
Abstract
Background
Particular interest has been generated regarding the possible influence of statin use on sleep quality. However, no conclusive evidence exists that a particular statin is more likely to be associated with sleep disturbances versus others. It remains uncertain whether different statins produce different risks for sleep disturbance.
Objective
To examine the association between statin use and the risk of sleep disturbances, we conducted data mining using the US Food and Drug Administration Adverse Event Reporting System (FAERS) and a large organized database of prescriptions constructed by a database vendor (Japan Medical Information Research Institute, Inc. Japan).
Methods
Relevant reports in the FAERS were identified and analyzed. Data from the first quarter of 2004 through the end of 2013 were included in this study. The reporting odds ratio (ROR) was used to detect spontaneous report signals, calculated using the case/non-case method. For the ROR, a signal was detected if the lower limit of 95 % two-sided confidence interval (95 % CI) was >1. Additionally, signal detection using the IC was conducted using the IC025 metric, a lower limit of the 95 % CI of the IC, where a signal is detected if the IC025 value exceeds 0. In addition, symmetry analysis was used to identify the risk of insomnia after using statins over the period of January 2006 to August 2013.
Results
In the analyses of the FAERS database, significant signals for sleep disturbances including disturbances in initiating and maintaining sleep, sleep disorders NEC, sleeping disorders due to a general medical condition, and parasomnias were found. In the prescription sequence symmetry analysis, a significant association between statin use and hypnotic drug use was found, with adjusted sequence ratios of 1.14 (1.03–1.26), 1.20 (1.11–1.29), and 1.18 (1.11–1.25) at intervals of 91, 182, and 365 days, respectively.
Conclusion
Multi-methodological approaches using different algorithms and databases strongly suggest that statin use is associated with an increased risk for sleep disturbances including insomnia.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Significant signals for sleep disturbances associated with statin use were found in the analysis of the US Food and Drug Administration Adverse Event Reporting System database. |
Significant associations between statin use and hypnotic drug use were found in the prescription sequence symmetry analysis. |
Multi-methodological approaches using different algorithms and databases strongly suggested that statin use is associated with an increased risk for sleep disturbances including insomnia. |
1 Background
HMG-CoA reductase inhibitors (statins) are effective and widely used drugs in patients with hypercholesterolemia, and the efficacy and safety of statins have been studied in a number of large trials of long duration [1, 2]. From a safety perspective, both clinical trials and post-marketing surveillance have demonstrated that statins are generally well tolerated, with rare but severe adverse effects that mainly affect the muscle, liver, and kidney [1]. These trials have shown that medically significant adverse effects are uncommon. Although the safety profile of statins is well documented and the majority of people treated with statins enjoy good outcomes, no drug is without the potential for adverse effects. The most recognized and commonly reported adverse statin-related events pertains to muscle complications, including pain, fatigue, and weakness, in addition to rhabdomyolysis [3–6].
In recent years, interest has been focused on the potential risk of adverse psychiatric reactions to statins, including memory loss, depression, suicidality, aggression, and antisocial behavior [7–10]. Particular interest has been also raised about the possible influence of statin treatment on sleep quality. However, several studies focused on possible statin-induced insomnia and sleep alterations have generated conflicting or non-conclusive results.
A Europe-wide review conducted by the Medicine and Healthcare Products Regulatory Agency (MHRA) assessed the evidence available on the following adverse drug reactions (ADRs) associated with the use of statins (atorvastatin, fluvastatin, lovastatin, pravastatin, rosuvastatin, and simvastatin): sleep disturbances, memory loss, micturition disorders (problems with urination), sexual disturbances, depression, and interstitial pneumopathy [11]. The evidence assessed included data from clinical trials, post-marketing reported cases of ADRs, and the published literature. This report concluded that it seemed practical to include core safety information for sleep disturbances in the Summary of Product Characteristics (SPC) for all statins. However, it remains uncertain whether different statins produce different risks for sleep disturbance. A further clarification of the data related to statin-induced sleep disturbances should be presented to improve safe use in clinical practice.
Recently, data mining with different methodologies and algorithms has been applied to identify safety signals within medical databases, including spontaneous ADR databases, claims databases, and prescription databases. We examined the association of statin use and sleep disturbances using the US Food and Drug Administration (FDA) Adverse Event Reporting System (FAERS), which is a large and useful spontaneous database of adverse event reports. In addition, a large and well organized database of prescriptions constructed by a database vendor (Japan Medical Information Research Institute, Inc. Japan [JMIRI]) was also analyzed. The aim of our study was to examine the hypothesis that sleep disturbances are associated with the use of statins by employing different methodologies, algorithms, and databases.
