
Abstract
Introduction
Clinical pharmacology QT/QTc studies can be smaller if they more efficiently use the data generated.
Objective
The aim was to use large sets of electrocardiograms (ECGs) deposited at the US Food and Drug Administration to investigate the implications of heart rate measurement on the accuracy of QTc data.
Methods
Using the data of 80 thorough QT studies, we investigated whether placing study subjects in supine positions during short-term time points stabilizes heart rate (part I, based on 73 studies with 747,912 measured ECGs in 6786 healthy subjects) and whether heart rate measurements different from RR intervals captured simultaneously with QT intervals decrease QTc variability (part II, based on seven studies with 897,570 ECG measurements in 751 healthy subjects).
Results
In the part I data, when subjects were placed in supine undisturbed positions, heart rate instability (max–min of repeatedly measured heart rates within the same study time point) exceeding 5 beats per minute (bpm) was observed 40 % of the time and exceeded 10 bpm 10 % of the time. In the part II data, even when including QT measurements preceded by variable heart rates, correction of QT durations for RR interval values derived through a simple QT/RR hysteresis model with 95 % adaptation in 120 s led to mean intra-subject standard deviation of QTc (Fridericia formula) of only 7.14 ± 1.98 and 6.38 ± 1.50 ms in women and men, respectively.
Conclusion
The QT/RR hysteresis model with 95 % adaptation in 120 s is universally applicable to healthy subjects, providing small QTc variability. Supine positions do not generally stabilize heart rates in healthy subjects. Universally applicable QT/RR hysteresis correction allows clinical QT/QTc studies to include variable heart rate episodes in the time points.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Contrary to the present design of thorough QT/QTc studies, placing healthy subjects into undisturbed supine positions does not stabilize heart rates even over short (i.e., 1- to 3-min) analysis windows. |
A universally applicable correction for QT/RR hysteresis with a 95 % constant of 120 s provides RR′ values for QT interval heart rate correction that are little different from RR′ values based on individually optimized QT/RR hysteresis corrections. |
Universal correction for QT/RR hysteresis allows clinical pharmacology QT/QTc studies to include QT measurements that are preceded by variable heart rates. |
1 Introduction
While investigation of drug-induced QT/QTc interval changes is mandated for practically all new pharmaceuticals [1], the design of relevant investigations is under constant evolution. Different innovations have been proposed to modify the concept of thorough QT studies (TQTS), but all expect the assessment of drug-induced QT/QTc changes to be based on small studies, possibly first-in-man investigations [2]. Achieving results with narrow confidence limits with small sample sizes requires optimum use of available data.
This is well understood, and the accuracy of QT interval measurements receives attention in pharmaceutical studies. Lesser attention is usually paid to the measurement of heart rate (HR) for QT interval correction. Among other considerations, while QT interval dependency on HR (i.e., how much QT interval changes when HR changes) is practically always incorporated into QT interval correction, the speed of QT interval HR adaptation (the so-called QT/RR hysteresis, i.e., how quickly QT interval changes when HR changes) is frequently neglected.
Most frequently, TQTS place investigated subjects into a supine position during protocol-specified analysis windows around the sample times for plasma drug levels (e.g., of 5-min duration), during which repeated (e.g., triplicate) measurements are made. This is based on the expectation that keeping the subjects in supine positions stabilizes HR over the analysis window so that the effects of QT/RR hysteresis can be neglected and that simple short-term data of QT/RR interval pairs are sufficient, especially if a few such pairs are averaged at each measurement.
Using the data of previously conducted TQTS, the electrocardiograms (ECGs) of which were deposited in the ECG warehouse of the USA Food and Drug Administration (FDA) [3], we investigated (part I) whether placing study subjects in supine positions indeed stabilizes HR and (part II) whether different HR measurement methods decrease QTc variability.
2 Methods
We used data of TQTS previously conducted in healthy volunteers. All source studies were conducted according to approved protocols, and all of them reported that all participants gave informed written consent. Since we used only drug-free parts of the investigations, the specific details of the investigated drugs are irrelevant.
2.1 Source Studies
2.1.1 Part I Studies
Part I used the data of 73 TQTS submitted to the ECG warehouse of the FDA between 2005 and 2012. These studies were all crossover TQTS and had multiple drug-free ECG measurements made at each period. The studies were used both individually and with their ECG measurements and subjects pooled. Altogether, these studies investigated 6786 subjects (range per study 19–339, mean age 32.14 ± 10.14 years), of whom 2806 (41.3 %) were women (0–139 per study). The submissions of the studies to the warehouse contained 747,912 ECG samples and their drug-free (baseline + placebo) measurements (558–50,211 per study) in 207,846 individual per-protocol analysis windows (336–6070 per study). In all studies, the subjects were positioned, per protocol, in undisturbed supine positions during analysis windows. The majority of the studies (n = 46) used triplicate ECG measurements per analysis window, one study used duplicated measurements, and 26 studies used four or more time-point replicates. The average of mean durations of study time points (the interval between the first and the last measured ECG within the same analysis window) was 158 s (39–482 s per study). Data on ECG times and QT and RR interval durations reported by study sponsors were used.
