
Abstract
Background
There is no cure for alopecia areata, nor is there any universally proven therapy that induces and sustains remission. Treatment choices are frequently based on disease duration, extent, and activity as well as the age of the patient.
Objective
Our objective was to review all randomized controlled studies on the treatment of alopecia areata.
Methods
We performed a search in the biomedical literature database PubMed, and used the terms ‘alopecia areata treatment’ and article type ‘randomized controlled trials’.
Results
Following this algorithm, we reviewed, analyzed, and reported on 29 trials that examined the efficacy of anthralin, antidepressants, biologics, calcineurin inhibitors, corticosteroids (topical and systemic), minoxidil, prostaglandin analogs, sensitizers, and a miscellaneous group of topical and oral drugs with less scientific evidence (aromatherapy, photodynamic therapy, azelaic acid, garlic gel, bexarotene, triiodothyronine, inosiplex, and total glucosides of paeony).
Conclusion
Using the American College of Physicians Guideline grading system, our assessment is that the majority of published randomized controlled studies of alopecia areata are only of moderate quality. A number of treatments were found to be effective, for example, topical and oral corticosteroids and the sensitizing agents diphenylcyclopropenone and dinitrochlorobenzene; however, most studies had major limitations that hinder the interpretation of these results.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
Alopecia areata affects anagen hair follicles and is considered to be a complex genetic, immune-mediated disease. Alopecia areata can be a chronic relapsing disorder that results in a non-scarring hair loss of which there are three major clinical presentations. Alopecia areata affects children and adults, both males and females, and people of all ages and races. Limited alopecia areata is characterized by round or oval patches of non-scarring hair loss in any hair-bearing area. This may advance to loss of all scalp hair (alopecia totalis) or all body hair (alopecia universalis), but many patients may present anywhere along the spectrum from patchy to total body hair loss. Not all patients may require treatment, as it is estimated that up to 50 % of patients with limited disease of less than 1 year’s duration can experience spontaneous hair regrowth [1, 2].
For the patient with alopecia areata, there is currently no universally proven therapy that induces and sustains remission, nor is there a cure for this disease [3]. However, many therapies are available for this disease, and treatment choices are frequently based on disease extent, activity, duration of disease, and age of the patient.
As discussion of all the treatment modalities for alopecia areata is beyond the scope of this article, we elected to focus our attention on randomized controlled studies for the treatment of this disease.
2 Materials and Methods
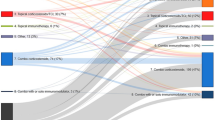
In April 2014 we performed a search in PubMed, a database that comprises 23 million citations for biomedical literature from MEDLINE, life science journals, and online books. We used the terms ‘alopecia areata treatment’ and article type ‘randomized controlled trials’. A total of 37 items were retrieved (Fig. 1). Review of these articles revealed that the search had detected four articles that were not about alopecia areata [4–7].

Flow chart depicting the identification and selection of studies
Further review of the remaining 33 articles revealed three with an inadequate study design. For example, Khoury et al. [8] performed statistical analyses only on the histological findings and not the clinical outcome. The study by Warin [9], although selected by PubMed as a randomized clinical trial was not a randomized clinical trial, and the study by Kurosawa et al. [10] was found to be neither randomized nor controlled.
Two publications discussed the same trial for the treatment of severe alopecia areata with topical diphenylcyclopropenone and 5 % minoxidil. For this review, we chose the 1993 publication because it contained more complete reported data [11, 12].
Following this algorithm, 29 trials were reviewed and analyzed and will be further discussed in this article. These are summarized in Table 1. Articles in which investigators studied two treatment options at the same time are included twice. Treatment modalities with randomized controlled trials identified using the above methodology include anthralin, antidepressants, biologics, calcineurin inhibitors, corticosteroids (topical and systemic), minoxidil, prostaglandin analogs, sensitizers, and a miscellaneous group of topical and oral drugs with less scientific evidence (aromatherapy, photodynamic therapy, azelaic acid, garlic gel, bexarotene, triiodothyronine, inosiplex, and total glucosides of paeony). No randomized controlled trials were identified on the use of methotrexate, cyclosporin, mycophenolate mofetil, sulfasalazine, squaric acid dibutylester, intralesional corticosteroids, excimer laser, or phototherapy. Studies were judged on the quality of evidence and strength of recommendation for each treatment modality as described in the American College of Physicians’ guideline grading system [57].
3 Results and Discussion
3.1 Anthralin
3.1.1 Rationale for Use in Alopecia Areata
Since first described in 1979, the irritant contact dermatitis caused by anthralin has been thought to be associated with the induction of regrowth of hair. In a non-controlled study, a cosmetically acceptable response to anthralin was seen in 25 % of patients with severe alopecia areata [13].
3.1.2 Randomized Controlled Study
Only one randomized controlled trial used 0.5 % anthralin in patchy alopecia areata. In this study, anthralin was used as the ‘positive control’ to study the efficacy of 20 % azelaic acid in this disease [14]. Similar percentages (p > 0.05) of cosmetically acceptable regrowth in patchy alopecia areata were found for patients treated with anthralin (56.2 %) or azelaic acid (53.3 %). The study was not blinded, and there was no placebo group. Results were maintained even after discontinuation of therapy and no new patches developed in patients with complete response, suggesting control of the disease outside the treated area. The similar results might mean treatments are equally effective or equally ineffective.
