
Abstract
Purpose
Ultrasound is commonly used to measure changes in skeletal muscle morphology in response to both acute and chronic resistance exercise, but little is known on how muscle stiffness changes via ultrasound elastography, which was the purpose of this systematic review and meta-analysis.
Methods
The online data bases of Pubmed, Scopus, and Web of Science were each searched up until February 2020 and the data were analyzed using a random effects model.
Results
A total of eight studies (four acute and four chronic) met the inclusion criteria for the quantitative analysis. Following a single bout of exercise, muscle stiffness was increased within the first hour [ES: 1.52 (95% CI 0.14, 2.91); p = 0.031], but was no longer elevated when measured 2 days post-exercise [ES: 0.76 (95% CI − 0.32, 1.83); p = 0.16] or ≥ 7 days post-exercise [ES: 0.20 (95% CI − 0.53, 0.94); p = 0.58]. There was no impact of long-term resistance training on changes in muscle stiffness [ES: − 0.04 (95% CI − 0.24, 0.15); p = 0.653].
Conclusion
The primary findings from this meta-analysis indicate that muscle stiffness increases acutely following a single bout of resistance exercise, but does not change long-term with chronic resistance training when measured via ultrasound shear elastography. Given the small number of studies included in this review, future studies may wish to examine changes in muscle stiffness in response to both acute and chronic resistance exercise.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Ultrasound measurements of elastography allow for the assessment of tissue stiffness via either shear or strain elastography. Strain elastography examines tissue deformation in response to external pressure applied by the ultrasound technician; whereas, shear elastography evaluates the speed at which shear waves from the ultrasound probe travel [1]. While this technique is commonly used to assess different types of cancers and liver diseases [1], it is gaining more frequent use as a measure performed in skeletal muscle in response to resistance exercise. Traditional measures of skeletal muscle stiffness involved assessments of resting joint angles [2], forces required to lengthen muscles [2], palpations [3], myometer assessments [4], and subjective rating scales [5], but ultrasound measured elastography [6] allows for a visualization and objective measure of the muscle being assessed. Furthermore, the use of ultrasound provides a more portable and less expensive modality of assessment in comparison to magnetic resonance elastography [7] and ultrasound is already commonly used for the assessment of muscle size and morphology. This review examines the ability of ultrasound elastography to detect acute and chronic changes in muscle stiffness that occur with resistance exercise, and the direction, magnitude, and implications of these potential changes.
Ultrasound is often used to measure acute changes that occur in response to resistance exercise by examining numerous variables such as pennation angle, blood flow, echo-intensity, and muscle thickness [8]. While muscle stiffness is often examined as a measure of acute exercise-induced muscle damage, this measure is not commonly performed using ultrasound. Given the objective and non-invasive nature of ultrasound measures, this may provide an ideal avenue for assessing acute changes in muscle stiffness that are present following damaging resistance exercise. Furthermore, little is known on how muscle stiffness changes following a more traditional bout of exercise not intended to induce muscle damage, and whether this can be detected by ultrasound elastography. It can be hypothesized that tissue stiffness may increase given cell swelling and increases in tissue pressure, but evidence in this area is lacking.
In addition to examining acute changes in muscle stiffness, it may also be important to understand chronic changes in muscle stiffness that occur following a resistance training program. It has previously been shown that stiffer muscles are stronger muscles even after adjusting for the amount of muscle mass present, and therefore, muscle stiffness was hypothesized to be a potential measure of muscle quality such that a stiffer muscle was a higher quality muscle [9]. Support for this hypothesis exists in that muscle stiffness has been shown to be inversely correlated with intramuscular fat [10]. As resistance exercise would be expected to improve muscle quality, one may hypothesize that muscle stiffness may increase as a result of resistance exercise. It would also seem reasonable to hypothesize that a change in muscle stiffness may have a relationship with overall injury risk, which may be particularly important for athletic populations. Despite its potential importance, the effects of chronic resistance exercise on changes in passive muscle stiffness are largely unknown. Given the increasing use of ultrasound to assess changes in both acute and chronic muscle stiffness occurring in response to resistance exercise, a systematic review and meta-analysis were performed to synthesize the current information. The purpose of this review was to examine the acute and chronic changes in muscle stiffness as detected by ultrasound measured shear wave elastography.
