
Abstract
Purpose of Review
Our aims are to explore the evidence for egg consumption effects on cardiovascular disease risk factors and the relationship between egg consumption with risk of coronary heart disease, stroke, heart failure, hypertension, and also to briefly discuss cardiovascular implications of egg consumption in individuals with diabetes and chronic kidney disease. Additionally, we provide a framework for health professionals when counseling patients on egg consumption as it relates to cardiovascular disease risk, and highlight areas where evidence is inconclusive and in need of future investigation.
Recent Findings
The relationship between egg consumption and cardiovascular diseases remains an area of significant debate among health professionals, as historically, eggs have been seen as potentially harmful if consumed frequently. The majority of existing evidence supports that assertion that moderate egg consumption of up to one egg per day in otherwise healthy individuals is not associated with a higher risk of ASCVD. In fact, eggs are a nutritious staple food that can be consumed in moderation in healthy individuals.
Summary
Diet is all about balance. Moderate egg consumption, i.e., up to one egg per day, is not associated with a higher risk of cardiovascular diseases. Besides, eggs are an affordable food with a high content of many important nutrients.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Eggs are a popular dietary component in the general population. The USDA reports that per capita consumption of eggs peaked in the 1940s and steadily declined until the early 1990s and consumption has now increased over the past three decades [1]. Indeed, US citizens are estimated to have consumed 245 eggs per person in 2011. This increase in egg consumption has been hypothesized to be due to changes in the health perceptions of eggs, as well as increased use of processed eggs and their derived products over the past few decades [2].
According to the USDA, one large egg contains approximately 5 g of fat, 2/3 of which is unsaturated; 187 mg of cholesterol; 147 mg of choline; and 6 g of high-quality protein, along with iron, vitamins, minerals, and carotenoids. Historically, healthcare and nutrition professionals have advised individuals to limit the consumption of eggs given the relatively high amounts of cholesterol per egg [3] and the potential association with increased risk of atherosclerotic cardiovascular disease (ASCVD). However, the relationship between increased egg and dietary cholesterol intake with ASCVD risk remains a topic a great debate in nutrition [4]. Interestingly, the 2015 edition of Dietary Guidelines for Americans no longer contains the recommendation to limit daily dietary cholesterol intake to 300 mg. However, the guidelines do suggest that individuals should limit cholesterol intake whenever possible in the context of an overall healthy diet [5]. Similarly, although current guidelines from the American Heart Association (AHA) and American College of Cardiology (ACC) do include specific recommendations to reduce dietary cholesterol, the specific amount are not specified [6, 7].
Egg consumption and ASCVD risk associations are considerably debated, and evidence linking the two have been mixed [8, 9]. This observed heterogeneity has a number of possible explanations. For one, it is important to consider that an individual’s response to dietary cholesterol consumption can vary significantly. Prior studies have demonstrated hypo- and hyper-responders to dietary cholesterol consumption and possible genetic variations in lipid metabolism [10,11,12,13]. Additionally, multiple potential mechanisms have been proposed to link egg consumption to ASCVD. Serum cholesterol effects have been the most studied mechanism; however, other potential mechanistic links such as trimethylamine N-oxide (TMAO) levels, increased LDL oxidation, endothelial dysfunction, and vascular inflammation have also been proposed [14,15,16,17,18]. Furthermore, observed differences in clinical outcomes may vary geographically with differences in socioeconomic, nutritional, and health status, as well as difference in egg consumption habits [19]. Thus, although a significant number of systematic reviews and meta-analyses have shown no higher risk of ASCVD with egg consumption or dietary cholesterol, these various results must be interpreted carefully. In this state-of-the-art review, our aim is to provide a critical appraisal of the available literature regarding egg consumption and ASCVD risk and clarify these associations. Figure 1 summarizes egg consumption and cardiovascular health.

Central illustration: egg consumption effects on cardiovascular health
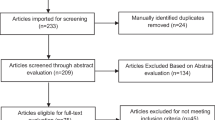
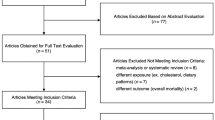
Methodology
In this critical review, we extensively searched PubMed for studies pertaining to egg consumption and cardiovascular disease within the past 15 years for consideration of inclusion. We searched using keywords such as “egg,” “egg consumption,” “cardiovascular,” “disease,” “atherosclerosis,” “stroke,” “hypertension,” coronary artery disease,” “ischemic heart disease,” “acute myocardial infarct,” “acute coronary syndrome,” “stroke,” “heart failure,” “cardiac failure,” and “mortality.” We only included studies that were observational, prospective cohorts, randomized controlled trial, or case control design. Animal studies were not included. Additionally, epidemiologic studies that did not directly observe egg consumption and cardiovascular outcomes were not included.
Current Dietary Cholesterol Guidelines and Recommendations
As the principle concern for egg consumption relates to dietary cholesterol intake, the following guidelines are briefly reviewed. Historically, dietary cholesterol recommendations have been explicitly mentioned in multiple scientific and nutritional society guidelines; however, in recent years, these recommendations have become generally less stringent. For example, the 2013 AHA/ACC guidelines for lifestyle changes to reduce ASCVD risk do not provide a specific directive on dietary cholesterol. The authors concluded that there is insufficient evidence to support that increased dietary cholesterol increases low-density lipoprotein cholesterol (LDL-C) levels in the blood [20].
Additionally, the 2015 edition of the Dietary Guidelines for Americans no longer contains the recommendation to limit daily dietary cholesterol intake to 300 mg; however, the authors do suggest that individuals should limit cholesterol intake when possible [5]. Ultimately, the guidelines emphasize an overall heart-healthy eating pattern rich in plant foods which tends to lower overall dietary cholesterol intake anyway.
The most recent 2019 ACC/AHA guidelines on the Primary Prevention of Cardiovascular Disease emphasize an overall healthy diet including vegetables, fruits, nuts, whole grains, lean protein, and fish and to limit dietary fat intake [6]. The guidelines also discuss the beneficial evidence for plant-based diets and recommend that reduced cholesterol and sodium intake may decrease the risk of ASCVD (class IIa evidence). Additionally, the 2018 Guideline on the Management of Blood Cholesterol make similar dietary recommendations and further advise LDL-lowering dietary interventions in individuals with various dyslipidemias [7].
Finally, the National Lipid Association Recommendations for Patient-Centered Management for Dyslipidemia advised that for individuals with elevated blood cholesterol levels, dietary cholesterol intake should be limited to 200 mg per day (i.e., the content of 1 egg) [21]. The authors also note that there are those “hyper-responders” to dietary cholesterol intake and these individuals should also be limited to < 200 mg/day.