3.1.3 Conclusion
Anthralin compared with placebo has not been studied in a blinded, placebo-controlled trial in alopecia areata. Although 0.5 % anthralin has been shown to have similar results to 20 % azelaic acid in the management of patchy areata, spontaneous regrowth cannot be excluded in this study population.
3.2 Antidepressants
3.2.1 Rationale for Use in Alopecia Areata
Many patients with alopecia areata describe stressful life events in relationship to the onset and/or progression of their alopecia areata. Although the influence of stress is difficult to prove, it is generally well accepted that stress may play a role in the pathogenesis of alopecia areata.
3.2.2 Randomized Controlled Studies
Two double-blind, randomized, placebo-controlled trials have been published [15, 16]: one studying imipramine and the other studying paroxetine. The antidepressant effect of imipramine is hypothesized as being due to potentiation of adrenergic synapses by blocking uptake of norepinephrine at nerve endings. Paroxetine is a selective serotonin reuptake inhibitor. How either of these medications interacts with the cutaneous nervous system is not known.
Patients who received paroxetine 20 mg once a day for 3 months showed better results than placebo when “any regrowth” was considered as the primary endpoint (six of eight in the active group vs. one of five in the control group). No difference was observed for complete regrowth. p-Values were not mentioned. Characteristics of the selected studied group were not described, but 4 of the 13 patients had alopecia totalis/alopecia universalis. Improvement in psychometric scores was noted in both groups and, therefore, would not be directly related to taking paroxetine.
In the study by Perini et al. [16], patients who received imipramine 75 mg once a day for 6 months showed a significantly higher percentage of “any regrowth” compared with the placebo group (71 vs 0 %, p < 0.01), but when complete regrowth was assessed the difference disappeared (1/7 vs 0/6). Only cases with less than 6 months disease duration were selected, including 7/14 with alopecia universalis. Improvement in psychiatric symptomatology was observed in both groups.
3.2.3 Conclusion
No complete regrowth has been related to the use of antidepressants. When the end point of “any regrowth” was used, both the administration of imipramine and of paroxetine resulted in some hair regrowth as compared with the placebo-treated groups.
3.3 Biologics
3.3.1 Rationale for Use in Alopecia Areata
Biologics are molecular engineered drugs designed to block the inflammatory cascade at very specific points. In case reports, improvement of alopecia areata with biologics such as alefacept and efalizumab has been described [17–19]. On the other hand, recurrence of alopecia areata in patients receiving biologics such as etanercept, adalimumab, and infliximab for other reasons has been published [20–22].
3.3.2 Randomized Controlled Studies
Two double-blind, randomized, placebo-controlled trials have studied formerly available biologics, efalizumab and alefacept, in alopecia areata. Efalizumab is a recombinant humanized monoclonal antibody that binds to the CD11a subunit of lymphocyte function-associated antigen 1 and acts as an immunosuppressant by inhibiting lymphocyte activation and cell migration out of blood vessels into tissues. Alefacept interferes with lymphocyte activation by specifically binding to the lymphocyte antigen, CD2, and inhibiting the interaction between CD2 and its ligand, LFA-3. Administration of alefacept 15 mg intramuscularly once a week did not decrease the Severity of Alopecia Tool (SALT) score, nor did it induce regrowth of at least 50 % in patients with extensive patchy alopecia areata, when compared with placebo [23]. Administration of efalizumab was also not found to be effective or statistically significantly superior at inducing hair regrowth greater than 75 % when 1 mg/kg was injected subcutaneously once a week in patients with greater than 50 % hair loss when compared with placebo in this double-blind trial [24].
3.3.3 Conclusions
Double-blind, randomized, placebo-controlled trials with either efalizumab or alefacept failed to show regrowth of at least 50 % in patients with extensive patchy alopecia areata.
3.4 Calcineurin Inhibitors
3.4.1 Rationale for Use in Alopecia Areata
Calcineurin inhibitors are immunosuppressive drugs that inhibit the activation and maturation of T cells and block the transcriptional activation of several lymphokine genes. Effects of systemic cyclosporin in alopecia areata led to the idea that topical calcineurin inhibitors could induce some local immunosuppression with fewer side effects. Currently available topical formulations include tacrolimus and pimecrolimus. In the past, topical cyclosporin has also been studied.
3.4.2 Randomized Controlled Study
Only one randomized controlled trial has compared pimecrolimus 1 % with clobetasol propionate 0.05 % and placebo in patch-type alopecia areata [25]. Application of pimecrolimus 1 % cream was not found to be statistically different from clobetasol propionate 0.05 % cream or placebo when hair regrowth was evaluated.
3.4.3 Conclusion
Pimecrolimus 1 % was not better than clobetasol propionate 0.05 % or placebo for the treatment of non-extensive patchy alopecia areata.
3.5 Corticosteroids (Systemic)
3.5.1 Rationale for Use in Alopecia Areata
Corticosteroids are anti-inflammatory drugs that can be used systemically, intralesionally, or topically. In alopecia areata, they are thought to affect peribulbar lymphocytes, thereby allowing follicles to enter a normal hair cycle. Since 1952, many non-controlled studies of different systemic corticosteroid regimens have shown them to be effective in alopecia areata [26]. Regrowth greater than 75 % may occur in 16–88 % of patients, perhaps depending on disease extent and duration [27].