Materials and methods
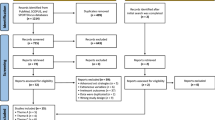
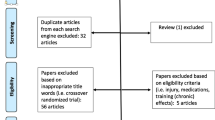
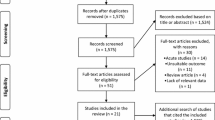
The online data bases of Pubmed, Scopus, and Web of Science were each searched using the following search terms: (1) “elastography” and “resistance exercise” (2) “elastography” and “weight lifting”; (3) “elastography” and “strength training”; (4) “muscle stiffness” and “resistance exercise” (5) “muscle stiffness” and “weight lifting” and (6) “muscle stiffness” and “strength training” up until February 2020. References of the included articles were also searched for additional articles to include in the quantitative meta-analysis. A flow chart showing the included studies is detailed in Fig. 1. For studies to be included in the quantitative meta-analysis, they had to meet the following criteria: (1) must be performed in humans; (2) must be written in English; and (3) must include an ultrasound measure of shear wave muscle stiffness before and after a single training session or chronic training intervention.

Flow chart detailing search results and rationale for excluding studies
Effect sizes are expressed in the raw units (meters per second) by which the measurements were taken and they were analyzed using a within group effect size (post measure–pre measure) to determine if changes in muscle stiffness were present. Each of the studies were weighted using the inverse of the sample variance with the variability taken from the change score (i.e., the variability of the intervention itself) [11]. The effect sizes represent the change in ultrasound shear wave speed (i.e., muscle stiffness) and the variability of this change [11]. In the event that change score variability measures were not reported, but an exact p value was reported, the t statistic was computed using the inverse of the cumulative distribution function as detailed elsewhere [11]. The t statistic, sample size, and mean change were then used to calculate the change score standard deviation using the following formula:
If neither of these values were reported, the variability of the change score was estimated using a test–retest correlation coefficient obtained from a previous study that assessed reliability within and between sessions [12]. For acute studies, the within-session r value of 0.77 was used and for chronic studies, the between-session r value of 0.61 was used. These r values were then entered into the following formula to obtain the change score standard deviation:
To ensure that all measurements were reported in the same units, studies that reported stiffness using shear modulus were converted back to shear wave speed using the following formula:
where shear wave speed is expressed in meters per second, shear modulus is expressed in pascals and muscle density is expressed in kg per cubic meter. The muscle densities were provided in the original papers as either 1000 kg per cubic meter [13, 14] or 1084 kg per cubic meter [15, 16]. When not provided [17, 18], the muscle density was estimated to be 1084 kg per cubic meter. If multiple joint angles were assessed [13], the measurement taken in the most relaxed position was used to match the protocols performed in the other included studies. If multiple different sites were taken within a given muscle [13, 16], the average of all the measured sites was used. Entirely different muscles, however, were treated as their own samples. Several studies assessed multiple time points to detect acute change in stiffness across time, and therefore, multiple acute analyses were performed to avoid violating the assumption of independence. The time frames that were chosen were done so to try and match the time frames across studies. To assess the quality of studies included in the meta-analysis, the quality assessment tool for pre–post studies without a control group was adapted from the National Institute of Health (NIH) (Table 1). All statistical analyses were computed using JASP version 0.11.1. Given the few number of studies meeting the criteria for inclusion in the meta-analysis, no moderating variables were evaluated. Statistical significance was set at p < 0.05.