2 Methods
2.1 FAERS Data Mining
2.1.1 Data Sources
The FAERS is a computerized information database designed to support the FDA’s post-marketing safety surveillance program for all approved drugs and therapeutic biological products. The system contains all reports of adverse events reported spontaneously by healthcare professionals, manufacturers, and consumers worldwide. The FAERS consists of seven data sets that include patient demographic and administrative information (file descriptor DEMO), drug and biologic information (DRUG), adverse events (REAC), patient outcomes (OUTC), report sources (RPSR), start of drug therapy and end dates (THER), and indications for use/diagnosis (INDI). A unique number for identifying a FAERS report allows all the information from different files to be linked. Raw data from the FAERS database can be downloaded freely from the FDA website (http://www.fda.gov/Drugs/InformationOnDrugs/ucm135151.htm). Data from the first quarter of 2004 through the end of 2013 were included in this study. A total of 4,052,885 reports were obtained. Reports with a common CASE number were identified as duplicated reports. We deleted duplicates and excluded from the analyses. Finally, a total of 54,841,322 drug-reaction pairs were identified in 3,308,116 reports. The Medical Dictionary for Regulatory Activities (MedDRA® version 17.0) preferred terms (PTs) was used to classify the adverse events. The structure of the FAERS database is described elsewhere [12].
The FAERS data have some limitations. First, there is no certainty that the reported event (adverse event or medication error) was actually due to the drug. Second, the FDA does not receive reports on every adverse event or medication error that occurs with a product [13, 14]. Therefore, the FAERS data cannot be used to calculate the incidence of an adverse event or medication error in the population. However, FAERS data could be used for signal detection [15, 16].
2.1.2 Identifying Statins
FAERS permits the registration of arbitrary drug names including trade names, generic names, and abbreviations. All drug names were extracted from the DRUG file of FAERS and recorded. A drug name archive that included the names of all preparations, generic names, and synonyms of drugs marketed in the world was created using the Martindale website (https://www.medicinescomplete.com/mc/login.htm). Simvastatin, rosuvastatin, pravastatin, atorvastatin, fluvastatin, lovastatin, and pitavastatin were identified by linking this archive with the FAERS database. All records including statins in the DRUG files were selected and the relevant reactions from the REACTION files were then identified.
2.1.3 Definition of Adverse Events
Adverse events in the FAERS database are coded using the PTs in the MedDRA® terminology.Footnote 1 The MedDRA® includes groupings of PTs that relate to defined medical conditions or areas of interest. Sleep disorders and disturbances related to the high level terms and PTs used in the study were listed in Table 1.
2.1.4 Data Mining
The reporting odds ratio (ROR) [17], and the information component (IC) [18] were used to detect spontaneous report signals. These signal scores were calculated using a case/non-case method [19, 20]. Cases are the reports with the event of interest (i.e., sleep disturbance), and the non-cases are all the other reports. ROR and IC are widely used and employed by the Netherlands Pharmacovigilance Centre and the World Health Organization (WHO), respectively [17, 18].
All of these algorithms were used to calculate signal scores to assess whether a drug was significantly associated with an adverse event or not from a two-by-two frequency table of counts. However, these calculations or algorithms, so-called disproportionality analyses or measures, differ from one another in that the ROR is frequentist (non-Bayesian), whereas the IC is Bayesian. For the ROR, a signal is detected if the lower limit of 95 % two-sided confidence interval (95 % CI) is >1 [17]. Signal detection using the IC is conducted using the IC025 metric, a lower limit of the 95 % CI of the IC, and a signal is detected if the IC025 value exceeds 0 [18]. In the current study, two methods were used to detect signals, and the adverse events were listed as drug associated when two indices met the criteria indicated above. Data management and analyses were performed using Visual Mining Studio software (version 7.3; Mathematical Systems, Inc., Tokyo, Japan).
2.2 Prescription Sequence Symmetry Analysis
2.2.1 Data Source
A large organized database of prescriptions constructed by a database vendor (JMIRI) was used in the study. The JMIRI prescription database consisted of prescriptions collected from approximately 400 pharmacies in Japan. The database included approximately 69,000,000 prescriptions for about 7,230,000 patients from January 2006 to August 2013. For the prescription sequence symmetry analysis, we identified cases extracted from the JMIRI prescription database in which statins or drugs for sleep disturbance were prescribed at least once during the study period. The data included an encrypted personal identifier: month/year of birth and gender of the patient, drug name, unique drug code and generic name, and prescribing date. Data on drugs dispensed in hospitals were not included. This study was approved by the Ethics Committee of Kinki University School of Pharmacy.
