
Abstract
Background
After more than three decades of free medicines for the elderly in Spain, in the context of heavy austerity reforms of public financing, a set of cost-sharing reforms on pharmaceutical prescriptions with regional variants have been established in Spain since July 2012.
Objective
The purpose of this analysis is to present the first attempt to provide accurate estimates of the overall impact at the regional level of these cost-sharing reforms.
Methods
We estimated the impact of the reforms on the quantity of dispensed medicines during the first 14 months. We estimated 17 autoregressive integrated moving average (ARIMA) time series models of the monthly number of prescriptions dispensed in pharmacies for the period January 2003–May 2012 in each one of the 17 regions (Autonomous Communities) of Spain. We calculated dynamic forecasts for the horizon June 2012–July 2013 in order to estimate the counterfactual (number of prescriptions that would had been observed without the intervention), and we estimated the impact of cost-sharing changes as the difference between the observed number of accumulated prescriptions at 3, 6, 12, and 14 months and the number predicted by our time-series models (in percentages).
Results
During the last decade the number of dispensed prescriptions has experienced rapid and continuous increases. In the first 14 months after the co-payment reform, the total number of prescriptions decreased dramatically, by more than 20 % in Catalunya, Valencia, and Galicia, by more than 15 % in nine other regions, and by more than 10 % in 15 of the 17 Spanish regions. The results of our model suggest that the new co-payment caused an abrupt shift in the mean level of the time series. No shift in trend has been detected; the previous positive trend remains unchanged in most of the Autonomous Communities.
Conclusion
After decades of unsuccessfully trying to reduce drug spending in the Spanish National Health System through actions on prices and on prescribers, the co-payment established in mid-2012 led to a dramatic reduction in the use of drugs. The health effects of this reduction are not known.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
After a decade of rapid and continuous increases, the number of dispensed prescriptions decreased dramatically in the first year after the co-payment reform. |
The new co-payment appeared to cause an abrupt downward shift in the number of dispensed prescriptions, although the previous positive trend appears unchanged in most regions. |
Although the level of the new national co-insurance rate is dependent on income, a small portion of patients supports a large part of the expense. |
Regional differences in co-payment policies are also consistent with the hypothesis that the first euro of cost sharing has a large impact on drug use. |
Further research is needed to determine the change in distribution of prescriptions across different patients groups, any reductions in moral hazard, the financial impact on patients, and any effects on health, both positive and negative. |
1 Introduction
The sudden fall of public revenues after 2008 and the long-lasting economic crisis have led many public health systems in European countries to cut public health financing through high co-payments or co-insurance rates on drug prescriptions dispensed in pharmacies [1–6]. This is specially the case in Spain, where until July 2012 nearly three out of four prescriptions were dispensed free of charge, Spain being until then one of the European countries with the highest number of prescriptions per capita [7].
In some national health systems funded primarily though taxation, as the Spanish one is, medical treatments are free for a large part of the population. That is because those systems are concerned with equity of access to healthcare. Since 1978, Spanish pensioners, whether they were in a low-, middle-, or high-income bracket, had enjoyed free access to practically all medicines prescribed by National Health System (NHS) physicians. As a consequence, there was a significant increase in the number of prescriptions, and public expenditure per patient rose by around 25 % in the first year of free medication [8]. Potential moral hazard—the increase in consumption by those who acquire the right to free medicines, attributable solely to this change in status—was concentrated in the consumption of those medicines affected by 40 % co-insurance before the medication became free, i.e., those that had been most expensive for the patient. Over-prescription [9]—when a prescription is given without the pertinent indication—is a common form of inappropriate utilization of healthcare that causes not only an inefficient increase in costs but also a higher number of adverse events and related health problems [10]. There is broad evidence that over-prescribing is associated with an increased risk of adverse drugs events, morbidity, mortality, and healthcare utilization, such as emergency visits [11, 12].
Free medication for all Spanish pensioners has also been shown to be clearly inequitable. As it was independent of financial circumstances, a pensioner who received a large pension or had assets worth millions would pay nothing, while an unemployed person or a family with young children and an income of barely €1,000 per month would pay their share. Half of all the cost sharing contributed by patients is concentrated in a small group of sick people: it was provided by just 5 % of users, for whom it can represent a heavy burden [13].
The severe economic crisis in Spain and the subsequent need for a reduction in public expenditure were the main drivers of change [1]. After more than three decades of free medicines for the elderly, in mid 2012 a new co-payment policy was adopted.