3.5.2 Randomized Controlled Study
Only one randomized controlled trial was found using the search methods described on the use of systemic corticosteroids in alopecia areata [28]. Administration of oral pulse prednisolone 200 mg once a week for 3 months was found to induce regrowth greater than 30 % in 8 of 20 (40 %) patients treated with the active drug in comparison with none of 16 (0 %) in the placebo group. The statistical significance of results for greater regrowth area or follow-up time were not mentioned, but seemed to be equally important (regrowth >60 % in 3 months was 10 vs. 0 %; regrowth >30 % in 6 months was 20 vs. 6 %). Only patients with greater than 40 % hair loss or more than ten patches were included. Favorable prognostic factors were early age of onset, duration of disease less than 2 years, and first episode; poor prognostic factors were presence of atopy, nail involvement, multiple episodes, and a prolonged duration (more than 2 years). Short-term side effects were seen in 55 % of patients receiving prednisolone and included general weakness, acneiform eruption, weight gain, gastrointestinal upset, moon facies, and oligomenorrhea.
3.5.3 Conclusion
The only randomized controlled trial published confirms data from previous non-controlled trials of the efficacy of systemic corticosteroids in alopecia areata. Results vary according to disease duration and extent, and long-term side effect profiles need to be taken into consideration when treatment is given over a prolonged period.
3.6 Corticosteroids (Topical)
3.6.1 Rationale for Use in Alopecia Areata
As mentioned in Sect. 3.5, in alopecia areata, corticosteroids are thought to decrease inflammation around the bulb region, thereby allowing follicles to enter a normal hair cycle. Topical formulations have the advantage of fewer side effects than oral formulations, and different vehicles may be used (solutions, lotions, foam, creams, and ointments), with direct influence on drug penetration and perhaps patient compliance.
3.6.2 Randomized Controlled Studies
Five randomized controlled trials have investigated topical corticosteroids in alopecia areata, three of which are double blind and placebo controlled (one with desoximetasone and two with clobetasol propionate). In the two others, different corticosteroid compounds were tested (betamethasone valerate foam [BVF] vs. betamethasone dipropionate lotion [BDL] and clobetasol 0.05 % cream vs. hydrocortisone 1 % cream) [25, 29–32].
In the study by Charuwichitratana et al. [29], at least 25 % regrowth was seen in 25 of 26 patients applying 0.25 % desoximetasone cream twice a day but in only 21 of 28 (75 %) of the placebo group (p ≤ 0.05). Analysis was not conducted on an intention-to-treat basis and 16 of the 70 patients initially enrolled withdrew. No statistical difference was found between groups for patients with good response (>75 % regrowth) due to the great number of complete responses in both groups (14/26 with active vs. 11/28 with placebo). Only patients with patchy alopecia areata were included.
Clobetasol propionate 0.05 % foam applied 5 days per week was found to be better than placebo in inducing regrowth greater than 25 % in patients with moderate to severe alopecia areata (42 % for clobetasol propionate 0.05 % foam vs. 13 % for placebo, p = 0.027) by Tosti et al. [30]. Regrowth >50 % also seemed more frequent in the treated group (20 % active vs. 3 % placebo), but a p-value was not mentioned. No statistical difference was found for patients with good response (>75 % regrowth) due to the small number in both groups (1/34 clobetasol vs. 0/34 placebo; p-value not mentioned) [30].
In a third study, when clobetasol propionate 0.05 % cream was compared with pimecrolimus 1 % cream and placebo in patients with patchy alopecia areata, no statistical difference in percentage recovery and recovery score was found among the groups in the study completed by Ucak et al. [25].
In the fourth study, which was investigator blinded, two different corticosteroid preparations—BVF and BDL—were studied in patchy alopecia areata. A greater percentage of regrowth >75 % was found with the foam formulation (61 % BVF vs. 27 % BDL, p < 0.03) [31].
The fifth study compared clobetasol propionate 0.05 % cream and hydrocortisone 1 % cream in children who had at least 10 % scalp hair loss. After two cycles of 6 weeks on and 6 weeks off medication (total of 24 weeks), a greater percentage of patients in the clobetasol group demonstrated at least a 50 % reduction in scalp surface hair loss (85 % with clobetasol vs. 33.3 % with hydrocortisone, p < 0.001) [32].
3.6.3 Conclusions
In two double-blind, randomized, placebo-controlled trials, regrowth of at least 25 % with the use of highly potent topical corticosteroids was observed. Regrowth of more than 75 % was not demonstrated to be related to the drugs. In one randomized, double-blind, placebo-controlled trial, clobetasol propionate was found to be no better than placebo. In these studies, both patchy and moderate to severe disease were studied. Also, BVF was statistically better than BDL in inducing significant regrowth in patients with patchy alopecia areata, and clobetasol propionate 0.05 % cream was better than hydrocortisone 1 % cream in reducing the extent of hair loss area in children with alopecia areata.
3.7 Minoxidil
3.7.1 Rationale for Use in Alopecia Areata
The effect of minoxidil in hair growth was first noticed in the 1980s when prominent hypertrichosis was found in almost every patient using it as a vasodilating antihypertensive drug. The exact mechanism by which it increases anagen is not known, but is thought to be related to an effect on calcium channels.