2.2.2 Study Design
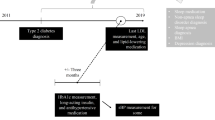
The prescription sequence symmetry analysis (PSSA) was performed to test the hypothesis that statins increase the risk for insomnia. The PSSA method has been described in detail in several published studies, which have investigated the associations between the use of certain target drugs and potential adverse events [21, 22]. Briefly, the PSSA evaluates asymmetry in the distribution of an incident event (e.g., prescription of another drug) before and after the initiation of a specific treatment. Asymmetry may indicate an association of the specific treatment of interest with the event. The PSSA is based on a situation when drug A is suspected of causing an adverse event that itself is treated by drug B [21]. In this study, hypnotic drugs were used as markers of insomnia caused by statins, and the association between statin use and the use of hypnotic drugs was analyzed.
The ratio of the number of patients with a prescription for hypnotic drugs after the initiation of statins versus the number of patients with the event before the initiation of statins was defined as the crude sequence ratio (SR). A SR >1 indicated an increased risk for statin-induced insomnia. The SR is sensitive to prescribing trends over time. Therefore, the SRs were adjusted for temporal trends in statins and hypnotic drugs using the method proposed by Halls [21]. The probability for statins to be prescribed first, in the absence of any causal relationship, can be estimated by the so-called null-effect SR [21]. The null-effect SR produced by the proposed model may be interpreted as a reference value for the SR. Therefore, the null-effect SR is the expected SR in the absence of any causal association, after taking the incidence trends into account. By dividing the crude SR by the null-effect SR, an adjusted SR (ASR) can be obtained that is corrected for temporal trends. A slightly modified model was used to account for the limited time interval allowed between statins and treatment for insomnia [22]. The major advantage of the SR is that it is robust for confounders that are stable over time. Significant confounding factors, including age, gender, and frequency of visits did not cause an asymmetrical distribution of the statins and hypnotic drugs [22].
2.2.3 Data Analysis
The PSSA was undertaken to identify the new use of hypnotic drugs listed in Table 2 as a surrogate for statin-induced insomnia. All incident users of statins and hypnotic drugs were identified during the period from January 2006 to August 2013. For this study, patients included in the database were followed up to August 2013 and therefore different patients had different follow-up periods. Incidence was defined as the first prescription for target drugs. To exclude prevalent users of target drugs, the analysis was restricted to users who presented their first prescription on July 2006 or later, that is, after a run-in period of 6 months. To ensure that our analysis was restricted to incident users, we also did a waiting time distribution analysis [23]. An identical run-in period was also applicable to patients enrolled into the cohort after July 2006 to exclude the prevalent use of target drugs. The analysis was based on the principle that by observing the first occurrence of a prescription within a specific time window, prevalent users of the drug will cluster at the beginning of the observation period when the prescription is repeated within a short time period. In contrast, incident users will be distributed evenly throughout the observation period. Incident users were identified by excluding those patients who had received their first prescription for the target drugs prior to June 2006. All patients were identified who initiated a new treatment with statins and hypnotic drugs within 91-, 182-, and 365-day periods. Patients who had received their first prescriptions for statins and hypnotic drugs on the same date were not included in the determination of SR.
Results are expressed as the means ± standard deviation (SD) for quantitative data and as frequencies (percentage) for categorical data. Ninety-five percent CI for the ASRs were calculated using a method for exact CIs for binomial distributions [24].
3 Results
3.1 FAERS Database Analyses
A total of 8,270 PTs were found in reports for simvastatin, 5,923 for rosuvastatin, 5,815 for pravastatin, 9,014 for atorvastatin, 1,258 for pitavastatin, 3,417 for fluvastatin, and 4,196 for lovastatin. The total number of drug-reaction pairs for statins was 1,433,826 including 487,237 for simvastatin, 177,763 for rosuvastatin, 122,768 for pravastatin, 556,579 for atorvastatin, 5,424 for pitavastatin, 28,010 for fluvastatin, and 56,045 for lovastatin. The number of drug-reaction pairs was 269,084 for disturbances in initiating and maintaining sleep, 51,463 for sleep disorders NEC, 263,872 for dyssomnias, 2,210 for sleep disorders due to a general medical condition, 98 for sleep disorders related to another mental condition, 2,088 for sleep-phase rhythm disturbances, 76,936 for parasomnias, and 4,088 for narcolepsy and associated conditions.