In July 2012, a combined set of cost-sharing policies (“three-payment” reforms) described in Table 1 abruptly ended this scenario by first introducing a national co-insurance rate of 10 % for retirees with a monthly income-related cap. The individual monthly contribution was limited via a cap of €8, €18, or €60, depending on income. Additionally, two regions (Catalunya and Madrid) temporarily charged a €1 co-payment per prescription. Finally, the national reforms stopped funding a long list of medicines indicated for minor symptoms, which is equivalent to a 100 % co-insurance rate for those medicines. Under the new co-insurance formula medicines remain free for disadvantaged people. One region (País Vasco) did not apply the national co-insurance reform until 1 year later. These “three-payment” reforms have been applied to the population covered by the NHS, excluding civil servants, who are covered under a different health insurance plan.
The monthly limit encourages long-term patients to concentrate their prescriptions into the minimum number of months. To avoid this opportunistic behavior it would be advisable to set annual limits, which are also easier to manage. In some Autonomous Communities patients pay as if there is no monthly limit, and they have to wait for the reimbursement some months later. This is an expensive bureaucratic procedure and overrides the protective effect of the co-payment ceiling. This was the case for most of the Autonomous Communities during the first months of the new system, as only Catalunya and Andalusia had been able to apply the co-insurance caps in the real time since implementation of the reforms.
Co-insurance rates for non-pensioners increased from 40 to 50 or 60 % depending on income; there is no cap for them. Some medications for chronic conditions have a co-payment rate of 10 % with a maximum per prescription. In the new scheme, the percentage of the price paid depends on income, but, in contrast to how it appears at first glance, the new co-payment is not progressive, because a small number of seriously ill patients who require a lot of medication and are not pensioners bear the greatest load.
The regional fee of €1 per prescription might be an appropriate tool for reducing the over-consumption associated with the cost-free status. It was universal (with a few exemptions for the most deprived), established an annual limit per person, was quite low, and reasonably easy to manage. However, this low-intensity fee was suspended in January 2013 by the Spanish Constitutional Court, not because of a lack of effectiveness or any side effects, but because of a debate regarding whether it is constitutionally within the scope of the Spanish Government and the Regions.
No other demand-side measures—besides the three described above concerning co-payment—were implemented after July 2012.
This is the first attempt to estimate the short-term overall impact at the regional level of the three combined cost-sharing reforms on the quantity of dispensed medicines during the first 14 months after their establishment.
2 Data and Methods
We used monthly NHS data regarding dispensed prescriptions in each Autonomous Community from January 2003 to July 2013. These data are available at the webpage of the Spanish Ministry of Health [14].
First, we estimated 17 autoregressive integrated moving average (ARIMA) time series models of the monthly number of prescriptions dispensed in pharmacies for the period January 2003–May 2012. More specifically, for each Autonomous Community we used a univariate ARIMA model. In order to identify the models, following the Box–Jenkins method [15] we estimated average-rank regressions with annual data (for deciding between logarithmic or linear models) and we used the standard integration tests to specify the number of regular and seasonal differences needed. The significance of the regression coefficients and the residual correlograms guided the interactive process of selection of regressors. In some Autonomous Communities we included specific dummy variables for certain months or time intervals with extreme-outlier-residuals (more than 2 standard deviations in absolute value). We also calculated the Q test by Ljung–Box–Pierce (Portmanteau test) in order to verify the white noise condition for the residuals. We selected the model with the best fit among alternative specifications that had passed all the tests described above. The fit was measured with the Aikaike Information Criterion (AIC) and the coefficient of determination.
Second, we calculated dynamic forecasts for the post-sample period of June 2012–July 2013 in order to estimate the counterfactual number of prescriptions that would have been observed if the reform had not taken place.
Third, we estimated the impact of cost-sharing changes as the difference between the observed number of accumulated prescriptions at 3, 6, 12, and 14 months and the number predicted by our time-series models (in percentages). We also calculated 95 % confidence intervals adjusted by correlations between subsequent forecasts. For each Autonomous Community we calculated 95 % confidence intervals of the predicted effects on the overall impact of the co-payment reform. To estimate confidence intervals for the cumulative effects of the new co-payment, we derived the specific formulas (available upon request), based on the monthly forecasts resulting from the ARIMA models and taking into account that the standard errors of consecutive predictions are correlated.
Although the reform came into force in July 2012, our forecast horizon starts in June 2012 in order to consider the anticipation effect (stockpiling) in the month before the reform.
