
Abstract
Introduction
Diabetes mellitus is a global public health emergency in the twenty-first century. Diabetes patients who had to adhere to good self-care recommendation can prevent the complication associated with diabetes mellitus. Self-care management of diabetes mellitus in Sub-Saharan Africa was poor including Ethiopia. The aim of this study was to assess factors influencing diabetes self-care practice among type 2 diabetes patients at Debre Tabor General Hospital, Northwest Ethiopia diabetes clinic follow up unit.
Methods
An institutional based cross-sectional survey was conducted on systematically sampled 405 type 2 diabetes patients at Debre Tabor General Hospital diabetes clinic from June 02/2018 to June 30/2018. Bivariate and multivariable logistic regression was fitted to identify independent predictors of diabetes self-care practice. A p value of less than 0.05 was used to declare statistical significance.
Results
A total of 385 type 2 diabetes patients participated with a response rate of 95%, of which 243 (63.1%) study participants had good self-care practice. The mean ± SD age of the respondents and the duration of diagnosed for diabetes mellitus was 52.28 ± 12.45 and 5.09 ± 3.80 years respectively. Type 2 diabetes patients who had a glucometer at home (AOR = 7.82 CI (3.24, 18.87)), getting a diabetes education (AOR = 2.65 CI (1.44, 4.89)), and having social support (AOR = 2.72 CI (1.66, 4.47)) were statistically associated with good self-care practice.
Conclusion
Despite, the importance of diabetes self-care practice for the management of diabetes and preventing its complications, a significant number of type 2 diabetes patients had poor diabetes self-care practice. So, to enhance this poor practice of diabetes self-care, provision of diabetes self-care education and counseling on self-monitoring blood glucose should be promote by health care providers during their follow up.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Diabetes mellitus is a global public health emergency in the twenty-first century [1]. Globally, the number of people with diabetes (20–79 years) was 425 million in 2017 and it will be predicted to 629 million by 2045. From this Africa accounts 16 million adults have diabetes in 2017 and will be predicted 41 million by the year 2045 [2]. According to IDF diabetics atlas eighth edition, approximately 4 million people aged between 20 and 79 years died from diabetes that equivalent to one death in every eight seconds [2]. Globally, it is estimated that 212.4 million diabetes cases are undiagnosed, among this 84.5% of cases are in low and middle-income countries [2]. Type 2 diabetes mellitus accounts 90–95% among all the cases of diabetes mellitus [3]. The prevalence of type 2 diabetes mellitus was increasing in sub-Saharan Africa due to rapid urbanization and lifestyle changes [4]. Ethiopia ranks third by the prevalence of diabetes mellitus in the Africa region [3].
As far as diabetes mellitus is a chronic medical illness that requires lifelong medical care, continuing patient self-management and requires multifactorial risk reduction strategies beyond glycemic control [5]. Self-management of diabetes mellitus in Sub-Saharan Africa was poor and therefore a serious threat to the health of individuals in the health system [6]. Different studies showed that poor adherence to recommended self-care practice in Ethiopia [7,8,9,10,11].
There are seven essential self-care behaviors in people with diabetes which predict good self-care outcomes. These are healthy eating, being physically active, self-monitoring of blood glucose, compliant with medications, good problem-solving skills, healthy coping skills and risk-reduction behaviors [12,13,14]. Different studies evidenced that a lot of determinant factors for diabetes self-care practice, which is diabetes education, duration of disease, presence of another disease besides diabetes, regular checking of blood sugar, overweight, physical inactivity, dietary factors, foot care, and Smoking are the most significant factor for type 2 diabetes mellitus [15,16,17,18].