Results
Acute impact of resistance exercise on muscle stiffness
A total of four studies met the criteria for inclusion in the quantitative analysis examining the influence of acute exercise on muscle stiffness (Table 2). There was a wide range of post-exercise time points that were assessed ranging from 15 min post-exercise [16, 19] all the way up to 21 days post-exercise [13]. We elected to run three different analyses to assess the acute time course of changes in muscle stiffness which included studies that assessed muscle stiffness within 1 h post-exercise [13, 16, 19], 2 days post-exercise [13, 19, 20], and ≥ 7 days post-exercise [13, 19] (Fig. 2). Studies taking muscle stiffness within the first hour, revealed a significant increase in muscle stiffness [ES: 1.52 (95% CI 0.14, 2.91); p = 0.031]. There was no longer an increased muscle stiffness when measured either 2 days post-exercise [ES: 0.76 (95% CI − 0.32, 1.83); p = 0.16] or ≥ 7 days post-exercise [ES: 0.20 (95% CI − 0.53, 0.94); p = 0.58]. This corresponds to an estimated increase of 2.47, 0.62 and 0.04 kilopascals at each the ≤ 1 h, 2 day, and ≥ 7 day time points, respectively, using the shear modulus of skeletal muscle tissue with an estimated muscle density of 1084 kg per cubic meter [15, 16].

Acute effects of resistance exercise on muscle stiffness. Effect size units are expressed in the raw units of m/sec
Chronic impact of resistance training on muscle stiffness
A total of four studies met the criteria for inclusion in the quantitative analysis examining the influence of chronic resistance training on muscle stiffness (Table 3). Of the four included studies, two studies assessed the knee extensors [14, 17], one study assessed the knee flexors [18] and one study assessed the elbow extensor muscles [15]. All of the chronic training studies included in this analysis involved untrained participants who were measured using an Aixplorer SuperSonic Imagine ultrasound machine. Collectively, there was no impact of long-term resistance exercise on changes in muscle stiffness [ES: − 0.04 (95% CI − 0.24, 0.15); p = 0.653; Fig. 3].

Chronic effects of resistance exercise on muscle stiffness. Effect size units are expressed in the raw units of m/sec
Discussion
Acute impact of resistance exercise on muscle stiffness
The primary finding from the acute analysis demonstrated that a single bout of resistance exercise increased muscle stiffness immediately post-exercise, but this subsided as time progressed (Fig. 2). Of the protocols listed in Table 2, the Lacourpaille et al. study [13] was the only study to employ maximal eccentric contractions on an isokinetic dynamometer, which likely induced the greatest muscle damage. The greater muscle damage also resulted in the largest magnitude of change in muscle stiffness, and this change was still elevated for at least one muscle group 3 weeks after the damaging exercise bout (Fig. 2). The Agten et al. study [19] also employed eccentric exercises but with a lighter load corresponding to 90% of the individual’s one-repetition maximum (1RM) strength. The authors noted increases in muscle stiffness immediately post-exercise, but this was no longer present when re-assessed 2 days post-exercise. Protocols that involved traditional isotonic resistance exercises, most likely to resemble what would be performed by individuals engaging in resistance exercise, demonstrated smaller increases in muscle stiffness immediately post-exercise [16]; while no changes where present when assessed 2 days post-exercise [20]. These results would suggest that the magnitude of muscle stiffness appears to be related to the level of muscle damage caused by the exercise protocol. Traditional resistance exercise protocols not intended to induce muscle damage may result in small changes in muscle stiffness immediately post-exercise, but this stiffness would be unlikely to remain present 2 days post-exercise. Contrarily, protocols intended to induce muscle damage will likely result in larger increases in muscle stiffness that will last a longer duration (upwards of 1 week).