3 Results
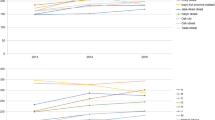
The time series for the monthly number of prescriptions from January 2003 to July 2013 points to a dramatic change in July 2012. Figure 1 presents three of those time series for three selected regions that represent three “models” of cost sharing being implemented: Catalunya (regional fee of €1 per prescription and new co-insurance rates), Castilla-León (only national co-insurance), and País Vasco (no change in cost sharing until July 2013). According to these descriptive data, an anticipation effect (stockpiling) happened in all regions the month before the measure was enacted. It also appears that in Catalunya there was a large drop in the number of prescriptions in July 2012, despite the fact that only the €1 fee was applied to pensioners in this region from July to September. This immediate drop was equal to or higher than in other regions where the national co-insurance rate was applied, as is the case in Castilla-León.

Monthly number of prescriptions from January 2003 to July 2013 in three Autonomous Communities
Table 3 in the Appendix shows the detailed estimates of the 17 ARIMA models, their coefficients of determination, and the Q 6 and Q 12 statistics of the Ljung–Box–Pierce test Portmanteau.
According to the results of our ARIMA models, a significant, dramatic, and sudden reduction in the number of dispensed prescriptions compared to the absence of reforms has been estimated for all regions (Table 2) with the exception of País Vasco, where only the delisting policy had been applied prior to July 2013.
The highest impact of the intervention has been observed in Catalunya, where the co-insurance reform and the new regional co-payment were applied concurrently. Our estimation of the impact in Catalunya is a 23.7 % decrease in the number of prescriptions after 14 months (95 % CI −27.0 to −20.5). Applying the cap at purchase reduces the impact of the co-payment; if patients have already reached their maximum for the month, they get their prescription from the pharmacy free of charge. Among the regions that only applied the state co-payment, Andalucía was the only one able to manage the cap in time. In the remaining regions patients were required to prepay and were reimbursed afterwards. Andalucía showed the smallest reduction in prescriptions in this group [9.4 % (95 % CI −13.4 to −5.5)].
In summary, concurrent co-payment policies had a dramatic impact, which is statistically significant when applied to a NHS system that used to provide free drugs to retired patients. Catalunya, where the €1 per prescription was applied first and then the state co-payment was added (see details in Table 1), experienced a 23.9 % reduction in the number of prescriptions in 12 months. By contrast, País Vasco, which did not apply any co-payments until July 2013, had a reduction of only 3.8 %.
4 Discussion and Policy Implications
Spain had become one of the countries with the highest per capita levels of pharmaceutical usage in the world: a comparison of per capita usage levels in 14 developed countries for 14 disease areas concluded that France, the USA, and Denmark have generally high levels of usage, although this is not uniform across all diseases or drug categories. Spain was one of three countries with higher per capita usage of pharmaceuticals for the treatment of osteoporosis, hepatitis C, cancer, and dementia, and antipsychotics [7]. However, mainly due to lower prices, Spanish per capita expenditure (adjusted by purchasing parity power) was only 3.5 % above the OECD average in 2011 [16]. Several studies have shown that medication over-prescription not only affects costs, it induces adverse health outcomes, particularly in the elderly, with the reduction in the number of drugs given being the main preventable factor [12, 17].
The severe economic crisis in Spain and the subsequent need for a reduction in public expenditure were the main drivers of change. After more than three decades of free medicines for the elderly, co-payment was established in mid-2012.
A notable contribution of this analysis is the provision of evidence regarding the important changes in the demand for prescription of medicines as a response to increases in the price paid by the patient and showing that a small linear co-payment (€1 per prescription) has a large impact on the use of medicines. By exploiting regional differences in co-payment policies, our results are also consistent with the hypothesis that the first euro of cost sharing has a large impact on drug use [18].
The estimates reported in this paper provide an aggregate measure of the impact at the regional level of the concurrent measures that came into force with the Decree 16/2012. This impact has been measured using the number of prescriptions issued in the NHS. Despite the fact that the “three-payment” reforms are the most notable, other measures taken during the period, such as the exclusion of undocumented immigrants from healthcare coverage, may also have had some influence on the number of prescriptions.
Our results should be taken with caution as we do not know whether this reduction in prescriptions was the result of a reduction in the practice of overprescribing and useless stockpiling, which would indicate a positive effect, or rather the result of some patients not being able to access medicines they needed (which would be a negative effect), or a mix of the two. Another obvious limitation of our results is that they are based on the dynamics of the number of prescriptions at the regional level, but there is no available information on changes in the number of a more homogeneous consumption measure such as defined daily doses prescribed.