Egg Composition, Dietary Cholesterol, and Lipidemic Effects
Eggs are a nutrient-dense food with relatively high protein content. They are a significant potential source of trace elements and minerals (e.g., Ca, Fe, Mg, P, K, Na, and Zn), as well as important vitamins (e.g., vitamins A, D, B6, and B12; thiamin; riboflavin; and niacin) [22]. Certain bioactive ingredients in eggs may be anti-inflammatory and antimicrobial and have anti-oxidant effects [23]. Furthermore, eggs are affordable for most consumers with a current average ad price of around $1.12 per dozen of conventional shell eggs as of October 23, 2020 [24]. These factors together make eggs an interesting dietary component for many individuals. However, in one egg, the amount of cholesterol ranges from 187 to 227 mg on average [22]. This would suggest that one egg alone could exceed some national health organizations recommendations [21] for daily dietary cholesterol intake in certain at-risk individuals. Clearly, eggs are a significant source of dietary cholesterol; yet, egg consumption may not be associated with an increased risk of ASCVD outcomes.
It is well established that LDL-C elevation is associated with an increased risk of ASCVD. Whether or not and to what extent increased dietary cholesterol leads to an elevated LDL-C is an area of significant debate and has been evaluated in previous studies [25,26,27,28,29,30]. Some meta-analyses have shown that increased dietary cholesterol does modestly increase total blood cholesterol levels and LDL-C levels; however, other studies have shown conflicting results [4]. Of note, most cholesterol-containing food sources also contain significant amounts of saturated fats which can have a cholesterol-raising effect making such interpretation difficult. Thus, the specific relationship between egg consumption and various blood lipid parameters has been an area of ongoing investigation.
Multiple feeding studies have been conducted which examined the effects of egg consumption on various blood lipid parameters. In a recent scientific advisory from the American Heart Association, Carson et al. [4] performed a meta-regression analysis which included controlled feeding studies in order to analyze the effects of dietary cholesterol on blood lipid levels. Of the 11 studies included for analysis, 9 of them used eggs as the source of dietary cholesterol. The other two studies did not explicitly report the dietary cholesterol source. The authors found a positive association between dietary cholesterol intake and total cholesterol (TC) concentration with a change in dietary cholesterol of 300 mg/day correlating to an increase in total serum cholesterol of approximately 10 mg/dL as seen in prior feeding studies [31,32,33]. A positive trend remained after eliminating studies that had a very high dietary cholesterol intake protocol (> 1000 mg/day).
Rouhani et al. [34] performed a meta-analysis which included 28 randomized controlled trials that compared blood lipid levels in egg and non-egg consuming groups. The authors demonstrated a modest increase in TC (5.6 mg/dL), LDL (5.55 mg/dL), and HDL (2.13 mg/dL) cholesterol in egg consuming groups. There was no increase in the LDL to HDL or TC to HDL ratios which are also important CVD risk factors [35]. There was no increase in triglyceride levels with egg consumption. Recently, Khalighi Sikaroudi et al. [36] performed meta-analysis which included 66 clinical trials pertaining to egg consumption and various blood lipid component levels. Similarly, the authors found a positive associated increase in TC (9.12 mg/dL), LDL (7.39 mg/dL), and HDL (1.41 mg/dL). There was no significant effect seen with egg consumption and LDL to HDL ratio or triglycerides. It should be noted however that the heterogeneity among studies included in this meta-analysis was rather high.
It is important to note that when interpreting and analyzing randomized controlled trials involving egg consumption effects on blood lipid levels, other foods are often replaced by the eggs in the study design. Thus, increasing egg consumption necessarily implies reducing the intake of other dietary components which can be problematic when drawing clinical conclusions as dietary patterns can vary greatly [37]. Additionally, not all studies controlled for concomitant saturated fat intake which is important to take into consideration given the cholesterol-raising effects of saturated fat and the close relationship between dietary cholesterol and saturated fat sources. Thus, there is some evidence that egg consumption may have a modest effect on blood lipid parameters; however, this does not seem to translate to worse ASCVD outcomes.
Egg Consumption and Trimethylamine N-oxide: an Alternative Link to CVD
Mechanistically, cholesterol intake leading to atherosclerosis represents one potential explanation for increased ASCVD risk in egg consuming individuals. However, research has also emerged investigating another potential mechanism in ASCVD and egg consumption. Eggs contain relatively high amounts of choline which are converted to trimethylamine in the gastrointestinal tract by bacteria. Trimethylamine is ultimately converted to trimethylamine N-oxide (TMAO) in the liver. It has been suggested in both animal and human studies that increased TMAO levels are associated with an increased risk of adverse cardiovascular events [38••]. Given this potential association, recent studies have been conducted assessing the effects of egg consumption and TMAO levels as a possible mechanistic link to ASCVD.
In a randomized crossover study which included 20 overweight postmenopausal women, Zhu et al. [39] administered 2 whole eggs versus an equivalent yolk free substitute for 4 weeks each. The authors found that choline and betaine levels were significantly increased after the whole egg diet; however, TMAO levels did not increase. In a similar randomized crossover trial, Lemos et al. [40] administered either whole eggs or a choline supplement to 30 study participants. When comparing post-intervention data of the two groups, plasma TMAO levels were not significantly affected with either whole eggs or the choline supplement when compared to baseline levels. However, post- versus pre-intervention study design is notoriously problematic in nutritional studies [37]. This was again confirmed in a 14-week crossover study of 38 participants who were given no eggs followed by 1, 2, and 3 eggs/day for 4 weeks each. The investigators found that higher egg consumption was associated with increased HDL cholesterol, reduced LDL/HDL cholesterol ratio, and increased plasma choline [41]. Most importantly, there was no increase in TMAO concentrations with egg consumption.
Additionally, Messimer et al. [42] made a similar observation in a randomized crossover trial including 50 healthy adults who ate either oatmeal or 2 eggs for breakfast for 4 weeks. In the egg-consuming group, plasma choline levels were higher compared to baseline, but there was no increase in TMAO levels.
Finally, Rohrmann et al. [43] conducted an observational study which measured TMAO levels in 271 adults. The authors found that egg, meat, or fish consumption were not associated with increased TMAO concentrations. Interestingly, they did note a positive relationship between TMAO levels and milk and dairy food consumption.
Although TMAO may have important cardiovascular implications, egg consumption does not seem to have a significant short-term effect on TMAO levels based upon review of contemporary literature. As previously demonstrated, there is significant inter-individual variability in TMA/TMAO metabolism linking to dietary nutrients, and TMAO clearance seems to change over time [44]. It is also conceivable that the source and the form of choline may have potential impact in the ability for the microbes to increase TMA production, and whole foods containing choline may differ from oral supplementation of choline that is commonly used as dietary supplementation. Certainly, more robust clinical trials would be needed to clarify the potential relationship between TMAO and egg consumption.
