the trials reviewed above have clinically significant effect sizes but fail to separate from placebo. While the exact mechanism of the placebo response is unclear, recent evidence suggests associations with the immune system. For example, a recent PET study found that analgesic placebo led to a reduction in pro-inflammatory cytokine IL-18, which was correlated with pain reduction [75]. If the suspected mechanism of antidepressant action of repurposed anti-inflammatories is the attenuation of an activated inflammatory response, a comparison with placebo, which may have its own anti-inflammatory effects, may negate otherwise positive trials.
The specific anti-inflammatory drug and dosage utilized is another factor that may explain conflicting findings from current RCTs. It is unclear whether dosages used in currently published trials are sufficient to reduce neuroinflammation. A recent study investigating the efficacy of minocycline 100 mg BID for adults with MDD found that despite being clinically effective in other inflammatory physical health conditions, the 200 mg daily dosage did not reduce central markers of neuroinflammation nor did it reduce depressive symptoms [42]. Minocycline, like several other repurposed anti-inflammatories trialed in mood disorders, has non-specific anti-inflammatory effects, which may or may not lead to a reduction in inflammatory processes related to depression. Future work should investigate agents that have more direct and specific actions on the immune system. We are aware of at least one clinical trial investigating a novel agent that blocks the P2X7 receptor, which plays a key role in the release of inflammatory cytokines (NCT04116606). Results of this and other trials of direct cytokine inhibitors will be important contributions to the current evidence on the safety and efficacy of targeting the inflammatory response system to treat depression.
Conclusions
The growing field of immunopsychiatry suggests that immunomodulatory agents may one day play a role in the treatment of a subset of depressed individuals. However, studies highlighted in this updated review continue to display conflicting results, likely due to the continued inclusion of heterogeneous patients in contemporary clinical trials. To accelerate clinical translation of these repurposed agents, future studies need to move towards a stratified design while assessing agents with specific anti-inflammatory actions. Future immunomodulatory RCT designs should specifically target individuals with biochemical or phenotypical evidence of an aberrant inflammatory response, integrated with specific depressive symptom subsets that are suggested as epiphenomenon of an activated immune response. Without these more nuanced approaches, there will be limited advances in immunopsychiatry, and repurposed anti-inflammatory agents are unlikely to translate to efficacious treatment algorithms for mood disorders.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
World Health Organization. Depression and Other Common Mental Disorders: Global Health Estimates. World Health Organization, 2017.
Liu Q, He H, Yang J, Feng X, Zhao F, Lyu J. Changes in the global burden of depression from 1990 to 2017: Findings from the Global Burden of Disease study. J Psychiatr Res. 2020;126:134–40.
Greenberg PE, Fournier AA, Sisitsky T, Simes M, Berman R, Koenigsberg SH, et al. The economic burden of adults with major depressive disorder in the United States (2010 and 2018). Pharmacoeconomics. 2021;39(6):653–65.
Cuijpers P, Vogelzangs N, Twisk J, Kleiboer A, Li J, Penninx BW. Comprehensive meta-analysis of excess mortality in depression in the general community versus patients with specific illnesses. Am J Psychiatry. 2014;171(4):453–62.
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5). American Psychiatric Association, 2013.
World Health Organization. The ICD-10 Classification of Mental and Behavioural Disorders Clinical Descriptions and Diagnostic Guidelines. WHO, 1992.
Kennedy SH. Core symptoms of major depressive disorder: relevance to diagnosis and treatment. Dialogues Clin Neurosci. 2008;10(3):271–7.
Rush AJ, Trivedi MH, Wisniewski SR, Nierenberg AA, Stewart JW, Warden D, et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D report. Am J Psychiatry. 2006;163(11):1905–17.
Warden D, Rush AJ, Trivedi MH, Fava M, Wisniewski SR. The STAR*D Project results: a comprehensive review of findings. Curr Psychiatry Rep. 2007;9(6):449–59.
Jones BDM, Daskalakis ZJ, Carvalho AF, Strawbridge R, Young AH, Mulsant BH, et al. Inflammation as a treatment target in mood disorders: review. BJPsych Open. 2020;6(4): e60. A scoping review of published RCTs in the field of immunopsychiatry from inception to 2019, to which the present review serves as an update.