Three studies were not included in the quantitative analysis because strain elastography was used instead of shear elastography [21,22,23]. Each of these studies corroborated the findings of the acute quantitative analysis demonstrating that muscle stiffness increased following an acute bout of resistance exercise. Following a traditional exercise bout of elbow flexion at 70% 1RM, muscle stiffness increased immediately post-exercise but then returned back close to baseline levels 30 min post-exercise [22]. The magnitude of stiffness present when examining the changes to eccentrically induced muscle damage appeared to be greater and also sustained for a much longer duration, remaining elevated for up to 4 days [21] or even 7 days post-exercise [23]. The duration that muscle stiffness remained elevated is unknown since it was still present at the last time point measured for each of these studies [21, 23]. Collectively, the results of these studies incorporating strain elastography yield the same conclusion as our acute quantitative analysis assessing shear wave elastography.
A few studies included in the acute analysis assessed different portions of the same muscle group. At baseline, there appeared to be a greater stiffness present in muscles that were more distal and this held true for both the biceps brachii [13] and triceps brachii [16]. There did not appear to be any difference; however, in the sensitivity to changes in muscle stiffness that occurred within each portion of the muscle in response to an acute bout of exercise [13, 16]. When looking at the magnitude of change in muscle stiffness, it appeared to be the greatest immediately post-exercise, even among studies that employed eccentrically damaging exercise [13]. Thus, this does not necessarily follow the traditional time course of delayed onset muscle soreness (DOMS) which usually peaks 24–48 h post-exercise [24]. The immediate post-exercise increase in muscle stiffness may be related to an increase in blood flow and fluid pressure within the exercising tissue which has been shown to be greater following eccentric exercise [25]. While acute studies assessing muscle stiffness using magnetic resonance imaging (MRI) [26] or passive torque production [27] demonstrate increases in stiffness 1 h post exercise, they noted larger increases present 1–2 days post exercise. This finding appeared to be true for the gastrocnemius muscle, but not the soleus muscle which peaked 1 h post-exercise [26]. These findings suggest that muscle stiffness measures are capable of detecting different rates of DOMS that are known to be present based on differences in muscle fiber types (more type two fibers result in more DOMS) [28]. Whether ultrasound measured elastography is capable of detecting these differences is difficult to conclude from the studies included in this review.
Chronic impact of resistance training on muscle stiffness
The primary finding of the chronic analysis demonstrated that resistance exercise did not result in any changes in muscle stiffness (Fig. 3). Of the studies included in the analysis, only one study found an increase in muscle stiffness [17]. The authors of this study [17] postulated they may have observed an increase in stiffness; whereas other studies did not because they used different probe orientations [15] or also included stretching as part of the intervention [18]. This is not supported by the results of this review as another study included in the quantitative analysis [14] used the same longitudinal probe orientation, trained for a longer duration, and specifically informed participants to avoid any stretching over the course of the study period. Therefore, it remains unknown as to why the Mannarino et al. [17] study observed an increase in muscle stiffness, whereas others did not.
When examining both Table 3 and Fig. 3, it appears that there is not any clear relationship between specific muscle groups and/or the mode of exercise used for resistance training. One study employed an eccentric only training intervention and also noted no changes in chronic muscle stiffness [18]. The lack of a change in chronic muscle stiffness also tended to hold true across both pennate and fusiform muscles. All of the interventions included in the analysis were sufficient to increase either muscle size, muscle strength, or both. Given that, collectively, there was no change in muscle stiffness in response to either concentric or eccentric resistance exercise, this would indicate that either muscle stiffness does not change appreciably with resistance exercise, or it requires a longer training period to adapt. A number of acute studies have tested muscle stiffness during different isometric contraction intensities, demonstrating that more forceful contractions result in greater muscle stiffness [29, 30]. Therefore, it is possible that engagement in resistance exercise does not result in any chronic changes in resting muscle stiffness, but may increase maximal muscle stiffness obtained during a maximal muscle contraction. This hypothesis may be difficult to test, however, given that the stiffness of muscle during maximal contractions may result in ultrasound wave speeds that are too fast to be detected [6].