Egg Consumption and Cardiovascular Disease Outcomes
Overall CVD Risk and Mortality Outcomes
Multiple studies evaluated the potential association between egg intake and CVD outcomes as well as mortality. Several studies delineate comorbidities and the specific types of cardiovascular disease (CVD), while others do not. Here we review relevant research on the topic to date (Table 1).
Qureshi et al. [45] evaluated the potential association of egg consumption and risk of overall ASCVD (stroke and CAD), and mortality. The study included a national cohort of 9734 adults. After adjusting for demographics, the authors found that participants did not have higher risk of overall ASCVD or all-cause mortality when comparing those who ate < 1 egg per week to those that ate > 6 eggs per week. Djousse and Gaziano [46] performed an observational study using 21 327 participants from the Physicians’ Health Study to evaluate egg consumption and ASCVD risk and mortality. In a multivariate Cox regression, the authors observed that egg consumption was not associated with incident MI or stroke. However, adjusted hazard ratios for mortality indicated higher mortality risk with higher egg consumption (HR of 1.23 in those who consumed at least 7 eggs per week) which was even stronger in those patients with diabetes (HR 2.0).
In 2011, Zazpe et al. [47] evaluated incident ASCVD risk in 14,185 individuals based upon egg consumption with a median 6-year follow-up. There was no association between egg consumption and ASCVD incidence. Similarly, in a prospective cohort study including 70,571 participants from two separate cohorts composed of men and women free of CVD (coronary heart disease (CHD), stroke, or HF) at baseline, Larsson et al. [48] reported no relationship between egg consumption and risk of myocardial infarction (MI) or stroke in either cohort. Additionally, in a large Mediterranean cohort study, Diez-Espino et al. [49] followed 7216 individuals considered to be at high risk of ASCVD at baseline. The investigators found no association between cardiovascular events and egg consumption.
Farvid et al. [50] conducted a large observational cohort study which analyzed association between various dietary protein intake and risk of all-cause, CVD, and cancer-related mortality. Higher egg consumption was associated with lower risk of all-cause mortality in this study. It is worth noting that the median in the highest quartile was 0.48 servings of eggs per day which is generally lower than high consuming groups used in most other studies involving egg consumption.
Nakamura et al. [51] conducted an observational cohort study of 4686 Japanese women which evaluated egg consumption association with age-adjusted total cholesterol, CVD risk, cancer-specific, and all-cause mortality. The lowest consuming group consumed eggs less than once per week and the highest group consumed two eggs or more per day. The authors found no increased risk of CVD-related mortality. There was however an increased total (HR 2.05) and cancer-related (3.20) mortality when comparing the highest to the lowest egg-consuming groups. Qin et al. [52] conducted a large cohort study in China from the Kadoorie Biobank registry and found that a moderate associated reduced risk of CVD was observed in moderate egg-consuming individuals (up to 1 egg per day).
A recent large prospective study, which included 29,615 participants from 6 different US cohorts, analyzed self-reported food intake over a 30-year period. The investigators demonstrated that for each additional 300 mg per day of cholesterol reported in the individuals’ diet, there was an associated higher risk of CVD incidence and all-cause mortality (adjusted HR of 1.17 and 1.18, respectively) [53]. Similarly, each additional half an egg per day that was consumed was associated with increased CVD incidence and all-cause mortality (adjusted HR of 1.06 and 1.08, respectively).
This was again observed by Dehghan et al. [54••] who conducted a study of 146,011 individuals from the Prospective Urban Rural Epidemiology (PURE) study. The authors excluded those with existing ASCVD and found that in those who consumed 7 eggs per week or more, there was no increased risk of blood lipid elevations, ASCVD, overall mortality, or the primary composite outcome which included mortality or major adverse cardiac events.
Xia PF et al. [63] conducted an observational study which included 37,121 subjects from the National Health and Nutrition Examination Survey 1999–2014 to explore the association between egg consumption and mortality from all-cause and heart disease. They did not find significant association between egg consumption and all-cause or heart disease mortality. However, there was a positive association between increased dietary cholesterol and all-cause mortality when levels reached 250 mg per day or more. An inverse association with all-cause mortality was seen in those consuming less than 250 mg of cholesterol per day. Finally, there was no association between heart-specific mortality and dietary cholesterol intake.
Finally, Drouin-Chartier et al. [64] recently conducted the largest cohort analysis on egg consumption and CVD in the USA. The authors statistically modeled the replacement of one whole egg per day by one serving per day of another food and found a higher risk of cardiovascular disease when eggs were replaced with processed red meat (hazard ratio 1.15, 95% confidence interval 1.05 to 1.27), unprocessed red meat (1.10, 1.02 to 1.18), or full fat milk (1.11, 1.03 to 1.20). Statistical model replacement of one whole egg per day with one daily serving of fish, poultry, legumes, nuts, whole or refined grains, potatoes, reduced fat milk, cheese, or yogurt was not associated with increased cardiovascular disease risk.
Overall, results should be interpreted carefully as the included cohorts used multiple types of dietary assessment tools which were not all the same. However, the investigators did harmonize data prior to analysis and overall data supports that higher egg consumption is not observed with higher cardiovascular disease risk.
A significant number of meta-analyses have been conducted on associations of egg consumption and CVD risk. In one meta-analysis, the investigators analyzed 8 different prospective cohort studies examining the potential dose-response association of egg consumption with ASCVD risk. The investigators demonstrated that there was no higher risk of CHD or stroke among those who consumed higher amounts of egg (up to one per day) compared with low consumers [55]. These findings are consistent with another meta-analysis published which also found a slight reduction in stroke risk in high egg-consuming individuals [56].
Another similar analysis included 7 prospective cohort studies which looked specifically at egg consumption with risk of ASCVD. Interestingly, the authors demonstrated a statistically significant lower risk of stroke in the high consuming group (approximately 1 egg per day) when compared to the low consumers (less than 2 eggs per week) with a summary relative risk estimate of 0.88 [57]. Furthermore, there was no significant association with risk of CHD. In individuals who consumed > 7 eggs per week, there was no increased risk of ischemic heart disease, and a statistically significant lower stroke risk was observed (HR 0.91).
