
Abstract
Natural killer (NK) cell-mediated cancer immunotherapy has grown significantly over the past two decades. More recently, multi-specific engagers have been developed as cancer therapeutics to effectively arm endogenous NK cells to more potently induce specific cytolytic responses against tumor targets. This review explores the bi- and tri-specific NK/tumor engagers that are emerging as a new generation of immunotherapeutics. These molecules vary in configuration, but they typically have small molecular weights and domains that engage specific tumor antigens and NK cell-activating receptors such as CD16, NKp30, NKp46, and NKG2D. They have demonstrated compelling potential in boosting NK cell cytotoxicity against specific tumor targets. This highly adaptable off-the-shelf platform, which in some formats also integrates cytokines, is poised to revolutionize targeted NK cell immunotherapy, either as a monotherapy or in combination with other effective anti-cancer therapies.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Two main areas of NK cell-directed cancer immunotherapy include adoptive transfer of NK cells and biological agents designed to enhance endogenous NK cells. |
Bi-specific and tri-specific NK cell engagers are a new generation of cancer therapeutics that facilitate targeted NK cell-mediated antibody-dependent cellular cytotoxicity against specific tumor antigens. |
IL-15-bearing TriKETM promotes NK-cell proliferation, in conjunction with tumor targeting, while facilitating NK cell escape from immunosuppressive cells. |
1 Introduction
Decades of fruitful research in uncovering basic natural killer (NK) cell biology has paved the way for novel NK cell-mediated antitumor therapies. This has been further spurred by recent successes achieved in T cell-mediated immunotherapies involving chimeric antigen receptors (CAR), bi-specific T-cell engagers (BiTEs), and checkpoint blockade, which catalyzed a renewed interest in the potential that NK cells hold as another subset of anti-tumor immune cells. The innate properties of NK cells in surveillance and clearance of abnormal cells, such as tumor cells, justify the emergence of NK cells as a promising tool in cancer immunotherapy. There are currently a number of NK cell products and NK cell-enhancing agents in ongoing clinical trials. Here, we review these therapeutic approaches with a particular focus on the targeted bi- and tri-specific NK cell engagers.
2 Human NK Cell Functional Biology
NK cells are innate immune cells that can autonomously eliminate tumor and virus-infected cells. Unlike adaptive immune cells that require prior exposure and recognition of antigens, NK cells do not require prior sensitization to become activated [1]. A balance between activating and inhibitory signals determine NK cell responses against cells they interact with. Killer cell immunoglobulin-like receptors (KIR) on NK cells, like KIR2DL1, KIR2DL3, and KIR3DL2, bind to self major histocompatibility complex (MHC)-I, also referred as human leukocyte antigen (HLA), which is expressed on healthy cells and induces inhibitory signals upon said interaction [2]. Additionally, the c-type lectin heterodimer NKG2A/CD94 is another common inhibitory receptor expressed by NK cells that recognizes HLA-E molecules and transmits inhibitory signals. In contrast, activating receptors like natural cytotoxic receptors (NCRs), including NKp30/NCR3, NKp44/NCR2, NKp46/NCR1, c-type lectin receptor complexes like CD94/NKG2C and NKG2D, and the low affinity Fcγ receptor, CD16 (FcγRIII), trigger cytotoxic responses in NK cells [3]. Unlike B cells and T cells, NK cells have germline-encoded receptors that do not undergo gene rearrangement.
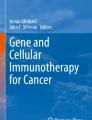
Antibody-dependent cellular cytotoxicity (ADCC), a key mechanism of NK cell responses, is mediated by CD16 crosslinking upon engagement of the Fc portion of an antibody (Fig. 1). This mechanism of action is potent and can be triggered without the combination of signals from other activating receptors [4]. Likely due to the robust nature of CD16 signaling, CD16 surface expression is tightly controlled by A disintegrin and metalloproteinase (ADAM) 17 that rapidly sheds CD16 on NK cells via clipping between residues 195 and 196 upon activation [5, 6]. Decreased surface CD16 expression leads to dampened NK cell responses, highlighting the role of ADAM17 in maintaining NK cell homeostasis to prevent excessive killing and non-specific tissue damage. However, in the context of NK cell cytotoxicity against tumor targets, ADAM17 undesirably diminishes ADCC, and inhibition of ADAM17, or modification of CD16 to prevent ADAM17 activity, has gained interest in this context [6, 7]. Undeniably, long-term administration of ADAM17 inhibitors as a treatment for chronic diseases such as rheumatoid arthritis and inflammatory bowel disease has been shown to cause deleterious effects [8]. Nevertheless, with careful consideration, ADAM17 inhibition is still a viable approach for shorter term cancer treatments.

Illustration of various mono- or multi-specific engagers developed as biologics to enhance NK-cell effector functions. ADCC antibody-dependent cellular cytotoxicity, Ag antigen, mAb monoclonal antibody, NKCE natural killer cell engager, ROCK® redirected optimized cell killing, TriKETM Tri-specific killer engager, TriNKET™ tri-specific NK-cell engager therapy. Created with BioRender.com
NK cell activation and inhibition are regulated by a complex series of signaling pathways. Briefly, upon engagement of activating receptors with their ligands, activation signals propagate through tyrosine-based activation motif (ITAM)-bearing adaptor proteins including FcεRIγ, CD3ζ, and the DAP12 [9]. Src family tyrosine kinases like Fyn, Lck, and Lyn phosphorylate the ITAM, which leads to recruitment of tyrosine kinase Syk and Zap70, which consequently cause phosphorylation of other proteins and activation of mitogen-activated protein kinases (MAPKs) and extracellular signal-regulated kinases (ERKs) [10]. Ultimately, these signals cause calcium ions (Ca2+) to release from intracellular compartments, activation of cytokine gene transcription, and actin cytoskeleton reorganization, resulting in the release of cytolytic granules containing perforin and granzyme. On the other hand, inhibitory signals propagate through tyrosine-based inhibition motifs (ITIMs) found in cytoplasmic tails of inhibitory receptors. Upon ligand engagement, ITIMs undergo phosphorylation and recruit phosphatases such as Src homology-containing tyrosine phosphatase 1 (SHP-1), SHP-2, and lipid phosphatase SH2 domain-containing inositol-5-phosphatase (SHIP), which dephosphorylate Lck, Fyn, Syk, Zap70, and Vav1 to terminate downstream activating signals [11, 12].
Productive NK cell contact with targets mediates formation of an immunological synapse (IS), which facilitates the delivery of cytolytic granules to target cells [13]. Perforin and granzyme enclosed in these granules function to kill target cells by puncturing the cell membrane and inducing apoptosis [14]. NK cell cytolytic degranulation is almost exclusively employed to ensure fast and efficient killing [15]. A recent study showed that upon depletion of perforin and granzyme, during serial killing, the NK cells switch from this methodology of killing to a slower death receptor-regulated killing approach [16]. This process is mediated by CD95L (Fas Ligand) or TNF-related apoptosis-inducing ligand (TRAIL) present on NK cell surfaces, which induce target cell death when engaged with their respective death receptors on target cells [17, 18].
In addition to perforin and granzyme release, activated NK cells secrete a wide variety of chemokines such as macrophage inflammatory protein (MIP)-1α, MIP-1β, interleukin (IL)-8, and RANTES (CCL5) and cytokines such as interferon-γ (IFN-γ), tumor necrosis factor-α (TNF-α), granulocyte-macrophage colony-stimulating factor (GM-CSF), IL-10, IL-5, and IL-13 [19]. These factors orchestrate many adaptive immune cell behaviors. For instance, IFN-γ released by NK cells induce naïve T-cell differentiation into cytotoxic T cells [20]. Similarly, IFN-γ and TNF-α released by NK cells promote dendritic cells (DC) maturation and migration to draining lymph nodes [21]. In return, DCs produce IL-15 and IL-12 that contribute to NK cell survival and activation. Evidently, soluble factors released by NK cells steadily regulate the crosstalk between NK cells and other immune cells.
In the past decade, evidence has shown that NK cells display memory-like properties usually attributed to adaptive immune cells. Although antigen specificity is considered the hallmark of immunological memory in B and T cells, cytokine induction is one of the mechanisms described to generate memory-like NK cells where NK cell pre-activation by IL-12 and IL-18 plus IL-15 enhances persistence, proliferative capacity and cytotoxic responses to tumor targets upon re-stimulation [22, 23]. Exposure to human cytomegalovirus (HCMV) is a different well described way to induce NKG2Chi CD57+ adaptive NK cell generation [24,25,26,27]. A lower activation threshold is achieved when one or several intracellular signaling proteins including FcεRIγ, SYK and EAT-2 are downregulated upon exposure to HCMV which ultimately leads to increased anti-tumor responses when adaptive NK cells are activated [26, 28]. Despite sharing similar properties, active investigations in mouse and human NK cells have revealed that cytokine- and HCMV-induced memory/adaptive NK cells have distinct cellular and molecular mechanisms leading to discrete functionalities [29]. For example, in mice, both subsets of memory/adaptive NK cells have enhanced IFN-γ production upon stimulation but cytokine-induced adaptive NK cells do not display enhanced cytotoxicity when restimulated [30]. More research is needed to further explore and define these unique NK cell subpopulations.
3 Natural Killer (NK) Cells in Cancer Immunotherapy
Over the years, NK cells have been extensively studied as a tool in cancer immunotherapy. There are two major areas of NK cell-directed immunotherapy: cellular therapeutics and biologics to enhance NK cell function. Both approaches are discussed in the subsequent sections, with more emphasis being placed in the targeted biologics.
3.1 Cellular NK Cell Therapeutics
Hematopoietic stem cell therapy (HSCT) is historically a major form of rescue therapy post high-dose radiation and chemotherapy in treating patients with hematologic malignancies like leukemia [31]. NK cells are the first lymphocyte group that repopulates post HSCT [32] and play an immediate role in inhibiting tumor recurrence [33]. Since NK cells display high efficiency in tumor clearance, this has led to the development of adoptive NK-cell transfer using autologous NK cells, donor-derived (allogeneic) NK cells, or other formats of NK cell products [34]. Unlike allogeneic T cell transfer approaches, NK cell transfer therapies have a low risk of graft-versus-host disease (GVHD) since activation and proliferation of alloreactive T cells are responsible for eliciting host tissue damage. However, simple autologous approaches using in vivo-expanded NK cells were found to have compromised cytotoxic responses partially due to the inhibitory effects mediated by interactions between the autologous NK cells and self MHC I molecules, resulting in low tumor regression [35]. Eventually, adoptive transfer of allogeneic or related donor NK cells became a more attractive alternative. Indeed, partial mismatch between inhibitory KIR of haploidentical donor NK cell and patient HLA maximizes NK cell cytotoxicity and in vivo expansion with IL-2 administration post NK cell infusion [36]. In this study, a more intense preparative regimen of high-dose cyclophosphamide and fludarabine (Hi-Cy/Flu), which induced lymphopenia, led to higher endogenous IL-15 levels, donor NK cell expansion, and induction of complete remission in five of 19 poor-prognosis patients with AML. This study demonstrated that adoptively transferred human NK cells can be expanded in vivo. More recently, utilization of membrane-bound IL-21 and 41BBL-expressing feeders has been used for robust in vitro expansion of NK cells for utilization in a number of clinical settings [37].