2.1.2 Part II Studies
For part II, we used a pooled data set of seven TQTS conducted between 2004 and 2013 that all included QT interval data together with 5-min RR interval histories before each QT measurement derived from continuous 12-lead ECGs. These were all the studies available to us with data of this kind. Altogether, these studies investigated 751 subjects (mean age 34.18 ± 9.56 years, 311 women). All the seven studies followed practically the same protocol for obtaining detailed characteristics of subject-specific QT/RR relationship during drug-free baselines. In each subject, multiple baseline recordings were used and thus, in addition to per-protocol analysis windows, free scans of the continuous ECGs were made to measure QT intervals at different HR [4]. The baseline days of the studies also included postural provocative maneuvers to achieve wide HR spans. This pool of the seven studies contained 897,570 drug-free ECG measurements (QT interval + RR history, range 321–1560 per subject).
2.2 Data Analyses
Since we used only drug-free ECG measurements with no systematic HR changes expected, we used primarily Fridericia correction to derive the QTcF values [4, 5]. As small QT studies require reduced variability of QTc data, we have used the intra-subject standard deviation (SD) of QTcF values as the metric characterizing the QTcF data quality.
2.2.1 Part I Analyses
In the part I data, two analytical steps were carried out.
Firstly, we assessed HR instability within analysis windows by calculating the HR ranges (max–min) in repeated ECG measurements of the same time point [reported RR intervals were converted to HR in beats per minute (bpm)]. For each study, the time-point HR instability was characterized by median, 75 and 90 percentiles of these ranges. For each subject, the mean of the HR ranges over different analysis windows characterized a subject’s HR instability. Similarly, the mean and upper percentiles of HR instability in the data of a study characterized the HR instability in the given study (e.g., influenced by the diligence of study conduct).
Secondly, we investigated how the HR instabilities in analysis windows were related to the intra-subject SD of QTcF, both per subject and per study. In each subject and each study, we also investigated the percentage of analysis windows in which the HR ranges exceeded 5 and 10 bpm.
2.2.2 Part II Analyses
Since the baseline day protocols of part II studies were practically identical, we pooled all the subjects together. Four analytical steps were performed with the part II data.
Firstly, we divided all the QT measurements into those that were per protocol selected from long-term ECG recordings aiming at identifying episodes preceded by stable HR (ideally ±2 bpm differences in the preceding 2 min, but this included episodes within per-protocol analysis windows where the HR stability was not always achieved) and those selected per protocol aiming at finding episodes preceded by variable HR. For these separately and pooled together, we investigated intra-subject SD of QTcF when correcting the QT measurements for (a) the average of N preceding RR intervals and (b) the average of RR intervals over preceding N seconds, varying N in both cases from 1 to 300.
Secondly, we investigated intra-subject SD of QTcF when correcting the QT measurements for the RR′ values (i.e., the weighted averages of RR intervals preceding QT interval measurement) derived from the 5-min histories using the exponential decay models of QT/RR hysteresis [6, 7] (see the Sect. 5 for details). For this purpose, we considered models assuming QT adaptation driven by a number of cardiac cycles and by elapsed time, varying the 95 % hysteresis constant (the interval of 95 % adaptation of QT interval duration) between 20 and 280 cardiac cycles and 20 and 280 s, respectively. From this analysis, we derived a global model of QT/RR hysteresis, i.e., the model that led to the minimum averaged intra-subject SD of QTcF.
Thirdly, individually optimized models of QT/RR hysteresis and individually optimized HR corrections were also available in part II, derived by previously published technologies [8]. The individually optimized HR corrections involved both optimization of QT/RR curvatures [9] (providing QTcI values) and optimization of a universal parabolic correction model in the form of QTc = QT/RRβ. Using these, we investigated the differences between the hysteresis derived RR′ values obtained with the global model and the individually optimized models, and the differences between the QTcI and QTcF values. For the purposes of distinguishing the QTc differences caused by replacing subject-specific QT/RR hysteresis models with the global model from the differences caused by replacing subject-specific QT/RR correction formula with the Fridericia formula, we calculated QTcF values twice, that is using the RR′ value derived by the subject-specific QT/RR hysteresis model and by the global QT/RR hysteresis model.
Finally, we investigated the differences between the intra-subject SD of QTcF derived from the global hysteresis correction with the Fridericia formula and the intra-subject SD of QTcI derived from individually optimized hysteresis and HR corrections.
2.3 Statistics
All analyses were performed separately for male and female subpopulations of part I and II data sets. Descriptive data are presented as mean ± SD, with cumulative distributions compared by Kolmogorov–Smirnov test where appropriate. Linear regressions are reported with 95 % confidence intervals and accompanied by Pearson correlation coefficients. Within-subject changes in SD of QTc were compared using Wilcoxon matched pairs test. Mutually corresponding data sets were also displayed using Bland–Altman-like graphs.
3 Results
3.1 Part I
3.1.1 Distribution of Heart Rate Instability
Figure 1 summarizes the HR instability data in the pool of part I studies. In the pooled data, there were more than 40 and 10 % of the study analysis windows with HR ranges exceeding 5 and 10 bpm, respectively (Fig. 1c). Not surprisingly, the HR ranges were correlated with the mean HR of the time points (r = 0.281 and r = 0.280 in females and males, respectively; Fig. 1a, b), but contrary to our expectations that HR measurements more distant from each other are more likely to be different, they were not related to the differences between the times at which the maximum and minimum HRs were measured in the same analysis window (r = 0.012 and r = −0.001 in women and men, respectively; Fig. 1d, e).