Parkin J, Cohen B. An overview of the immune system. Lancet. 2001;357(9270):1777–89.
Berk M, Williams LJ, Jacka FN, O’Neil A, Pasco JA, Moylan S, et al. So depression is an inflammatory disease, but where does the inflammation come from? BMC Med. 2013;11:200.
Fleshner M. Stress-evoked sterile inflammation, danger associated molecular patterns (DAMPs), microbial associated molecular patterns (MAMPs) and the inflammasome. Brain Behav Immun. 2013;27(1):1–7.
Rivest S. Molecular insights on the cerebral innate immune system. Brain Behav Immun. 2003;17(1):13–9.
D’Mello C, Le T, Swain MG. Cerebral microglia recruit monocytes into the brain in response to tumor necrosis factorα signaling during peripheral organ inflammation. J Neurosci. 2009;29(7):2089–102.
Hansen MK, Taishi P, Chen Z, Krueger JM. Vagotomy blocks the induction of interleukin-1beta (IL-1beta) mRNA in the brain of rats in response to systemic IL-1beta. J Neurosci. 1998;18(6):2247–53.
Miller AH, Haroon E, Felger JC. Therapeutic implications of brain-immune interactions: treatment in translation. Neuropsychopharmacology. 2017;42(1):334–59.
Banks WA. The blood-brain barrier in neuroimmunology: tales of separation and assimilation. Brain Behav Immun. 2015;44:1–8.
Smith RS. The macrophage theory of depression. Med Hypotheses. 1991;35(4):298–306.
Beurel E, Toups M, Nemeroff CB. The bidirectional relationship of depression and inflammation: double trouble. Neuron. 2020;107(2):234–56.
Rosenblat JD, McIntyre RS. Are medical comorbid conditions of bipolar disorder due to immune dysfunction? Acta Psychiatrica Scandanavia. 2015;132(3):180–91.
Evans DL, Charney DS, Lewis L, Golden RN, Gorman JM, Krishnan KR, et al. Mood disorders in the medically ill: scientific review and recommendations. Biol Psychiatry. 2005;58(3):175–89.
Gold SM, Köhler-Forsberg O, Moss-Morris R, Mehnert A, Miranda JJ, Bullinger M, et al. Comorbid depression in medical diseases. Nat Rev Dis Primers. 2020;6(1):69.
Enache D, Pariante CM, Mondelli V. Markers of central inflammation in major depressive disorder: a systematic review and meta-analysis of studies examining cerebrospinal fluid, positron emission tomography and post-mortem brain tissue. Brain Behav Immun. 2019;81:24–40.
Köhler CA, Freitas TH, Maes M, de Andrade NQ, Liu CS, Fernandes BS, et al. Peripheral cytokine and chemokine alterations in depression: a meta-analysis of 82 studies. Acta Psychiatrica Scandanavia. 2017;135(5):373–87.
Dowlati Y, Herrmann N, Swardfager W, Liu H, Sham L, Reim EK, et al. A meta-analysis of cytokines in major depression. Biol Psychiatry. 2010;67(5):446–57.
Haapakoski R, Mathieu J, Ebmeier KP, Alenius H, Kivimaki M. Cumulative meta-analysis of interleukins 6 and 1β, tumour necrosis factor α and C-reactive protein in patients with major depressive disorder. Brain Behav Immun. 2015;49:206–15.
Shen Y, Connor TJ, Nolan Y, Kelly JP, Leonard BE. Differential effect of chronic antidepressant treatments on lipopolysaccharide-induced depressive-like behavioural symptoms in the rat. Life Sci. 1999;65(17):1773–86.
Kubera M, Simbirtsev A, Mathison R, Maes M. Effects of repeated fluoxetine and citalopram administration on cytokine release in C57BL/6 mice. Psychiatry Res. 2000;96(3):255–66.
Baraldi S, Hepgul N, Mondelli V, Pariante CM. Symptomatic treatment of interferon-α-induced depression in hepatitis C: a systematic review. J Clin Psychopharmacol. 2012;32(4):531–43.