One of the major limitations, as is common with meta-analyses, is that there was a large degree of heterogeneity in the included studies. This was particularly problematic given the few studies that met the criteria for inclusion in the analyses, which limited our ability to include these variables as moderators of the effect size estimates. This was apparent in the acute studies tracking changes in muscle stiffness where some studies used exercise protocols intended to induce muscle damage (maximal eccentric actions) [13] and others used more standard protocols that would be performed as part of a resistance training program (sets of eight at 80% 1RM) [16]. Other moderator variables that may dictate the magnitude of change in both acute and chronic muscle stiffness may include the muscle architecture, muscle fiber type, prior resistance training status, the length of the muscle when the measurement is taken, the location of the muscle being assessed (i.e., more proximal vs. more distal), and the orientation of the probe relative to the muscle fibers, but the influence of these moderator variables could not be assessed in the current review.
Conclusions
The primary findings from this meta-analysis indicate that muscle stiffness increased acutely following a bout of resistance exercise, but did not change long term with chronic exercise training when measured via ultrasound shear elastography. The increase in acute muscle stiffness appears proportional to the magnitude of muscle damage induced by the exercise protocol, but this could not be quantitatively assessed given the few number of studies included in the analysis. Future studies may wish to use ultrasound elastography as a non-invasive measure of muscle damage.
References
Ozturk A, Grajo JR, Dhyani M, Anthony BW, Samir AE (2018) Principles of ultrasound elastography. Abdom Radiol (NY) 43:773–785
Jones DA, Newham DJ, Clarkson PM (1987) Skeletal muscle stiffness and pain following eccentric exercise of the elbow flexors. Pain 30:233–242
Davidson MJ, Nielsen PMF, Taberner AJ, Kruger JA (2020) Is it time to rethink using digital palpation for assessment of muscle stiffness? Neurourol Urodyn 39:279–285
Kerins CM, Moore SD, Butterfield TA, McKeon PO, Uhl TL (2013) Reliability of the myotonometer for assessment of posterior shoulder tightness. Int J Sports Phys Ther 8:248–255
Balci BP (2018) Spasticity Measurement. Noro Psikiyatr Ars 55:S49–S53
Brandenburg JE, Eby SF, Song P, Zhao H, Brault JS, Chen S et al (2014) Ultrasound elastography: the new frontier in direct measurement of muscle stiffness. Arch Phys Med Rehabil 95:2207–2219
Bensamoun SF, Ringleb SI, Littrell L, Chen Q, Brennan M, Ehman RL et al (2006) Determination of thigh muscle stiffness using magnetic resonance elastography. J Magn Reson Imaging: JMRI 23:242–247
Pillen S, van Alfen N (2011) Skeletal muscle ultrasound. Neurol Res 33:1016–1024
Muraki S, Fukumoto K, Fukuda O (2013) Prediction of the muscle strength by the muscle thickness and hardness using ultrasound muscle hardness meter. SpringerPlus 2:457
Rosskopf AB, Ehrmann C, Buck FM, Gerber C, Fluck M, Pfirrmann CW (2016) Quantitative shear-wave us elastography of the supraspinatus muscle: reliability of the method and relation to tendon integrity and muscle quality. Radiology 278:465–474
Dankel SJ, Loenneke JP (2018) Effect sizes for paired data should use the change score variability rather than the pre-test variability. J Strength Cond Res. https://doi.org/10.1519/jsc.0000000000002946
Šarabon N, Kozinc Ž, Podrekar N (2019) Using shear-wave elastography in skeletal muscle: a repeatability and reproducibility study on biceps femoris muscle. PLoS ONE 14:e0222008
Lacourpaille L, Nordez A, Hug F, Couturier A, Dibie C, Guilhem G (2014) Time-course effect of exercise-induced muscle damage on localized muscle mechanical properties assessed using elastography. Acta Physiol (Oxf) 211:135–146