Panels a (women) and b (men) show the relationship between mean heart rate and heart rate instability (i.e., the max–min range of heart rates measured within the ECG multiplets of the same study time point) in individual time points. Panels d (women) and e (men) show the relationship between time span between maximum and minimum heart rates and heart rate instability in individual time points (pooled data of all part I studies). Panel c shows, for individual part I subjects, the cumulative distribution of the proportions of study time points in which the heart rate instability exceeded 5 bpm (full bold lines) and 10 bpm (dotted lines), e.g., heart rate instability above 5 bpm in more than 30 % of measured study time points was seen in approximately 70 % of all part I subjects. Panel f shows the same for individual part I studies (note that in panel c, similar to panel f, all curves end at 100 % frequency for 0 % of measured time points. There were 6.1 % female subjects and 4.5 % male subjects in whom all the study time points had heart rate instability below 5 bpm; for the 10-bpm threshold, these numbers were 28.4 % and 26.7 %, respectively). Panel g shows the distributions of median (dotted lines), 75 percentiles (dashed lines) and 90 percentiles (full lines) of heart rate instability in individual part I studies. Panel h shows the cumulative distributions of mean (full lines), minimum (dashed and dotted lines) and maximum (dotted lines) of heart rate instability in all part I subjects. Panel i summarizes mean heart rate instability in individual part I subjects and shows the distribution of their means (full lines), minima (dashed and dotted lines) and maxima (dotted lines) calculated within individual part I studies. In panels c, f, g, h, and i, the red and blue lines correspond to the data in women and men, respectively. bpm Beats per minute, ECG electrocardiogram
Nevertheless, these global observations did not apply to individual studies equally, with substantial differences in the within-analysis-window HR instability study to study. Similarly, there were differences between individual subjects, including those participating in the same study. Pooling all part I subjects together, there were only 6.1 % of women and 4.5 % of men in whom the HR instability in all analysis windows did not exceed 5 bpm. For HR instability not exceeding 10 bpm, the corresponding numbers were 28.4 and 26.7 % (Fig. 1c, h). On the contrary, 20 % of all the women and 20 % of all the men had HR instability exceeding 5 bpm in 65.5 and 66.7 % of the analysis windows (Fig. 1c). One half of the studies had HR instability exceeding 5 bpm in 41.6 and 39.7 % of analysis windows in women and men, respectively (Fig. 1f).
Looking at the data differently, there were 20 (27.0 %) and 19 studies (25.7 %) in which the median of HR instability exceeded 5 bpm in women and men, respectively, and 29 (39.2 %) and 25 studies (33.8 %) in which HR instability of more than 10 % of the analysis windows exceeded 10 bpm in women and men, respectively (Fig. 1g). When characterizing each subject by the mean HR instability over all analysis windows and calculating the mean of these characteristics for each study, this mean of means exceeded 5 bpm in 43.9 and 49.5 % of studies for women and men, respectively (Fig. 1i).
Statistical comparisons between women and men were performed for characteristics of individual studies. Of these, the distributions of HR median, 75 and 90 percentiles of HR instability per study (Fig. 1g) were statistically significantly different in women and men (p < 0.001). However, the numerical differences were small and of no practical implication.
3.1.2 Relationship Between Heart Rate Instability and QTcF Variability
Figure 2 shows the associations between HR instability and QTcF variability. As expected (Fig. 2a, b), the larger the HR instability in an analysis window, the larger the range (max–min) of QTcF in the analysis. However, the relationship between HR instability and QTcF variability was also valid for individual subjects and individual studies. The intra-subject SD of QTc was significantly correlated with the intra-subject mean HR instability (r = 0.209 and r = 0.274, linear slope of 0.200 and 0.230 ms/bpm in women and men, respectively, both p < 0.0001, Fig. 2d, e). Similarly, the mean HR instability in a study was correlated with the mean intra-subject SD of QTcF (r = 0.353 and r = 0.443, linear slope of 0.192 and 0.192 ms/bpm in women and men, respectively, both p < 0.01, Fig. 2c, f).

Panels a (women) and b (men) show the relationship between heart rate instability and QTcF range in individual time points (pooled data of all part I studies). Panels d (women) and e (men) show the relationships between subject’s mean heart rate instability and intra-subject SD of QTcF (pool of all part I subjects). Panels c and f show the relationship between mean (panel c) and 75 percentile (panel f) of heart rate instability in a study and the mean (panel c) and 75 percentile (panel f) of intra-subject SD of QTcF in the same part I study (red females, blue males). Panels d and e are shown with linear regressions and their 99.9 % confidence intervals, and panels c and f with linear regressions and their 95 % confidence intervals. bpm Beats per minute, SD standard deviation
3.2 Part II
Using HR measurements over six adjacent 20-s windows within 2 min before QT measurement, the selections aiming at stable preceding HR included 608,331 ECG measurements (range 223–1040 in individual subjects) was preceded, on average, by HR differences of 7.38 ± 6.79 bpm, while the selections aiming at preceding variable HR included 289,240 ECG measurements (98–520 in individual subjects) was preceded, on average, by HR differences of 16.34 ± 8.89 bpm. The terminology of measurements preceded by “stable” and “variable” HR is used to differentiate between these data sets.