Adaptive NK cells that are a population of hyper-functional yet naturally occurring NK cells, as discussed above, are also emerging as another form of therapeutic NK cells. Ex vivo expansion of adaptive NK cells from healthy HCMV-seropositive individuals using IL-15 and a pharmacological GSK3 inhibitor, CHIR99021, has been previously described [38]. These culture-enriched NKG2C+CD57+ adaptive NK cells show enhanced effector functions. The efficacy of adaptive NK cells is currently being evaluated in several clinical trials [NCT03383055, NCT03081780, NCT03319459]. Cytokine-induced memory-like (CIML) NK cells are also being tested clinically to treat AML, multiple myeloma (MM), and head and neck cancer patients [NCT02782546, NCT01898793, NCT03068819, NCT04354025, NCT04024761, NCT04634435, NCT04290546]. Initial results from a phase I/II clinical study revealed that CIML-NK cells demonstrated capabilities to expand and actively respond to leukemia targets, resulting in complete remission in four out of nine AML patients above age 60 years [39] [NCT01898793]. These patients were pre-treated with Hi-Cy/Flu and CIML-NK cells administered were derived from donors with mismatched between KIR and their cognate HLA ligands.
Other alternative allogeneic NK cell sources include third-party NK cell products such as NK cell lines, induced pluripotent stem cells (iPSC) and umbilical cord blood (UCB)-derived NK cells. NK cell lines such as NK92 have demonstrated promising anti-cancer activity in clinical trials [40] [NCT03383978, NCT00900809, NCT00990717]. The lack of inhibitory receptors on NK92 cells results in maximum cytotoxicity towards a wide array of tumor types [41]. However, the genetic instability and high expansion rate of NK92 cells requires them to be irradiated prior to infusion, which compromise in vivo persistence [40]. Genetic modifications of NK92 cells are being actively investigated to improve their efficacy as an adoptive immunotherapy. Most recently, a site-specific CRISPR genome-editing tool for NK92 cells using Cas9 ribonucleoproteins was developed, showing promising advancement to unleash NK92 cells persistence in killing cancer [42]. Many preclinical and clinical trials are also evaluating CAR-engineered NK92 cells targeting various tumor antigens [43] [NCT02944162, NCT03027128, NCT02839954]. Similar to NK cell lines that can be used as an “off-the-shelf” therapy, UCB and stem cell-derived NK cells also hold great promises for the development of effective cancer treatments. Not only do UCB-derived NK cells share similar properties with peripheral blood NK cells, they also account for up to 30% of the lymphocyte population within UCB, which is approximately three times more than in peripheral blood [44]. A recent clinical study [NCT03056339] utilizing UCB NK cells expressing a CAR against CD19 and producing IL-15 showed promising clinical effects against B-cell cancers while also displaying minimal toxicity [45]. CAR-NK clinical and preclinical studies have been comprehensively described prior [46,47,48]. Besides isolation of NK cells from UCB, CD34+ hematopoietic progenitor cells found in abundance in UCBs can be differentiated into homogenous NK cells in large scales to be used in adoptive cell therapy [49]. Similarly, NK cells can also be easily differentiated and genetically manipulated from iPSCs, allowing unlimited scalability for adoptive transfer therapy [50,51,52,53,54]. Several variants of iPSC-derived NK cell products are currently undergoing phase I clinical investigations as a monotherapy or in combination with various other anti-tumor treatments. This includes FT500, the first-in-class, off-the-shelf, iPSC-NK cell therapy for advanced solid tumors [NCT03841110] [55]; FT516 that expresses high-affinity, non-cleavable CD16 (hnCD16) for treating AML or B cell lymphoma [NCT04023071]; FT596 that expresses anti-CD19 CAR, hnCD16 and membrane-bound IL-15 for treating chronic lymphocytic leukemia or B cell lymphoma [NCT04245722]; and FT538 with hnCD16, membrane-bound IL-15 and CD38 knockout for AML or MM treatment [NCT04614636]. While the safety profile of these platforms is still being actively investigated to determine if they are indeed safer than T-cell platforms, off-the-shelf NK-cell approaches garner a great deal of clinical potential.
3.2 Biologics to Enhance NK Cell Functions
Another prominent area of interest in NK cell immunotherapy involves the use of biologics to amplify endogenous or transferred NK cell activity. Although adoptive transfer of NK cells shows encouraging potential in combating cancers, those treatments can be limited by engraftment efficiency, risk of GvHD elicited by contaminating donor T cells within the graft, high cost of treatment, time-consuming processes to generate large numbers of NK cells, and risky preparative lymphodepleting treatments. Biologics that enhance NK cell function endogenously do not share most of these issues and thus have potential as individual or complimentary approaches to NK cellular therapy.
3.2.1 Cytokine-Based NK Cell Enhancement
NK cell development and priming relies heavily on cytokine signaling. IL-2 and IL-15 play key roles in regulating NK cell function. These cytokines signal through common receptor subunits that include the gamma-chain (γc) chain/CD132 and the IL2Rβ/ IL15Rβ/ CD122 complex [56]. IL-2 and IL-15-based therapeutics have been developed based on their ability to enhance NK-cell proliferation, survival, and cytotoxic abilities.
IL-2-based immunotherapy has been demonstrated to mediate tumor regression in early studies of patients with advanced cancer [57]. However, further studies showed that patient survival did not improve and severe adverse side effects were reported post high-dose IL-2 treatment such as vascular leak syndrome, pulmonary edema, and hypotension, among others [58, 59]. Low-dose IL-2 also preferentially expands regulatory T cell (Treg) populations, leading to increased immunosuppression, which may play a significant role in limiting lymphocyte anti-tumor responses [60]. While IL-2 monotherapy is faced with major challenges associated with toxicity, its combination with other anti-cancer immunotherapies is being evaluated in the clinic [61].
IL-15 is an attractive substitute for IL-2 for NK cell immunotherapy as it has a prominent role in NK cell development, supports NK cell function and persistence in a similar fashion to IL-2, and does not induce Treg proliferation due to its utilization of IL-15Rα rather than IL-2Rα for signaling [56]. Various formats of IL-15 molecules have been created for clinical use. For example, monomeric recombinant human IL-15 (rhIL-15) treatment has shown therapeutic benefits as a monotherapy and also in combination with other anti-cancer therapies [62, 63] [NCT01727076, NCT01385423, NCT02395822]. Additionally, IL-15 receptor complexes have also been developed to enhance potency by mimicking cell trans-presentation of IL-15. These complexes have been tested in the clinic, such as the heterodimeric mammalian IL-15/IL-15Rα (hetIL-15) molecule, which as the name suggests, consists of IL-15 and IL-15Rα components [64] [NCT04261439]; the SO-C101 molecule that is a receptor-linker-IL-15 (RLI) comprised of IL-15 linked to IL-15Rα sushi domain [65] [NCT04234113]; and the N-803 molecule (formerly known as ALT-803) which contains a mutated IL-15 “supergonist” linked to the sushi domain of IL-15Rα fused with human IgG1 Fc fragment [66] [NCT01946789]. Clinical use of IL-15 has garnered a lot of interest across a number of settings either as a monotherapy or in combination with other immune-oncological therapies.
3.2.2 Monoclonal Antibody Treatment
Monoclonal antibodies (mAbs) are well-established therapeutics that in some instances, depending on the Fc portion of the antibody, mediate NK cell ADCC against tumors [67] (Fig. 1). Selectively coating tumor cells with mAbs provide strong activating signals to NK cells, resulting in enhanced ADCC. However, the benefits of mAbs depend on a number of factors such as: the affinity of mAbs against the tumor antigen, which determines cytotoxic potency; affinity of CD16 against the Fc portion of the mAb; specificity of mAb against antigens uniquely expressed by cancer cells and not healthy cells; antigen density on target cells that can be regulated by recycling or internalization of antigens; and mAb bioavailability to the tumor [68].
In 1997, rituximab, an anti-CD20 mAb, was first approved to be used for treating non-Hodgkin’s lymphoma [69]. This was followed by various mAb that eventually developed into the standard of care for treating solid and blood cancers including cetuximab (anti-EGFR for colorectal and head and neck cancers) [70], trastuzumab (anti-HER2 for breast cancer) [71], dinutuximab (anti-GD2 for neuroblastoma) [72], daratumumab (anti-CD38 for MM) [73], among others. To fully unleash the efficacy of mAb treatments, they are often paired with other immunomodulatory treatments actively being tested in the clinic [NCT03769311, NCT04590963, NCT04644237, NCT02573896, NCT02944565].
Although various other innate immune cells including monocytes, macrophages, neutrophils, eosinophils, and dendritic cells are capable of mediating ADCC [74], NK cell-mediated ADCC was shown to significantly contribute to the success of mAb treatments such as rituximab and trastuzumab for hematological and solid tumors [75, 76]. It was revealed that patients with homozygous 158 valine/valine (V/V) alleles of CD16a, which has higher affinity to therapeutic antibody, displayed significantly improved clinical responses upon rituximab treatment as compared to patients with weaker phenylalanine (F) allele of CD16a [75]. In order to improve NK cell ADCC, approaches to modify the Fc portion of antibodies to enhance CD16 binding have been employed [77]. Conversely, in instances where ADCC is not desirable, the Fc binding has also been silenced through genetic manipulation. In addition to NK cell receptor binding affinity, a low pre-treatment NK cell count in peripheral blood is associated with worse outcome upon antibody treatment [78]. mAb treatment can also correlate to differential NK cell homing and infiltration to the tumor microenvironment (TME), which can influence outcomes. For example, the treatment efficacy of trastuzumab against breast cancer was shown to positively correlate with higher numbers of tumor-infiltrating NK cells [79]. Collectively, these factors support the notion that NK cells have a role in mAb treatment outcomes.
3.2.3 Checkpoint Blockade
NK cells naturally possess inhibitory receptors to restrain them from damaging normal and healthy tissues. Like other immune cells, NK cell inhibitory receptors consist of an ITIM within their cytoplasmic domain that dampens activation signals [80]. This inhibitory property clearly opposes NK cell anti-tumor functions, and therefore motivated the development of a wide array of checkpoint blockade approaches to influence NK cell activity.