Co-payment reform could change both the level and the time trend of the number of prescriptions, but for now we cannot make reliable statements about the magnitude of these changes. Rigorous evaluations should wait until the NHS discloses the data to researchers. In fact, our models suggest that the new co-payment caused an abrupt shift in the mean level of the time series of dispensed prescriptions. However, so far our data and methods do not allow us to test rigorously the hypothesis of an unchanged trend, an issue that clearly deserves further research. Our provisional results show that in most of the Autonomous Communities the previous positive trend, i.e., the monthly growth rate, seems to remain unchanged after the reform. This may be due to the fact that other prescription incentives have not been altered. The effects of various interventions on drug prices [19] applied in Spain from 1995 to 2006 provide another example of a temporary impact, which is diluted over a year or so.
If prescribing still shows upward trends after typical demand-side measures, such as the co-payment reforms adopted since July 2012, it would be advisable to adopt a wider range of policy measures directed to influence prescription practices. Among those, an appropriate mix of financial incentives (such as indicative or coactive prescribing budgets included or not in comprehensive budgets) and non-financial incentives (such as information, training, prescription monitoring, formularies, and treatment protocols) may be appropriate. Such policies have been mostly neglected in Spain until recently, but they should play a more prominent and urgent role [9].
Even though the reform does not change the underlying trend, as we provisionally conclude, this does not mean that the impact of the co-payment is being progressively diluted; rather, it means that the underlying causes of the proclivity to demand/prescribe/dispense an ever-increasing number of medicines has not gone away. This is because the dynamics of prescriptions depends on many other factors besides co-payment: industry pressure on prescribers, general practitioner workload, training and incentives for prescribers, etc. In fact, it could be that the initial effect, i.e., the sudden shift in the mean level of the number of prescribed medicines, is non-permanent, changing once the awareness of paying a price is instilled in patients’ minds. If that is the case, in a few months we will see the series back at their pre-reform levels. This will eventually be revealed with an impact analysis with more appropriate assessment techniques and more disaggregated data.
Finally, some regions were not able to manage individual’s monthly caps effectively because they lack individual income data and information technology. Those regions implemented an expensive and lengthy administrative reimbursement process for those patients that had paid over their cap. It would have been better either to wait or to design a simpler procedure.
It would be a mistake to increase cost sharing on medication across long-term and effective treatments. If one thing is clear from randomized and natural experiments, it is that cost sharing should be lower the greater the need for the treatment and the more effective that treatment is [20]. The high concentration of expenditure in patients with long-term conditions recommends the maintenance of low rates, together with the application of upper limits to the amount payable out of the patient’s pocket, either as a monetary amount that would be the same for all, or—a finer adjustment—as a percentage of each patient’s income. Otherwise, the cost in the form of greater use of emergency and hospital services may more than cancel out the savings attained through cost sharing for chronic patients [21].
5 Conclusions
This article provides empirical evidence that after a continuous increase in the number of prescriptions dispensed in Spain during the last two decades, insensitive to the many price control measures, the total number of prescriptions has been dramatically cut by nearly a quarter after 14 months of the “three payment” reforms in Catalunya, and by more than one tenth in 15 out of 17 Spanish regions.
Overall, our results provide new information on the price sensitivity of the prescriptions issued in a NHS, and they also raise several new questions relevant to policies. It is necessary and urgent to know which groups of patients and therapeutic groups have been most affected, in order to evaluate the potential reduction in the abuse (moral hazard) attributable to free medicines and equity issues.
These questions deserve urgent attention from health policy makers in order to evaluate overall welfare effects of these finance-oriented reforms and to redefine co-payment policies. Potential unwanted side effects on adherence, health, and use of other health resources should also be investigated.
References
Legido-Quigley H, Otero L, la Parra D, Alvarez-Dardet C, Martin-Moreno JM, McKee M. Will austerity cuts dismantle the Spanish healthcare system? BMJ. 2013;346:f2363.
Urbanos R, González B, Puig-Junoy J. La crisis económica llega a la sanidad. Economistas 2012;131:158–67.
Thomson S, Mossialos E. Primary care and prescription drugs: coverage, cost-sharing, and financial protection in six European countries. Issue Brief (Commonw Fund) 2010;82:1–14.