3.2.1 Correction of QT Intervals for Averages of Preceding RR Intervals
Figure 3 shows the development of the intra-subject SD of QTcF when correcting the QT interval for averages of preceding RR intervals. Even for QT interval measurements that were preceded by stable HR (Fig. 3a, d), prolonged averaging of preceding RR intervals decreased the intra-subject SD of QTcF. For instance, correcting the QT intervals preceded by stable HR for the preceding RR interval, average of the preceding ten RR intervals, and average of the preceding 120 RR intervals led to intra-subject SD of QTcF in women of 11.19 ± 2.53, 8.36 ± 2.07, and 7.52 ± 2.21 ms, respectively. In men, the corresponding values were 11.10 ± 2.61, 8.05 ± 2.55, and 6.63 ± 1.73 ms. All these differences were highly statistically significant (p < 0.0001). Similar highly significant differences were also obtained for the RR averages over 1, 10, and 120 s preceding QT measurement, as well as for the SD of QTcF based on all QT measurements irrespective of whether preceded by stable or variable HR (Fig. 3c, f). In QT intervals preceded by variable HR (Fig. 3b, e), there were little differences between the correction for the preceding RR interval or the average of the preceding ten intervals (or RR intervals in preceding 10 s), but with RR averages around 120 cardiac cycles or seconds, the intra-subject SD of QTcF reached similar levels to those of data preceded by stable HR.

Dependency of intra-subject SD of QTcF on the number of preceding RR intervals (lighter graphs) and the duration of preceding RR intervals (darker graphs) that are averaged before correcting the QT intervals for them (pool of all part II subjects). Panels a + d, b + e, and c + f show results for QT data preceded by stable heart rates, preceded by variable heart rates, and all data together, respectively. Top panels a + b + c = women; bottom panels d + e + f = men. SD standard deviation
3.2.2 Correction of QT Intervals for Hysteresis-Derived RR Intervals
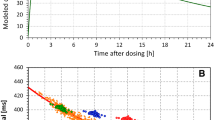
Figure 4 shows the development of intra-subject SD of QTcF dependent on the settings of QT/RR hysteresis models. While the curves are rather flat, minima were reached with the time-based hysteresis model with 95 % hysteresis constant around 120 s. With this model, the values of intra-subject SD of QTcF in women were 7.15 ± 2.07, 6.98 ± 1.52, and 7.14 ± 1.98 ms for data preceded by stable HR, variable HR, and all data combined, respectively. There were no significant differences among these values. The corresponding values in men were 6.27 ± 1.61, 6.50 ± 1.35, and 6.38 ± 1.50 ms. While there were significant differences among these values, they were similarly close to each other as in women (note that, as previously observed [9], the QTc variability was marginally larger in women compared with in men). Importantly, in the total data, the mean intra-subject SD of QTcF obtained with 95 % hysteresis constant between 100 and 140 s fluctuated by only 1.10 % and 1.09 % in women and men, respectively. The exact setting of the 95 % hysteresis constant at 120 s was therefore not crucial.

Dependency of intra-subject SD of QTcF on the QT/RR hysteresis 95 % adaptation constant (see the text for details) as a number of RR intervals (lighter graphs) and as the total time of RR intervals (darker graphs) preceding QT measurement (pool of all part II subjects). Panels a + d, b + e, and c + f show results for QT data preceded by stable heart rates, preceded by variable heart rates, and all data together, respectively. Top panels a + b + c = women; bottom panels d + e + f = men. SD standard deviation
Importantly, in all QT measurements irrespective of whether preceded by stable or variable HR, the lowest SD of QTcF achieved with simple RR averaging (7.67 ± 1.99 ms and 7.03 ± 1.60 ms in women and men, respectively, Fig. 3c, f) was significantly higher than the lowest SD of QTcF achieved with the hysteresis model as shown above (Fig. 4c, f; both p < 0.0001).
3.2.3 Individual QT/RR Profile Characteristics
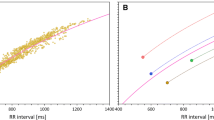
Figure 5 shows the parameter distributions of individually modeled QT/RR patterns of part II subjects. The distributions of optimum 95 % hysteresis time constant (Fig. 5a), QT/RR curvature (Fig. 5b), and the optimum correction parameter of the QT/RRβ correction formula (Fig. 5c) were all statistically significantly different between women and men (hysteresis time constant p < 0.05, QT/RR curvature p < 0.01, parameter β p < 0.001). The median values of the optimum 95 % hysteresis time constant were 109.6 and 113.8 s in women and men, both within the 100- to 140-s region discussed with Fig. 4. The median β parameter values were 0.363 and 0.334 in women and men.