Programmed death 1 (PD-1) and cytotoxic T lymphocyte antigen-4 (CTLA4) checkpoint blockades have achieved major successes in overcoming T-cell tolerance against various cancers [81,82,83]. While some studies have shown that NK cells within the tumor microenvironment express PD-1 and may be functionally impacted by PD-1 checkpoint blockade [84,85,86,87,88,89], including a recent human study, other studies demonstrated minimal PD-1 expression on NK cells highlighting the controversy of NK cell immunoregulation and anti-PD-1 treatments [90, 91]. Although expression of PD-1 on circulating NK cells has been controversial, combination treatment of multiple mAbs targeting both activating and inhibitory receptors has been shown to further enhance tumor clearance by NK cells. For example, blocking PD-1 on NK cells with high PD-1 expression with nivolumab can reverse NK cell dysfunction and greatly improve cetuximab-mediated NK cell cytotoxicity against head and neck cancer [85]. CTLA4 expression, however, has not been found on NK cells. Further investigations are needed to more clearly identify the expression levels of PD-1 and CTLA4 on NK cells to determine the efficacy of these well-known checkpoint blockades on NK cells.
The KIR family are by far the most studied group of inhibitory receptors expressed by NK cells [2, 92]. The constant interactions between KIR and MHC-I molecules is the driving factor in NK-cell “education,” a dynamic process that ensures mature NK cells gain and retain maximal cytotoxic functions when encountered with targets that do not express MHC-I [93]. Since tumors develop from normal cells, in many instances they maintain MHC-I expression and thereby send inhibitory signals upon engagement with KIR on NK cells, resulting in restricted anti-tumor response. This inhibitory interaction can be blocked with an anti-KIR antibody. The KIR2D-specific mAb, IPH2101, tested clinically in AML and MM patients, showed efficient KIR2D binding and some enhanced tumor cytotoxicity by NK cells [94, 95] [NCT00552396, NCT01248455]. Unfortunately, further clinical studies of patients with smoldering MM showed no therapeutic benefit [96], and this was later found to be due to inhibited interactions between KIR2D and its cognate ligand that prevented NK cells from becoming “educated,” and hence decreased overall NK cell function against MM cells [97].
NKG2A, which forms a heterodimer with CD94, is another inhibitory receptor found on NK cells that has been targeted as a checkpoint blockade. Like KIR, NKG2A is selectively expressed on NK cells but studies have shown upregulation of NKG2A expression post IL-12 treatment, suggesting that NK cells in the TME that are exposed to IL-12 likely have restricted anti-tumor responses [98]. The ligand of NKG2A, HLA-E, was found to be expressed by 33 tumor types, supporting the notion that blocking NKG2A may have therapeutic potential [99]. These findings, along with other preclinical studies, have brought an anti-NKG2A mAb, IPH2201-monalizumab, into clinical trials in combination with other treatments for various tumor types [100] [NCT02643550, NCT02671435]. However, like inhibitory KIR, NKG2A is also involved in NK cell education, thus the issues seen in the KIR blockade trials might also influence the outcome of NKG2A blockade [101,102,103].
T-cell immunoreceptors with Ig and ITIM domains (TIGIT) and T-cell immunoglobulin mucin receptor 3 (TIM3) are inhibitory receptors expressed on both T cells and NK cells [104, 105]. Interestingly, unlike other inhibitory receptors described, TIM3 does not have defined inhibitory cytoplasmic signaling motifs but can suppress NK-cell activation upon engagement with its ligand, galectin-9, which is commonly expressed on tumors and is associated with cancer metastasis [105, 106]. The expression of both TIM3 and TIGIT were found to be regulated by cytokines present in the surrounding of NK cells [105, 107]. In vitro and preclinical mouse models showed blockade of TIGIT promoted NK cell-dependent tumor immunity [108, 109]. Several clinical trials are ongoing to examine the efficacy of TIGIT and TIM3 antagonists in combination with other therapeutics [NCT02913313, NCT03066648].
3.2.4 Bi- and Tri-specific Engagers
Over the past decade a number of efforts, using bi- and tri-specific engagers to target NK cells to specific tumor antigens, have come to light and are starting to be translated into the clinic. These molecules are typically composed of two or more antibody fragments connected via short flexible linkers.
Affimed, based in Heidelberg, Germany, brought its bi-specific redirected optimized cell killing (ROCK®) antibody platform into the clinic first. This platform is a tetravalent bi-specific antibody (bsAb) that consists of two diabodies with Fv domains against CD16a and a tumor-associated antigen [110] (Fig. 1). The format of CD16a binding in this molecule is not disrupted by serum IgG and keeps the Fc-binding region free, allowing for combination treatment with mAb to further enhance NK cell-mediated ADCC. AFM13, which binds CD30, has been tested against relapsed or refractory Hodgkin or non-Hodgkin lymphoma, alone or in combination with checkpoint blockade, in a number of clinical trials [111, 112] (Table 1). This state-of-the-art bispecific diabody molecule has demonstrated surprising safety across a broad range of doses from 0.05 to 7 mg/kg in the clinic with a disease control rate of 77%. Affimed has also developed engagers against EGFR (AFM24) for solid tumor treatment [113], and B-cell maturation antigen (BCMA) (AFM26/ RO7297089) for treatment of MM [114], both of which entered the clinic last year, as well as AFM28 and AFM32, which are under preclinical studies (Table 1).
Dragonfly Therapeutics, based in Waltham, Massachusetts, has developed a Tri-specific NK cell Engager Therapies (TriNKET™) technology. Though not much information is publicly available for this platform it seems to consist of multi-specific NK cell engagers targeting CD16 and NKG2D receptors on NK cells and a tumor-associated antigen (Fig. 1). DF1001, their first TriNKET™ to hit the clinic, is specific against HER2 and is currently being evaluated as a treatment of advanced solid HER2-positive tumors and in combination therapies with the anti- PD-1 antibody pembrolizumab (Table 1). Besides HER2-specific DF1001, several other TriNKETs™ targeting hematological malignancies, such as DF2-3-4-5001, are currently under development [115, 116].
More recently, a novel trifunctional NK cell engager (NKCE) consisting of antibody fragments targeting two NK cell-activating receptors, CD16 and NKp46, and one tumor-associated antigen including CD19, CD20, or EGFR has been described [117] (Fig. 1). In this study, in vitro and preclinical mouse models showed more efficient tumor clearance with NKCE treatments as compared to mAbs. Innate Pharma, based in Marseille, France are developing these engagers, IPH6101/ SAR443579 and IPH62, which will soon be available in the clinic for testing.
Another newly established multi-specific engager against NKp46 is the tetravalent bispecific trifunctional antibody, also known as FLEX-NK®, which is developed by Cytovia Therapeutics, based in New York, NY, USA. CYT 303 and CYT 338 are FLEX-NK® engagers against GPC3, a glycoprotein highly expressed on solid tumors, and CD38 to treat solid cancers and MM respectively [118].
CTX-8573 is another novel multi-specific engager developed by Compass Therapeutics, based in Boston, MA, USA, that targets BCMA and elicits potent cytotoxicity in NK and γδ T cells by engaging with activating receptors including NKp30 and CD16a [119]. Preclinical investigation has shown robust enhanced killing of tumor cells both in vitro and in vivo with CTX-8573 treatment. No evidence of systemic immune activation or toxicity was displayed in a non-human primate model, suggesting promising potential of CTX-8573 advancement into the clinic.
4 Development of First-Generation BiKE and TriKETM Molecules
Since ADCC, initiated by CD16 activation, is a prominent mechanism of action by NK cells against tumor cells, targeting CD16 on NK cells is a logical therapeutic choice [120]. Like the previous bi- and tri-specifics described, which all utilize CD16 mediated activation, this insight led to the development of Bi- and Tri-specific Killer Engager (BiKE and TriKETM) molecules that engage CD16 to ensure maximum activation of NK cells.
The BiKE and TriKETM molecules each have two or three scFvs, which consist of a variable heavy (VH) and a light (VL) chain, or single domain antibodies (VHH) connected by short peptide linkers [120]. These scFv or VHH are specific for CD16 on NK cells and tumor antigen on tumor cells (Fig. 1). TriKETM molecules contain an IL-15 cytokine moiety, based on the fact that CD16 ligation alone does not induce proliferation. To date, BiKEs and TriKEsTM have been generated against CD19/CD22 on B-cell non-Hodgkin’s lymphomas [121, 122]; CD33 and CLEC12A on AML, myelodysplastic syndrome (MDS) and neoplastic mast cells [123,124,125,126,127]; and EpCAM, CD133, and B7-H3 on various solid tumor types such as breast, prostate, colon, ovarian, non-small-cell lung cancer, and head and neck cancers [128,129,130,131,132,133]. Compared to whole antibody molecules that are approximately 150kDa, BiKE and TriKETM molecules are smaller and range from 50 to 96 kDa [121, 134]. This is also true for most of the bi- and tri-specific molecules discussed in the previous section.
The production of BiKE and TriKETM molecules has been previously described [120]. Briefly, the components of the BiKE or TriKETM must first be designed by identifying sequences of scFv or VHHs against specific antigens of interest and appropriate linkers that are flexible and provide optimal separation between scFv or VHH [135]. Stretches of small and hydrophilic amino acids like glycine (G) and serine (S) can provide necessary flexibility to linkers, as demonstrated by the (GGGGS)3 peptide designed by Huston et al. [136, 137]. Once the sequences of each component have been identified, they can then be incorporated into vectors to be expressed in either the bacterial or mammalian expression systems. Although the bacterial expression system is more time and cost efficient [138], proteins produced can sometimes be shuttled to inclusion bodies, which requires the use of detergent for extraction of the proteins, thus necessitating refolding of said proteins, a factor that may introduce more variables and create inconsistency in the proteins generated [139]. In contrast, the mammalian expression system using Expi293 cells allows proteins to be directly collected from culture supernatant without refolding. The Gibson assembly method is used to clone selected sequences into appropriate vectors [140]. The final step involves protein purification through an ion exchange column and size exclusion chromatography, or column isolation with an affinity tag (usually His).
Given the clinical success demonstrated by BLINCYTO (blinatumomab, Amgen), a bi-specific T-cell engager (BiTETM) against CD19 [141], the following molecules were produced for targeting B-cell non-Hodgkin’s lymphomas: an original BiKE consisting of one scFv against CD16 and one scFv against CD19, and a tri-specific engager against CD16, CD19, and CD22 [121]. When compared to the BiKE, the tri-specific engager had similar enhancement of NK-cell degranulation and cytokine release upon activation. This suggested that in the settings tested, one scFv targeting tumor cells was sufficient. An improved tri-specific engager, termed TriKETM, was later developed to accommodate a novel modified human IL-15 as a functional linker between two scFv segments [124]. In addition to target specificity, absolute NK cell count is equally important for clinical efficacy. Since IL-15 plays a role in NK cell development, homeostasis, proliferation, survival, and activation [142], the goal of this modification was to improve NK cell maintenance and expansion by directly delivering IL-15 to NK cells in addition to mediating killing of tumors. TriKETM is the first multi-specific molecule that incorporates not only engagers against NK cells and tumor targets, but also a functionally significant IL-15 linker. As expected, the TriKETM against CD16 and CD33, termed 161533 TriKETM, not only enhanced NK cell-mediated anti-tumor responses against CD33+ targets, but also improved NK cell survival, proliferation, and persistence in vivo [124]. Revisiting the CD19 targeting, a TriKETM expressing IL-15, termed 161519, was later described [122]. This molecule demonstrated in vitro NK specific proliferative activity, as well as cytolytic activity in vitro against Raji cells (Burkitt’s lymphoma) and primary CLL tumor. A similar 161519 molecule was later generated by a separate group, reproducing many of the initial 161519 in vitro findings but also demonstrating in vivo activity [143]. While these approaches complement the BiTE and CAR-T studies targeting CD19, they might also offer reduced toxicity given their mechanism of action through NK cells instead of T cells.