Mazidi et al. [58] similarly performed a meta-analysis and systematic review of prospective data regarding egg consumption and associated with total mortality, CHD, and stroke mortality. The analysis included 10 prospective studies and 110,400 individuals. The authors found no increased risk of total or CHD-related mortality with egg consumption. Furthermore, there was an inverse relationship between egg consumption and stroke mortality.
Drouin-Chartier et al. [64] conducted a large recent meta-analysis of 28 studies which included 1,720,108 participants evaluating egg intake and ASCVD risk and found an inverse relationship restricted to the Asian cohort only. This finding provided novel insights on the explanations underlying this observed discrepancy in previous analysis.
Krittanawong et al. [60] also found similar results in their recent large meta-analysis and systematic review exploring the association between egg consumption and ASCVD. The authors included 23 studies including 1,415,839 participants. The authors specifically compared individuals consuming no or 1 egg/day to higher consuming individuals (i.e., more than one egg/day). There was no increased risk of cardiovascular events in the high consuming group. Furthermore, there was an associated decreased risk of coronary artery disease in the higher egg-consuming groups.
Finally, a very recent meta-analysis by Godos et al. [61] included almost 2 million participants from 39 different prospective studies pertaining to egg consumption and CVD risk or mortality including CHD, stroke, and heart failure (HF). The authors reported an inverse association with CVD incidence or mortality in higher consuming (up to 6 eggs per week) groups when compared to low consuming groups. There was no association with egg consumption and stroke specifically. With the exception of the stroke association, the authors note that the evidence strength of the associations observed was relatively low and ultimately future studies would be needed to clarify the association.
In general, most observational studies, including several meta-analyses, indicate that modest egg consumption is not associated with overall ASCVD risk in otherwise healthy individuals. Regarding mortality, CVD-related mortality does not seem to be positively associated with increased egg consumption.
Atherosclerosis and Coronary Heart Disease
A number of studies have looked at the potential association with egg consumption and coronary heart disease (CHD) or atherosclerosis specifically. Nakamura et al. [65] conducted a study with two separate cohorts with a total of 90,735 subjects. The follow-up duration varied from 7 to 11 years depending on which cohort was used. The researchers specifically aimed to evaluate the relationship between egg consumption with CHD risk. The study participants were categorized into 4 separate groups based upon egg consumption with < 1 day per week or never as the lowest consuming group and almost every day as the highest consuming group. The authors found that higher egg consumption to almost daily was not associated with a higher risk of CHD. The authors note that in patients with hypercholesterolemia, egg consumption was lower on average which suggest that participants may be avoiding eggs due to their higher cholesterol content.
Similarly, Haring et al. [66] conducted a prospective cohort study including 12,066 individuals and evaluated the effects of dietary protein consumption on total CHD risk. Eggs were included as part of subgroup analysis. The median follow-up in this study was 22 years. Food group analysis revealed that among others, egg consumption was not significantly associated with CHD risk. This was true for up to one serving of eggs per day.
In one unique study, Virtanen et al. [67] evaluated egg consumption in 1032 men which delineated between those with a ɛ4 allele in the apolipoprotein E gene (ApoE4) as well. The study analyzed incident CHD as well as carotid artery intima-media thickness. Overall, egg or dietary cholesterol intake was not associated with CHD risk in ApoE4 carriers or non-carriers.
In another observational study which assessed atherosclerotic burden in 382 subjects who consumed eggs, Chagas et al. [68] demonstrated a decreased in Friesinger score among individuals who consumed more eggs. The Friesinger index score is a measure of atherosclerotic coronary artery disease which scores the three main coronary arteries with a total range of 0–15 (15 being total occlusion of all three vessels). Each vessel is scored from 0 to 5 depending on percentage amount of stenosis seen (5 being total vessel occlusion) and are added together for a final score. This decreased Friesinger score association was present after multivariate analysis for demographic factors as well. Similarly, in a study which used a sub-cohort of 1429 subjects in the Northern Manhattan Study, Goldberg et al. [69] analyzed dietary habits and carotid artery media thickness (cIMT) in study participants. The investigators demonstrated an inverse relationship between cIMT and egg consumption, and for every additional egg consumed per week, the risk of plaque formation reduced by 11%. Virtanen et al. [67] also demonstrated no increased cIMT with egg consumption. This trend was again confirmed using coronary artery calcium (CAC) scores in 1848 subjects from the National Heart, Lung, and Blood Institute Family Heart Study by Robbins et al. [70]. There was no association with CAC scores and egg consumption after adjusting for multiple variables.
However, not all studies have been negative regarding egg consumption and atherosclerosis or CHD risk. In one of the largest studies of its kind, Choi et al. [71] conducted a cross-sectional study including 23,417 asymptomatic adults without CVD history. The authors developed a multivariable-adjusted CAC score ratio and analyzed the association with egg consumption using food frequency questionnaires at an initial health screening evaluation. The authors found a higher CAC score ratio in individuals consuming one egg per day.
In a large recent meta-analysis, Takagi et al. [62] analyzed 16 studies including 1,285,505 individuals to determine the association between egg consumption and CHD incidence and mortality. The authors found that there was an overall lower CHD incidence and mortality in individuals who consumed increasing amounts of eggs similar to the findings of Krittanawong et al. [60] mentioned previously.
Overall, there is increasing evidence that suggests egg consumption is not associated with increased risk of CHD. In healthy individuals, it seems that egg consumption alone does not significantly increase the risk of CHD and moderate egg consumption of up to once per day is acceptable.
Stroke
Given that stroke may be the initial presentation of ASCVD, a many number of studies have evaluated the potential association of stroke and egg consumption. Sauvaget et al. [72] mailed a self-administered questionnaire pertaining to animal product intake to participants of the Life Span Study in Japan. This study included 40,349 individuals with more than 16 years of follow-up period. Result of this study showed that eggs, dairy products, fish, and broiled fish were inversely associated with risk of stroke. The composite HR was 0.8 (95%CI).
Bernstein et al. [73] conducted a study including 117,933 participants of two prospective cohorts and demonstrated an increased stroke risk associated with red meat consumption. The authors then used statistical models to predict the effects of substituting various foods with red meat. The authors found no association or risk difference when red meat was substituted with eggs.
Similarly, Abdollahi et al. [74] conducted a prospective cohort study including 1950 men from the Kuopio Ischemic Heart Disease Risk Factor Study. The cohort also included a subset of participants with the apolipoprotein E (APOE) phenotype. Egg consumption was not associated with stroke regardless of APOE carrier status.