The top line of panels shows the cumulative distributions of subject-specific QT/RR models in part II subjects: QT/RR hysteresis 95 % adaptation constant as the total time of RR intervals (panel a); QT/RR curvatures [9] (panel b); and parameter β of subject-specific QTc = QT/RRβ correction (panel c). The bottom line of panels shows the details of individual optimization of the subject-specific QTc = QT/RRβ correction. In panels d (women) and e (men), each line corresponds to one subject and, for different values of the correction coefficient α, shows the correlation coefficients between QT/RR′α values and the RR′ values (where the RR′ values are derived by individually optimized QT/RR hysteresis models). Panel f shows the cumulative distribution of the correlation coefficients between QTcF values and RR′ values calculated in individual part II subjects. In panels a, b, c, and f, the red and blue lines correspond to the data in women and men, respectively. The green dotted line in panel c and the dashed green lines in panels d and e mark the correction coefficient of the Fridericia formula
While the correction factor of the Fridericia formula was close to the median of the male population (49.4 and 50.6 % of males with optimum β parameter below and above 0.3333), it was different from the median of the female population (23.3 and 76.7 % of women with optimum β parameter below and above 0.3333). The median values of the individually optimized β parameters were 0.3634 and 0.3339 in women and men, respectively. However, in both women and men, the Fridericia formula was only infrequently close to the individual QT/RR pattern (Fig. 5d, e). The correlation coefficient between QTcF values and the underlying RR′ intervals (derived by individual-specific hysteresis models) was between −0.2 and +0.2 in only 31.0 % of women and 32.9 % of men. For the correlation coefficients between −0.1 and +0.1, the corresponding numbers were 14.6 and 14.7 % (Fig. 5f). Not surprisingly, the distribution of the correlation coefficients between QTcF values and the underlying RR′ intervals (Fig. 5f) was also statistically different between women and men (p < 0.0001).
3.2.4 Differences Between Individual-Specific and Global Corrections
Figure 6 shows the differences between RR′ values obtained from individually optimized hysteresis models and the RR′ values obtained with the global hysteresis model using a fixed 95 % time constant of 120 s (Fig. 6a, b). The figure also shows the differences between the individually optimized QTcI values and QTcF values obtained using the RR′ values obtained from individually optimized hysteresis models (Fig. 6d, e) and the differences between QTcF values obtained using the RR′ values obtained from individually optimized hysteresis models and from the global hysteresis model using a fixed 95 % time constant of 120 s (Fig. 6g, h). Importantly and somewhat surprisingly, the RR′ values obtained with the individual optimized and global hysteresis models differed rather little, particularly in comparison to the differences between QTcI values and QTcF values correcting for RR′ by individual hysteresis models (compare the distributions in Fig. 6b, e). The mean difference between the RR′ values obtained with the individual optimized and global hysteresis models was between −4 and +4 ms in all part II subjects (Fig. 6a, b), but the mean difference between QTcI values and QTcF value correction for RR′ by individual hysteresis models exceeded ±5 ms in 30.1 % of women and 14.2 % of men (Fig. 6d, e). Similar comparisons were observed when studying the difference in individual ECG readings rather than averaged for each subject (Fig. 6b, e).

Panels a + b, d + e, and g + h show the differences between RR′ intervals derived from individually optimized and global hysteresis models (panels a + b), differences between QTcI values and QTcF values correcting QT interval for RR′ derived from individually optimized hysteresis models (panels d + e), and the differences between QTcF values correcting QT interval for RR′ derived from individually optimized hysteresis models and RR′ derived from the global hysteresis model with a fixed 95 % time constant of 120 s (panels g + h). Panels a, d, and g show scatter diagrams between the initial values and the differences; panels d, e, and h show the cumulative distributions of the differences in individual phase II ECG samples (dotted lines) and their means in individual phase II subjects (full lines). Note that the vertical axes in panels a, d, and g and the horizontal axes in panels d, e, and h use very different scales. Panels c (women) and f (men) show the differences between intra-subject SDs of QTcF (correcting from RR′ intervals derived from the global hysteresis model) and intra-subject SD of QTcI in the dependency on intra-subject SD of QTcI (bold and dashed horizontal lines show population means ± SD). Panel i shows the cumulative distribution of the differences shown in panels c and f. In panels a, c, d, f, and g, the red circle and blue square marks correspond to data of individual part II women and men, respectively. In panels b, e, h, and i, the red and blue lines correspond to data in women and men, respectively. SD standard deviation
The differences between QTcF values correcting the QT intervals for RR′ by individual hysteresis models and RR′ by global hysteresis model were tiny (Fig. 6g, h). Their averages per subject were all between −0.8 and +0.8 ms, and the individual values exceeded ±5 ms only in 0.41 and 0.36 % of individual ECG readings in women and men, respectively.
Figure 6 also shows the differences between the intra-subject SD of the QTcI and QTcF values correcting the QT intervals for RR′ by the global hysteresis model with a fixed 95 % time constant of 120 s (Fig. 6c, f, i). By design of the individual correction models, the intra-subject SD of QTcI was always smaller than that of QTcF. In women and men, the intra-subject SD of QTcI was 5.71 ± 1.10 and 5.36 ± 1.10 ms, respectively, and the reduction of intra-subject SD from QTcF to QTcI was 1.41 ± 1.30 and 1.02 ± 0.91 ms, respectively (Fig. 6c, f; all p < 0.0001). The difference was more than 1 ms in 46.6 and 32.7 % of women and men, respectively (Fig. 6i). The distribution of the differences between intra-subject SD of QTcF and QTcI was significantly different between the sexes (p < 0.001).