As discussed previously, BiKEs and TriKEsTM have also been generated to target solid tumors. The epithelial cell-adhesion molecule (EpCAM) is known for its expression in various types of carcinoma such as colon, ovary, breast, and prostate cancers, and is thus a marker with high therapeutic potential [144]. A BiKE with scFvs targeting CD16 and EpCAM was previously developed and showed enhanced in vitro NK cell killing of prostate, breast, colon, and head and neck cancer even at very low effector: target ratios [132]. An EpCAM TriKETM, containing an IL-15 moiety between the anti-CD16 and anti-EpCAM scFvs, was later described and demonstrated not only enhanced cytolytic activity and inflammatory cytokine production, but also increased NK cells proliferative capacity when compared to the EpCAM BiKE [128]. In addition to EpCAM+ tumor targets, CD133-expressing cancer stem cells (CSC) are emerging as a new treatment target due to their cancer-initiating characteristics [145]. A CD133-targeting TriKETM termed 1615133 TriKETM that consists of an IL-15 linker between two scFvs against CD16 and CD133 was generated and described to efficiently enhance NK cell killing of CSCs [130]. These findings have led to the development of a tetra-specific killer engager (TetraKE or dual targeted TriKETM) specific for CD16, EpCAM, and CD133 held together by a modified IL-15 linker, referred as 1615EpCAM133, which facilitates dual-antigen ADCC and displayed capability to attack solid cancer and its basal roots, the CSC [131]. Taken together, the first generation TriKETM platform displayed promising translational potential.
5 BiKEs and TriKEsTM Help NK Cells Overcome Suppressive Cells
One of the biggest hurdles faced by endogenous and therapeutic NK cells is the encounter of an immune-suppressive TME, especially in solid tumors. High levels of tumor-infiltrating NK cells provide better prognosis but the presence of immune-suppressive cells, like Tregs and myeloid-derived suppressor cells (MDSCs), in the TME undesirably weaken NK cell functions, leading to tumor progression [146]. In MDS patients, the number of MDSCs is reported to be significantly higher than healthy individuals, which partly explains reduced NK cell counts in these patients [147]. With limited NK cell surveillance, disease progression is augmented. A BiKE against CD16 and CD33 was initially developed to facilitate NK-cell engagement with AML tumor targets [147]. In this study, the 1633 BiKE not only increased NK cell-driven killing of CD33+ tumor cells, but also induced lysis of MDSCs that expressed CD33. In vitro, the CD33-targeting BiKE was capable of reversing MDSC immunosuppression on NK cells.
It is essential to understand the inhibitory mechanisms adopted by immune-suppressive cells in order to develop effective NK cell-mediated anti-cancer therapeutics. It has been previously reported that NK cells upregulate TIGIT in the presence of soluble IL-15 [108]. This consequently leads to higher interaction of TIGIT on NK cells with its high affinity ligand, CD155, expressed on MDSCs. The MDSC-NK cell interaction results in suppressed NK-cell proliferation, degranulation, and IFN-γ production when activated [108, 148] . However, IL-15 presented as a linker in 161533 TriKETM did not alter TIGIT expression on NK cells and, therefore, contributed to MDS-NK cell resistance to immune-suppressive cells like MDSCs [149]. Since MDSCs are also targeted by the 161533 TriKETM, NK cell-mediated MDSC lysis also contributed to the relieved suppression. Although the evolutionary role of immune-suppressive cells is to maintain immune homeostasis, cancer immunotherapy aims to unleash this control especially in the tumor microenvironment. Therefore, CD33-targeting TriKETM shows promising potential to surpass MDSC inhibition in the suppressive tumor milieu.
6 Clinical Implementation of First-Generation TriKETM (GTB-3550)
The main goal of TriKETM molecules is to drive directed cytotoxicity against tumor targets through creation of a cytolytic bridge or synapse between the NK cell and the tumor, and to deliver IL-15 specifically to the NK cell to enhance NK-cell expansion, survival, and priming. GT Biopharma, Beverly Hills, CA, USA, currently has one TriKETM in the clinic, 161533 TriKETM (GTB-3550), with several others in the pipeline. The robust anti-tumor activities and enhanced proliferation of NK cells post GTB-3550 treatment in preclinical studies led to the onset of a phase I/II clinical trial involving patients with relapsed and/or refractory AML or high risk MDS [NCT03214666]. In this study GTB-3550 is infused intravenously in three blocks of 96 h over the course of 3 weeks. Initial findings were recently presented at the American Society of Hematology annual meeting, showing GTB-3550 TriKETM safely drives robust NK-cell proliferation/expansion in the initial cohorts of patients [150]. NK-cell activation was reported to increase 3 days post GTB-3550 treatment, with maximal proliferation seen at day 8 and robust NK-cell expansion seen in all patients evaluated by the end of treatment. Unlike the adverse toxicity caused by rhIL15 infusion at a maximum tolerated dose as low as 2 µg/kg/day [151] [NCT01572493], patients treated with 5, 10, and 25 µg/kg/day GTB-3550 TriKETM did not show toxicity, indicating that IL-15 sandwiched between two scFvs is less toxic and encourages efficient and direct IL-15 delivery to CD16+ NK cells. Although significant clinical efficacy has yet to be reported, higher-dose cohorts may clarify the potential of GTB-3550 as a therapy for AML and MDS patients. Future clinical studies will address the continuous infusion dosing strategy for more patient-friendly administration. Approaches with subcutaneous injections, previously tested on rhIL-15 and blinatumomab, or modifications to make the engager larger or cleared less have increased the half-life of these types of molecules and thus hold promise for TriKETM immunotherapy [62, 152] [NCT01727076, NCT02961881, NCT04521231].
7 Second-Generation TriKEsTM
A recent study has shown that the mutant IL-15, with an N72D substitution, that is incorporated within 161533 TriKETM is significantly less potent than recombinat human wildtype IL-15 (rhIL-15) on its own, leading to the development of the second-generation TriKETM [125]. Potentially due to steric hindrance of two scFv arms in the first generation 161533 TriKETM, the incorporation of wild type IL-15 (wtIL15) resulted in a non-functional first generation molecule. Therefore, in order to develop a second-generation TriKETM containing wildtype IL-15, the scFv anti-CD16 arm was replaced with a smaller humanized single-domain anti-CD16 VHH derived from camelids, termed cam16. With these modifications, the second-generation cam16-wtIL15-33 TriKETM is functionally superior to the first-generation TriKETM, displaying better proliferative activity on NK cells, and inducing better tumor control in vitro and in preclinical mouse models [125].
The second-generation platform was also employed in a different study targeting CLEC12A also in the myeloid malignancy setting [126]. The initial 161533 TriKETM has potential off-target effects against normal CD33-expressing myeloid and myeloid progenitor cells [149]. CLEC12A is expressed steadily on AML blasts but less so on nonmalignant hematopoietic stem cells (HSCs), making this a more suitable tumor antigen to target [153]. In fact, various other therapies under development such as conjugated antibodies and CAR T-cell therapy are utilizing CLEC12A as a target [154,155,156]. Nonetheless, CLEC12A-directed CAR T-cell therapy and antibody-drug conjugates may lead to long lasting cytopenias due to high perseverance of this treatment approach. One advantage the TriKETM approach offers is quick turnover, allowing for reduced toxicities through quicker drug withdrawal. Altogether, CLEC12A TriKETM can efficiently target AML cells while sparing healthy HSCs, suggesting a promising option for clinical translation.
Similar to the EpCAM approaches previously described with the first generation TriKETM, B7-H3 is another marker commonly expressed by solid tumors that has gained great interest as a target for cancer therapeutics [157]. There are several ongoing clinical trials targeting B7-H3 using Fc optimized antibodies [NCT02982941] and CAR T cells [NCT04077866]. Using the second-generation TriKETM bioengineering platform, a TriKETM was described incorporating an anti-B7-H3 scFv, termed cam1615B7H3 TriKETM [133]. Besides improving in vitro NK cell killing of ovarian, prostate, and lung cancers, treatment with cam1615B7H3 TriKETM also demonstrated potent activity in a xenogeneic ovarian cancer model. This evidence supports clinical development of second-generation solid tumor-targeting TriKEsTM.
8 Advantages and Future Directions of TriKETM
The TriKETM platform is versatile and has many advantages as a cancer therapeutic. Firstly, the small molecular size of the TriKETM molecule increases biodistribution which is especially important in targeting solid tumors [158,159,160]. The incorporation of IL-15 in a TriKETM molecule ensures direct delivery of IL-15 to NK cells and strongly limits off-target CD8+ T cell stimulation. rhIL-15 has been tested to enhance adoptive cell therapies [62, 161], so it makes sense that the TriKETM could be used as a combination therapy with adoptive cell transfer to enhance NK cell killing and persistence. Furthermore, to overcome rapid CD16 clipping by ADAM17 upon activation, TriKEsTM could be used in conjunction with ADAM17 inhibitors. This approach was previously investigated using CD16xCD33 BiKE, which showed further enhancement in NK-cell killing of AML targets [123]. The feasibility to readily engineer and produce TriKEsTM highlights the flexibility of this platform to generate a variety of molecules targeting many types of cancer.
The established TriKETM platform shows convincing translational potential. However, modifications can still be made to maximize TriKETM efficacy in mediating NK-cell killing of tumor targets. Existing TriKETM molecules only target CD16 on NK cells but a TriKETM molecule specific for other NK-cell activating or co-stimulatory receptors holds equal potential in facilitating NK cell-mediated ADCC. For instance, NKG2D and 2B4 co-engagement has been shown to induce similar activation as CD16 alone [162]. This is a potential alternative approach to avoid weakened NK cell activation due to rapid shedding of CD16 by ADAM17 upon activation [5]. Inhibitory scFvs against checkpoint receptors such as TIGIT, PD-1, KIRs, and NKG2A may also be incorporated into TriKEsTM to block inhibitory signals. Similarly, TGF-β-mediated NK-cell suppression, especially in solid tumor TME, may be blocked using a TriKETM with TGF-β antagonism. Since TriKEsTM are amendable to target any antigen of interest, a wide variety of TriKEsTM with unique specificity can be generated. These antigens include, but are not limited to, EGFR (for breast, glioma, lung, colon, and head and neck tumors), HER2 (for breast, colon, lung, ovarian, and prostate tumors), CEA (for breast, colon, and lung tumors), CD30 (for Hodgkin’s lymphoma), CD52 (for chronic lymphocytic leukemia), gpA33 (for colorectal tumor), PSMA and Trop-2 (for prostate tumor) and VEGFR (for epithelium-derived solid tumors) [160]. Collectively, the TriKETM platform holds great potential in establishing a new avenue of cancer immunotherapy.
