
Abstract
Background
Thorough QT studies are typically conducted for drugs with systemic bioavailability and include a positive control, typically moxifloxacin, with a well-described QTc effect.
Objective
This study tested two hypotheses: that (i) re-measuring the QT intervals based on electrocardiogram (ECG) pattern similarity improves the moxifloxacin time profile, and (ii) that study conduct influences the ability to detect a typical moxifloxacin time profile.
Methods
ECGs from 65 studies with available moxifloxacin plasma concentrations were obtained, including four studies with an unexpected moxifloxacin response. Residual error of a concentration–QT model was evaluated before and after re-measuring the QT interval based on ECG pattern similarity. Intra-replicate heart rate differences were calculated using the original heart rate measurements and the 10-s average heart rates.
Results
Similarity re-measurements reduced the residual error of the model (before vs. after of 8.43 ± 2.00 vs. 7.55 ± 1.86 ms; p < 0.001). For both original and averaged 10-s heart rate, intra-replicate heart rate differences were significantly lower (p < 0.001) in studies with the expected response than in those with an unexpected time profile.
Discussion
The pattern similarity measurement methodology reduces the residual error of the model, which influences the time profile of the moxifloxacin response. Accuracy of study conduct, represented by intra-replicate heart rate differences, separated studies with and without the expected moxifloxacin time profile.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Adjustment of QT measurement based on pattern-matching techniques reduces intra-individual QTc and improves time profile of moxifloxacin. |
Consistency of heart rates within ECG replicates is a quantifier of study conduct. |
1 Introduction
All new drugs with systemic bioavailability, and drugs for which a new indication or a new target patient population is proposed with a dose increase, have to undergo the so-called thorough QT (TQT) study [1, 2], assessing whether and to what extent the drug affects cardiac repolarization [3]. A negative TQT study establishes the maximum mean effect on the corrected QT interval (QTc) having an upper 90 % confidence interval (CI) below 10 ms [1].
To ensure that the TQT study is capable of detecting such small drug-induced QTc effects, a proof of assay sensitivity is needed. Therefore, a pharmacologic positive control is included for which the QTc prolongation is known. Typically, a single 400-mg dose of moxifloxacin is used, as the QTc prolongation of moxifloxacin is well established, reaching the maximum around 10–14 ms between 2–4 h after oral administration or at the end of a 1-h infusion [4–7]. Two regulatory requirements are placed on moxifloxacin-based assay sensitivity. The study must (i) detect the mean effect of moxifloxacin-induced placebo-corrected QTc prolongation with lower 90 % CI above 5 ms, and (ii) establish ‘typical’ time course of the effect that is based on existing regulatory experience [1]. If both these conditions are satisfied, the moxifloxacin QTc response is considered to follow an expected time profile.
The ‘typical’ time profile is influenced by pharmacokinetic factors (e.g., over-encapsulation, food ingestion, and body mass index of subjects [8]), study conduct, and QTc measurement. Although the factors of the pharmacokinetic properties influence the exposure and the rate of absorption, the moxifloxacin time profile of successful assay sensitivity proof is still expected to parallel the pharmacokinetic profile.
Of all the influences, factors of QTc measurements are of obvious importance. They include study conduct, appropriateness of QT measurement, and QTc computation. While moxifloxacin does not change heart rate, optimized QTc computation might lead to reduced QTc variability [9]. If study subjects are not investigated in a standardized environment (e.g., not systematically quiet relaxed supine positions), heart rates within ECG replicates of the same time point could vary, influencing the accuracy of heart rate correction and consequently of the moxifloxacin response.
No gold standard for QT interval measurement can be postulated, since the definition of the QRS onset and T-wave offset depends on electrocardiographic (ECG) interpretation. However, since the investigated QTc effect of moxifloxacin is placebo corrected, the exact definition of the T-wave offset (and of QRS onset) is less important as long as the measurement is systematic with consistent ECG interpretation. Hnatkova et al. [10] proposed a methodology for ensuring consistent QT measurements using the so-called pattern-matching adjustment of QT interval measurements based on similarity. It seems intuitively plausible that by ensuring consistent ECG interpretation, the moxifloxacin response would be detected more consistently and systematically. The consistency of moxifloxacin response can be quantified in different ways, with the residual error of a concentration–QTc model likely being the most direct.