3.7.2 Randomized Controlled Studies
Eight randomized controlled trials investigated minoxidil in alopecia areata, only one of which was not double blind. Four of the studies demonstrate positive results, while the other four had negative results.
3.7.2.1 Positive Results (Four Studies)
Fenton and Wilkinson [33] reported cosmetically acceptable regrowth in 58 % of patients treated with minoxidil 1 % (0.5 mL solution or 0.5 g ointment) versus only 5 % treated with placebo (p-value not mentioned). Significant p-values were found for “any regrowth” at 3 months (73 % active vs. 7 % placebo) and 6 months (81 % active vs. 5 % placebo) [33].
In another randomized placebo-controlled trial, Shi [34] showed statistical significance for cosmetically acceptable regrowth with minoxidil 1 % cream applied once a day, but neither investigator nor patients were blinded, and most of the participants (41/54) presented with their first episode of alopecia areata.
In the study by Olsen et al. [35], maintenance or gain of new hair was observed with minoxidil 2 % in 86 % of patients who had previously responded to a 6-week taper of prednisone, compared with only 17 % who received placebo. Patients who had not responded to prednisone did not show any benefit from using topical minoxidil. Intention to treat was not considered in the analysis.
Similar to the study by Olsen et al. [35], Chowdury et al. [36] also compared minoxidil 2 % versus placebo thrice a day after a 6-week course of tapered oral prednisolone; however, the comparison between minoxidil and placebo groups did not take into account differences in previous response to prednisolone among groups.
3.7.2.2 Negative Results (Four Studies)
White and Friedmann [37] randomized a group of 15 patients with alopecia totalis to receive either minoxidil 3 % twice a day or placebo. No significant regrowth of terminal hairs occurred in any group after 16 weeks of active treatment.
In a 4-month study by Vestey and Savin [38], 50 patients applied minoxidil 1 % once a day. No difference in results for “any regrowth” or cosmetically acceptable response, compared with placebo, was seen.
No difference was found in cosmetically acceptable regrowth in a group of patients studied by Fransway and Muller [39]. Patients with extensive alopecia areata (>65 % scalp involvement) applied minoxidil 3 % lotion 0.5 mL twice a day, and results were compared with a placebo-treated group. This 1-year study of alopecia areata is one of the longest topical minoxidil studies in the literature.
The trial published by Shapiro et al. [12] studied whether minoxidil 5 % solution twice a day would add any benefit to diphenylcyclopropenone in the treatment of alopecia areata patients with more than 50 % scalp involvement. Regrowth of at least 75 % was considered the primary endpoint. No statistically significant difference was found between the topical minoxidil- and placebo-treated groups in this half-head study—half of the scalp of each patient was used as a control (no treatment) to exclude the possibility of spontaneous regrowth.
3.7.3 Conclusions
Eight trials have been conducted with topical minoxidil of different concentrations and study design in alopecia areata. Four studies had negative results. Positive results were found in studies in which patients had already responded to oral corticosteroids, if “any regrowth” was the primary endpoint and when the first episode of the disease was part of the study design.
3.8 Prostaglandins
3.8.1 Rationale for Use in Alopecia Areata
Prostaglandins in ophthalmic solutions are traditionally used to treat open-angle glaucoma and were incidentally found to increase eyelash length as a side effect in 77 % of patients [40]. Laboratory studies in vitro and in animal models have also shown the stimulatory effects of prostaglandin analogs on hair growth through the influence of prostaglandin F2alpha and its analogs [41]. Furthermore, in a non-blinded, non-randomized, controlled eyelash alopecia areata study with latanoprost ophthalmic solution in 40 patients for 2 years, 45 % of patients showed cosmetically acceptable eyelash regrowth [42].
3.8.2 Randomized Controlled Studies
Two randomized controlled trials have been conducted on prostaglandins in alopecia areata: one in eyelash alopecia areata and the other in eyebrow alopecia areata.
Roseborough et al. [43] observed no eyelash improvement after 4 months of topical application of either latanoprost or bimatoprost in 11 patients who completed an investigator-blinded, randomized, side-controlled study. Eyelash regrowth was assessed by direct measurement of eyelash length and by digital photographs [43]. In another study, by Ross et al. [44], severe eyebrow alopecia areata (>50 % bilaterally) did not respond to topical latanoprost 3 µg once a day in any of the eight patients who completed a 3-month study period. Investigators were blinded in this study, and the contra-lateral eye was not treated and therefore served as a control site.
3.8.3 Conclusions
Prostaglandins have not been shown to be effective in the treatment of eyelash or eyebrow alopecia areata. However, different concentrations, application frequency, vehicle, and duration of treatment need to be studied in future trials.
3.9 Sensitizers
3.9.1 Rationale for Use in Alopecia Areata
Sensitizers have the capacity of inducing an allergic contact dermatitis. In 1986, Happle et al. [45] proposed the theory of immunomodulation and showed that topical sensitizers could change the peribulbar CD4/CD8 lymphocyte ratio and that this was associated with hair growth.
3.9.2 Randomized Controlled Studies
Two randomized controlled trials have involved sensitizers, one with dinitrochlorobenzene (DNCB) and one with diphenylcyclopropenone (DPCP).