9 Concluding Remarks
Cancer immunotherapy is constantly evolving as we better understand the complex dynamics between tumor cells and the immune system. With advancements made in genetic and molecular editing technologies, various sources of NK cells have been successfully modified to increase tumor clearance efficiency. Needless to say, the generation of advanced NK cell biologics like modified IL-15 products, ROCK®, NKCE, TriNKET™, BiKE, and TriKE™ are made possible by active investigations along using novel genetic-engineering platforms. As discussed in this review, NK cell products and immunomodulatory drugs both come with undesirable shortcomings. With considerations of cancer types, stage of disease, the immunosuppressive microenvironment, presence of immune cells in different compartments, therapeutic-driven antigen escape, and drug-related toxicities, the future of NK cell-based immunotherapy likely lies in a dynamic combination therapy approach rather than monotherapy. Based on the pool of knowledge uncovered by previous research and new insights that constantly arise, we as a field are motivated to further advance NK cell-based cancer therapy with the hope of achieving robust clinical efficacy as well as a wide therapeutic window.
References
Morvan MG, Lanier LL. NK cells and cancer: you can teach innate cells new tricks. Nat Rev Cancer. 2016;16(1):7–19.
Lanier LL. Follow the leader: NK cell receptors for classical and nonclassical MHC class I. Cell. 1998;92(6):705–7.
Sivori S, Vacca P, Del Zotto G, Munari E, Mingari MC, Moretta L. Human NK cells: surface receptors, inhibitory checkpoints, and translational applications. Cell Mol Immunol. 2019;16(5):430–41. https://doi.org/10.1038/s41423-019-0206-4.
Bryceson YT, March ME, Ljunggren H-G, Long EO. Synergy among receptors on resting NK cells for the activation of natural cytotoxicity and cytokine secretion. Blood. 2006;107(1):159–66.
Romee R, Foley B, Lenvik T, Wang Y, Zhang B, Ankarlo D, et al. NK cell CD16 surface expression and function is regulated by a disintegrin and metalloprotease-17 (ADAM17). Blood. 2013;121(18):3599–608.
Moss ML, Minond D. Recent advances in ADAM17 research: a promising target for cancer and inflammation. Mediators Inflamm. 2017;2017:1–21.
Wu J, Mishra HK, Walcheck B. Role of ADAM17 as a regulatory checkpoint of CD16A in NK cells and as a potential target for cancer immunotherapy. J Leukoc Biol. 2019;105(6):1297–303. https://doi.org/10.1002/JLB.2MR1218-501R.
Blaydon DC, Biancheri P, Di W-L, Plagnol V, Cabral RM, Brooke MA, et al. Inflammatory skin and bowel disease linked to ADAM17 deletion. N Engl J Med. 2011;365(16):1502–8. https://doi.org/10.1056/NEJMoa1100721.
Vivier E, Nunès JA, Vély F. Natural killer cell signaling pathways. Science (80-). 2004;306(5701):1517–9.
Paul S, Lal G. The molecular mechanism of natural killer cells function and its importance in cancer immunotherapy. Front Immunol. 2017;8:1124.
Veillette A, Latour S, Davidson D. Negative regulation of immunoreceptor signaling. Annu Rev Immunol. 2002;20(1):669–707. https://doi.org/10.1146/annurev.immunol.20.081501.130710.
Stebbins CC, Watzl C, Billadeau DD, Leibson PJ, Burshtyn DN, Long EO. Vav1 dephosphorylation by the tyrosine phosphatase SHP-1 as a mechanism for inhibition of cellular cytotoxicity. Mol Cell Biol. 2003;23(17):6291–9.
Davis DM, Chiu I, Fassett M, Cohen GB, Mandelboim O, Strominger JL. The human natural killer cell immune synapse. Proc Natl Acad Sci. 1999;96(26):15062–7. https://doi.org/10.1073/pnas.96.26.15062.
Voskoboinik I, Whisstock JC, Trapani JA. Perforin and granzymes: function, dysfunction and human pathology. Nat Rev Immunol. 2015;15(6):388–400.
Lopez JA, Susanto O, Jenkins MR, Lukoyanova N, Sutton VR, Law RHP, et al. Perforin forms transient pores on the target cell plasma membrane to facilitate rapid access of granzymes during killer cell attack. Blood. 2013;121(14):2659–68.
Prager I, Liesche C, van Ooijen H, Urlaub D, Verron Q, Sandström N, et al. NK cells switch from granzyme B to death receptor-mediated cytotoxicity during serial killing. J Exp Med. 2019;216(9):2113–27.
Kagi D, Vignaux F, Ledermann B, Burki K, Depraetere V, Nagata S, et al. Fas and perforin pathways as major mechanisms of T cell-mediated cytotoxicity. Science (80-). 1994;265(5171):528–30. https://doi.org/10.1126/science.7518614.
Strasser A, Jost PJ, Nagata S. The many roles of FAS receptor signaling in the immune system. Immunity. 2009;30(2):180–92.
Fauriat C, Long EO, Ljunggren H-G, Bryceson YT. Regulation of human NK-cell cytokine and chemokine production by target cell recognition. Blood. 2010;115(11):2167–76.
Hu X, Ivashkiv LB. Cross-regulation of signaling pathways by interferon-gamma: implications for immune responses and autoimmune diseases. Immunity. 2009;31(4):539–50.
Ferlazzo G, Morandi B. Cross-talks between natural killer cells and distinct subsets of dendritic cells. Front Immunol. 2014. https://doi.org/10.3389/fimmu.2014.00159/abstract.
Pahl JHW, Cerwenka A, Ni J. Memory-like NK cells: remembering a previous activation by cytokines and NK Cell receptors. Front Immunol. 2018. https://doi.org/10.3389/fimmu.2018.02796/full.
Ni J, Miller M, Stojanovic A, Garbi N, Cerwenka A. Sustained effector function of IL-12/15/18-preactivated NK cells against established tumors. J Exp Med. 2012;209(13):2351–65.
Lopez-Verges S, Milush JM, Schwartz BS, Pando MJ, Jarjoura J, York VA, et al. Expansion of a unique CD57+NKG2Chi natural killer cell subset during acute human cytomegalovirus infection. Proc Natl Acad Sci. 2011;108(36):14725–32. https://doi.org/10.1073/pnas.1110900108.
Foley B, Cooley S, Verneris MR, Pitt M, Curtsinger J, Luo X, et al. Cytomegalovirus reactivation after allogeneic transplantation promotes a lasting increase in educated NKG2C+ natural killer cells with potent function. Blood. 2012;119(11):2665–74.
Schlums H, Cichocki F, Tesi B, Theorell J, Beziat V, Holmes TD, et al. Cytomegalovirus infection drives adaptive epigenetic diversification of NK cells with altered signaling and effector function. Immunity. 2015;42(3):443–56.
Barnes S, Schilizzi O, Audsley KM, Newnes HV, Foley B. Deciphering the immunological phenomenon of adaptive natural killer (NK) cells and cytomegalovirus (CMV). Int J Mol Sci. 2020;21(22):8864.
Zhang T, Scott JM, Hwang I, Kim S. Cutting edge: antibody-dependent memory-like NK cells distinguished by FcRγ deficiency. J Immunol. 2013;190(4):1402–6. https://doi.org/10.4049/jimmunol.1203034.
O’Sullivan TE, Sun JC, Lanier LL. Natural killer cell memory. Immunity. 2015;43(4):634–45.
Cooper MA, Elliott JM, Keyel PA, Yang L, Carrero JA, Yokoyama WM. Cytokine-induced memory-like natural killer cells. Proc Natl Acad Sci. 2009;106(6):1915–9. https://doi.org/10.1073/pnas.0813192106.
Leung W. Use of NK cell activity in cure by transplant. Br J Haematol. 2011;155(1):14–29. https://doi.org/10.1111/j.1365-2141.2011.08823.x.
Rooney CM, Wimperis JZ, Brenner MK, Patterson J, Hoffbrand AV, Prentice HG. Natural killer cell activity following T-cell depleted allogeneic bone marrow transplantation. Br J Haematol. 1986;62(3):413–20. https://doi.org/10.1111/j.1365-2141.1986.tb02952.x.
Triplett BM, Horwitz EM, Iyengar R, Turner V, Holladay MS, Gan K, et al. Effects of activating NK cell receptor expression and NK cell reconstitution on the outcomes of unrelated donor hematopoietic cell transplantation for hematologic malignancies. Leukemia. 2009;23(7):1278–87.
Woan KV, Miller JS. Harnessing natural killer cell antitumor immunity: From the bench to bedside. Cancer Immunol Res. 2019;7(11):1742–7.
Parkhurst MR, Riley JP, Dudley ME, Rosenberg SA. Adoptive transfer of autologous natural killer cells leads to high levels of circulating natural killer cells but does not mediate tumor regression. Clin Cancer Res. 2011;17(19):6287–97. https://doi.org/10.1158/1078-0432.CCR-11-1347.
Miller JS, Soignier Y, Panoskaltsis-Mortari A, McNearney SA, Yun GH, Fautsch SK, et al. Successful adoptive transfer and in vivo expansion of human haploidentical NK cells in patients with cancer. Blood. 2005;105(8):3051–7.
Lee DA. Cellular therapy: adoptive immunotherapy with expanded natural killer cells. Immunol Rev. 2019;290(1):85–99. https://doi.org/10.1111/imr.12793.
Cichocki F, Valamehr B, Bjordahl R, Zhang B, Rezner B, Rogers P, et al. GSK3 inhibition drives maturation of NK cells and enhances their antitumor activity. Cancer Res. 2017;77(20):5664–75. https://doi.org/10.1158/0008-5472.CAN-17-0799.
Romee R, Rosario M, Berrien-Elliott MM, Wagner JA, Jewell BA, Schappe T, et al. Cytokine-induced memory-like natural killer cells exhibit enhanced responses against myeloid leukemia. Sci Transl Med. 2016;8(357):357ra123. https://doi.org/10.1126/scitranslmed.aaf2341.
Suck G, Odendahl M, Nowakowska P, Seidl C, Wels WS, Klingemann HG, et al. NK-92: an ‘off-the-shelf therapeutic’ for adoptive natural killer cell-based cancer immunotherapy. Cancer Immunol Immunother. 2016;65(4):485–92. https://doi.org/10.1007/s00262-015-1761-x.
Gong JH, Maki G, Klingemann HG. Characterization of a human cell line (NK-92) with phenotypical and functional characteristics of activated natural killer cells. Leukemia. 1994;8(4):652–8.
Huang R-S, Shih H-A, Lai M-C, Chang Y-J, Lin S. Enhanced NK-92 cytotoxicity by CRISPR genome engineering using Cas9 ribonucleoproteins. Front Immunol. 2020. https://doi.org/10.3389/fimmu.2020.01008/full.