The statistical data on statin-associated sleep disturbances are presented in Table 3. The signal scores suggested that the statins were associated with sleep disturbances including disturbances in initiating and maintaining sleep, sleep disorders NEC, sleeping disorders due to a general medical condition, and parasomnias. In the analysis of individual statins, simvastatin showed significant signals for disturbances in initiating and maintaining sleep, sleep disorders NEC, dyssomnia and parasomnias, rosuvastatin for disturbances in initiating and maintaining sleep, sleep disorders NEC, sleep disorders due to general medical condition and parasomnias, pravastatin for sleep disorders NEC, fluvastatin for sleep disorders NEC, and lovastatin for disturbances in initiating and maintaining sleep and parasomnias. Atorvastatin and pitavastatin did not show a significant signal for sleep disturbances.
3.2 Prescription Sequence Symmetry Analysis
The PSSA characteristics of the study population are summarized in Table 4. The numbers of prescriptions including statins during the study period were 6,377,132. Of the 300,141 statin users, 87,718 incident users were identified. The mean age of statin incident users was 64.96 ± 12.37 years.
The associations between statin and hypnotic drug use are shown in Table 5. Of the 87,718 statin incident users, 12,053 were identified as incident users of hypnotic drugs, before or after the initiation of statins. A significant association between statin and hypnotic drug use was found, with ASRs of 1.14 (1.03–1.26), 1.20 (1.11–1.29), and 1.18 (1.11–1.25) at intervals of 91, 182, and 365 days, respectively. Analysis of individual statins showed no significant associations.
4 Discussion
Analyses of the FAERS database and the JMIRI prescription database suggested that statin use was associated with developing sleep disturbances including insomnia. In the present study, significant signals for disturbances in initiating and maintaining sleep were found for the whole class of statins in the analysis of the FAERS database, and a significant association was found between statin use and hypnotic drug use in the analysis of the JMIRI prescription database. Consistent findings from the independent analyses, using different methodologies, algorithms, and databases strongly suggest that statin use is associated with the development of insomnia. The MHRA Public Assessment Report evaluated the association of statin use with sleep disturbances [11]. Although the SPC for pravastatin lists sleep disturbances, the MHRA Public Assessment Report concluded that it was necessary to list sleep disturbance in the SPC for the remaining statins. Given these considerations, it is reasonable to assume that all statins increase the risk for sleep disturbances including insomnia.
The specific rate of psychiatric adverse events associated with different statins is probably related to the ability of each drug to cross the blood-brain barrier [25, 26]. Thus, it is hypothesized that statins with a high degree of lipophilicity might be associated with a higher rate of central nervous system disturbances in comparison with hydrophilic statins [27]. In fact, the majority of available reports have referred to lipophilic statins, namely simvastatin and lovastatin [28–30]. However, no conclusive evidence exists that a particular statin is more likely to be associated with sleep disturbances over others.
With regard to insomnia, there are a number of reports concerning its association with statin use. Schaefer reported that a higher prevalence of sleep complaints was observed in patients receiving lovastatin than in patients receiving pravastatin, which is a predominant hydrophilic statin [31]. Vgontzas et al. [32] found that prolonged administration of lovastatin, but not pravastatin, increased the wake time after sleep onset in controlled studies comparing the effects of lovastatin and pravastatin on sleep. In addition, decreased sleep time was observed after administration of simvastatin to patients who had not previously complained of sleep problems [33], and our present analysis of the FAERS database also showed that simvastatin showed an increased ROR for disturbances in initiating and maintaining sleep. These studies and our finding may support the notion that lipophilic statins are more likely to be associated with psychiatric ADRs; however, several conflicting findings have also been reported. Tuccori et al. [25] found a significant association between insomnia and statins as a whole class, but did not find a relationship for individual statins in an analysis of Italian data obtained from spontaneous reporting. Ehrenberg et al. reported that lovastatin and pravastatin did not exert significant effects on sleep parameters in hypercholesterolaemic patients [34]. In the present PSSA using the JMIRI prescription database, a significant association of hypnotic drug use was found with the whole class of statins but not with individual statins. In the present study using the FAERS database, significant signals for disturbances in initiating and maintaining sleep were found for the whole class of statins; however, in the analysis of individual statins, significant signals for disturbances in initiating and maintaining sleep were found for simvastatin, rosuvastatin, and lovastatin, but not for the other statins. Additionally, it has been reported that switching to a different statin was able to resolve symptoms in some cases, but in other cases, switching to a different statin was not able to resolve symptoms [35]. These findings may suggest that individual statins are associated with different degrees of risk for psychiatric adverse events and also may not support the hypothesis that hydrophilic statins are safer than lipophilic statins in the production of sleep disturbances including insomnia. However, in the present analysis of some stains, sample sizes are too small to allow the identification of weak signals. Although significant signals of sleep disturbances were not found in some analyses in the present study, this may be mainly attributable to a limited sample size and insufficient power to detect small risks. In addition, many factors may contribute to the development of sleep disturbances including insomnia. In the present study, individual cases were not reviewed and the causes other than statin use were not considered. This is a significant limitation in our study. Consequently, it is reasonable that the whole class of statins produces an increased risk for sleep disturbances including insomnia; however, individual statins may have a different degree of risk for sleep disturbances. To ensure that our findings are reliable, a number of confounding factors associated with the development of sleep disturbances including insomnia should be investigated in future studies.