Evidence showed that 98% of diabetes treatment depend on havening good self-care behaviors and patients with diabetes adhere to self-care can prevent the complications associated with diabetes mellitus (retinopathy, nephropathy, neuropathy, and cardiovascular disease), which take over mostly by patients and their families [19]. Lifestyle management is a central aspect of diabetes care and that includes diabetes self-management support, diabetes self-management education, physical activity, smoking cessation counseling and psychosocial care, and the ultimate prerequisite for diabetes self-management patient education [20]. However, self-care practice highly recommended for diabetes patients [21], in Ethiopia, there is still a low practice of diabetes self-care behavior. Furthermore, there are limited studies conducted to address the issue of diabetes self-care practice and its associated factors in the study area. In Ethiopia, there is no diabetes self-care recommendation guideline and there is lack of information on the proper self-care practice for people with T2DM. Moreover, because of the paucity of evidence-based research, the health policy of Ethiopia, is still unable to give attention to this diabetes self-care practice recommendation. Conducting and documenting such kind of research would have a positive influence on the designing and implementation of diabetes self-care practice recommendation for people with T2DM in Ethiopian clinicians, policymakers, and health planners.
The aim of this study was to assess factors influencing diabetes self-care practice among type 2 diabetes patients at Debre Tabor General Hospital, Northwest Ethiopia diabetes clinic follow up unit.
Methods
Study design, period and settings
An institution based cross-sectional study was conducted at Debre Tabor General Hospital diabetes clinic from June 02/2018 to June 30/2018. Debre Tabor General Hospital is found in Debre Tabor Town, South Gondar Zone of Amhara Regional state which is 667 km far from Addis Ababa the capital city of Ethiopia in Northwest direction and 102 km far from Bahir Dar town the capital city of Amhara Regional State.
Study participants
All Type 2 diabetes (T2DM) patients aged >18 years who had diabetes follow up from Debre Tabor General Hospital for at least 12 months were included in the study whereas, newly diagnosed type 2 diabetes patients, severely ill, unable to hear and/or speak and having mental disorder among type 2 diabetes patients were excluded from the study.
A total of 405 study participants were included for the study by using single population proportion formula, considering that the prevalence of good self-care practice of 60.3% from a previous study [11] with assumptions of 95% CI, 5% margin of error and by adding of 10% nor response rate. Systematic random sampling technique was employed to select the study participants. A total of 920 type 2 diabetes patients were registered per month for diabetes follow up then we calculated the Kth interval that was 2. So, we interview the study participants every 2 T2DM patients.
Data quality control technique
The data were collected by two trained nurses and supervised by one public health officer. The data were collected by face to face interview and Patient chart review. The structured questionnaire first prepared in English then translated to the local language (Amharic) again translated back to English to check consistency. Training was given for data collectors and supervisors. The questionnaire was pretested of 5% of the sample size before the actual data collection period. The internal reliability of the tool (SDSCA) was evaluated with a Cronbach alpha value of 0.78 which is tested on 30 individual patients.
Data collection tools
The data collection tool for this study was used after adaptation of from previous validated studies. The structured questionnaire has two major parts for the interview. Part one: Socio-demographic characteristics and other associated factors. Part two: The revised scale of Summary of Diabetes Self-Care Activities Measure (SDSCA) was used for diabetes self-care practice measurement [22]. The revised scale of SDSCA contains fifteen items which are to measure the adherence of diabetes self-care practice. The response is based on the seven-point Likert scale to answer the question phrased as “On how many of the last SEVEN DAYS have/did you …?” (Table 2), and diabetic related knowledge was assessed by after adaptation of Revised brief Diabetes Knowledge Test (DKT2) validated by the University of Michigan scholars [23].
Operational definitions
Good self-care practice
The overall score of the mean number of days ≥4 days per week from the total self-care practice measurement items were considered as good self-care practice [22, 24].
Poor self-care practice
The overall score of the mean number of days less than 4 days per week from total self-care practice measurement items were considered as poor self-care practice [22, 24].
Revised brief Diabetes Knowledge Test (DKT2) questionnaire has 23-item multiple choice questions which have three up to four choices with only one correct answer. Item 1–14 designed for all adult diabetes patients and item 15–23 for only insulin-dependent diabetes patients. The DKT2 was recorded as zero for incorrect response and one for a correct response. Patients answering greater than seven correct answers were declared as having good diabetic related knowledge.
Good controlled blood glucose level was defined as an average of three consecutive fasting blood glucose (FBS) measurement of 80–130 mg/dl. Poor controlled blood glucose was defined as patients who had average blood glucose measurements on three consecutive visits >130 or < 70 mg/dl [21, 25].