Mehta RS, Rezvani K. Chimeric antigen receptor expressing natural killer cells for the immunotherapy of cancer. Front Immunol. 2018. https://doi.org/10.3389/fimmu.2018.00283/full.
Sarvaria A, Jawdat D, Madrigal JA, Saudemont A. Umbilical cord blood natural killer cells, their characteristics, and potential clinical applications. Front Immunol. 2017. https://doi.org/10.3389/fimmu.2017.00329/full.
Liu E, Marin D, Banerjee P, Macapinlac HA, Thompson P, Basar R, et al. Use of CAR-transduced natural killer cells in CD19-positive lymphoid tumors. N Engl J Med. 2020;382(6):545–53. https://doi.org/10.1056/NEJMoa1910607.
Marofi F, Al-Awad AS, Sulaiman Rahman H, Markov A, Abdelbasset WK, Ivanovna Enina Y, et al. CAR-NK cell: a new paradigm in tumor immunotherapy. Front Oncol. 2021. https://doi.org/10.3389/fonc.2021.673276/full.
Marofi F, Saleh MM, Rahman HS, Suksatan W, Al-Gazally ME, Abdelbasset WK, et al. CAR-engineered NK cells; a promising therapeutic option for treatment of hematological malignancies. Stem Cell Res Ther. 2021;12(1):374. https://doi.org/10.1186/s13287-021-02462-y.
Xie G, Dong H, Liang Y, Ham JD, Rizwan R, Chen J. CAR-NK cells: A promising cellular immunotherapy for cancer. EBioMedicine. 2020;59:102975.
Knorr DA, Ni Z, Hermanson D, Hexum MK, Bendzick L, Cooper LJN, et al. Clinical-scale derivation of natural killer cells from human pluripotent stem cells for cancer therapy. Stem Cells Transl Med. 2013;2(4):274–83. https://doi.org/10.5966/sctm.2012-0084.
Saetersmoen ML, Hammer Q, Valamehr B, Kaufman DS, Malmberg K-J. Off-the-shelf cell therapy with induced pluripotent stem cell-derived natural killer cells. Semin Immunopathol. 2019;41(1):59–68. https://doi.org/10.1007/s00281-018-0721-x.
Cichocki F, Bjordahl R, Gaidarova S, Mahmood S, Abujarour R, Wang H, et al. iPSC-derived NK cells maintain high cytotoxicity and enhance in vivo tumor control in concert with T cells and anti-PD-1 therapy. Sci Transl Med. 2020;12(568): eaaz5618. https://doi.org/10.1126/scitranslmed.aaz5618.
Li Y, Hermanson DL, Moriarity BS, Kaufman DS. Human iPSC-derived natural killer cells engineered with chimeric antigen receptors enhance anti-tumor activity. Cell Stem Cell. 2018;23(2):181.e5-1925.e5.
Zhu H, Blum RH, Bernareggi D, Ask EH, Wu Z, Hoel HJ, et al. Metabolic reprograming via deletion of CISH in human iPSC-derived NK cells promotes in vivo persistence and enhances anti-tumor activity. Cell Stem Cell. 2020;27(2):224.e6-237.e6. https://doi.org/10.1016/j.stem.2020.05.008.
Zhu H, Blum RH, Bjordahl R, Gaidarova S, Rogers P, Lee TT, et al. Pluripotent stem cell-derived NK cells with high-affinity noncleavable CD16a mediate improved antitumor activity. Blood. 2020;135(6):399–410.
Hong D, Patel S, Patel M, Musni K, Anderson M, Cooley S, et al. Preliminary results of an ongoing phase I trial of FT500, a first-in-class, off-the-shelf, induced pluripotent stem cell (iPSC) derived natural killer (NK) cell therapy in advanced solid tumors. J Immunother Cancer. 2020;8(Suppl 3):A405. https://doi.org/10.1136/jitc-2020-SITC2020.0380.
Waldmann TA. The shared and contrasting roles of IL2 and IL15 in the life and death of normal and neoplastic lymphocytes: implications for cancer therapy. Cancer Immunol Res. 2015;3(3):219–27. https://doi.org/10.1158/2326-6066.CIR-15-0009.
Rosenberg SA, Lotze MT, Muul LM, Leitman S, Chang AE, Ettinghausen SE, et al. Observations on the systemic administration of autologous lymphokine-activated killer cells and recombinant interleukin-2 to patients with metastatic cancer. N Engl J Med. 1985;313(23):1485–92. https://doi.org/10.1056/NEJM198512053132327.
Law TM, Motzer RJ, Mazumdar M, Sell KW, Walther P, O’Connell M, et al. Phase III randomized trial of interleukin-2 with or without lymphokine-activated killer cells in the treatment of patients with advanced renal cell carcinoma. Cancer. 1995;76(5):824–32. https://doi.org/10.1002/1097-0142(19950901)76:5%3C824::AID-CNCR2820760517%3E3.0.CO;2-N.
Lentsch AB, Miller FN, Edwards MJ. Mechanisms of leukocyte-mediated tissue injury induced by interleukin-2. Cancer Immunol Immunother. 1999;47(5):243–8. https://doi.org/10.1007/s002620050527.
Sim GC, Martin-Orozco N, Jin L, Yang Y, Wu S, Washington E, et al. IL-2 therapy promotes suppressive ICOS+ Treg expansion in melanoma patients. J Clin Invest. 2014;124(1):99–110.
Jiang T, Zhou C, Ren S. Role of IL-2 in cancer immunotherapy. Oncoimmunology. 2016;5(6): e1163462. https://doi.org/10.1080/2162402X.2016.1163462.
Miller JS, Morishima C, McNeel DG, Patel MR, Kohrt HEK, Thompson JA, et al. A first-in-human phase I study of subcutaneous outpatient recombinant human IL15 (rhIL15) in adults with advanced solid tumors. Clin Cancer Res. 2018;24(7):1525–35. https://doi.org/10.1158/1078-0432.CCR-17-2451.
Cooley S, He F, Bachanova V, Vercellotti GM, DeFor TE, Curtsinger JM, et al. First-in-human trial of rhIL-15 and haploidentical natural killer cell therapy for advanced acute myeloid leukemia. Blood Adv. 2019;3(13):1970–80.
Chertova E, Bergamaschi C, Chertov O, Sowder R, Bear J, Roser JD, et al. Characterization and favorable in vivo properties of heterodimeric soluble IL-15·IL-15Rα cytokine compared to IL-15 monomer*. J Biol Chem. 2013;288(25):18093–103.
Mortier E, Quéméner A, Vusio P, Lorenzen I, Boublik Y, Grötzinger J, et al. Soluble interleukin-15 receptor α (IL-15Rα)-sushi as a selective and potent agonist of IL-15 action through IL-15Rβ/γ. J Biol Chem. 2006;281(3):1612–9.
Chen X, Liu B, Han K, Kong L, Noel T, Jeng EK, et al. Combination therapy of an IL-15 superagonist complex, ALT-803, and a tumor targeting monoclonal antibody promotes direct antitumor activity and protective vaccinal effect in a syngenic mouse melanoma model. J Immunother Cancer. 2015;3(Suppl 2):P347. https://doi.org/10.1186/2051-1426-3-S2-P347.
Lo Nigro C, Macagno M, Sangiolo D, Bertolaccini L, Aglietta M, Merlano MC. NK-mediated antibody-dependent cell-mediated cytotoxicity in solid tumors: biological evidence and clinical perspectives. Ann Transl Med. 2019;7(5):105–105.
Glassman PM, Balthasar JP. Mechanistic considerations for the use of monoclonal antibodies for cancer therapy. Cancer Biol Med. 2014;11(1):20–33.
Smith MR. Rituximab (monoclonal anti-CD20 antibody): mechanisms of action and resistance. Oncogene. 2003;22(47):7359–68.
Fornasier G, Francescon S, Baldo P. An update of efficacy and safety of cetuximab in metastatic colorectal cancer: a narrative review. Adv Ther. 2018;35(10):1497–509. https://doi.org/10.1007/s12325-018-0791-0.
Van den Nest M, Glechner A, Gold M, Gartlehner G. The comparative efficacy and risk of harms of the intravenous and subcutaneous formulations of trastuzumab in patients with HER2-positive breast cancer: a rapid review. Syst Rev. 2019;8(1):321. https://doi.org/10.1186/s13643-019-1235-x.
Hoy SM. Dinutuximab: a review in high-risk neuroblastoma. Target Oncol. 2016;11(2):247–53. https://doi.org/10.1007/s11523-016-0420-2.
Salomon-Perzyński A, Walter-Croneck A, Usnarska-Zubkiewicz L, Dytfeld D, Zielińska P, Wojciechowska M, et al. Efficacy of daratumumab monotherapy in real-world heavily pretreated patients with relapsed or refractory multiple myeloma. Adv Med Sci. 2019;64(2):349–55.
Nimmerjahn F, Ravetch JV. Fcγ receptors as regulators of immune responses. Nat Rev Immunol. 2008;8(1):34–47.
Weng W-K, Levy R. Two immunoglobulin G fragment C receptor polymorphisms independently predict response to rituximab in patients with follicular lymphoma. J Clin Oncol. 2003;21(21):3940–7. https://doi.org/10.1200/JCO.2003.05.013.
Varchetta S, Gibelli N, Oliviero B, Nardini E, Gennari R, Gatti G, et al. Elements related to heterogeneity of antibody-dependent cell cytotoxicity in patients under trastuzumab therapy for primary operable breast cancer overexpressing Her2. Cancer Res. 2007;67(24):11991–9. https://doi.org/10.1158/0008-5472.CAN-07-2068.
Saunders KO. Conceptual approaches to modulating antibody effector functions and circulation half-life. Front Immunol. 2019. https://doi.org/10.3389/fimmu.2019.01296/full.
Klanova M, Oestergaard MZ, Trněný M, Hiddemann W, Marcus R, Sehn LH, et al. Prognostic impact of natural killer cell count in follicular lymphoma and diffuse large B-cell lymphoma patients treated with immunochemotherapy. Clin Cancer Res. 2019;25(15):4634–43. https://doi.org/10.1158/1078-0432.CCR-18-3270.
Arnould L, Gelly M, Penault-Llorca F, Benoit L, Bonnetain F, Migeon C, et al. Trastuzumab-based treatment of HER2-positive breast cancer: an antibody-dependent cellular cytotoxicity mechanism? Br J Cancer. 2006;94(2):259–67.
Long EO. Negative signaling by inhibitory receptors: the NK cell paradigm. Immunol Rev. 2008;224(1):70–84. https://doi.org/10.1111/j.1600-065X.2008.00660.x.
Wei SC, Duffy CR, Allison JP. Fundamental mechanisms of immune checkpoint blockade therapy. Cancer Discov. 2018;8(9):1069–86. https://doi.org/10.1158/2159-8290.CD-18-0367.