Most recently, in the large cohort study by Drouin-Chartier [64] mentioned previously, the authors found no association with risk among those who consumed at least one egg per day compared with those who consumed less than one egg per month (0.99, 0.81 to 1.22 for stroke)
Tang et al. [19] conducted a large meta-analysis of 24 prospective cohorts. Ultimately, there was no associated between egg consumption and risk of stroke when comparing the lowest and highest quartile consuming groups. A dose-response analysis demonstrated a J-shaped curve with egg consumption and stroke risk; however, results were not statistically significant. Interestingly, subgroup analysis revealed that egg consumption was associated with reduced risk of stroke in Asia; however, this was not observed in North American or European cohorts.
As mentioned previously, multiple meta-analyses [55,56,57,58, 61] have been conducted that explore the association between stroke risk and egg consumption. Largely, there has been no significant evidence that egg consumption increases stroke risk. In fact, a number of meta-analyses have shown a decrease in stroke risk [56,57,58] with increased egg consumption consistent with prior prospective observational data mentioned above. In otherwise healthy individuals, egg consumption is likely safe in moderate servings of up to one egg per day in regard to stroke risk, and there may even be a reduction in overall stroke risk in healthy individuals. This potential risk reduction should be investigated with future clinical trials.
Heart Failure
Little evidence regarding egg consumption and heart failure risk exists; however, here we discuss some important research which may suggest egg consumption confers an increased risk of heart failure and would be an important area of future investigation.
Djousse and Gaziano [75•] performed a second study using the cohort of individuals from the Physicians’ Health Study to investigate the association between egg consumption and HF risk. The average follow-up time was 20.4 years. The investigators found that in the group of individuals who consumed eggs at least 7 times a week or more, there was a higher risk of developing HF. Less frequent consumption of eggs (up to 6 times per week and less) did not have an associated increased risk of HF.
Similarly, Nettleton et al. [76] demonstrated in an observational cohort including 14,153 adults which administered food frequency questionnaires that in individuals who consumed eggs, there was a higher HF incidence association (HR 1.23). Larsson et al. [48] also observed an increased HF risk in men who consumed eggs at least once per day or more (RR 1.3). Finally, in the meta-analysis by Godos et al. [61] mentioned previously, the authors demonstrated that consuming one egg per day was associated with a higher HF risk when compared to non-consuming groups.
Existing data are limited and mostly observational which raises concerns for residual confounding bias. Overall, egg consumption may have important implications for individuals at risk for or who have HF, but this hypothesis must be investigated with additional studies before any specific recommendations are made with regard to egg consumption and HF.
ASCVD Risk in Individuals with Diabetes
Evidence on association between egg and diabetes is limited. Some studies have indicated that individuals with diabetes may have an increased CVD risk with increased egg consumption. In the subgroup analysis by Qureshi et al. [45], the authors found that among individuals with diabetes who ate more than 6 eggs per week, there was a significantly increased risk of CHD (RR 2.0).
As mentioned previously, Djousse and Gaziano [46] performed an observational study using participants from the Physicians’ Health Study. Interestingly, the mortality association with egg consumption that the authors demonstrated was significantly stronger in those patients with diabetes (HR 2.0). In contrast, Larsson et al. [48] did not find any increased association with egg consumption and ASCVD outcomes in individuals with diabetes.
Although the potential association with egg consumption and incident diabetes risk is beyond the scope of this review, we note that a recent large study by Drouin-Chartier et al. [59] was conducted to evaluate the association between the risk of developing type 2 diabetes (an important risk factor for ASCVD) and egg consumption. The study included an updated meta-analysis of the topic as well as a separate observation study including over 200,000 individuals from 3 large US prospective cohorts. The updated analysis included 16 cohort studies (589,559 subjects). The author’s individual cohort study did observe an increased risk of type 2 diabetes with egg consumption; however, the meta-analysis found no such association. Notably, there was an associated increased risk of developing type 2 diabetes and egg consumption in US studies specifically; however, this is likely explained by differences in lifestyle and dietary habits in this cohort. This was not seen among European or Asian studies.
As diabetes is an important independent risk factor for ASCVD, this may confound the observed association of increased ASCVD risk in these studies. Most evidence suggesting increased ASCVD risk from egg consumption in patients with diabetes is the result of secondary analysis and is largely observational and hypothesis-generating. Future clinical trials are needed to explore the effects of egg consumption in patients with diabetes.
Hypertension
The effects of egg consumption on blood pressure and hypertension (HTN) risk are mixed. MacDonald et al. [77] conducted a prospective cohort study which included 46,424 French women from the E3N cohort. HTN was a self-reported diagnosis and the authors found that increased egg and cholesterol intake was associated with higher rates of HTN. However, it is very difficult to attribute the specific effects of egg consumption given the study design and inclusion of multiple food groups.
An observational meta-analysis by Zhang et al. [78] included 10 prospective cohort studies (351,819 individuals) evaluated various food groups and associated HTN. In subgroup analysis, 3 studies specifically included egg consumption and the authors demonstrated that there was lower risk of HTN with higher egg consumption. Wang et al. [79] conducted a large meta-analysis including 8 RCTs which found that higher egg consumption (> 4 whole eggs/week) was not associated with differential effects on blood pressure or blood lipid levels when compared to lower consuming groups (< 4 eggs/week).
Finally, in a recent systematic review and meta-analysis by Kolahdouz-Mohammadi et al. [80] that included 15 randomized controlled trials which included 748 participants, there was no effect of egg consumption found on blood pressure. Although evidence is limited, there does not seem to be a significant link between HTN risk and egg consumption.
Limitations
There are several limitations which must be considered in our review. First, there is significant heterogeneity among epidemiologic studies which observe egg consumption and cardiovascular outcomes, and many confounders may be present including region, lifestyle factors, and comorbidities, and other uncontrolled eating habits and factors can cause inconsistencies in outcomes observed. Secondly, not all studies account for and control the various ways that eggs are prepared and consumed such as fried, boiled, or combined with other foods and this may introduce confounding effects. Finally, it is difficult to eliminate various other forms of bias such as self-recall bias, selection bias, and residual bias in observational and epidemiologic studies, so results must be evaluated carefully.
Future Directions
Future studies that evaluate egg consumption and CVD risk would be important to perform in certain groups of individuals. For example, more studies that explore the apparent discrepancy in egg consumption and CVD risk in international cohorts may help describe an observed reduction in stroke risk seen in some populations that are not seen in the USA [64]. There is also very limited observational evidence regarding egg consumption and heart failure risk or heart failure progression which is an area of ongoing interest and would be an important area of future research. Finally, chronic kidney disease (CKD) is an important risk factor for ASCVD; however, this has almost no data regarding egg consumption and CKD. Thus, studies which looked at dietary patterns and outcomes in these individuals would be an important area of future analysis.