This study therefore tested the hypothesis that pattern matching leads to an improved moxifloxacin response, defined as the reduction in the residual error in the concentration–QTc model. Additionally, we evaluated the influence of the quality of study conduct on the appropriateness of the moxifloxacin response. Since no other data were available, we approximated the quality of study conduct by the heart rate stability during individual time points.
2 Methods
2.1 Data
TQT study reports (N = 238) submitted to the US FDA between January 2006 and December 2012 were available for the purposes of this study. From these, we excluded TQT studies completed before 2005 (N = 14); that used an unacceptable design, such as a two-stage investigation (N = 21); or had no digital 12-lead ECGs available (N = 5)—note that there might be delay between the completion of the study and submission of the report to the Agency. In the remaining 198 studies, a regulatory decision was previously made whether the time profile of QTc changes on moxifloxacin was as expected (N = 179) or whether the test of assay sensitivity failed because of an unexpected time profile (N = 19) (examples in Fig. 1).

An example of (a) an expected time profile for moxifloxacin response and (b) an unexpected time profile for moxifloxacin
Moxifloxacin plasma concentrations were available in 64 studies (32 %) of the 198 non-excluded studies. From this set, five studies were excluded, as the sampling of the moxifloxacin plasma concentrations was not sufficient, and one for data issues. The remaining studies (N = 58) were used to evaluate the hypothesis that pattern matching reduces the residual error of a linear concentration–QTc model; of these studies, four studies had an unexpected moxifloxacin time profile.
For the analysis of factors that influence the moxifloxacin time profile, we compared studies with an unexpected moxifloxacin time profile (N = 19) with the studies with expected QTc profile of moxifloxacin and available moxifloxacin concentration data (N = 54). This included 48 cross-over and 25 parallel studies (two hybrid design, i.e., nested cross-over). The choice of baseline was time-matched for all parallel studies and for 19 of the cross-over studies; the remaining of the cross-over studies (N = 29) used pre-dose baseline.
In 8 of the 58 of studies, moxifloxacin was administered on multiple days and each day was treated as an individual study in the analysis. This resulted in an ‘additional’ ten studies, of which all but three had an expected moxifloxacin time profile and available moxifloxacin concentration data. The total dataset thus included 65 studies (four of which had an unexpected moxifloxacin profile) with available moxifloxacin concentration data, and 22 studies with an unexpected profile (83 studies in total).
All ECG waveforms, QT, and R-R interval (RR) measurements for the placebo, moxifloxacin, and baseline treatment periods, and, where available, moxifloxacin plasma concentrations, were retrieved from the FDA database. All ECG waveforms were 10-s 12-lead recordings and were retrieved from the ECG Warehouse (http://www.ecgwarehouse.com). The ECGs were most often sampled at 1 kHz (N = 46) or 500 Hz (N = 20), with the remainder having a sampling frequency of 200 Hz or less (N = 7). The amplitude resolution was typically 2.5 μV (N = 39) or 1.0 μV (N = 13), with the rest being <1.0 μV (N = 2) or >2.5 μV (N = 19). The QT was measured in lead II in 56 studies, globally in 12 studies, in V2 in three studies, and in V3 and in V5 in one study each.
2.2 Moxifloxacin Response Evaluation
The moxifloxacin response was evaluated by the standard ΔΔ approach. That is, the change from baseline on moxifloxacin and on placebo at each time point was calculated, and subsequently the baseline-corrected placebo response was subtracted from the baseline-corrected moxifloxacin response. In cross-over studies without time-matched baseline, the average of pre-dose time points was used for baseline correction. Since moxifloxacin does not influence heart rate, the analysis of its response was based on the Fridericia corrected QTc interval [9, 11].