Liu X, Hogg GD, DeNardo DG. Rethinking immune checkpoint blockade: ‘Beyond the T cell.’ J Immunother Cancer. 2021;9(1): e001460. https://doi.org/10.1136/jitc-2020-001460.
Cao Y, Wang X, Jin T, Tian Y, Dai C, Widarma C, et al. Immune checkpoint molecules in natural killer cells as potential targets for cancer immunotherapy. Signal Transduct Target Ther. 2020;5(1):250.
Pesce S, Greppi M, Tabellini G, Rampinelli F, Parolini S, Olive D, et al. Identification of a subset of human natural killer cells expressing high levels of programmed death 1: a phenotypic and functional characterization. J Allergy Clin Immunol. 2017;139(1):335.e3-346.e3.
Concha-Benavente F, Kansy B, Moskovitz J, Moy J, Chandran U, Ferris RL. PD-L1 mediates dysfunction in activated PD-1 + NK cells in head and neck cancer patients. Cancer Immunol Res. 2018;6(12):1548–60. https://doi.org/10.1158/2326-6066.CIR-18-0062.
Mariotti FR, Petrini S, Ingegnere T, Tumino N, Besi F, Scordamaglia F, et al. PD-1 in human NK cells: evidence of cytoplasmic mRNA and protein expression. Oncoimmunology. 2019;8(3):1557030. https://doi.org/10.1080/2162402X.2018.1557030.
Quatrini L, Wieduwild E, Escaliere B, Filtjens J, Chasson L, Laprie C, et al. Endogenous glucocorticoids control host resistance to viral infection through the tissue-specific regulation of PD-1 expression on NK cells. Nat Immunol. 2018;19(9):954–62.
Hsu J, Hodgins JJ, Marathe M, Nicolai CJ, Bourgeois-Daigneault M-C, Trevino TN, et al. Contribution of NK cells to immunotherapy mediated by PD-1/PD-L1 blockade. J Clin Invest. 2018;128(10):4654–68.
Pomeroy EJ, Hunzeker JT, Kluesner MG, Lahr WS, Smeester BA, Crosby MR, et al. A genetically engineered primary human natural killer cell platform for cancer immunotherapy. Mol Ther. 2019;28(1):52–63. https://doi.org/10.1016/j.ymthe.2019.10.009.
Judge SJ, Dunai C, Aguilar EG, Vick SC, Sturgill IR, Khuat LT, et al. Minimal PD-1 expression in mouse and human NK cells under diverse conditions. J Clin Invest. 2020;130(6):3051–68.
Davis Z, Felices M, Lenvik T, Badal S, Walker JT, Hinderlie P, et al. Low-density PD-1 expression on resting human natural killer cells is functional and upregulated after transplantation. Blood Adv. 2021;5(4):1069–80.
Pende D, Falco M, Vitale M, Cantoni C, Vitale C, Munari E, et al. Killer Ig-like receptors (KIRs): their role in NK cell modulation and developments leading to their clinical exploitation. Front Immunol. 2019;May 28:10;1179.
Anfossi N, André P, Guia S, Falk CS, Roetynck S, Stewart CA, et al. Human NK cell education by inhibitory receptors for MHC class I. Immunity. 2006;25(2):331–42.
Vey N, Bourhis J-H, Boissel N, Bordessoule D, Prebet T, Charbonnier A, et al. A phase 1 trial of the anti-inhibitory KIR mAb IPH2101 for AML in complete remission. Blood. 2012;120(22):4317–23.
Benson DM, Hofmeister CC, Padmanabhan S, Suvannasankha A, Jagannath S, Abonour R, et al. A phase 1 trial of the anti-KIR antibody IPH2101 in patients with relapsed/refractory multiple myeloma. Blood. 2012.;120(22):4324–33.
Korde N, Carlsten M, Lee M-J, Minter A, Tan E, Kwok M, et al. A phase II trial of pan-KIR2D blockade with IPH2101 in smoldering multiple myeloma. Haematologica. 2014;99(6):e81–3. https://doi.org/10.3324/haematol.2013.103085.
Carlsten M, Korde N, Kotecha R, Reger R, Bor S, Kazandjian D, et al. Checkpoint inhibition of KIR2D with the monoclonal antibody IPH2101 induces contraction and hyporesponsiveness of NK cells in patients with myeloma. Clin Cancer Res. 2016;22(21):5211–22. https://doi.org/10.1158/1078-0432.CCR-16-1108.
Sáez-Borderías A, Romo N, Magri G, Gumá M, Angulo A, López-Botet M. IL-12-dependent inducible expression of the CD94/NKG2A inhibitory receptor regulates CD94/NKG2C + NK cell function. J Immunol. 2009;182(2):829–36. https://doi.org/10.4049/jimmunol.182.2.829.
Kamiya T, Seow SV, Wong D, Robinson M, Campana D. Blocking expression of inhibitory receptor NKG2A overcomes tumor resistance to NK cells. J Clin Invest. 2019;129(5):2094–106.
André P, Denis C, Soulas C, Bourbon-Caillet C, Lopez J, Arnoux T, et al. Anti-NKG2A mAb is a checkpoint inhibitor that promotes anti-tumor immunity by unleashing both T and NK cells. Cell. 2018;175(7):1731.e13-1743.e13.
Yu J, Heller G, Chewning J, Kim S, Yokoyama WM, Hsu KC. Hierarchy of the human natural killer cell response is determined by class and quantity of inhibitory receptors for self-HLA-B and HLA-C ligands. J Immunol. 2007;179(9):5977–89. https://doi.org/10.4049/jimmunol.179.9.5977.
Fernandez NC, Treiner E, Vance RE, Jamieson AM, Lemieux S, Raulet DH. A subset of natural killer cells achieves self-tolerance without expressing inhibitory receptors specific for self-MHC molecules. Blood. 2005;105(11):4416–23.
Highton AJ, Diercks B-P, Möckl F, Martrus G, Sauter J, Schmidt AH, et al. High metabolic function and resilience of NKG2A-educated NK cells. Front Immunol. 2020. https://doi.org/10.3389/fimmu.2020.559576/full.
Meng F, Li L, Lu F, Yue J, Liu Z, Zhang W, et al. Overexpression of TIGIT in NK and T cells contributes to tumor immune escape in myelodysplastic syndromes. Front Oncol. 2020. https://doi.org/10.3389/fonc.2020.01595/full.
Ndhlovu LC, Lopez-Vergès S, Barbour JD, Jones RB, Jha AR, Long BR, et al. Tim-3 marks human natural killer cell maturation and suppresses cell-mediated cytotoxicity. Blood. 2012;119(16):3734–43.
Chou F-C, Chen H-Y, Kuo C-C, Sytwu H-K. Role of Galectins in Tumors and in Clinical Immunotherapy. Int J Mol Sci. 2018;19(2):430.
Sun H, Sun C, Xiao W. Expression regulation of co-inhibitory molecules on human natural killer cells in response to cytokine stimulations. Cytokine. 2014;65(1):33–41.
Sarhan D, Cichocki F, Zhang B, Yingst A, Spellman SR, Cooley S, et al. Adaptive NK cells with low TIGIT expression are inherently resistant to myeloid-derived suppressor cells. Cancer Res. 2016;76(19):5696–706.
Zhang Q, Bi J, Zheng X, Chen Y, Wang H, Wu W, et al. Blockade of the checkpoint receptor TIGIT prevents NK cell exhaustion and elicits potent anti-tumor immunity. Nat Immunol. 2018;19(7):723–32.
Ellwanger K, Reusch U, Fucek I, Wingert S, Ross T, Müller T, et al. Redirected optimized cell killing (ROCK®): a highly versatile multispecific fit-for-purpose antibody platform for engaging innate immunity. MAbs. 2019;11(5):899–918. https://doi.org/10.1080/19420862.2019.1616506.
Rothe A, Sasse S, Topp MS, Eichenauer DA, Hummel H, Reiners KS, et al. A phase 1 study of the bispecific anti-CD30/CD16A antibody construct AFM13 in patients with relapsed or refractory Hodgkin lymphoma. Blood. 2015;125(26):4024–31.
Bartlett NL, Herrera AF, Domingo-Domenech E, Mehta A, Forero-Torres A, Garcia-Sanz R, et al. A phase 1b study of AFM13 in combination with pembrolizumab in patients with relapsed or refractory Hodgkin lymphoma. Blood. 2020;136(21):2401–9.
Reusch U, Damrat M, Wingert S, Knackmuss SHJ, Mueller T, Fucek I, et al. Abstract 5659: AFM24, a bispecific EGFR/CD16A innate cell engager with the potential to overcome resistance to current targeted treatments for EGFR-positive malignancies. Abstract In: Immunology. American Association for Cancer Research; 2020. p. 5659. https://doi.org/10.1158/1538-7445.AM2020-5659.
Kakiuchi-Kiyota S, Schutten MM, Adedeji AO, Cai H, Hendricks R, Liu L, et al. Abstract 4556: preclinical pharmacology and safety of RO7297089, a novel anti-BCMA/CD16a bispecific antibody for the treatment of multiple myeloma. Abstract In: Immunology. American Association for Cancer Research; 2020. p. 4556. https://doi.org/10.1158/1538-7445.AM2020-4556.
Merck & Co. Partners with dragonfly on NK-based cancer immunotherapies. Genetic Engineering and Biotechnology News. 2018 [cited 2021 Mar 4].
Demaria O, Gauthier L, Debroas G, Vivier E. Natural killer cell engagers in cancer immunotherapy: next generation of immuno-oncology treatments. Eur J Immunol. 2021. https://doi.org/10.1002/eji.202048953.
Gauthier L, Morel A, Anceriz N, Rossi B, Blanchard-Alvarez A, Grondin G, et al. Multifunctional natural killer cell engagers targeting NKp46 trigger protective tumor immunity. Cell. 2019;177(7):1701-1713.e16.
Cytovia therapeutics files new patents for its natural killer cell engager multifunctional antibodies (FLEX-NK®) for the treatment of hematological and solid tumors [Internet]. globenewswire.com. [cited 2021 Jul 7].
Watkins-Yoon J, Guzman W, Oliphant A, Haserlat S, Leung A, Chottin C, et al. CTX-8573, an innate-cell engager targeting BCMA, is a highly potent multispecific antibody for the treatment of multiple myeloma. Blood. 2019;134(Supplement_1):3182–3182.
Felices M, Lenvik TR, Davis ZB, Miller JS, Vallera DA. Generation of BiKEs and TriKEs to improve NK cell-mediated targeting of tumor cells. Am J Gastroenterol. 2016:333–46.
Gleason MK, Verneris MR, Todhunter DA, Zhang B, McCullar V, Zhou SX, et al. Bispecific and trispecific killer cell engagers directly activate human NK cells through CD16 signaling and induce cytotoxicity and cytokine production. Mol Cancer Ther. 2012;11(12):2674–84.
Felices M, Kodal B, Hinderlie P, Kaminski MF, Cooley S, Weisdorf DJ, et al. Novel CD19-targeted TriKE restores NK cell function and proliferative capacity in CLL. Blood Adv. 2019;3(6):897–907.