Although a plausible pharmacological mechanism for sleep disturbance is unknown, several theories have been reported. Reduced serum cholesterol levels might decrease brain cell membrane cholesterol, lower lipid microviscosity, and decrease the expression of serotonin receptors on the membrane surface; this would lead ultimately to a reduction in the control of serotonin on neuronal activity [36]. As central serotonergic pathways are involved in behavioral control, reduced cholesterol levels could facilitate the occurrence of adverse psychiatric events. If this mechanism is correct, the degree of lipophilicity for statins would not primarily affect the development of sleep disturbances. Tuccori et al. also proposed seven mechanisms to explain the neuropsychiatric effects of statins, which are not mutually exclusive and are related mainly to inhibition of HMG-CoA reductase. At the present time, it is unclear whether statins with a high degree of lipophilicity might be associated with a higher rate of insomnia in comparison with hydrophilic statins. Further study is required to define the pharmacological mechanisms underlying sleep disturbances.
The present study detected reliable but weak signals for sleep disturbances including insomnia in statin users. Chronic insufficient sleep or sleep loss, which might be attributed to insufficient sleep duration, insomnia, and irregular sleep-wake schedules, is a common problem in humans in industrial societies. Symptoms of insomnia are a common complaint among community residents and primary care patients. Liu et al. [37] reported that the prevalence rate for insomnia in the general adult population of Japan was 21 %, while 6 % took sleep-enhancing medications. The prevalence of self-reported sleep difficulty is in the range of 10–40 % [38–42]. Problems with sleep are a common event in elderly patients [37, 43], and statin-related insomnia may go unnoticed or missed in clinical practice. Therefore, it may not be easy to find an association between symptoms related to sleep disturbances and drug therapy.
The analysis of spontaneous reports is a useful method for identifying signals, and the FAERS database is considered the largest source of these data. However, there are several potential limitations that should be taken into account when interpreting results obtained from the FAERS database [44]. First, the database has missing data and also frequent misspelling of drug names. Second, there are a number of duplicate entries in the database. To overcome problems with data quality, we manually corrected mistakes in the data entries and deleted duplicates. Third, slightly increased ROR and IC values do not imply an unmistakable risk of sleep disturbance in clinical practice. These data mining algorithms and criteria were assessed from the standpoint of early and timely signal detection when used for pharmacovigilance [45–47]. These quantitative pharmacovigilance methods and criteria may also be helpful in providing further information on the known adverse event, and many studies in this area have been reported [48–52]. However, no individual algorithm to detect signals is adequate and the concurrent use of other algorithm is essential. Therefore, the ROR and IC algorithms were used in the analysis of the FAERS database, and our study detected weak but reliable signals for sleep disturbances. Furthermore, in the current study, a different methodology, the PSSA of the JMIRI prescription database, was used to confirm the findings of FAERS database analyses, and produced consistent findings. Of course, the PSSA is associated with several potential limitations because of its use of a prescription database from pharmacies. First, data for drugs dispensed in hospitals were not included. Second, drugs approved for use against insomnia were used as surrogate markers for insomnia. Therefore, some patients may not in fact have had insomnia. Third, other causes of insomnia were not considered in interpreting the results. Insomnia may be attributed to various causes including depression, stress, and anxiety associated with cardiovascular and cerebrovascular events and treatment. Additionally, it is known that statin-treated patients have an increased risk of depression. In the present study, individual cases were not reviewed, and other causes were not considered. This is a significant limitation in the study. Finally, the relatively short intervals (91, 182, and 365 days) were used to identify the association between statin use and hypnotic drug use. The PSSA has a lower sensitivity when the time between statin initiation and the event is restricted to a short interval [53]. This low sensitivity is possibly because of the small sample sizes and an inadequate time window frame particularly for adverse events that may take longer to manifest [53]. When a long interval is used, potential time-varying covariates would make it difficult to determine the causality of exposure and outcome [54]. Tuccori et al. [35] reported that the median time for overall psychiatric events since the first statin administration was 41 days (range 4–420 days) in 45 cases reported in the period 1992–2012. Taking into account these findings, the relatively short intervals were used.