Topical DPCP was studied in a bilateral non-blinded comparison study that also assessed the efficacy of topical minoxidil [12]. A total of 13 patients with extensive disease completed the protocol; five patients (38 %) experienced regrowth of more than 75 % on the treated side. Of note, the number of non-treated sides that also improved was not mentioned nor was the p-value for the difference. Only patients with more than 50 % scalp involvement were included.
DNCB-induced allergic contact dermatitis was compared with croton oil induced-irritant dermatitis in the management of alopecia areata in a study by Swanson et al. [46]. A clear benefit of DNCB over croton oil was seen, with regrowth greater than 75 % in 7 of 11 patients treated with DNCB in contrast with none of seven (0 %) of those treated with croton oil (p = 0.0069). Only patients with extensive disease were included in this study; 13 of 25 had alopecia totalis/alopecia universalis.
3.9.3 Conclusions
Two randomized controlled trials showed that sensitizers (DNCB and DPCP) can induce regrowth of at least 75 % in patients with severe alopecia areata. Of note, DNCB is not commonly used at the present time because of its potential mutagenicity.
3.10 Miscellaneous Systemic Treatments
3.10.1 Rationale for Use in Alopecia Areata
Inosiplex (Isoprinosine) is an immunomodulating agent that augments cell-mediated immunity. Total glucosides of paeony capsule (TGPC) are Chinese herbal extracts with a reported immunoregulatory action that inhibits activation of T lymphocytes by dendritic cells.
3.10.2 Randomized Controlled Studies
We found one randomized controlled trial for each of the above immunoregulators, inosiplex, and TGPC.
Administration of inosiplex 50 mg/kg/day in five divided doses for 3 months induced regrowth greater than 50 % in 13 of 16 patients (81 %), while only 4 of 14 placebo-treated patients experienced the same regrowth (29 %), p < 0.01, with significance maintained after an intention-to-treat analysis. Complete regrowth with inosiplex also appeared to be better than with placebo (31 vs. 0 %), but a p-value was not mentioned. Most patients presented with patchy alopecia areata, and results were not specified according to disease extent [47].
Administration of TGPC was compared with compound glycyrrhizin tablets, a common alternative therapy used in China to treat alopecia areata. Only cases with hair loss greater than 50 % were included in this double-blind study. Regrowth of at least 70 % was used as the primary endpoint, and no significant difference was found (p = 0.281) between these two treatment modalities [48]. Because glycyrrhizin tablets were considered an effective treatment for alopecia areata by the authors, this result would mean TGPC is equally effective.
3.10.3 Conclusions
The results of the inosiplex study in a group of 32 alopecia areata patients, most with patchy disease longer than 1 year duration, are encouraging. The use of TGPC was shown to be equal to glycyrrhizin tablets, neither of which are currently scientifically proven to be effective in alopecia areata.
3.11 Miscellaneous Topical Treatments
3.11.1 Rationale for Use in Alopecia Areata
A variety of topical treatments have been tried in alopecia areata, including aromatherapy, garlic, photodynamic therapy (PDT), azelaic acid, bexarotene, and triiodothyronine. Aromatherapy and garlic are claimed to have hair growth-promoting properties. PDT could preferentially destroy activated lymphocytes around hair bulbs [49]. The irritant dermatitis induced by azelaic acid could also be beneficial in the management of alopecia areata lesions. Bexarotene is a retinoid X receptor agonist that induces T-cell apoptosis [50]. Thyroid hormone receptors are expressed on hair follicles, and thyroid hormone is known to have an effect on the hair cycle and hair growth [51].
3.11.2 Randomized Controlled Studies
One randomized controlled trial on each of these topical treatments was found: aromatherapy, azelaic acid, garlic gel, PDT, bexarotene, and triiodothyronine. Positive results were found with aromatherapy, azelaic acid, and garlic gel combined with betamethasone valerate cream.
3.11.2.1 Positive Results
In a randomized trial of aromatherapy, regrowth was seen more frequently with aromatherapy (44 % vs. 15 % for essential oils, p = 0.008). Regrowth of greater than 80 % was observed in 6 of 43 patients in the active group, but in only 3 of 41 in the control group (p-value not mentioned). Extension and duration of the disease of the participants were not described. Age, associated conditions (atopy, thyroid disease), and family history were similar between groups [52].
In a separate study, azelaic acid 20 % cream was compared with anthralin 0.5 %, and no significant difference in cosmetically acceptable regrowth was noted (p > 0.05). Only patients with patchy alopecia areata were selected, and response rates were 53.3 % (8 of 15) in the azelaic acid group and 56.2 % (9 of 16) in the anthralin-treated group. Results were maintained even 8 weeks after discontinuation of therapy. Patients who had a complete response also had no new patches develop, suggesting to the investigators that there was possible control of the disease outside the treated area. Because anthralin is considered a useful irritant treatment in the management of alopecia areata, the authors considered these results as a proof of azelaic acid’s efficacy for the treatment of alopecia areata [14].
A combination of garlic gel and betamethasone valerate cream was compared with betamethasone valerate cream alone in a double-blind, randomized, placebo-controlled trial involving 40 patients with patchy alopecia areata of recent onset (less than 1 month). Primary endpoints of the study included mean patch size, number of hair fibers, and number of terminal hair fibers. After 3 months of therapy, the number of total and terminal hair fibers in the group treated with garlic was significantly higher than those of the control group; and the size of the patches significantly decreased in the active group [53].