Data processing and analysis
The collected data first has been rechecked manually for its completeness and consistency. The data were entered into EpiData version 3.1. The entered data were exported in to with Statistical Package for Social Science (SPSS) version 24 software for windows for analysis. Descriptive statistics was employed for the socio-demographic and clinical characteristics of the respondents. Bivariate logistic regression was performed for each independent variable with the outcome variable. A variable whose bivariate test had a p value <0.20 was considered as a candidate for the multivariable logistic regression model. Hosmer and Lemeshow’s goodness-of-fit test was used to check the data appropriateness for the multivariable logistic regression model. Finally, by backward LR variable selection method, a multivariable logistic regression model was fitted to determine the independent predictors of diabetes self-care practice. Crude Odds Ratio (COR), Adjusted Odds Ratio (AOR) with 95%CI were computed to determine the associated factor of type 2 diabetic patient self-care practice and P- value less or 0.05 was considered as declared statically significant.
Ethical consideration
The study was conducted after getting an ethical clearance letter from Debre Tabor University College of Health Sciences and collected after obtaining permission from Debre Tabor General Hospital. Informed consent was secured from each study participants and personal identifiers were excluded during the data collection to assure confidentiality. Respondents can withdraw at any time from the interview.
Results
Socio-demographic characteristics of the respondents
A total of 385 Type 2 diabetes (T2DM) patients participated in the study a response rate of 95%. From the total of respondents, 202 (52.5%) were males and 164 (42.6%) were unable to read and write. The mean ± SD age of the respondents was 52.28 ± 12.45 years, and 182 (47.3%) were in the age group of 41–59 years. Most of (70.4%) the study participants have no family history of T2DM and majority (58.7%) of the respondents were urban in residence (Table 1).
Self-care practice adherence and clinical characteristics of the study participants
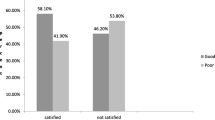
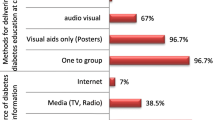
Overall, 243 (63.1%) study participants had good self-care practice among type 2 diabetes patients. The self-care practice was different among different recommendations. The highest mean score was found “On how many of the last SEVEN DAYS, did you take your recommended diabetes medication?” and the lowest mean score found “On how many of the last SEVEN DAYS did you test your blood sugar? And On how many of the last SEVEN DAYS did you test your blood sugar the number of times recommended by your health care provider?”, which is on self-monitoring blood glucose domain (Table 2). The mean ± SD duration of diagnosed for diabetes mellitus was 5.09 ± 3.80 years. The mean ± SD Fasting Blood Sugar (FBS) was 173.31 ± 69.97 mg/dl. Most of 326 (84.7%) of study participants got a diabetes education during their follow from the health professionals, and 81 (21%) of study participants had a glucometer at home for self-monitoring blood glucose level. Only 121 (31.4%) of type 2 diabetes patients had good glycemic control, and 128 (33.2%) of patients had good diabetes-related knowledge (Table 3).
Factors associated with self-care practice among type 2 diabetes patients
In bivariate logistic regression residence, educational status, occupation, having their own glucometer at home for self-monitoring blood glucose, having diabetes education, having social support, glycemic control level, and diabetes-related knowledge was significantly associated with type 2 diabetes patient self-care practice.
In multivariable logistic regression type 2 diabetes patients who had a glucometer at home for self-monitor blood glucose, having diabetes education, and having social support were significantly associated with diabetes self-care practice among type 2 diabetes patients. Type 2 diabetes patients who were having their own glucometer at home for self- monitoring blood glucose 7.82 times more likely had good self-care practice than type 2 diabetes patients who had not their own glucometer at home (AOR = 7.82 CI (3.24, 18.87)). Type 2 diabetes patients who had a diabetes education from health professionals during their follow up 2.65 times more likely to had good self-care practice than type 2 diabetes patients who had not diabetes education (AOR = 2.65 CI (1.44, 4.89)). Type 2 diabetes patients who had social support 2.72 times more likely had good self-care practice than those who had no social support (AOR = 2.72 CI (1.66, 4.47)) (Table 4).