The relationship between the moxifloxacin plasma concentrations and the ΔΔQTc values was modeled using a linear-mixed effects model with random effects on the slope and intercept as previously described [12]. The residual error of the model was used to quantify the quality of the QTc measurements in addition to the intra-subject variability.
2.3 Pattern Matching
The principle of the pattern-matching approach [10] is to extract a segment around a fiducial point, i.e. the T-wave offset or QRS-onset, from a globally formed lead (e.g., the vector magnitude or root-mean-square of the leads by time), align all extracted segments from one subject, and correct the aligned measurements based on waveform similarity. The pattern matching approach was shown to decrease the intra-subject variability [10]. The reduction reflects the extent of reader variability, and does not require any operator intervention. An example of this is shown in Fig. 2, where applying pattern matching corrected the T-wave measurement by 46 ms. In fact, the corrected T-wave offset aligns with the intersection of the steepest slope and isoelectric line, probably how the other ECGs from this subject were measured.

Example of an electrocardiograph where the measurements were corrected using the so-called pattern-matching methodology originally proposed by Hnatkova et al [10]. The vertical lines represent the original (dashed) and pattern-corrected (solid) Q-onset and T-wave offset. The difference is 3 for the Q-onset and 46 for the T-wave offset. The corrected T-wave offset coincides with the intersection of the maximum slope (dashed) and the isoelectric line (solid)
To achieve 1 ms precision of the alignment patterns, the ECG waveforms were cubic spline interpolated to 1,000 Hz sampling frequency. Noise reduction of the ECGs was achieved by applying a zero-phase infinite impulse response filter. QRS complexes were detected and delineated using a previously developed system [13]. Subsequently, cardiac beats of non-sinus origin and their surrounding beats were excluded. Using the remaining cardiac beats, the 10-s average heart rate and the median QRST waveform was computed. The fiducial points provided by the study sponsor were projected onto the median waveform.
The fiducial points in the median QRST waveforms associated with the QRS onset and T-wave offset were re-positioned using pattern matching [10]. This resulted in a re-measured QT interval duration.
The original QT interval duration and heart rate provided by the study sponsor and the re-measured 10-s heart rate and pattern-matching re-positioned QT interval duration led to four different possibilities of QTc calculation: original QT and original heart rate (data 1), original QT and re-measured 10-s heart rate (data 2), re-positioned QT interval and original heart rate (data 3), and re-positioned QT interval and re-measured 10-s heart rate (data 4). All four data types were included in the results to compare the benefit by pattern-matching re-positioning or by averaging heart rate alone or by their combination.
2.4 Quality of Study Conduct
All studies required that, for every time point, the investigated subjects were placed in standardized supine resting positions during which the replicated ECG measurements were made. Assuming strict adherence to this requirement, heart rates of replicated ECGs of the same time point should be nearly the same in each subject. Consequently, to approximate the quality of the study conduct, we evaluated the difference between the maximum and minimum heart rate in each time point and each subject. The median value of these differences over all study subjects and all time points was used as the characterization of the adherence to the protocol. The calculation was repeated for the originally reported heart rate values and for the heart rate values derived from the complete 10-s ECG tracings (as used in data 2 and data 4).
2.5 Statistical Analysis
Where appropriate, and unless stated otherwise, continuous data are presented as mean ± standard deviation.
The impact of the pattern matching on the concentration-c analysis was evaluated by comparing the residual error of the concentration–QTc model before and after the application of the pattern-matching adjustment and before and after the recalculation of heart rates. Concentration–QTc modeling was performed using Proc Mixed in SAS 9.2 (SAS Institute, Cary, NC, USA). The residual errors in the model obtained for data 1–4 were compared using the paired t test. These characteristics of study conduct quality were compared using a Mann–Whitney test. p values <0.05 were considered statistically significant. All statistical tests were performed using the R 2.15.3 (R Foundation for Statistical Computing, Vienna, Austria).