3.11.2.2 Negative Results
Topical PDT with 5-aminolevulinic acid once a week did not induce hair regrowth in any of six patients with extensive alopecia areata (>75 % of scalp). Three different concentrations of 5-aminolevulinic acid and vehicle alone were tested, each in a quarter of the affected scalp. A phototoxic effect of PDT was achieved in all cases [54].
In an investigator-blinded, placebo-controlled study of topical bexarotene 1 % gel, treatment was found not to be any better than “no treatment” for alopecia areata. Patients with both patchy disease (34 patients) and alopecia totalis/alopecia universalis (three/five patients) were included [55].
Topical triiodothyronine ointment was tested and found to be no more effective than placebo in the management of ten patients with patchy alopecia areata (p > 0.05). Comparison was made between two patches in the same patient randomly assigned to either treatment or placebo [56].
3.11.3 Conclusions
PDT, bexarotene, and triiodothyronine as used in the above studies were not effective in the treatment of alopecia areata. Azelaic acid was shown to be equally effective as anthralin in patchy alopecia areata, but both may not be particularly effective. Both aromatherapy and the combination of garlic and betamethasone valerate cream were shown to induce some hair growth as compared with a placebo-treated group of alopecia areata patients.
4 Summary
No drug is currently approved by the US FDA for the treatment of alopecia areata. At the present time, many therapies are available and treatment choices are frequently based on disease extent, duration, activity, and age of the patient. As shown in this review, there exist relatively few published randomized controlled trials, and the majority of the studies are only of moderate quality as assessed by the authors using the American College of Physicians (ACP) guideline grading system (Table 2) [57].
Although a number of treatments were found to be effective using the ACP criteria, for example, topical and oral corticosteroids and the sensitizing agents DPCP and DNCB, major limitations in most of the studies include either a very small number of participants, significant disease heterogeneity in study design, or lack of follow-up to be able to document sustainability of a positive clinical response. To help better design future studies, in 1999 and 2004 the Alopecia Areata Investigational Assessment Guidelines were published, and when used, provide some standardization to the description of disease extent and percent improvement in response to therapy [58, 59]. These guidelines are now commonly being implemented into alopecia areata clinical trials. Further research using these guidelines and more appropriately powered studies should greatly improve the confidence in the estimate of an effect of a particular approach to treatment.
References
Messenger A. Management of alopecia areata. In: UpToDate, Basow DS (ed), UpToDate, Waltham, MA. Accessed 11 March 2014.
Hordinsky M. Treatment of alopecia areata. What is new on the horizon? Dermatol Ther. 2011;24:364–8.
Delmere FM, Sladden MJ, Dobbins HM, et al. Interventions for alopecia areata. Cochrane Database Syst Rev. 2008;(2):CDO04413.
Malhotra AK, Khaitan BK, Sethuraman G, Sharma VK. Betamethasone oral mini-pulse therapy compared with topical triamcinolone acetonide (0.1%) paste in oral lichen planus: a randomized comparative study. J Am Acad Dermatol. 2008;58(4):596–602.
Yosefy C, Ronnen M, Edelstein D. Pseudo alopecia areata caused by skull-caps with metal pin fasteners used by Orthodox Jews in Israel. Clin Dev Immunol. 2003;10(2–4):193–5.
Duvic M, Lemak NA, Valero V, Hymes SR, Farmer KL, Hortobagyi GN, Trancik RJ, Bandstra BA, Compton LD. A randomized trial of minoxidil in chemotherapy-induced alopecia. J Am Acad Dermatol. 1996;35(1):74–8.
Olsen EA. Topical minoxidil in the treatment of androgenetic alopecia in women. Cutis. 1991;48(3):243–8.
Khoury EL, Price VH, Abdel-Salam MM, Stern M, Greenspan JS. Topical minoxidil in alopecia areata: no effect on the perifollicular lymphoid infiltration. J Invest Dermatol. 1992;99(1):40–7.
Warin AP. Dinitrochlorbenzene in alopecia areata. Lancet. 1979;1(8122):927.
Kurosawa M, Nakagawa S, Mizuashi M, Sasaki Y, Kawamura M, Saito M, Aiba S. A comparison of the efficacy, relapse rate and side effects among three modalities of systemic corticosteroid therapy for alopecia areata. Dermatology. 2006;212(4):361–5.
Shapiro J, Tan J, Ho V, Tron V. Treatment of severe alopecia areata with topical diphenylcyclopropenone and 5% minoxidil: a clinical and immunopathologic evaluation. J Invest Dermatol. 1995;104(5 Suppl):36S.
Shapiro J, Tan J, Ho V, Abbott F, Tron V. Treatment of chronic severe alopecia areata with topical diphenylcyclopropenone and 5% minoxidil: a clinical and immunopathologic evaluation. J Am Acad Dermatol. 1993;29(5 Pt 1):729–35.
Fiedler-Weiss VC, Buys CM. Evaluation of anthralin in the treatment of alopecia areata. Arch Dermatol. 1987;123:1491.
Sasmaz S, Arican O. Comparison of azelaic acid and anthralin for the therapy of patchy alopecia areata: a pilot study. Am J Clin Dermatol. 2005;6(6):403–6.