Discussion
Worldwide, the prevalence of chronic, non-communicable diseases is increasing at an alarming rate, and diabetes mellitus is becoming a major public health chronic, non-communicable diseases [26]. The global prevalence and impact of diabetes mellitus had increased dramatically, particularly in sub-Saharan Africa due to the most rapid urbanization and lifestyle changes [4, 27]. Achieving good self-care recommendations such as dietary practice, pharmacotherapy, physical activity, blood glucose monitoring, and foot care is the central part to decreases morbidity and mortality related to diabetes and its complications [19, 28, 29].
This study revealed that 63.1% of type 2 diabetes patients adhered to good self-care recommendations practice which is consistent with the study done at India (52–70%), and Addis Ababa (60.3%) [11, 30,31,32], whereas it is higher than the study done Tigray region (39.3%), Nekemte, West Ethiopia (45%), Bahir Dar, Ethiopia (28.4%), and Iran (36.4%) [24, 33,34,35]. The possible justification of this variation might be socio-economic status and time of the study. In contrast to the finding of our study, higher good self-care practice was reported from Dilla University Referral Hospital, South Ethiopia (76.8%) [36]. The possible variation of this result might socio-demographic characteristics which is most of the respondents come from a rural area in our study, lack of self-glucose monitoring machine, and level of information education, and communications from the health professionals.
This study evidenced that having a glucometer at home for self-monitoring blood glucose was significantly associated with good self-care practice. Type 2 diabetes patients who had a glucometer at home 7.82 times more likely adhere to good self-care practice than type 2 diabetes patients who had not glucometer for self-monitoring blood glucose. This finding was similar to the study done at Tigray region [24], Iran [35], but this finding is not similar to the study done at Jimma, Southwest Ethiopia [9]. This might be type 2 diabetes patients having a glucometer at home could know the update of their blood glucose level this may be led to patients to had good self-care practice accordingly their blood glucose level.
Having diabetes education was significantly associated with good diabetes self-care practice. Type 2 diabetes patients those who got a diabetes education from health professionals 2.65 times more likely had good self-care practice than those who did not get a diabetes education from health professionals, which is similarly finding a study done at Addis Ababa Public Hospitals [11], and Tigray region [24]. The possible reason may be got a diabetes education from health professionals enhance self-care related knowledge and self-care management.
Furthermore, this study evidenced that having social support from their relatives/peers were significantly associated with self-care practice. Type 2 diabetes patients who had social support were 2.72 times more likely had good self-care practice than those who had no social support. This is similar with the evidence from Addis Ababa Public Hospitals [11], a report from the role of self-care [37], Bahir Dar, Northwest Ethiopia [34], a review of self-management in Africa [38], and Filipino Americans [39]. This determinant factor may enhance a potential impact on medication adherence, dietary adherence, and other self-care recommendations due to social advice and other supports.
Strength and limitation of the study
Since there are no similar studies in the study area it will be baseline information for health planners and further studies. As far as a self-reported interview question and the data collector were nurses it may prone to social desirability bias. As well, the study was a cross-sectional study the temporal relationship cannot always determined.
Conclusion and recommendations
Even though, adhering to good self-care practice recommendations were an invaluable issue to prevent type 2 diabetes morbidity and mortality, the result of this study evidenced that a significant number of type 2 diabetes patients had poor self-care practice. Therefore, strategies like having a glucometer at home, getting diabetes education, and social support could improve diabetes self-care practice among type 2 diabetes patients. So, health care professionals should encourage diabetes education and promote counseling on self-monitoring blood glucose during their follow up emphasized on diabetes self-care practice recommendations.
Data availability
We, all the authors do have the data of this study and we can provide as per the request.
References
IDF diabetes atlas: Seventh edition. International Diabetes Federation. 2015;144. http://www.diabetesatlas.org
International Diabetes Federation (IDF). Eighth edition 2017. IDF Diabetes Atlas, 8th edition. 2017;1–150
Peer N, Kengne AP, Motala AA, Mbanya JC. Diabetes in the Africa region: an update. Diabetes Res Clin Pract. 2014;103(2):197–205.