Conclusions
In comparison to other reviews, our findings discuss and included the most current evidence to date regarding egg consumption and CVD, which includes 3 large meta-analyses on the topic within the past year. These most recent analyses as well as the majority of epidemiologic data observed to date provide evidence that moderate egg consumption of up to one egg per day in otherwise healthy individuals does not have an observed association with increased CVD risk. Diet is all about balance. Up to one egg per day seems safe and likely beneficial through its nutrient density. Overall, eggs are a nutritious stable food that can be consumed in moderation in healthy individuals.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Agriculture UDSA. How many eggs do Americans eat each year? https://ask.usda.gov/s/article/How-many-eggs-do-Americans-eat-each-year. Accessed 24 Oct 2020.
Huang X, Ahn DU. How can the value and use of egg yolk be increased? J Food Sci. Feb 2019;84(2):205–12. https://doi.org/10.1111/1750-3841.14430.
McNamara DJ. The fifty year rehabilitation of the egg. Nutrients. 2015;7(10):8716–22. https://doi.org/10.3390/nu7105429.
Carson JAS, Lichtenstein AH, Anderson CAM, et al. Dietary cholesterol and cardiovascular risk: a science advisory from the American Heart Association. Circulation. 2020;141(3):e39–53. https://doi.org/10.1161/cir.0000000000000743.
U.S. Department of Health and Human Services. 2015-2020 Dietary Guidelines for Americans. https://health.gov/our-work/food-nutrition/2015-2020-dietary-guidelines/guidelines/. Accessed 3/7/2021.
Arnett DK, Blumenthal RS, Albert MA, et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;140(11):e596–646. https://doi.org/10.1161/cir.0000000000000678.
Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;139(25):e1082–143. https://doi.org/10.1161/cir.0000000000000625.
Spence JD, Jenkins D. Cardiovascular benefit of egg consumption is most unlikely. Heart. Nov 2018;104(21):1805–6. https://doi.org/10.1136/heartjnl-2018-313687.
Chrysant SG, Chrysant GS. The debate over egg consumption and incident cardiovascular disease. Cardiol Rev. 2020. https://doi.org/10.1097/crd.0000000000000325.
Katan MB, Beynen AC, de Vries JH, Nobels A. Existence of consistent hypo- and hyperresponders to dietary cholesterol in man. Am J Epidemiol. Feb 1986;123(2):221–34. https://doi.org/10.1093/oxfordjournals.aje.a114231.
Beynen AC, Katan MB, Van Zutphen LF. Hypo- and hyperresponders: individual differences in the response of serum cholesterol concentration to changes in diet. Adv Lipid Res. 1987;22:115–71. https://doi.org/10.1016/b978-0-12-024922-0.50008-4.
Ordovas JM. The genetics of serum lipid responsiveness to dietary interventions. Proc Nutr Soc. 1999;58(1):171–87. https://doi.org/10.1079/pns19990023.
Ordovas JM, Schaefer EJ. Genetic determinants of plasma lipid response to dietary intervention: the role of the APOA1/C3/A4 gene cluster and the APOE gene. Br J Nutr. 2000;83(Suppl 1):S127–36. https://doi.org/10.1017/s0007114500001069.
Levy Y, Maor I, Presser D, Aviram M. Consumption of eggs with meals increases the susceptibility of human plasma and low-density lipoprotein to lipid peroxidation. Ann Nutr Metab. 1996;40(5):243–51. https://doi.org/10.1159/000177964.
Schwab US, Ausman LM, Vogel S, Li Z, Lammi-Keefe CJ, Goldin BR, et al. Dietary cholesterol increases the susceptibility of low density lipoprotein to oxidative modification. Atherosclerosis. 2000;149(1):83–90. https://doi.org/10.1016/s0021-9150(99)00310-x.
Terasaka N, Yu S, Yvan-Charvet L, Wang N, Mzhavia N, Langlois R, et al. ABCG1 and HDL protect against endothelial dysfunction in mice fed a high-cholesterol diet. J Clin Invest. 2008;118(11):3701–13. https://doi.org/10.1172/jci35470.
Vogel RA, Corretti MC, Plotnick GD. Effect of a single high-fat meal on endothelial function in healthy subjects. Am J Cardiol. 1997;79(3):350–4. https://doi.org/10.1016/s0002-9149(96)00760-6.
Njike V, Faridi Z, Dutta S, Gonzalez-Simon AL, Katz DL. Daily egg consumption in hyperlipidemic adults--effects on endothelial function and cardiovascular risk. Nutr J. 2010;9:28. https://doi.org/10.1186/1475-2891-9-28.
Tang H, Cao Y, Yang X, Zhang Y. Egg consumption and stroke risk: a systematic review and dose-response meta-analysis of prospective studies. Front Nutr. 2020;7:153. https://doi.org/10.3389/fnut.2020.00153.
Eckel RH, Jakicic JM, Ard JD, et al. 2013 AHA/ACC guideline on lifestyle management to reduce cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129(25 Suppl 2):S76–99. https://doi.org/10.1161/01.cir.0000437740.48606.d1.
Jacobson TA, Maki KC, Orringer CE, et al. National Lipid Association recommendations for patient-centered management of dyslipidemia: part 2. J Clin Lipidol. 2015;9(6 Suppl):S1-122.e1. https://doi.org/10.1016/j.jacl.2015.09.002.
U.S. Department of Agriculture. Food Data Central: eggs, grade A, large, egg whole. https://fdc.nal.usda.gov/fdc-app.html#/food-details/748967/nutrients. Accessed 3/7/2021.
Xiao N, Zhao Y, Yao Y, et al. Biological activities of egg yolk lipids: a review. J Agric Food Chem. 2020;68(7):1948–57. https://doi.org/10.1021/acs.jafc.9b06616.
U.S. Department of Agriculture. Egg markets overview: a weekly publication of the USDA AMS Livestock and Poultry Program, Agricultural Analytics Division. https://www.ams.usda.gov/sites/default/files/media/Egg%20Markets%20Overview.pdf. Accessed 24 Oct 2020.
Hopkins PN. Effects of dietary cholesterol on serum cholesterol: a meta-analysis and review. Am J Clin Nutr. 1992;55(6):1060–70. https://doi.org/10.1093/ajcn/55.6.1060.
Hegsted DM, Ausman LM, Johnson JA, Dallal GE. Dietary fat and serum lipids: an evaluation of the experimental data. Am J Clin Nutr. Jun 1993;57(6):875–83. https://doi.org/10.1093/ajcn/57.6.875.
Clarke R, Frost C, Collins R, Appleby P, Peto R. Dietary lipids and blood cholesterol: quantitative meta-analysis of metabolic ward studies. Bmj. 1997;314(7074):112–7. https://doi.org/10.1136/bmj.314.7074.112.