Ochi E, Maruo M, Tsuchiya Y, Ishii N, Miura K, Sasaki K (2018) Higher training frequency is important for gaining muscular strength under volume-matched training. Front Physiol 9:744
Akagi R, Shikiba T, Tanaka J, Takahashi H (2016) A six-week resistance training program does not change shear modulus of the triceps brachii. J Appl Biomech 32:373–378
Akagi R, Tanaka J, Shikiba T, Takahashi H (2015) Muscle hardness of the triceps brachii before and after a resistance exercise session: a shear wave ultrasound elastography study. Acta Radiol 56:1487–1493
Mannarino P, Matta TTd, Oliveira LFd (2019) An 8-week resistance training protocol is effective in adapting quadriceps but not patellar tendon shear modulus measured by shear wave elastography. PLoS ONE 14:e0205782
Seymore KD, Domire ZJ, DeVita P, Rider PM, Kulas AS (2017) The effect of Nordic hamstring strength training on muscle architecture, stiffness, and strength. Eur J Appl Physiol 117:943–953
Agten CA, Buck FM, Dyer L, Fluck M, Pfirrmann CW, Rosskopf AB (2017) Delayed-onset muscle soreness: temporal assessment with quantitative MRI and shear-wave ultrasound elastography. AJR Am J Roentgenol 208:402–412
Hotfiel T, Kellermann M, Swoboda B, Wildner D, Golditz T, Grim C et al (2018) Application of acoustic radiation force impulse elastography in imaging of delayed onset muscle soreness: a comparative analysis with 3T MRI. J Sport Rehabil 27:348–356
Niitsu M, Michizaki A, Endo A, Takei H, Yanagisawa O (2011) Muscle hardness measurement by using ultrasound elastography: a feasibility study. Acta Radiol 52:99–105
Yanagisawa O, Niitsu M, Kurihara T, Fukubayashi T (2011) Evaluation of human muscle hardness after dynamic exercise with ultrasound real-time tissue elastography: a feasibility study. Clin Radiol 66:815–819
Yanagisawa O, Sakuma J, Kawakami Y, Suzuki K, Fukubayashi T (2015) Effect of exercise-induced muscle damage on muscle hardness evaluated by ultrasound real-time tissue elastography. SpringerPlus 4:308
Miles MP, Clarkson PM (1994) Exercise-induced muscle pain, soreness, and cramps. J Sports Med Phys Fitness 34:203–216
Friden J, Sfakianos PN, Hargens AR, Akeson WH (1988) Residual muscular swelling after repetitive eccentric contractions. J Orthop Res: Off Publ Orthop Res Soc 6:493–498
Green MA, Sinkus R, Gandevia SC, Herbert RD, Bilston LE (2012) Measuring changes in muscle stiffness after eccentric exercise using elastography. NMR Biomed 25:852–858
Hoang PD, Herbert RD, Gandevia SC (2007) Effects of eccentric exercise on passive mechanical properties of human gastrocnemius in vivo. Med Sci Sports Exerc 39:849–857
Macaluso F, Isaacs AW, Myburgh KH (2012) Preferential type II muscle fiber damage from plyometric exercise. J Athl Train 47:414–420
Yavuz A, Bora A, Bulut MD, Batur A, Milanlioglu A, Goya C et al (2015) Acoustic radiation force impulse (ARFI) elastography quantification of muscle stiffness over a course of gradual isometric contractions: a preliminary study. Med Ultrason 17:49–57
Yoshitake Y, Takai Y, Kanehisa H, Shinohara M (2014) Muscle shear modulus measured with ultrasound shear-wave elastography across a wide range of contraction intensity. Muscle Nerve 50:103–113
Funding
None.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Neither SD nor BR has any conflicts of interest to declare.
Ethical approval
This is a systematic review and the Rowan University Institutional Review Board has confirmed that our study did not need ethical approval.
Informed consent
Prior informed consent was obtained by the researchers of the studies included in this review.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Dankel, S.J., Razzano, B.M. The impact of acute and chronic resistance exercise on muscle stiffness: a systematic review and meta-analysis. J Ultrasound 23, 473–480 (2020). https://doi.org/10.1007/s40477-020-00486-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40477-020-00486-3