In the analysis of the FAERS database, significant signals for disturbances in initiating and maintaining sleep, sleep disorders NEC, dyssomnias, and parasomnias were found. The ROR measure found the significant signal for fluvastatin-sleep phase rhythm disturbances combination, but the IC measure did not found this signal. Therefore, we decided that the fluvastatin-sleep phase rhythm disturbances combination was not significant. This may be mainly attributable to limited sample sizes and insufficient power to detect small risks. Statins may produce a wide variety of psychiatric adverse events. Among these sleep disturbances, insomnia was the most frequently occurring adverse event, and therefore close monitoring is required to prevent this adverse event in clinical practice.
5 Conclusions
Multi-methodological approaches using different methodologies, algorithms, and databases strongly suggest that statin use is associated with an increased risk for sleep disturbances including insomnia. Although it is proposed that statins with a high degree of lipophilicity might be associated with a higher rate of central nervous system disturbances in comparison with hydrophilic statins, we could not obtain clear evidence that hydrophilic statins produce a low degree of insomnia risk. Additionally, analysis of the FAERS database detected significant signals for sleep disturbances other than insomnia in statin users. Therefore, people prescribed statins should be considered as having an increased risk of sleep disturbance. Although the biological mechanism for this phenomenon remains unknown, the risk of sleep disturbance associated with statin use is a very important finding in clinical practice. Sleep disturbances associated with statins should be closely monitored in clinical practice, and further studies are needed to confirm our findings and elucidate the mechanism for statin-induced sleep disturbance.
Notes
MedDRA®, the Medical Dictionary for Regulatory Activities terminology, is the international medical terminology developed under the auspices of the International Conference on Harmonization of Technical Requirements for Registration of Pharmaceuticals for Human Use (ICH). The MedDRA® trademark is owned by the International Federation of Pharmaceutical Manufacturers and Associations (IFPMA) on behalf of the ICH.
References
Shepherd J, Cobbe SM, Ford I, Isles CG, Lorimer AR, MacFarlane PW, et al. Prevention of coronary heart disease with pravastatin in men with hypercholesterolemia: West of Scotland Coronary Prevention Study Group. N Engl J Med. 1995;333(20):1301–7.
Taylor F, Huffman MD, Macedo AF, Moore TH, Burke M, Davey Smith G, et al. Statins for the primary prevention of cardiovascular disease. Cochrane Database Syst Rev. 2013;1:CD004816.
Antons KA, Williams CD, Baker SK, Phillips PS. Clinical perspectives of statin-induced rhabdomyolysis. Am J Med. 2006;119(5):400–9.
Ronaldson KJ, O’Shea JM, Boyd IW. Risk factors for rhabdomyolysis with simvastatin and atorvastatin. Drug Saf. 2006;29(11):1061–7.
Ardati A, Stolley P, Knapp DE, Wolfe SM, Lurie P. Statin-associated rhabdomyolysis. Pharmacoepidemiol Drug Saf. 2005;14(4):287.
Eriksson M, Angelin B, Sjoberg S. Risk for fatal statin-induced rhabdomyolysis as a consequence of misinterpretation of ‘evidence-based medicine’. J Intern Med. 2005;257(3):313–4.
Parale GP, Baheti NN, Kulkarni PM, Panchal NV. Effects of atorvastatin on higher functions. Eur J Clin Pharmacol. 2006;62(4):259–65.
Tatley M, Savage R. Psychiatric adverse reactions with statins, fibrates and ezetimibe: implications for the use of lipid-lowering agents. Drug Saf. 2007;30(3):195–201.
Suribhatla S, Dennis MS, Potter JF. A study of statin use in the prevention of cognitive impairment of vascular origin in the UK. J Neurol Sci. 2005;229–230:147–50.
Golomb BA, Kane T, Dimsdale JE. Severe irritability associated with statin cholesterol-lowering drugs. QJM. 2004;97(4):229–35.
MHRA public assessment report. Statins: updates to product safety information. http://www.mhra.gov.uk/home/groups/pl-p/documents/websiteresources/n062559.pdf2009.
Ali AK. Pharmacovigilance analysis of adverse event reports for aliskiren hemifumarate, a first-in-class direct renin inhibitor. Ther Clin Risk Manag. 2011;7:337–44.
Hazell L, Shakir SA. Under-reporting of adverse drug reactions: a systematic review. Drug Saf. 2006;29(5):385–96.
Lopez-Gonzalez E, Herdeiro MT, Figueiras A. Determinants of under-reporting of adverse drug reactions: a systematic review. Drug Saf. 2009;32(1):19–31.
Rodriguez EM, Staffa JA, Graham DJ. The role of databases in drug postmarketing surveillance. Pharmacoepidemiol Drug Saf. 2001;10(5):407–10.