Cipriani R, Perini GI, Rampinelli S. Paroxetine in alopecia areata. Int J Dermatol. 2001;40(9):600–1.
Perini G, Zara M, Cipriani R, Carraro C, Preti A, Gava F, Coghi P, Peserico A. Imipramine in alopecia areata. A double-blind, placebo-controlled study. Psychother Psychosom. 1994;61(3–4):195–8.
Heffernan MP, Hurley MY, Martin KS, Smith DI, Anadkat MJ. Alefacept for alopecia areata. Arch Dermatol. 2005;141(12):1513–6.
Bui K, Polisetty S, Gilchrist H, Jackson SM, Frederic J. Successful treatment of alopecia universalis with alefacept: a case report and review of the literature. Cutis. 2008;81(5):431–4.
Kaelin U, Hassan AS, Braathen LR, Yawalkar N. Treatment of alopecia areata partim universalis with efalizumab. J Am Acad Dermatol. 2006;55(3):529–32.
Posten W, Swan J. Recurrence of alopecia areata in a patient receiving etanercept injections. Arch Dermatol. 2005;141(6):759–60.
Kirshen C, Kanigsberg N. Alopecia areata following adalimumab. J Cutan Med Surg. 2009;13(1):48–50.
Tosti A, Pazzaglia M, Starace M, Bellavista S, Vincenzi C, Tonelli G. Alopecia areata during treatment with biologic agents. Arch Dermatol. 2006;142(12):1653–4.
Strober BE, Menon K, McMichael A, Hordinsky M, Krueger G, Panko J, Siu K, Lustgarten JL, Ross EK, Shapiro J. Alefacept for severe alopecia areata: a randomized, double-blind, placebo-controlled study. Arch Dermatol. 2009;145(11):1262–6.
Price VH, Hordinsky MK, Olsen EA, Roberts JL, Siegfried EC, Rafal ES, Korman NJ, Altrabulsi B, Leung HM, Garovoy MR, Caro I, Whiting DA. Subcutaneous efalizumab is not effective in the treatment of alopecia areata. J Am Acad Dermatol. 2008;58(3):395–402.
Ucak H, Kandi B, Cicek D, Halisdemir N, Derthogul SB. The comparison of treatment with clobetasol propionate 0.05% and topical pimecrolimus 1% in the treatment of alopecia areata. J Dermatol Treat. 2012;23(6):410–20.
Dillaha CJ, Rothman S. Treatment of alopecia areata totalis and universalis with cortisone acetate. J Invest Dermatol. 1952;18(1):5–6.
Nakajima T, Inui S, Itami S. Pulse corticosteroid therapy for alopecia areata: study of 139 patients. Dermatology. 2007;215(4):320–4.
Kar BR, Handa S, Dogra S, Kumar B. Placebo-controlled oral pulse prednisolone therapy in alopecia areata. J Am Acad Dermatol. 2005;52(2):287–90.
Charuwichitratana S, Wattanakrai P, Tanrattanakorn S. Randomized double-blind placebo-controlled trial in the treatment of alopecia areata with 0.25% desoximetasone cream. Arch Dermatol. 2000;136(10):1276–7.
Tosti A, Iorizzo M, Botta GL, Milani M. Efficacy and safety of a new clobetasol propionate 0.05% foam in alopecia areata: a randomized, double-blind placebo-controlled trial. J Eur Acad Dermatol Venereol. 2006;20(10):1243–7.
Mancuso G, Balducci A, Casadio C, Farina P, Staffa M, Valenti L, Milani M. Efficacy of betamethasone valerate foam formulation in comparison with betamethasone dipropionate lotion in the treatment of mild-to-moderate alopecia areata: a multicenter, prospective, randomized, controlled, investigator-blinded trial. Int J Dermatol. 2003;42(7):572–5.
Lenane P, Macarthur C, Parkin PC, Krafchik B, DeGroot J, Khambalia A, Pope E. Clobetasol propionate, 0.05%, vs hydrocortisone, 1%, for alopecia areata in children: a randomized clinical trial. JAMA Dermatol. 2014;150(1):47–50.
Fenton DA, Wilkinson JD. Topical minoxidil in the treatment of alopecia areata. Br Med J (Clin Res Ed). 1983;287(6398):1015–7.
Shi YP. Topical minoxidil in the treatment of alopecia areata and male-pattern alopecia. Arch Dermatol. 1986;122(5):506.
Olsen EA, Carson SC, Turney EA. Systemic steroids with or without 2% topical minoxidil in the treatment of alopecia areata. Arch Dermatol. 1992;128(11):1467–73.
Chowdury MM, Rahman MH, Wahab MA. Efficacy of combination therapy for the management regime of alopecia areata. Mymensingh Med J. 2007;16(2 Suppl):S19–22.
White SI, Friedmann PS. Topical minoxidil lacks efficacy in alopecia areata. Arch Dermatol. 1985;121(5):591.
Vestey JP, Savin JA. A trial of 1% minoxidil used topically for severe alopecia areata. Acta Derm Venereol. 1986;66(2):179–80.
Fransway AF, Muller SA. 3 percent topical minoxidil compared with placebo for the treatment of chronic severe alopecia areata. Cutis. 1988;41(6):431–5.