3 Results
The studies used in the analyses (N = 83) included a median 81 (range 19–345) subjects and had a median of 45 % females (range 0–100). The average maximum moxifloxacin concentration was 2.3 ± 0.6 (range 1.7–4.1, N = 61) μg/mL and 1.8 ± 0.2 (range 1.6–2.2, N = 4) μg/mL in studies with the expected and unexpected time profile and available moxifloxacin plasma concentrations, respectively (p = 0.03 between the two groups of studies).
3.1 Pattern Matching
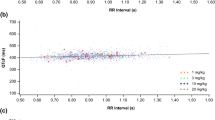
The difference between the original QT and the pattern corrected (QT pattern) was −0.39 ± 4.87 ms. The residual error of the model was 8.43 ± 2.00 for data 1, and 8.23 ± 1.88 ms for data 2 (data 1 vs. data 2; p < 0.001), 7.55 ± 1.86 ms for data 3 (data 3 vs. data 2; p < 0.001), and, finally, 7.12 ± 1.62 ms for data 4 (data 4 vs. data 3; p < 0.001). The improvement of each method compared with data 1 is shown in Fig. 3. Substantial improvements are seen in data 3 and data 4 in comparison with data 1. There was a small decrease in the intercept for data 3 and 4 compared with data 1 and 2 (2.25 ± 2.58 and 2.34 ± 2.59 vs. 1.67 ± 1.85 and 1.68 ± 1.84 for data 1 through 4, respectively). Additionally, there was a slight increase in slope, but no trend for increase or decrease across the different data types as observed for the residual errors of the model (4.05 ± 1.01, 3.98 ± 1.05, 4.12 ± 1.01, and 4.07 ± 1.02 for data 1 through 4, respectively).The data sequence also led to a slight decrease in the estimated mean effect and standard error (mean ± SE), using observed moxifloxacin concentrations (11.53 ± 1.20, 11.45 ± 1.19, 11.01 ± 1.10, 10.91 ± 1.08, for data 1 through 4).

Scatter diagrams comparing the (a) residual errors of the model for data 1 [original QT and R-R interval (RR) used for QTc computation] with those of data 2 (original QT and 10-s average RR); (b) the residual errors of the model for data 1 with those of data 3 (QT re-measured using pattern matching and original RR); (c) residual errors of the model for data 1 with those of data 4 (QT re-measured using pattern matching and 10-s average RR); (d) residual errors of the model for data 2 with those of data 3; (e) residual errors of the model for data 2 with those of data 4; (f) and residual errors of the model for data 3 those of data 4. The black line indicates the identity, meaning the model residual was equal
3.2 Quality of Study Conduct
The median intra-replicate maximum heart rate difference was 5.98 ± 2.19 (N = 22) beats per minute (bpm) for studies with an unexpected time profile and 3.86 ± 1.41 bpm (N = 61) for studies with an expected time profile (p < 0.001, Fig. 4). Similar values were obtained using the 10-s average heart rate, yielding 5.60 ± 2.42 bpm (N = 22) for studies with an unexpected time profile and 3.47 ± 1.13 bpm (N = 61) for studies with the expected time profile (p < 0.001, Fig. 4).

Comparison between the maximum intra-replicate heart rate differences between studies with an expected moxifloxacin time profile (N = 61) compared with those without (N = 22). The maximum intra-replicate heart rate differences computed using the raw heart rate is shown in (a), and the heart rate average for the 10-s recordings is shown in (b). In both cases, the difference between the groups of studies was statistically significant (p < 0.001)
4 Discussion
There are two principal findings of this investigation. First, the pattern-matching methodology (regardless of whether combined with the original heart rate measurements or with the heart rate-derived 10-s RR interval averages) leads to an improved moxifloxacin time profile with significantly lowered residual error of the concentration–QTc model. Second, the range of heart rates of replicated ECGs within the same time point appears a valid quantifier of study quality since it separated studies with and without the expected moxifloxacin time profile.
Additionally, we noticed lower maximum moxifloxacin concentration in studies with an unexpected moxifloxacin time profile compared with the studies with an expected concentration–QTc relationship. This might suggest that the unexpected moxifloxacin response might also be driven by below-expectation exposure.