Carone G, Schwierz C, Xavier A. Cost-containment policies in public pharmaceutical spending in the EU. Economic Papers 461. Belgium: European Commission; 2012 Sep.
Vandoros S, Stargardt T. Reforms in the Greek pharmaceutical market during the financial crisis. Health Policy. 2013;109:1–6.
Smith PC. Universal health coverage and user charges. Health Econ Policy Law. 2013;8(4):529–35.
Richards M. Extent and causes of international variation in drug usage. A report to the Secretary of State for Health 2010. https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/151987/dh_117977.pdf. Accessed 23 March 2014.
Puig-Junoy J, García-Gómez P, Casado-Marín D. Free medicines thanks to retirement: moral hazard and hospitalization offsets in an NHS. TinBergen Institute Discussion Paper TI 2011–108/3. http://papers.tinbergen.nl/11108.pdf. Accessed 2014 Mar 25.
Cabiedes L, Ortún V. Prescriber incentives. Chapter 9. In: Puig-Junoy J, editor. The public financing of pharmaceuticals. Northampton: Edward Elgar Publishing; 2005.
Meneu R, Peiró S. Elementos para la gestión de la prescripción y la prestación farmacéutica. Barcelona: Masson Ed; 2004.
Xu KT, et al. Over-prescribing of antibiotics and imaging in the management of uncomplicated URIs in emergency departments. BMC Emerg Med. 2013;13:7.
Sanfelix-Gimeno G, Peiro S, et al. Pharmaceutical prescription in primary care. SESPAS report 2012 [in Spanish]. Gac Sanit. 2012;26(Suppl 1):41–5.
Puig-Junoy J. Paying for free healthcare. The role of prices in our healthcare decisions. Barcelona: Libros del Lince; 2013.
Ministerio de Sanidad, Servicios Sociales e Igualdad. http://www.msssi.gob.es/. Accessed 23 March 2014.
Box GEP, Jenkins GM, Reinsel GC. Time series analysis: forecasting and control. 4th ed. San Francisco: Willey; 2008.
OECD. Health at a glance 2013: OECD indicators. Paris: OECD Publishing; 2013.
Laroche M-L, et al. Is inappropriate medication use a major cause of adverse drug reactions in the elderly? Br J Clin Pharmacol. 2007;63(2):177–86.
Ellis RP. Five questions for health economists. Int J Health Care Finance Econ. 2012;12:217–33.
Moreno-Torres I, Puig-Junoy J, Raya JM. The impact of repeated cost containment policies on pharmaceutical expenditure: experience in Spain. Eur J Health Econ. 2011;12:563–73.
van de Vooren K, Curto A, Garattini L. Optional copayments on anti-cancer drugs. BMJ. 2012;346:f349.
Chandra A, Gruber J, McKnight R. Patient cost sharing in low income populations. Am Econ Rev: P&P 2010;100:303–8.
Acknowledgments
This research has been financed by the Catalan Agency for Health Information, Assessment and Quality (CAHIAQ). The funder has played no role in the study, and the researchers are completely independent of the funders.
Conflict of interest
There is no relevant conflict of interest to disclose.
The plan for the analysis of data was designed by all of the authors. Beatriz G. Lopez-Valcarcel and Santiago Rodríguez-Feijoó conducted the statistical analysis. Jaume Puig-Junoy wrote a substantial proportion of the manuscript. He is the guarantor for the overall content of the manuscript and was also in charge of coordinating the manuscript preparation and submission process. All of the authors critically reviewed drafts of the manuscript prior to submission.
Author information
Authors and Affiliations
Corresponding author
Appendix
Appendix
See Table 3.
Y t is the number of prescriptions in month t
t = {1(January 2003), 2(February 2003), … ,}
Log(Y t ) is the natural logarithm of Y t
\( \varepsilon_{t} \) is a white noise series
Definition of dichotomous variables for the treatment of external effects
\( \phi_{j} \), autoregressive parameters
\( \theta_{j} \), moving average parameters
\( \gamma_{j} \), other model parameters (constant, dichotomous and linear trend)
L is the lag operator.
Rights and permissions
About this article
Cite this article
Puig-Junoy, J., Rodríguez-Feijoó, S. & Lopez-Valcarcel, B.G. Paying for Formerly Free Medicines in Spain After 1 Year of Co-Payment: Changes in the Number of Dispensed Prescriptions. Appl Health Econ Health Policy 12, 279–287 (2014). https://doi.org/10.1007/s40258-014-0097-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40258-014-0097-6