Howell WH, McNamara DJ, Tosca MA, Smith BT, Gaines JA. Plasma lipid and lipoprotein responses to dietary fat and cholesterol: a meta-analysis. Am J Clin Nutr. 1997;65(6):1747–64. https://doi.org/10.1093/ajcn/65.6.1747.
Weggemans RM, Zock PL, Urgert R, Katan MB. Differences between men and women in the response of serum cholesterol to dietary changes. Eur J Clin Invest. 1999;29(10):827–34. https://doi.org/10.1046/j.1365-2362.1999.00524.x.
Weggemans RM, Zock PL, Katan MB. Dietary cholesterol from eggs increases the ratio of total cholesterol to high-density lipoprotein cholesterol in humans: a meta-analysis. Am J Clin Nutr. 2001;73(5):885–91. https://doi.org/10.1093/ajcn/73.5.885.
Reaven GM, Abbasi F, Bernhart S, Coulston A, Darnell B, Dashti N, et al. Insulin resistance, dietary cholesterol, and cholesterol concentration in postmenopausal women. Metabolism. 2001;50(5):594–7. https://doi.org/10.1053/meta.2001.22559.
Quig DW, Thye FW, Ritchey SJ, Herbert WG, Clevidence BA, Reynolds LK, et al. Effects of short-term aerobic conditioning and high cholesterol feeding on plasma total and lipoprotein cholesterol levels in sedentary young men. Am J Clin Nutr. 1983;38(6):825–34. https://doi.org/10.1093/ajcn/38.6.825.
Johnson C, Greenland P. Effects of exercise, dietary cholesterol, and dietary fat on blood lipids. Arch Intern Med. 1990;150(1):137–41.
Rouhani MH, Rashidi-Pourfard N, Salehi-Abargouei A, Karimi M, Haghighatdoost F. Effects of egg consumption on blood lipids: a systematic review and meta- analysis of randomized clinical trials. J Am Coll Nutr. 2018;37(2):99–110. https://doi.org/10.1080/07315724.2017.1366878.
Wilson PW. High-density lipoprotein, low-density lipoprotein and coronary artery disease. Am J Cardiol. 1990;66(6):7a-10a. https://doi.org/10.1016/0002-9149(90)90562-f.
Khalighi Sikaroudi M, Soltani S, Kolahdouz-Mohammadi R, Clayton ZS, Fernandez ML, Varse F, et al. The responses of different dosages of egg consumption on blood lipid profile: an updated systematic review and meta-analysis of randomized clinical trials. J Food Biochem. 2020;44(8):e13263. https://doi.org/10.1111/jfbc.13263.
Gardner CD, Crimarco A, Landry MJ, Fielding-Singh P. Nutrition study design issues-important issues for interpretation. Am J Health Promot. 2020;34(8):951–4. https://doi.org/10.1177/0890117120960580d.
•• Tang WH, Wang Z, Levison BS, et al. Intestinal microbial metabolism of phosphatidylcholine and cardiovascular risk. N Engl J Med. 2013;368(17):1575–84. https://doi.org/10.1056/NEJMoa1109400. Findings from this study suggest that TMAO from dietary phosphatidylcholine is dependent on metabolism by the intestinal microbiota and increased TMAO levels are associated with an increased risk of incident major adverse cardiovascular events.
Zhu C, Sawrey-Kubicek L, Bardagjy AS, Houts H, Tang X, Sacchi R, et al. Whole egg consumption increases plasma choline and betaine without affecting TMAO levels or gut microbiome in overweight postmenopausal women. Nutr Res. 2020;78:36–41. https://doi.org/10.1016/j.nutres.2020.04.002.
Lemos BS, Medina-Vera I, Malysheva OV, Caudill MA, Fernandez ML. Effects of egg consumption and choline supplementation on plasma choline and trimethylamine-N-oxide in a young population. J Am Coll Nutr. 2018;37(8):716–23. https://doi.org/10.1080/07315724.2018.1466213.
DiMarco DM, Missimer A, Murillo AG, et al. Intake of up to 3 eggs/day increases HDL cholesterol and plasma choline while plasma trimethylamine-N-oxide is unchanged in a healthy population. Lipids. 2017;52(3):255–63. https://doi.org/10.1007/s11745-017-4230-9.
Missimer A, Fernandez ML, DiMarco DM, et al. Compared to an oatmeal breakfast, two eggs/day increased plasma carotenoids and choline without increasing trimethyl amine N-oxide concentrations. J Am Coll Nutr. 2018;37(2):140–8. https://doi.org/10.1080/07315724.2017.1365026.
Rohrmann S, Linseisen J, Allenspach M, von Eckardstein A, Muller D. Plasma concentrations of trimethylamine-N-oxide are directly associated with dairy food consumption and low-grade inflammation in a German adult population. J Nutr. 2016;146(2):283–9. https://doi.org/10.3945/jn.115.220103.
Kuhn T, Rohrmann S, Sookthai D, et al. Intra-individual variation of plasma trimethylamine-N-oxide (TMAO), betaine and choline over 1 year. Clin Chem Lab Med. 2017;55(2):261–8. https://doi.org/10.1515/cclm-2016-0374.
Qureshi AI, Suri FK, Ahmed S, Nasar A, Divani AA, Kirmani JF. Regular egg consumption does not increase the risk of stroke and cardiovascular diseases. Med Sci Monit. 2007;13(1):Cr1-8.
Djousse L, Gaziano JM. Egg consumption in relation to cardiovascular disease and mortality: the Physicians’ Health Study. Am J Clin Nutr. 2008;87(4):964–9. https://doi.org/10.1093/ajcn/87.4.964.
Zazpe I, Beunza JJ, Bes-Rastrollo M, et al. Egg consumption and risk of cardiovascular disease in the SUN Project. Eur J Clin Nutr. 2011;65(6):676–82. https://doi.org/10.1038/ejcn.2011.30.
Larsson SC, Akesson A, Wolk A. Egg consumption and risk of heart failure, myocardial infarction, and stroke: results from 2 prospective cohorts. Am J Clin Nutr. 2015;102(5):1007–13. https://doi.org/10.3945/ajcn.115.119263.
Diez-Espino J, Basterra-Gortari FJ, Salas-Salvado J, et al. Egg consumption and cardiovascular disease according to diabetic status: the PREDIMED study. Clin Nutr. 2017;36(4):1015–21. https://doi.org/10.1016/j.clnu.2016.06.009.