Hannestad J, DellaGioia N, Bloch M. The effect of antidepressant medication treatment on serum levels of inflammatory cytokines: a meta-analysis. Neuropsychopharmacology. 2011;36(12):2452–9.
Drevets WC, Wittenberg GM, Bullmore ET, Manji HK. Immune targets for therapeutic development in depression: towards precision medicine. Nat Rev Drug Discov. 2022;21(3):224–44. A comprehensive review of evidence linking inflammatory elevation to MDD, including purported biological mechanisms.
Li Q, Barres BA. Microglia and macrophages in brain homeostasis and disease. Nat Rev Immunol. 2018;18(4):225–42.
Meyer JH, Cervenka S, Kim MJ, Kreisl WC, Henter ID, Innis RB. Neuroinflammation in psychiatric disorders: PET imaging and promising new targets. Lancet Psychiatry. 2020;7(12):1064–74.
Giridharan VV, Sayana P, Pinjari OF, Ahmad N, da Rosa MI, Quevedo J, et al. Postmortem evidence of brain inflammatory markers in bipolar disorder: a systematic review. Mol Psychiatry. 2020;25(1):94–113. A systematic review of post-mortem data evaluating markers of brain inflammation in BD.
Csölle C, Baranyi M, Zsilla G, Kittel A, Gölöncsér F, Illes P, et al. Neurochemical changes in the mouse hippocampus underlying the antidepressant effect of genetic deletion of P2X7 receptors. PLoS ONE. 2013;8(6):e66547.
Delgado PL, Price LH, Miller HL, Salomon RM, Aghajanian GK, Heninger GR, et al. Serotonin and the neurobiology of depression. Effects of tryptophan depletion in drug-free depressed patients. Arch Gen Psychiatry. 1994;51(11):865–74.
Parrott JM, Redus L, Santana-Coelho D, Morales J, Gao X, O’Connor JC. Neurotoxic kynurenine metabolism is increased in the dorsal hippocampus and drives distinct depressive behaviors during inflammation. Transl Psychiatry. 2016;6(10):e918.
Shimizu E, Hashimoto K, Okamura N, Koike K, Komatsu N, Kumakiri C, et al. Alterations of serum levels of brain-derived neurotrophic factor (BDNF) in depressed patients with or without antidepressants. Biol Psychiatry. 2003;54(1):70–5.
Felger JC. The role of dopamine in inflammation-associated depression: mechanisms and therapeutic implications. Curr Top Behav Neurosci. 2017;31:199–219.
Maes M, Yirmyia R, Noraberg J, Brene S, Hibbeln J, Perini G, et al. The inflammatory & neurodegenerative (I&ND) hypothesis of depression: leads for future research and new drug developments in depression. Metab Brain Dis. 2009;24(1):27–53.
Attwells S, Setiawan E, Rusjan PM, Xu C, Kish SJ, Vasdev N, et al. A double-blind placebo-controlled trial of minocycline on translocator protein distribution volume in treatment-resistant major depressive disorder. Transl Psychiatry. 2021;11(1):334.
Nettis MA, Lombardo G, Hastings C, Zajkowska Z, Mariani N, Nikkheslat N, et al. Augmentation therapy with minocycline in treatment-resistant depression patients with low-grade peripheral inflammation: results from a double-blind randomised clinical trial. Neuropsychopharmacology. 2021;46(5):939–48. A recent RCT demonstrating the significance of baseline inflammatory tone when evaluating the anti-depressive effects of immunomodulating agents.
Husain MI, Chaudhry IB, Khoso AB, Husain MO, Hodsoll J, Ansari MA, et al. Minocycline and celecoxib as adjunctive treatments for bipolar depression: a multicentre, factorial design randomised controlled trial. The Lancet Psychiatry. 2020;7(6):515–27.
Kloiber S, Jones BDM, Hodsoll J, Chaudhry IB, Khoso AB, Husain MO, et al. Metabolic function in patients with bipolar depression receiving anti-inflammatory agents: Findings from the MINDCARE study, a multicentre, randomised controlled trial. J Affect Disord. 2022;299:135–41.
Halaris A, Cantos A, Johnson K, Hakimi M, Sinacore J. Modulation of the inflammatory response benefits treatment-resistant bipolar depression: a randomized clinical trial. J Affect Disord. 2020;261:145–52.