4 Discussion
The study provides three important observations. Firstly, positioning subjects of clinical studies in supine position does not stabilize their HR even during short analysis windows. (Note that by short analysis windows, we mean the durations shown in panels d and e of Fig. 1. The individual measurements are taken from standard 10-s ECG samples and should thus not be influenced by respiratory arrhythmia.) Secondly, a global hysteresis model with a 95 % constant of 120 s provides RR′ values for QT interval HR correction that are little different from RR′ values based on individually optimized hysteresis corrections. Only miniscule differences exist between QTcF values using RR′ values based on the global correction model and on the individually optimized models. Finally, the global hysteresis model reduces the difference in the QTc variability for the QT measurements preceded not only by variable but also by stable HR.
The first observation contradicts the assumptions usually made in the design of clinical QT studies. Nevertheless, although the extent of within-analysis-window HR changes in some studies might be unforeseen, this observation is easily understood. While strict supine position should eliminate physical influences on HR, psychological and psychosocial sources of HR changes remain. Different interpretations of the protocol-specified supine positions by individual clinical units are also possible.
The second observation is entirely unexpected. Previous studies showed that QT/RR hysteresis profiles (i.e., how quickly QT interval changes after HR changes), similar to QT/RR adaptation (i.e., how much QT interval changes after HR changes), show intra-subject stability and inter-subject differences [6, 10, 11]. The inter-subject differences are confirmed in Fig. 5a. Nevertheless, it now seems that the practical implications of these differences are negligible. The results shown in Fig. 6b, h should be noted. While it has been shown that inter-subject differences in QT/RR adaptation have practical implications [4, 11, 12], the inter-subject differences in QT/RR hysteresis can likely be safely ignored. This also fits with the results shown in Fig. 4c, f, suggesting that the 95 % hysteresis constant of 120 s is not performing too differently from its neighborhood. Figure 6 (compare panels e and h) also shows that the differences in QTcI based on individually optimized hysteresis and QTcF involving global hysteresis are almost exclusively caused by the Fridericia formula, i.e., by the individuality in QT/RR adaptation, rather than by the individuality in QT/RR hysteresis. For the standard QT studies, the global QT/RR hysteresis model is therefore universally applicable.
The third observation is equally surprising. It has previously been speculated that different stages of cardiac autonomic status (responsible, among other things, for HR variability) affect the QT/RR relationship [13]. Our observations suggest that if this notion is correct, the autonomic effects beyond the HR adaptation are not large. Intra-subject SD of QTcF in the region of 6–7 ms (Fig. 4) seen with both QT readings preceded by stable and variable HR does not leave too much room for HR-independent autonomic effects. Nevertheless, we can only comment on short-term oscillations of autonomic status that are always present in long-term recordings. Since part II data were obtained from drug-free baseline days of the studies, the investigated populations were not subjected to prolonged and sustained autonomic changes.
As far as the practically negligible difference between the individually optimized and global hysteresis correction is concerned, there is limited material in published literature with which we can compare our results. Nevertheless, the 95 % hysteresis constant of 120 s corresponds to the seminal monophasic action-potential study and to clinical observations [14, 15]. The difference between the substantial practical implications of individual patterns of QT/RR adaptation and the negligible implications of individual QT/RR hysteresis profiles is also in agreement with the previous observations that how much the QT interval alters and how quickly QT interval alters after HR changes are different and probably distinct physiological processes [6].
The substantial differences in the QT/RR adaptations between different part II subjects and the sex difference in the individually optimized QT/RRβ coefficients (see Fig. 5c–f) correspond well to similar previous observations [11, 12]. In particular, Fig. 5d, f show that the distribution of individually optimized QT/RRβ coefficients shown in Fig. 5c should not be interpreted as a suggestion (e.g., QT/RR0.3634) of a replacement of the Fridericia formula in women. Increased precision of HR correction of QT intervals is needed only when compared QT intervals are measured at different HR (e.g., when an investigated drug leads to tachycardia or bradycardia on active treatment). In such cases, individual corrections are needed [4] since any fixed formula (including those close to the median QT/RR adaptation) would over-correct and under-correct in a substantial number of subjects. This is clearly shown in Fig. 5d–f. (Although the figures deal only with the mathematical form of QTc = QT/RRα, the same is true for a fixed universal formula of any mathematical form [4, 11, 12].)