Assah F, Mbanya JC. Diabetes in sub-saharan Africa. Diabetes Mellit Dev Ctries Underserved Commun. 2016;375(9733):33–48.
Association AD. Standards of medical care in diabetes - 2013. Diabetes Care. 2013;36(SUPPL.1).
Stephani V, Opoku D, Beran D. Self-management of diabetes in sub-Saharan Africa: a systematic review. BMC Public Health. 2018;18:1148.
Ayub M, Ayub S, Masood F, Afzal A, Shafique M, Ullain N. Diabetes & metabolism evaluation of predisposing and Comorbodities associated with diabetes. Diabetes Metab. 2015;6(8):10–2.
Mariam TG, Alemayehu A, Tesfaye E, Mequannt W, Temesgen K, Yetwale F, et al. Prevalence of diabetic foot ulcer and associated factors among adult diabetic patients who attend the diabetic follow-up clinic at the University of Gondar referral hospital, north West Ethiopia, 2016: institutional-based cross-sectional study. J Diabetes Res. 2017;2017(11):4219–29.
Kassahun T, Gesesew H, Mwanri L, Eshetie T. Diabetes related knowledge, self-care behaviours and adherence to medications among diabetic patients in Southwest Ethiopia: a cross-sectional survey. BMC Endocr Disord. 2016;16(1):28.
Asegid A. Assessment of self care practice among adult diabetic patients in Nigist Elleni Mohamed memorial hospital Hossana. J Med Heal Res. 2017;2(1):26–35.
Mamo M, Demissie M. Self care practice and its associated factors among diabetic patients in Addis Ababa public hospitals , cross sectional study. J Diabetes Cholest Metab. 2016;1(Dcm):1–5.
Soediono B. American Association of Diabetes Educators (AADE) position statement. J Chem Inf Model. 1989;53(December):160.
Hill-Briggs F, Gemmell L. Problem solving in diabetes self-management and control. Diabetes Educ. 2007;33(6):1032–50.
Fisher EB, Thorpe CT, McEvoy DeVellis B, DeVellis RF. Healthy coping, negative emotions, and diabetes management. Diabetes Educ. 2007;33(6):1080–103.
Chen L, Magliano DJ, Zimmet PZ. The worldwide epidemiology of type 2 diabetes mellitus—present and future perspectives. Nat Rev Endocrinol. 2011;8(4):228–36.
Istek N, Karakurt P. Effect of activities of daily living on self-Care Agency in Individuals with type 2 diabetes. J Diabetes Mellit. 2016;06(04):247–62.
Weeks CE. Factors influencing self care behaviors of African Americans adults with type 2 diabetes. 2011;1–40.
Mogre V, Abanga ZO, Tzelepis F, Johnson NA, Paul C. Adherence to and factors associated with self-care behaviours in type 2 diabetes patients in Ghana. BMC Endocr Disord. 2017;17(1):1–8.
Toljamo M, Hentinen M. Adherence to self-care and glycaemic control among people with insulin-dependent diabetes mellitus. J Adv Nurs. 2001;34(6):780–6.
Pocius S, Miley K, Rockwood J. Accuracy and timeliness of RN vs. MD radiological interpretation of PICC tips. JAVA - J Assoc Vasc Access. 2009;14(3):143–6.
American Diabetes Association (ADA). Standard of medical care in diabetes - 2017. Diabetes Care. 2017;40(sup 1):s4–s128.
Toobert DJ, Hampson SE, Glasgow RE. The summary of diabetes self-care activities measure. Diabetes Care J. 2000;23(7):943–50.
Fitzgerald JT, Funnell MM, Anderson RM, Nwankwo R, Stansfield RB, Piatt GA. Validation of the revised brief diabetes knowledge test (DKT2). Diabetes Educ. 2016;42(2):178–87.