Edberg D, Hoppensteadt D, Walborn A, Fareed J, Sinacore J, Halaris A. Plasma MCP-1 levels in bipolar depression during cyclooxygenase-2 inhibitor combination treatment. J Psychiatr Res. 2020;129:189–97.
Morgan G. The established and emerging uses of aspirin. Basic Clin Pharmacol Toxicol. 2006;99(4):283–6.
Gomez-Garcia A, Martinez Torres G, Ortega-Pierres LE, Rodriguez-Ayala E, Alvarez-Aguilar C. Rosuvastatin and metformin decrease inflammation and oxidative stress in patients with hypertension and dyslipidemia. Rev Esp Cardiol. 2007;60(12):1242–9.
Berk M, Mohebbi M, Dean OM, Cotton SM, Chanen AM, Dodd S, et al. Youth Depression Alleviation with Anti-inflammatory Agents (YoDA-A): a randomised clinical trial of rosuvastatin and aspirin. BMC Med. 2020;18(1):16.
Yang C, Wardenaar KJ, Bosker FJ, Li J, Schoevers RA. Inflammatory markers and treatment outcome in treatment resistant depression: A systematic review. J Affect Disord. 2019;257:640–9. A systematic review of identified peripheral inflammatory markers and their respective utility in predicting treatment response in depression.
Chamberlain SR, Cavanagh J, de Boer P, Mondelli V, Jones D, Drevets WC, et al. Treatment-resistant depression and peripheral C-reactive protein. Br J Psychiatry. 2019;214(1):11–9.
Arteaga-Henríquez G, Simon MS, Burger B, Weidinger E, Wijkhuijs A, Arolt V, et al. Low-Grade Inflammation as a Predictor of Antidepressant and Anti-Inflammatory Therapy Response in MDD Patients: a Systematic Review of the Literature in Combination With an Analysis of Experimental Data Collected in the EU-MOODINFLAME Consortium. Front Psychiatry. 2019;10:458.
Uher R, Tansey KE, Dew T, Maier W, Mors O, Hauser J, et al. An inflammatory biomarker as a differential predictor of outcome of depression treatment with escitalopram and nortriptyline. Am J Psychiatry. 2014;171(12):1278–86.
Haroon E, Daguanno AW, Woolwine BJ, Goldsmith DR, Baer WM, Wommack EC, et al. Antidepressant treatment resistance is associated with increased inflammatory markers in patients with major depressive disorder. Psychoneuroendocrinology. 2018;95:43–9.
Lanquillon S, Krieg JC, Bening-Abu-Shach U, Vedder H. Cytokine production and treatment response in major depressive disorder. Neuropsychopharmacology. 2000;22(4):370–9.
Strawbridge R, Arnone D, Danese A, Papadopoulos A, HeraneVives A, Cleare AJ. Inflammation and clinical response to treatment in depression: A meta-analysis. Eur Neuropsychopharmacol. 2015;25(10):1532–43.
Liu JJ, Wei YB, Strawbridge R, Bao Y, Chang S, Shi L, et al. Peripheral cytokine levels and response to antidepressant treatment in depression a systematic review and meta-analysis. Mol Psychiatry. 2020;25(2):339–50. A recent review evaluating the role of inflammatory cytokines in anti-depressant response.
Lynall ME, Turner L, Bhatti J, Cavanagh J, de Boer P, Mondelli V, et al. Peripheral blood cell-stratified subgroups of inflamed depression. Biol Psychiatry. 2020;88(2):185–96. A paper suggesting distinct immunophenotypes in depression, with implications for symptom severity.
Chen Y, Jiang T, Chen P, Ouyang J, Xu G, Zeng Z, et al. Emerging tendency towards autoimmune process in major depressive patients: a novel insight from Th17 cells. Psychiatry Res. 2011;188(2):224–30.
Xue S, Hodsoll J, Khoso AB, Husain MO, Chaudhry IB, Young AH, et al. Suicidality in patients with bipolar depression: findings from a lower middle-income country. J Affect Disord. 2021;289:1–6.