Wysowski DK, Swartz L. Adverse drug event surveillance and drug withdrawals in the United States, 1969–2002: the importance of reporting suspected reactions. Arch Intern Med. 2005;165(12):1363–9.
van Puijenbroek EP, Bate A, Leufkens HG, Lindquist M, Orre R, Egberts AC. A comparison of measures of disproportionality for signal detection in spontaneous reporting systems for adverse drug reactions. Pharmacoepidemiol Drug Saf. 2002;11(1):3–10.
Bate A, Lindquist M, Edwards IR, Olsson S, Orre R, Lansner A, et al. A Bayesian neural network method for adverse drug reaction signal generation. Eur J Clin Pharmacol. 1998;54(4):315–21.
Sakaeda T, Tamon A, Kadoyama K, Okuno Y. Data mining of the public version of the FDA Adverse Event Reporting System. Int J Med Sci. 2013;10(7):796–803.
Almenoff JS, Pattishall EN, Gibbs TG, DuMouchel W, Evans SJ, Yuen N. Novel statistical tools for monitoring the safety of marketed drugs. Clin Pharmacol Ther. 2007;82(2):157–66.
Hallas J. Evidence of depression provoked by cardiovascular medication: a prescription sequence symmetry analysis. Epidemiology. 1996;7(5):478–84.
Tsiropoulos I, Andersen M, Hallas J. Adverse events with use of antiepileptic drugs: a prescription and event symmetry analysis. Pharmacoepidemiol Drug Saf. 2009;18(6):483–91.
Hallas J, Gaist D, Bjerrum L. The waiting time distribution as a graphical approach to epidemiologic measures of drug utilization. Epidemiology. 1997;8(6):666–70.
Morris JA, Gardner MJ. Calculating confidence intervals for relative risks (odds ratios) and standardised ratios and rates. Br Med J (Clin Res Ed). 1988;296(6632):1313–6.
Tuccori M, Lapi F, Testi A, Coli D, Moretti U, Vannacci A, et al. Statin-associated psychiatric adverse events: a case/non-case evaluation of an Italian database of spontaneous adverse drug reaction reporting. Drug Saf. 2008;31(12):1115–23.
Saheki A, Terasaki T, Tamai I, Tsuji A. In vivo and in vitro blood-brain barrier transport of 3-hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) reductase inhibitors. Pharm Res. 1994;11(2):305–11.
Galatti L, Polimeni G, Salvo F, Romani M, Sessa A, Spina E. Short-term memory loss associated with rosuvastatin. Pharmacotherapy. 2006;26(8):1190–2.
King DS, Wilburn AJ, Wofford MR, Harrell TK, Lindley BJ, Jones DW. Cognitive impairment associated with atorvastatin and simvastatin. Pharmacotherapy. 2003;23(12):1663–7.
Padala KP, Padala PR, Potter JF. Simvastatin-induced decline in cognition. Ann Pharmacother. 2006;40(10):1880–3.
Roth T, Richardson GR, Sullivan JP, Lee RM, Merlotti L, Roehrs T. Comparative effects of pravastatin and lovastatin on nighttime sleep and daytime performance. Clin Cardiol. 1992;15(6):426–32.
Schaefer EJ. HMG-CoA reductase inhibitors for hypercholesterolemia. N Engl J Med. 1988;319:1222–3.
Vgontzas AN, Kales A, Bixler EO, Manfredi RL, Tyson KL. Effects of lovastatin and pravastatin on sleep efficiency and sleep stages. Clin Pharmacol Ther. 1991;50(6):730–7.
Barth JD, Kruisbrink OA, Van Dijk AL. Inhibitors of hydroxymethylglutaryl coenzyme A reductase for treating hypercholesterolaemia. BMJ. 1990;301(6753):669.
Ehrenberg BL, Lamon-Fava S, Corbett KE, McNamara JR, Dallal GE, Schaefer EJ. Comparison of the effects of pravastatin and lovastatin on sleep disturbance in hypercholesterolemic subjects. Sleep. 1999;22(1):117–21.
Tuccori M, Montagnani S, Mantarro S, Capogrosso-Sansone A, Ruggiero E, Saporiti A, et al. Neuropsychiatric adverse events associated with statins: epidemiology, pathophysiology, prevention and management. CNS Drugs. 2014;28(3):249–72.
Engelberg H. Low serum cholesterol and suicide. Lancet. 1992;339(8795):727–9.
Liu X, Uchiyama M, Kim K, Okawa M, Shibui K, Kudo Y, et al. Sleep loss and daytime sleepiness in the general adult population of Japan. Psychiatry Res. 2000;93(1):1–11.
Mellinger GD, Balter MB, Uhlenhuth EH. Insomnia and its treatment: prevalence and correlates. Arch Gen Psychiatry. 1985;42(3):225–32.