4.1 Limitations
Before considering the practical implications of our observation, the limitations of the presented analyses need to be considered. While the power of QT/QTc studies depends more closely on SD of QTc changes on placebo [16], we investigated intra-subject SD of QTcF for which we had data and which is in direct relationship to changes on placebo. In part I, we relied on protocol specifications of the individual studies and had no control of how tightly the protocols were followed. Study differences in Fig. 1f, g, i might have been contributed to by different protocol interpretations. Nevertheless, even if the within-time-point HR variability was contributed to by relaxed protocol interpretations, the observations of Fig. 2 still hold. We have also relied on reported QT/QTcF readings and have not included any checks of measurement accuracy [17]. In part II, we used only the exponential decay model of QT/RR hysteresis, which might not be fully optimal [7]. However, the small SD of QTcF achieved with this model suggests that other hysteresis models [15, 18, 19] have a limited possibility of improving the results. In the sequences of RR intervals preceding QT interval readings, we have not distinguished between ectopic and sinus rhythm beats. Since the data came from studies in healthy volunteers, this omission was unlikely to have a noticeable impact. Finally, studying healthy subjects does not allow comment on whether the same “universal” hysteresis model applies to cardiac patients [20] and/or patients treated with repolarization active drugs. Nevertheless, it is to be expected that using the corrections for hysteresis derived from healthy subjects will improve the QTc data also in cardiac patients, that is, improve the QTc data compared with not using any correction for hysteresis, as is frequently the case at present. Universal HR corrections [5] that have also been derived from healthy population data are also used very frequently in populations of cardiac patients with little consideration of their appropriateness.
4.2 Conclusions and Recommendations
In spite of these limitations, the results suggest the following recommendations:
Since continuous 12-lead Holter ECGs are becoming widespread in QT/QTc studies, obtaining sequences of individual RR intervals is easily possible in recordings of reasonable quality.
In QT/QTc studies, correcting the measured QT intervals to the hysteresis-modeled RR′ interval derived from the history of RR intervals leads to substantial reduction of the QTc variability. This increases the statistical power of such studies and should allow them to be made smaller, consistent with the present trends. Correcting the QT interval for a simultaneously measured singular RR interval or an average of a small number of RR intervals should be avoided.
Supine positions do not stabilize HRs in healthy subjects. However, once the history of RR intervals and hysteresis modeling are used, there is little difference between QT readings made during stable and variable HR episodes. QT/QTc study analysis windows may be analyzed even if they include variable HR episodes without increasing the variability of QTc data.
The exponential decay hysteresis model with 95 % adaptation in 120 s can be proposed for universally applicable correction of QT/RR hysteresis in healthy subjects (see Sect. 5 for details). It leads to more compact QTc data compared with the simple averages of preceding RR intervals. (Once the sequence of RR intervals preceding QT interval reading is known, it is not more complicated to calculate their weighted average than the simple average.) Only when the QT/QTc study leads to systematic (e.g., drug-induced) HR changes and when individual profiles of QT/RR adaptation and QT/RR curvatures need to be obtained for individual study subjects [4] does it makes sense to also model the individual-specific QT/RR hysteresis profiles, since individual QT/RR curvature modeling also provides data for individual hysteresis modeling (see the further reduction of SD of QTc in Fig. 6c, f, i).
Preservation of the time course for hysteresis across studies and across individuals suggests that demonstrating the effects of QT hysteresis correction might also support the proof of quality of study data in cases when positive control, as mandated for TQTS, is not available. In other words, showing that even in the presence of HR instabilities (which could be expected, as shown in our part I analyses), correction for QT/RR hysteresis verifiably reduces the variability of QTc data might serve as one of the proofs that the measured QT and RR data are adequately accurate.
5 Technical Note
If QT interval reading is preceded by RR interval sequence \( \left\{ {RR_{i} } \right\}_{i = 0}^{N} \) (\( RR_{0} \) closest to the QT measurement), where \( N \cong 300,\;L = \mathop \sum \nolimits_{i = 0}^{N} RR_{i} \cong 300\;{\text{s}} \), the exponential hysteresis model suggests correcting the QT interval for \( RR^{'} = \mathop \sum \nolimits_{i = 0}^{N} \omega_{i} RR_{i} \), where for each \( j = 0, \ldots ,N \), \( \mathop \sum \nolimits_{i = 0}^{j} \omega_{i} = \frac{{1 - {\text{e}}^{{ - \frac{\partial (j + 1)}{N + 1}}} }}{{1 - {\text{e}}^{ - \partial } }} \) and \( \mathop \sum \nolimits_{i = 0}^{j} \omega_{i} = \frac{{1 - {\text{e}}^{{\frac{{ - \partial \mathop \sum \nolimits_{i = 0}^{j} RR_{i} }}{L}}} }}{{1 - {\text{e}}^{ - \partial } }} \) for hysteresis driven by the number of cardiac cycles and by the time from QT measurement, respectively, and where the coefficient \( \partial \) characterizes the time constant. The time-driven hysteresis with 95 % adaptation in 120 s corresponds to \( \partial \) = 7.4622.
References
E14 Clinical evaluation of QT/QTc interval prolongation and proarrhythmic potential for non-antiarrhythmic drugs. Guidance to industry. Fed Regist. 2005;70:61134–5.
Darpo B, Garnett C, Benson CT, Keirns J, Leishman D, Malik M, Mehrotra N, Prasad K, Riley S, Rodriguez I, Sager P, Sarapa N, Wallis R. Cardiac Safety Research Consortium: Can the thorough QT/QTc study be replaced by early QT assessment in routine clinical pharmacology studies? Scientific update and a research proposal for a path forward. Am Heart J. 2014;168:262–72.