Raison CL, Rutherford RE, Woolwine BJ, Shuo C, Schettler P, Drake DF, et al. A randomized controlled trial of the tumor necrosis factor antagonist infliximab for treatment-resistant depression: the role of baseline inflammatory biomarkers. JAMA Psychiat. 2013;70(1):31–41.
Porcu M, Urbano MR, Verri WA Jr, Barbosa DS, Baracat M, Vargas HO, et al. Effects of adjunctive N-acetylcysteine on depressive symptoms: modulation by baseline high-sensitivity C-reactive protein. Psychiatry Res. 2018;263:268–74.
Savitz JB, Teague TK, Misaki M, Macaluso M, Wurfel BE, Meyer M, et al. Treatment of bipolar depression with minocycline and/or aspirin: an adaptive, 2×2 double-blind, randomized, placebo-controlled, phase IIA clinical trial. Transl Psychiatry. 2018;8(1):27.
Dantzer R, O’Connor JC, Freund GG, Johnson RW, Kelley KW. From inflammation to sickness and depression: when the immune system subjugates the brain. Nat Rev Neurosci. 2008;9(1):46–56.
Milaneschi Y, Lamers F, Berk M, Penninx BWJH. Depression heterogeneity and its biological underpinnings: toward immunometabolic depression. Biol Psychiatry. 2020;88(5):369–80. A review article linking immune dysregulation to atypical symptoms of depression, suggesting a subgroup of patients for whom novel biological targets are particularly indicated.
Simmons WK, Burrows K, Avery JA, Kerr KL, Taylor A, Bodurka J, et al. Appetite changes reveal depression subgroups with distinct endocrine, metabolic, and immune states. Mol Psychiatry. 2020;25(7):1457–68.
Franklyn SI, Stewart J, Beaurepaire C, Thaw E, McQuaid RJ. Developing symptom clusters: linking inflammatory biomarkers to depressive symptom profiles. Transl Psychiatry. 2022;12(1):133. A recent cluster analysis suggesting inflammatory elevation is uniquely implicated in neurovegetative symptoms as compared to other symptoms of depression, suggesting a subgroup of patients for which immunomodulating agents may be clinically relevant.
Husain MI, Strawbridge R, Stokes PR, Young AH. Anti-inflammatory treatments for mood disorders: systematic review and meta-analysis. J Psychopharmacol. 2017;31(9):1137–48.
Beydoun MA, Obhi HK, Weiss J, Canas JA, Beydoun HA, Evans MK, Zonderman AB. Systemic inflammation is associated with depressive symptoms differentially by sex and race: a longitudinal study of urban adults. Mol Psychiatry. 2020 Jun;25(6)
Chen Y, Jin M, Shao Y, Xu G. Prognostic value of the systemic inflammation response index in patients with adenocarcinoma of the oesophagogastric junction: a propensity score-matched analysis. Dis Markers. 2019 Nov 4
Ellul P, Mariotti-Ferrandiz E, Leboyer M, Klatzmann D. Regulatory T cells as supporters of psychoimmune resilience: toward immunotherapy of major depressive disorder. Front Neurol. 2018;20(9):167.
Enache D, Pariante CM, Mondelli V. Markers of central inflammation in major depressive disorder: a systematic review and meta-analysis of studies examining cerebrospinal fluid, positron emission tomography and post-mortem brain tissue. Brain Behav Immun. 2019
Jones BDM, Razza LB, Weissman CR, Karbi J, Vine T, Mulsant LS, Brunoni AR, Husain MI, Mulsant BH, Blumberger DM, Daskalakis ZJ. Magnitude of the placebo response across treatment modalities used for treatment-resistant depression in adults: a systematic review and meta-analysis. JAMA Netw Open. 2021 Sep 1;4(9)
Müller N, Schwarz MJ, Dehning S, Douhe A, Cerovecki A, Goldstein-Müller B, et al. The cyclooxygenase-2 inhibitor celecoxib has therapeutic effects in major depression: results of a double-blind, randomized, placebo controlled, add-on pilot study to reboxetine. Mol Psychiatry. 2006;11:680–4.
Akhondzadeh S, Jafari S, Raisi F, Nasehi AA, Ghoreishi A, Salehi B, et al. Clinical trial of adjunctive celecoxib treatment in patients with major depression: a double blind and placebo controlled trial. Depress Anxiety. 2009;26:607–11.