Wiernik A, Foley B, Zhang B, Verneris MR, Warlick E, Gleason MK, et al. Targeting natural killer cells to acute myeloid leukemia in vitro with a CD16 × 33 bispecific killer cell engager and ADAM17 inhibition. Clin Cancer Res. 2013;19(14):3844–55.
Vallera DA, Felices M, McElmurry R, McCullar V, Zhou X, Schmohl JU, et al. IL15 trispecific killer engagers (TriKE) make natural killer cells specific to CD33+ targets while also inducing persistence, in vivo expansion, and enhanced function. Clin Cancer Res. 2016;22(14):3440–50.
Felices M, Lenvik TR, Kodal B, Lenvik AJ, Hinderlie P, Bendzick LE, et al. Potent cytolytic activity and specific IL15 delivery in a 2nd generation trispecific killer engager. Cancer Immunol Res. 2020;8(9):1139–49.
Arvindam US, van Hauten PMM, Schirm D, Schaap N, Hobo W, Blazar BR, et al. A trispecific killer engager molecule against CLEC12A effectively induces NK-cell mediated killing of AML cells. Leukemia. 2020. https://doi.org/10.1038/s41375-020-01065-5.
Yun HD, Felices M, Vallera DA, Hinderlie P, Cooley S, Arock M, et al. Trispecific killer engager CD16 × IL15 × CD33 potently induces NK cell activation and cytotoxicity against neoplastic mast cells. Blood Adv. 2018;2(13):1580–4.
Schmohl JU, Felices M, Taras E, Miller JS, Vallera DA. Enhanced ADCC and NK cell activation of an anticarcinoma bispecific antibody by genetic insertion of a modified IL-15 cross-linker. Mol Ther. 2016;24(7):1312–22.
Schmohl JU, Gleason MK, Dougherty PR, Miller JS, Vallera DA. Heterodimeric bispecific single chain variable fragments (scFv) killer engagers (BiKEs) enhance NK-cell activity against CD133+ colorectal cancer cells. Target Oncol. 2016;11(3):353–61. https://doi.org/10.1007/s11523-015-0391-8.
Schmohl JU, Felices M, Oh F, Lenvik AJ, Lebeau AM, Panyam J, et al. Engineering of anti-CD133 trispecific molecule capable of inducing NK expansion and driving antibody-dependent cell-mediated cytotoxicity. Cancer Res Treat. 2017;49(4):1140–52.
Schmohl JU, Felices M, Todhunter D, Taras E, Miller JS, Vallera DA. Tetraspecific scFv construct provides NK cell mediated ADCC and self-sustaining stimuli via insertion of IL-15 as a cross-linker. Oncotarget. 2016;7(45):73830–44.
Vallera DA, Zhang B, Gleason MK, Oh S, Weiner LM, Kaufman DS, et al. Heterodimeric bispecific single-chain variable-fragment antibodies against EpCAM and CD16 induce effective antibody-dependent cellular cytotoxicity against human carcinoma cells. Cancer Biother Radiopharm. 2013;28(4):274–82.
Vallera DA, Ferrone S, Kodal B, Hinderlie P, Bendzick L, Ettestad B, et al. NK-cell-mediated targeting of various solid tumors using a B7–H3 tri-specific killer engager in vitro and in vivo. Cancers (Basel). 2020;12(9):1–18.
Davis ZB, Vallera DA, Miller JS, Felices M. Natural killer cells unleashed: checkpoint receptor blockade and BiKE/TriKE utilization in NK-mediated anti-tumor immunotherapy. Semin Immunol. 2017;31(September):64–75.
Chen X, Zaro JL, Shen W-C. Fusion protein linkers: property, design and functionality. Adv Drug Deliv Rev. 2013;65(10):1357–69.
Huston JS, Levinson D, Mudgett-Hunter M, Tai MS, Novotny J, Margolies MN, et al. Protein engineering of antibody binding sites: recovery of specific activity in an anti-digoxin single-chain Fv analogue produced in Escherichia coli. Proc Natl Acad Sci. 1988;85(16):5879–83. https://doi.org/10.1073/pnas.85.16.5879.
Trinh R, Gurbaxani B, Morrison SL, Seyfzadeh M. Optimization of codon pair use within the (GGGGS)3 linker sequence results in enhanced protein expression. Mol Immunol. 2004;40(10):717–22.
Gopal GJ, Kumar A. Strategies for the production of recombinant protein in Escherichia coli. Protein J. 2013;32(6):419–25.
Burgess RR. Refolding solubilized inclusion body proteins. Methods Enzymol. 2009;463:259–82.
Akama-Garren EH, Joshi NS, Tammela T, Chang GP, Wagner BL, Lee D-Y, et al. A modular assembly platform for rapid generation of DNA constructs. Sci Rep. 2016;6(1):16836.
Topp MS, Gökbuget N, Stein AS, Zugmaier G, O’Brien S, Bargou RC, et al. Safety and activity of blinatumomab for adult patients with relapsed or refractory B-precursor acute lymphoblastic leukaemia: a multicentre, single-arm, phase 2 study. Lancet Oncol. 2015;16(1):57–66.
Steel JC, Waldmann TA, Morris JC. Interleukin-15 biology and its therapeutic implications in cancer. Trends Pharmacol Sci. 2012;33(1):35–41.
Cheng Y, Zheng X, Wang X, Chen Y, Wei H, Sun R, et al. Trispecific killer engager 161519 enhances natural killer cell function and provides anti-tumor activity against CD19-positive cancers. Cancer Biol Med. 2020;17(4):1026–38.
Baeuerle PA, Gires O. EpCAM (CD326) finding its role in cancer. Br J Cancer. 2007;96(3):417–23.
Glumac PM, LeBeau AM. The role of CD133 in cancer: a concise review. Clin Transl Med. 2018;7(1):18.
Melaiu O, Lucarini V, Cifaldi L, Fruci D. Influence of the tumor microenvironment on NK cell function in solid tumors. Front Immunol. 2020. https://doi.org/10.3389/fimmu.2019.03038/full.
Gleason MK, Ross JA, Warlick ED, Lund TC, Verneris MR, Wiernik A, et al. CD16xCD33 bispecific killer cell engager (BiKE) activates NK cells against primary MDS and MDSC CD33+ targets. Blood. 2014;123(19):3016–26.
Bruno A, Mortara L, Baci D, Noonan DM, Albini A. Myeloid derived suppressor cells interactions with natural killer cells and pro-angiogenic activities: roles in tumor progression. Front Immunol. 2019;10(April):771.
Sarhan D, Brandt L, Felices M, Guldevall K, Lenvik T, Hinderlie P, et al. 161533 TriKE stimulates NK-cell function to overcome myeloid-derived suppressor cells in MDS. Blood Adv. 2018;2(12):1459–69.
Warlick ED, Weisdorf DJ, Vallera DA, Wangen R, Lewis D, Knox J, et al. GTB-3550 TriKETM for the treatment of high-risk myelodysplastic syndromes (MDS) and refractory/relapsed acute myeloid leukemia (AML) safely drives natural killer (NK) cell proliferation at initial dose cohorts. In: Blood. 2020. p. 7–8. Available from: https://ash.confex.com/ash/2020/webprogram/Paper136398.html.
Conlon KC, Potter EL, Pittaluga S, Lee C-CR, Miljkovic MD, Fleisher TA, et al. IL15 by continuous intravenous infusion to adult patients with solid tumors in a phase I trial induced dramatic NK-cell subset expansion. Clin Cancer Res. 2019;25(16):4945–54. https://doi.org/10.1158/1078-0432.CCR-18-3468.
Baeuerle PA, Kufer P, Bargou R. BiTE: teaching antibodies to engage T-cells for cancer therapy. Curr Opin Mol Ther. 2009;11(1):22–30.
Morsink LM, Walter RB, Ossenkoppele GJ. Prognostic and therapeutic role of CLEC12A in acute myeloid leukemia. Blood Rev. 2019;34:26–33.
Zheng B, Yu S-F, del Rosario G, Leong SR, Lee GY, Vij R, et al. An Anti-CLL-1 antibody–drug conjugate for the treatment of acute myeloid leukemia. Clin Cancer Res. 2019;25(4):1358–68. https://doi.org/10.1158/1078-0432.CCR-18-0333.
Jiang Y-P, Liu BY, Zheng Q, Panuganti S, Chen R, Zhu J, et al. CLT030, a leukemic stem cell-targeting CLL1 antibody-drug conjugate for treatment of acute myeloid leukemia. Blood Adv. 2018;2(14):1738–49.
Wang J, Chen S, Xiao W, Li W, Wang L, Yang S, et al. CAR-T cells targeting CLL-1 as an approach to treat acute myeloid leukemia. J Hematol Oncol. 2018;11(1):7. https://doi.org/10.1186/s13045-017-0553-5.
Dong P, Xiong Y, Yue J, Hanley SJB, Watari H. B7H3 as a promoter of metastasis and promising therapeutic target. Front Oncol. 2018;8:264.
Holliger P, Hudson PJ. Engineered antibody fragments and the rise of single domains. Nat Biotechnol. 2005;23(9):1126–36.
Chames P, Van Regenmortel M, Weiss E, Baty D. Therapeutic antibodies: successes, limitations and hopes for the future. Br J Pharmacol. 2009;157(2):220–33.
Scott AM, Wolchok JD, Old LJ. Antibody therapy of cancer. Nat Rev Cancer. 2012;12(4):278–87.
Conlon KC, Lugli E, Welles HC, Rosenberg SA, Fojo AT, Morris JC, et al. Redistribution, hyperproliferation, activation of natural killer cells and CD8 T cells, and cytokine production during first-in-human clinical trial of recombinant human interleukin-15 in patients with cancer. J Clin Oncol. 2015;33(1):74–82. https://doi.org/10.1200/JCO.2014.57.3329.
Bryceson YT, Ljunggren H-G, Long EO. Minimal requirement for induction of natural cytotoxicity and intersection of activation signals by inhibitory receptors. Blood. 2009;114(13):2657–66.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
This work was supported, in part, by US Department of Defense PC190189, NCI P01 CA111412 and R35 CA197292.
Conflict of interest
Dr. Felices and Dr. Miller receive consulting honoraria, royalties and/or own stock from GT Biopharma, who licenses the TriKETM platform from the University of Minnesota. These interests have been reviewed and managed by the University of Minnesota in accordance with its conflict-of-interest policy.
Ethics approval
Not applicable
Consent
Not applicable
Author contributions
SKP wrote and edited manuscript; JSM and MF supervised, reviewed, wrote, and organized manuscript.
Data availability
Not applicable.
Rights and permissions
About this article

Cite this article
Phung, S.K., Miller, J.S. & Felices, M. Bi-specific and Tri-specific NK Cell Engagers: The New Avenue of Targeted NK Cell Immunotherapy. Mol Diagn Ther 25, 577–592 (2021). https://doi.org/10.1007/s40291-021-00550-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40291-021-00550-6