Kuppermann M, Lubeck DP, Mazonson PD, Patrick DL, Stewart AL, Buesching DP, et al. Sleep problems and their correlates in a working population. J Gen Intern Med. 1995;10(1):25–32.
Simon GE, VonKorff M. Prevalence, burden, and treatment of insomnia in primary care. Am J Psychiatry. 1997;154(10):1417–23.
Ancoli-Israel S, Roth T. Characteristics of insomnia in the United States: results of the 1991 National Sleep Foundation Survey. I. Sleep. 1999;22(Suppl. 2):S347–53.
Ford DE, Kamerow DB. Epidemiologic study of sleep disturbances and psychiatric disorders: an opportunity for prevention? JAMA. 1989;262(11):1479–84.
Klink ME, Quan SF, Kaltenborn WT, Lebowitz MD. Risk factors associated with complaints of insomnia in a general adult population: influence of previous complaints of insomnia. Arch Intern Med. 1992;152(8):1634–7.
Bate A, Evans SJ. Quantitative signal detection using spontaneous ADR reporting. Pharmacoepidemiol Drug Saf. 2009;18(6):427–36.
Motola D, Piccinni C, Biagi C, Raschi E, Marra A, Marchesini G, et al. Cardiovascular, ocular and bone adverse reactions associated with thiazolidinediones: a disproportionality analysis of the US FDA adverse event reporting system database. Drug Saf. 2012;35(4):315–23.
Sommet A, Grolleau S, Bagheri H, Lapeyre-Mestre M, Montastruc JL. Was the thrombotic risk of rofecoxib predictable from the French Pharmacovigilance Database before 30 September 2004? Eur J Clin Pharmacol. 2008;64(8):829–34.
Lindquist M, Stahl M, Bate A, Edwards IR, Meyboom RH. A retrospective evaluation of a data mining approach to aid finding new adverse drug reaction signals in the WHO international database. Drug Saf. 2000;23(6):533–42.
Tamura T, Sakaeda T, Kadoyama K, Okuno Y. Aspirin- and clopidogrel-associated bleeding complications: data mining of the public version of the FDA Adverse Event Reporting System, AERS. Int J Med Sci. 2012;9(6):441–6.
Murakami H, Sakaeda T, Kadoyama K, Okuno Y. Gender effects on statin-associated muscular adverse events: an analysis of the FDA AERS database. Pharmacol Pharmacy. 2013;4:340–6.
Moore N, Kreft-Jais C, Haramburu F, Noblet C, Andrejak M, Ollagnier M, et al. Reports of hypoglycaemia associated with the use of ACE inhibitors and other drugs: a case/non-case study in the French pharmacovigilance system database. Br J Clin Pharmacol. 1997;44(5):513–8.
Poluzzi E, Raschi E, Moretti U, De Ponti F. Drug-induced torsades de pointes: data mining of the public version of the FDA Adverse Event Reporting System (AERS). Pharmacoepidemiol Drug Saf. 2009;18(6):512–8.
Poluzzi E, Raschi E, Motola D, Moretti U, De Ponti F. Antimicrobials and the risk of torsades de pointes: the contribution from data mining of the US FDA Adverse Event Reporting System. Drug Saf. 2010;33(4):303–14.
Wahab IA, Pratt NL, Wiese MD, Kalisch LM, Roughead EE. The validity of sequence symmetry analysis (SSA) for adverse drug reaction signal detection. Pharmacoepidemiol Drug Saf. 2013;22(5):496–502.
Lai EC, Yang YH, Lin SJ, Hsieh CY. Use of antiepileptic drugs and risk of hypothyroidism. Pharmacoepidemiol Drug Saf. 2013;22(10):1071–9.
Acknowledgments
We thank the Japan Medical Information Research Institute, Inc. for providing the database of prescriptions.
Conflict of interest statement
No sources of funding were used to assist in the preparation of this study. Mitsutaka Takada, Mai Fujimoto, Kohei Yamazaki, Masashi Takamoto, and Kouichi Hosomi have no conflicts of interest that are directly relevant to the content of this study.
Author information
Authors and Affiliations
Corresponding author
Additional information
This study was conducted in the Division of Clinical Drug Informatics, School of Pharmacy, Kinki University, Higashi-osaka, Osaka, Japan.
Rights and permissions
About this article

Cite this article
Takada, M., Fujimoto, M., Yamazaki, K. et al. Association of Statin Use with Sleep Disturbances: Data Mining of a Spontaneous Reporting Database and a Prescription Database. Drug Saf 37, 421–431 (2014). https://doi.org/10.1007/s40264-014-0163-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40264-014-0163-x