Abbasi SH, Hosseini F, Modabbernia A, Ashrafi M, Akhondzadeh S. Effect of celecoxib add-on treatment on symptoms and serum IL-6 concentrations in patients with major depressive disorder: randomized double-blind placebo controlled study. J Affect Disord. 2012;141:308–14.
Majd M, Hashemian F, Hosseinib SM, Shariatpanahi MV, Sharifid A. A randomized, doubleblind, placebo-controlled trial of celecoxib augmentation of sertraline in treatment of drug-naive depressed women: a pilot study. Iran J Pharm Res. 2015;14:891–9.
McIntyre RS, Subramaniapillai M, Lee Y, Pan Z, Carmona NE, Shekotikhina M, et al. Efficacy of adjunctive infliximab vs placebo in the treatment of adults with bipolar I/II depression: a randomized clinical trial. JAMA Psychiat. 2019;76:783–90.
Emadi-Kouchak H, Mohammadinejad P, Asadollahi-Amin A, Rasoulinejad M, Zeinoddini A, Yalda A, et al. Therapeutic effects of minocycline on mild-to-moderate depression in HIV patients: a double-blind, placebo-controlled, randomized trial. Int Clin Psychopharmacol. 2016;31:20–6.
Husain MI, Chaudhry IB, Husain N, Khoso AB, Rahman RR, Hamirani MM, et al. Minocycline as an adjunct for treatment-resistant depressive symptoms: a pilot randomised placebo-controlled trial. J Psychopharmacol. 2017;31:1166–75.
Dean OM, Kanchanatawan B, Ashton M, Mohebbi M, Ng CH, Maes M, et al. Adjunctive minocycline treatment for major depressive disorder: a proof of concept trial. Aust N Z J Psychiatry. 2017;51:829–40.
Berk M, Dean OM, Cotton SM, Jeavons S, Tanious M, Kohlmann K, et al. The efficacy of adjunctive N-acetylcysteine in major depressive disorder. J Clin Psychiatry. 2014;75:628–36.
Berk M, Copolov DL, Dean O, Lu K, Jeavons S, Schapkaitz I, et al. N-Acetyl cysteine for depressive symptoms in bipolar disorder–a double-blind randomized placebo-controlled trial. Biol Psychiatry. 2008;64:468–75.
Bauer IE, Green C, Colpo GD, Teixeira AL, Selvaraj S, Durkin K, et al. A double blind, randomized, placebo-controlled study of aspirin and N-acetylcysteine as adjunctive treatments for bipolar depression. J Clin Psychiatry. 2019;80:1.
Ellegaard PK, Licht RW, Nielsen RE, Dean OM, Berk M, Poulsen HE, et al. The efficacy of adjunctive N-acetylcysteine in acute bipolar depression: a randomized placebo-controlled study. J Affect Disord. 2019;245:1043–51.
Berk M, Turner A, Malhi GS, Ng C, Cotton SM, Dodd S, et al. A randomised controlled trial of a mitochondrial therapeutic target for bipolar depression: mitochondrial agents, N-acetylcysteine, and placebo. BMC Med. 2019;17:18.
Author information
Authors and Affiliations
Contributions
All authors contributed to the review, conception, and design. Mary E. Kittur conducted the literature review, data collection and analysis, and original draft preparation with continued revision. Additional literature review and critical revision of the manuscript were performed by Brett D. M. Jones and corresponding author M. Ishrat Husain. Nasia Dai and Mariam Mahboob contributed to the literature review and data collection. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of Interest
Mary E. Kittur declares that she has no conflict of interest.
Brett D. M. Jones declares that he has no conflict of interest.
Nasia Dai declares that she has no conflict of interest.
Mariam Mahboob declares that she has no conflict of interest.
Muhammad I. Husain declares that he has no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Kittur, M.E., Jones, B.D.M., Dai, N. et al. Repurposing Anti-inflammatory Agents for Mood Disorders: an Updated Review of Current Evidence. Curr Treat Options Psych 9, 346–362 (2022). https://doi.org/10.1007/s40501-022-00267-1
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40501-022-00267-1