Kligfield P, Green CL, Mortara J, Sager P, Stockbridge N, Li M, Zhang J, George S, Rodriguez I, Bloomfield D, Krucoff MW. The Cardiac Safety Research Consortium electrocardiogram warehouse: thorough QT database specifications and principles of use for algorithm development and testing. Am Heart J. 2010;160:1023–8.
Garnett CE, Zhu H, Malik M, Fossa AA, Zhang J, Badilini F, Li J, Darpö B, Sager P, Rodriguez I. Methodologies to characterize the QT/corrected QT interval in the presence of drug-induced heart rate changes or other autonomic effects. Am Heart J. 2012;163:912–30.
Fridericia LS. Duration of systole in electrocardiogram. Acta Med Scandinav. 1920;53:469–86.
Malik M, Hnatkova K, Novotny T, Schmidt G. Subject-specific profiles of QT/RR hysteresis. Am J Physiol Heart CircPhysiol. 2008;295:H2356–63.
Malik M. QT/RR hysteresis. J Electrocardiol. 2014;47:236–9.
Malik M, van Gelderen EM, Lee JH, Kowalski DL, Yen M, Goldwater R, Mujais SK, Schaddelee MP, de Koning P, Kaibara A, Moy SS, Keirns JJ. Proarrhythmic safety of repeat doses of mirabegron in healthy subjects: a randomized, double-blind, placebo-, and active-controlled thorough QT study. Clin Pharm Therap. 2012;92:696–706.
Malik M, Hnatkova K, Kowalski D, Keirns JJ, van Gelderen EM. QT/RR curvatures in healthy subjects: sex differences and covariates. Am J Physiol Heart CircPhysiol. 2013;305:H1798–806.
Jacquemet V, Dubé B, Knight R, Nadeau R, LeBlanc AR, Sturmer M, Becker G, Vinet A, Kuś T. Evaluation of a subject-specific transfer-function-based nonlinear QT interval rate-correction method. PhysiolMeas. 2011;32:619–35.
Batchvarov VN, Ghuran A, Smetana P, Hnatkova K, Harries M, Dilaveris P, Camm AJ, Malik M. QT-RR relationship in healthy subjects exhibits substantial intersubject variability and high intrasubject stability. Am J Physiol Heart CircPhysiol. 2002;282:H2356–63.
Malik M, Färbom P, Batchvarov V, Hnatkova K, Camm AJ. Relation between QT and RR intervals is highly individual among healthy subjects: implications for heart rate correction of the QT interval. Heart. 2002;87:220–8.
Extramiana F, Maison-Blanche P, Badilini F, Pinoteau J, Deseo T, Coumel P. Circadian modulation of QT rate dependence in healthy volunteers: gender and age differences. J Electrocardiol. 1999;32:33–43.
Franz MR, Swerdlow CD, Liem LB, Schaefer J. Cycle length dependence of human action potential duration in vivo. Effects of single extrastimuli, sudden sustained rate acceleration and deceleration, and different steady-state frequencies. J Clin Invest. 1988;82:972–9.
Jacquemet V. Cassani González R, Sturmer M, Dubé B, Sharestan J, Vinet A, Mahiddine O, Leblanc AR, Becker G, Kus T, Nadeau R. QT interval measurement and correction in patients with atrial flutter: a pilot study. J Electrocardiol. 2014;47:228–35.
Zhang J, Machado SG. Statistical issues including design and sample size calculation in thorough QT/QTc studies. J Biopharm Stat. 2008;18:451–67.
Johannesen L, Garnett C, Malik M. Electrocardiographic data quality in thorough QT/QTc studies. Drug Safety. 2014;37:191–7.
Halamek J, Jurak P, Bunch TJ, Lipoldova J, Novak M, Vondra V, Leinveber P, Plachy M, Kara T, Villa M, Frana P, Soucek M, Somers VK, Asirvatham SJ. Use of a novel transfer function to reduce repolarization interval hysteresis. J Interv Card Electrophysiol. 2010;29:23–32.
Hadley DM, Froelicher VF, Wang PJ. A novel method for patient-specific QTc-modeling QT-RR hysteresis. Ann Noninvasive Electrocardiol. 2011;16:3–12.
Pueyo E, Smetana P, Caminal P, de Luna AB, Malik M, Laguna P. Characterization of QT interval adaptation to RR interval changes and its use as a risk-stratifier of arrhythmic mortality in amiodarone-treated survivors of acute myocardial infarction. IEEE Trans Biomed Eng. 2004;51:1511–20.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical standards
All the studies from which data were analyzed were conducted according to approved protocols, all were approved by relevant ethics bodies, and all reported that all participants gave informed written consent.
Funding
The data analysis reported here was supported in part by British Heart Foundation grants PG/12/77/29857 and PG/13/54/30358.
Conflicts of interest
Marek Malik, Lars Johannesen, Katerina Hnatkova and Norman Stockbridge have no conflicts of interest that are directly relevant to the content of this study.
Additional information
This article reflects the views of the authors and should not be construed to represent FDA’s views or policies.
Rights and permissions
About this article

Cite this article
Malik, M., Johannesen, L., Hnatkova, K. et al. Universal Correction for QT/RR Hysteresis. Drug Saf 39, 577–588 (2016). https://doi.org/10.1007/s40264-016-0406-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40264-016-0406-0