The residual error reduction of the concentration–QTc model by the so-called pattern-matching adjustment suggests that departures from the expected time profile of the moxifloxacin response can be attributed to reader variability. While our results support the notion that reader variability is a source of QTc variability, there are likely also other sources. The residual error reduction varied between studies, likely because of multiple factors, including the number of available ECGs, their signal quality, and the accuracy of electrode positioning. If only a small number of low-quality ECGs are available and if their measurements are substantially irregular, the pattern-matching methodology is unlikely to improve the data. Last, the pattern–matching adjustments also led to a slight decrease in the intercept and increase in the slope. This might suggest that the intercept could also be influenced by the variability in the measurements. Moreover, the application of pattern matching caused a slight decrease in the estimated effect, using the observed maximum concentration by study, and a decrease in the standard error.
Studies with an unexpected time profile had a higher intra-replicate difference of heart rate, which suggests that the quality of the study conduct also influences the observed moxifloxacin time profile. This is not surprising, since it can be expected that overall quality of a clinical investigation and adherence to the per-protocol procedures increases the likelihood of successful outcome. It also seems that, in some cases, the unexpected time profile may be caused by low exposure. However, since the moxifloxacin plasma samples were not analyzed in the majority of the studies with an unexpected QTc time profile, no definite conclusions are possible in this respect. Thus, an unexpected time profile of moxifloxacin can potentially be caused by study conduct, as evidenced by higher intra-replicate heart rate differences, by unexpectedly lower plasma concentrations, by reader variability, or by any combination of these factors. It is unlikely that any of these metrics alone would universally predict studies that do and do not have an expected moxifloxacin time profile. The principal problem is the signal-to-noise ratio. Thus, if the exposures are large, the QTc effects increase and consequently, heart rate stability, reader variability, and general quality of the study conduct likely matter less. With lower exposures, the opposite is the case and all aspects of diligent signal acquisition and processing matter more.
To our knowledge, no similar evaluations have been previously reported. We can therefore only compare our results with the seminal publication describing the pattern-matching methodology [10] and work by Meyer et al. [14], showing reduction of intra-individual QT variability by applying pattern-recognition software. Our observations are in full agreement with these reports.
Our findings suggest that when conducting TQT studies, it is important to ensure that the requirement of stable supine resting positions during individual study time points is strictly observed. Also, it is important to measure QT intervals consistently. While strict consistency of the measurement might be difficult to achieve during visual interpretations of ECG patterns, computerized technology (e.g., the pattern matching used in this study), is available to improve the systematic nature of ECG measurements. Finally, based on the analyzed studies, it can be recommended that moxifloxacin plasma samples are obtained in all TQT studies. This would allow the evaluation of whether low exposure contributes to the unexpected outcome that is observed.
4.1 Limitations
Several limitations also need to be considered. We used only studies with available moxifloxacin plasma concentrations to evaluate the intra-replicate heart rate differences. Other studies could also have been used in these comparisons, but the restriction allowed us to investigate an unbiased set of studies. The ECG data available in the FDA database are restricted to 10-s duration of individual tracings. We were therefore unable to study a longer history of heart rates preceding QT interval measurements. It has been shown that using a longer heart rate history to correct for QT/RR hysteresis lowers the residual error of the QT/RR model [15]. It is possible if not likely that accounting for QT/RR hysteresis would have further reduced the residual errors of the concentration–QTc model. Last, we assumed that the ECG signals obtained from the FDA database are unfiltered, as information on any filtering was not available. Our universal use of a zero-phase infinite impulse response filter was unlikely to influence the results in any significant way.
5 Conclusion
In spite of these limitations, this investigation shows that by applying computerized tools that make QT interval measurements consistent improves the moxifloxacin time profile. The investigation also suggests that in TQT studies using replicated ECG readings during controlled time point windows, the ranges of heart rates within the replicated ECG readings are a valid quantifier of the quality of study conduct.
References
ICH. Guidance for Industry E14 Clinical Evaluation of QT/QTc interval prolongation and proarrhythmic potential for non-antiarrhythmic drugs; 2005.