Demitsu T, Manabe M, Harima N, Sugiyama T, Yoneda K, Yamada N. Hypertrichosis induced by latanoprost. J Am Acad Dermatol. 2001;44(4):721–3.
Sasaki S, Hozumi Y, Kondo S. Influence of prostaglandin F2alpha and its analogues on hair regrowth and follicular melanogenesis in a murine model. Exp Dermatol. 2005;14:323–8.
Coronel-Pérez IM, Rodríguez-Rey EM, Camacho-Martínez FM. Latanoprost in the treatment of eyelash alopecia in alopecia areata universalis. J Eur Acad Dermatol Venereol. 2010;24(4):481–5.
Roseborough I, Lee H, Chwalek J, Stamper RL, Price VH. Lack of efficacy of topical latanoprost and bimatoprost ophthalmic solutions in promoting eyelash growth in patients with alopecia areata. J Am Acad Dermatol. 2009;60(4):705–6.
Ross EK, Bolduc C, Lui H, Shapiro J. Lack of efficacy of topical latanoprost in the treatment of eyebrow alopecia areata. J Am Acad Dermatol. 2005;53(6):1095–6.
Happle R, Klein HM, Macher E. Topical immunotherapy changes the composition of the peribulbar infiltrate in alopecia areata. Arch Dermatol Res. 1986;278(3):214–8.
Swanson NA, Mitchell AJ, Leahy MS, Headington JT, Diaz LA. Topical treatment of alopecia areata. Arch Dermatol. 1981;117(7):384–7.
Georgala S, Katoulis AC, Befon A, Georgala K, Stavropoulos PG. Inosiplex for treatment of alopecia areata: a randomized placebo-controlled study. Acta Derm Venereol. 2006;86(5):422–4.
Yang DQ, You LP, Song PH, Zhang LX, Bai YP. A randomized controlled trial comparing total glucosides of paeony capsule and compound glycyrrhizin tablet for alopecia areata. Chin J Integr Med. 2012;18(8):621–5.
Hryhorenko EA, Rittenhouse-Diakun K, Harvey NS, Morgan J, Stewart CC, Oseroff AR. Characterization of endogenous protoporphyrin IX induced by delta-aminolevulinic acid in resting and activated peripheral blood lymphocytes by four-color flow cytometry. Photochem Photobiol. 1998;67(5):565–72.
Zhang C, Hazarika P, Ni X, Weidner DA, Duvic M. Induction of apoptosis by bexarotene in cutaneous T-cell lymphoma cells: relevance to mechanism of therapeutic action. Clin Cancer Res. 2002;8(5):1234–40.
Ahsan MK, Urano Y, Kato S, Oura H, Arase S. Immunohistochemical localization of thyroid hormone nuclear receptors in human hair follicles and in vitro effect of L-triiodothyronine on cultured cells of hair follicles and skin. J Med Invest. 1998;44(3–4):179–84.
Hay IC, Jamieson M, Ormerod AD. Randomized trial of aromatherapy. Successful treatment for alopecia areata. Arch Dermatol. 1998;134(11):1349–52.
Hajheydari Z, Jamshidi M, Akbari J, Mohammadpour R. Combination of topical garlic gel and betamethasone valerate cream in the treatment of localized alopecia areata: a double-blind randomized controlled study. Indian J Dermatol Venereol Leprol. 2007;73(1):29–32.
Bissonnette R, Shapiro J, Zeng H, McLean DI, Lui H. Topical photodynamic therapy with 5-aminolaevulinic acid does not induce hair regrowth in patients with extensive alopecia areata. Br J Dermatol. 2000;143(5):1032–5.
Talpur R, Vu J, Bassett R, Stevens V, Duvic M. Phase I/II randomized bilateral half-head comparison of topical bexarotene 1% gel for alopecia areata. J Am Acad Dermatol. 2009;61(4):592.e1-9.
Nasiri S, Haghpanah V, Taheri E, Heshmat R, Larijani B, Saeedi M. Hair regrowth with topical triiodothyronine ointment in patients with alopecia areata: a double-blind, randomized pilot clinical trial of efficacy. J Eur Acad Dermatol Venereol. 2012;26(5):654–6.
Qaseem A, Snow V, Douglas K, Owens DK, Shekelle P. The development of clinical practice guidelines and guidance statements of the American College of Physicians: summary of methods. Ann Intern Med. 2010;153(3):194–9.
Olsen E, Hordinsky M, McDonald-Hull S, Price VH, Roberts JL, Shapiro J. Alopecia areata investigational assessment guidelines: National Alopecia Areata Foundation. J Am Acad Dermatol. 1999;40(2 Pt 1):242–6.
Olsen EA, Hordinsky M, Price VH, Roberts JL, Shapiro J, Canfield D, Duvic M, King LE, McMichael AJ, Randall VA, Turner ML, Sperling L, Whiting DA, Norris. Alopecia areata investigational assessment guidelines—Part II. J Am Acad Dermatol. 2004;51(3):440–7.
Acknowledgments
No sources of funding were used to prepare this review.
Maria Hordinsky, MD, and Aline Donati, MD have no conflicts of interest that are directly relevant to the content of this review.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Hordinsky, M., Donati, A. Alopecia Areata: An Evidence-Based Treatment Update. Am J Clin Dermatol 15, 231–246 (2014). https://doi.org/10.1007/s40257-014-0086-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40257-014-0086-4