Mariye T, Tasew H, Teklay G, Gerensea H, Daba W. Magnitude of diabetes self-care practice and associated factors among type two adult diabetic patients following at public hospitals in central zone, Tigray region, Ethiopia, 2017. BMC Res Notes 2018;11(1):1–6, 380.
Yigazu DM, Desse TA. Glycemic control and associated factors among type 2 diabetic patients at Shanan gibe hospital, Southwest Ethiopia. BMC Res Notes. 2017;10(1):1–6.
Tabish SA. Is diabetes becoming the biggest epidemic of the twenty-first century? Int J Health Sci (Qassim). 2007;1(2):V–VIII.
Pastakia SD, Pekny CR, Manyara SM, Fischer L. Diabetes in sub-Saharan Africa - from policy to practice to progress: targeting the existing gaps for future care for diabetes. Diabetes Metab Syndr Obes: Targets Ther. 2017;10:247–63.
Shrivastava SR, Shrivastava PS, Ramasamy J. Role of self-care in management of diabetes mellitus. J Diabetes Metab Disord. 2013;12(1):1.
England TN, Prevention D, Group DPPR. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. Engl J. 2002;346(6):393–403.
Raithatha SJ, Shankar SU, Dinesh K. Self-care practices among diabetic patients in Anand District of Gujarat. ISRN Fam Med. 2014;2014(December 2009):1–6.
Basu S, Garg S, Sharma N, Singh MM, Garg S. Adherence to self-care practices, glycemic status and influencing factors in diabetes patients in a tertiary care hospital in Delhi. World J Diabetes. 2018;9(5):72–9.
Basu S, Khobragade M, Kumar A, Raut DK. Medical adherence and its predictors in diabetes mellitus patients attending government hospitals in the Indian capital, Delhi, 2013: a cross sectional study. Int J Diabetes Dev Ctries. 2015;35:95–101.
Amente T, Teferea B, Endalew H, Berhanu N. Self-care practice and its predictors among adults with diabetes mellitus on follow up at Nekemte hospital diabetes clinic, West Ethiopia. World J Med Med Sci. 2014;2(3):1–16.
Abate TW, Tareke M, Tirfie M. Self-care practices and associated factors among diabetes patients attending the outpatient department in Bahir Dar, Northwest Ethiopia. BMC Res Notes. 2018;11(1):800.
Nejaddadgar N, Solhi M, Jegarghosheh S, Abolfathi M, Ashtarian H. Self-care and related factors in patients with type 2 diabetes. Asian J Biomed Pharm Sci. 2017;7(61):6–10.
Endalew Hailu AE. Assessment of diabetic patient perception on diabetic disease and self-care practice in Dilla University Referral Hospital, South Ethiopia. J Metab Syndr. 2014;03(04):4–11.
Shrivastava SB, Shrivastava PS, Ramasamy J. Role of self-care in management of diabetes mellitus. J Diabetes Metab Disord. 2013;12(14):1–5.
Iregbu S, Iregbu FU. A review of self-management of diabetes in Africa. African J Diabetes Med [Internet] 2016;24(2):5–8. Available from: http://search.ebscohost.com/login.aspx?direct=true&db=a9h&AN=120428063&site=ehost-live.
Sonsona JB. Factors influencing diabetes self-Management of Filipino Americans with type 2 diabetes mellitus : a holistic approach. Walden dissertations and doctoral studies collection. 2014.
Acknowledgments
We, authors, express their deep gratitude to all the study participants, data collectors and staff of Debre Tabor General Hospital for their cooperation.
Funding statement
We didn’t receive any fund for this study.
Author information
Authors and Affiliations
Contributions
All stated authors SA, AA, YK, HG, BA, MT, AD, are involved in the study from the inception to design, acquisition of data, analysis and interpretation and drafting of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Consent for publication
Not applicable.
Competing interests
We, authors, declare that we had no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Tiruneh, S.A., Ayele, A.A., Emiru, Y.K. et al. Factors influencing diabetes self-care practice among type 2 diabetes patients attending diabetic care follow up at an Ethiopian General Hospital, 2018. J Diabetes Metab Disord 18, 199–206 (2019). https://doi.org/10.1007/s40200-019-00408-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40200-019-00408-z