ICH. Guidance for Industry E14 Clinical Evaluation of QT/QTc interval prolongation and proarrhythmic potential for non-antiarrhythmic drugs. Questions and answers; 2008.
Malik M, Garnett CE, Zhang J. Thorough QT studies: questions and quandaries. Drug Saf. 2010;33(1):1–14.
Bloomfield DM, Kost JT, Ghosh K, Hreniuk D, Hickey LA, Guitierrez MJ, et al. The effect of moxifloxacin on QTc and implications for the design of thorough QT studies. Clin Pharmacol Ther. 2008;84(4):475–80.
Malik M, Hnatkova K, Schmidt A, Smetana P. Electrocardiographic QTc changes due to moxifloxacin infusion. J Clin Pharmacol. 2009;49(6):674–83.
Iwamoto M, Kost JT, Mistry GC, Wenning LA, Breidinger SA, Marbury TC, et al. Raltegravir thorough QT/QTc study: a single supratherapeutic dose of raltegravir does not prolong the QTcF interval. J Clin Pharmacol. 2008;48(6):726–33.
Kubitza D, Mueck W, Becka M. Randomized, double-blind, crossover study to investigate the effect of rivaroxaban on QT-interval prolongation. Drug Saf. 2008;31(1):67–77.
Florian JA, Tornoe CW, Brundage R, Parekh A, Garnett CE. Population pharmacokinetic and concentration–QTc models for moxifloxacin: pooled analysis of 20 thorough QT studies. J Clin Pharmacol. 2011;51:1152–62.
Garnett CE, Zhu H, Malik M, Fossa AA, Zhang J, Badilini F, et al. Methodologies to characterize the QT/corrected QT interval in the presence of drug-induced heart rate changes or other autonomic effects. Am Heart J. 2012;163(6):912–30.
Hnatkova K, Smetana P, Toman O, Bauer A, Schmidt G, Malik M. Systematic comparisons of electrocardiographic morphology increase the precision of QT interval measurement. Pacing Clin Electrophysiol. 2009;32(1):119–30.
Fridericia LS. Die Systolendauer im Elektrokardiogramm bei normalen Menschen und bei Herzkranken. Acta Med Scand. 1920;54(1):17–50.
Garnett CE, Beasley N, Bhattaram VA, Jadhav PR, Madabushi R, Stockbridge N, et al. Concentration–QT relationships play a key role in the evaluation of proarrhythmic risk during regulatory review. J Clin Pharmacol. 2008;48(1):13–8.
Johannesen L, Galeotti L. Automatic ECG quality scoring methodology: mimicking human annotators. Physiol Meas. 2012;33:1479–89.
Meyer O, Ferber G, Greig G, Holzgrefe HH. Pattern recognition analysis of digital ECGs: decreased QT measurement error and improved precision compared to semi-automated methods. J Electrocardiol. 2013;46(2):118–25.
Malik M, Hnatkova K, Novotny T, Schmidt G. Subject-specific profiles of QT/RR hysteresis. Am J Physiol Heart Circ Physiol. 2008;295(6):H2356–63.
Acknowledgments
The opinions presented here are those of the authors and no official support or endorsement by US Food and Drug Administration is intended or should be inferred. Lars Johannesen, Christine Garnett, and Marek Malik have no conflicts of interest directly related to this article. Marek Malik is an Honorary ORISE Research Fellow of the US Food and Drug Administration.
The authors are grateful to Dr. Norman Stockbridge of the US Food and Drug Administration for his substantial guidance on the topic and his help with preparing the manuscript. This project was supported in part by an appointment to the Research Participation Program at the Center for Drug Evaluation and Research administered by the Oak Ridge Institute for Science and Education through an interagency agreement between the US Department of Energy and the US Food and Drug Administration.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Johannesen, L., Garnett, C. & Malik, M. Impact of Electrocardiographic Data Quality on Moxifloxacin Response in Thorough QT/QTc Studies. Drug Saf 37, 183–189 (2014). https://doi.org/10.1007/s40264-014-0142-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40264-014-0142-2