Farvid MS, Malekshah AF, Pourshams A, Poustchi H, Sepanlou SG, Sharafkhah M, et al. Dietary protein sources and all-cause and cause-specific mortality: the Golestan Cohort Study in Iran. Am J Prev Med. 2017;52(2):237–48. https://doi.org/10.1016/j.amepre.2016.10.041.
Nakamura Y, Okamura T, Kita Y, et al. Re-evaluation of the associations of egg intake with serum total cholesterol and cause-specific and total mortality in Japanese women. Eur J Clin Nutr. 2018;72(6):841–7. https://doi.org/10.1038/s41430-017-0051-4.
Qin C, Lv J, Guo Y, Bian Z, Si J, Yang L, et al. Associations of egg consumption with cardiovascular disease in a cohort study of 0.5 million Chinese adults. Heart. Nov 2018;104(21):1756–63. https://doi.org/10.1136/heartjnl-2017-312651.
Zhong VW, Van Horn L, Cornelis MC, et al. Associations of dietary cholesterol or egg consumption with incident cardiovascular disease and mortality. Jama. 2019;321(11):1081–95. https://doi.org/10.1001/jama.2019.1572.
•• Dehghan M, Mente A, Rangarajan S, et al. Association of egg intake with blood lipids, cardiovascular disease, and mortality in 177,000 people in 50 countries. Am J Clin Nutr. 2020;111(4):795–803. https://doi.org/10.1093/ajcn/nqz348. Findings from this study suggest that no significant associations between egg intake and blood lipids, mortality, or major CVD events.
Rong Y, Chen L, Zhu T, et al. Egg consumption and risk of coronary heart disease and stroke: dose- response meta-analysis of prospective cohort studies. Bmj. 2013;346:e8539. https://doi.org/10.1136/bmj.e8539.
Xu L, Lam TH, Jiang CQ, Zhang WS, Zhu F, Jin YL, et al. Egg consumption and the risk of cardiovascular disease and all-cause mortality: Guangzhou Biobank Cohort Study and meta-analyses. Eur J Nutr. 2019;58(2):785–96. https://doi.org/10.1007/s00394-018-1692-3.
Alexander DD, Miller PE, Vargas AJ, Weed DL, Cohen SS. Meta-analysis of egg consumption and risk of coronary heart disease and stroke. J Am Coll Nutr. 2016;35(8):704–16. https://doi.org/10.1080/07315724.2016.1152928.
Mazidi M, Katsiki N, Mikhailidis DP, Pencina MJ, Banach M. Egg consumption and risk of total and cause-specific mortality: an individual-based cohort study and pooling prospective studies on behalf of the Lipid and Blood Pressure Meta-analysis Collaboration (LBPMC) Group. J Am Coll Nutr. 2019;38(6):552–63. https://doi.org/10.1080/07315724.2018.1534620.
Drouin-Chartier JP, Schwab AL, Chen S, et al. Egg consumption and risk of type 2 diabetes: findings from 3 large US cohort studies of men and women and a systematic review and meta-analysis of prospective cohort studies. Am J Clin Nutr. 2020;112(3):619–30. https://doi.org/10.1093/ajcn/nqaa115.
Krittanawong C, Narasimhan B, Wang Z, et al. Association between egg consumption and risk of cardiovascular outcomes: a systematic review and meta-analysis. Am J Med. 2020. https://doi.org/10.1016/j.amjmed.2020.05.046.
Godos J, Micek A, Brzostek T, et al. Egg consumption and cardiovascular risk: a dose-response meta-analysis of prospective cohort studies. Eur J Nutr. 2020. https://doi.org/10.1007/s00394-020-02345-7.
Takagi H, Hari Y, Nakashima K, Kuno T, Ando T. Egg consumption and coronary artery disease: a nice knockdown argument. Angiology. 2020;71(7):589–601. https://doi.org/10.1177/0003319719897493.
Xia PF, Pan XF, Chen C, Wang Y, Ye Y, Pan A. Dietary intakes of eggs and cholesterol in relation to all-cause and heart disease mortality: a prospective cohort study. J Am Heart Assoc. 2020;9(10):e015743. https://doi.org/10.1161/jaha.119.015743.
Drouin-Chartier JP, Chen S, Li Y, et al. Egg consumption and risk of cardiovascular disease: three large prospective US cohort studies, systematic review, and updated meta- analysis. Bmj. 2020;368:m513. https://doi.org/10.1136/bmj.m513.
Nakamura Y, Iso H, Kita Y, Ueshima H, Okada K, Konishi M, et al. Egg consumption, serum total cholesterol concentrations and coronary heart disease incidence: Japan Public Health Center-based prospective study. Br J Nutr. 2006;96(5):921–8. https://doi.org/10.1017/bjn20061937.
Haring B, Gronroos N, Nettleton JA, von Ballmoos MC, Selvin E, Alonso A. Dietary protein intake and coronary heart disease in a large community based cohort: results from the Atherosclerosis Risk in Communities (ARIC) study [corrected]. PLoS One. 2014;9(10):e109552. https://doi.org/10.1371/journal.pone.0109552.
Virtanen JK, Mursu J, Virtanen HE, et al. Associations of egg and cholesterol intakes with carotid intima-media thickness and risk of incident coronary artery disease according to apolipoprotein E phenotype in men: the Kuopio Ischaemic Heart Disease Risk Factor Study. Am J Clin Nutr. 2016;103(3):895–901. https://doi.org/10.3945/ajcn.115.122317.
Chagas P, Caramori P, Galdino TP, Barcellos Cda S, Gomes I, Schwanke CH. Egg consumption and coronary atherosclerotic burden. Atherosclerosis. 2013;229(2):381–4. https://doi.org/10.1016/j.atherosclerosis.2013.05.008.
Goldberg S, Gardener H, Tiozzo E, Ying Kuen C, Elkind MSV, Sacco RL, et al. Egg consumption and carotid atherosclerosis in the Northern Manhattan study. Atherosclerosis. 2014;235(2):273–80. https://doi.org/10.1016/j.atherosclerosis.2014.04.019.
Robbins JM, Petrone AB, Ellison RC, Hunt SC, Carr JJ, Heiss G, et al. Association of egg consumption and calcified atherosclerotic plaque in the coronary arteries: the NHLBI Family Heart Study. Espen j. 2014;9(3):e131–5. https://doi.org/10.1016/j.clnme.2014.04.004.
Choi Y, Chang Y, Lee JE, Chun S, Cho J, Sung E, et al. Egg consumption and coronary artery calcification in asymptomatic men and women. Atherosclerosis. 2015;241(2):305–12. https://doi.org/10.1016/j.atherosclerosis.2015.05.036.
Sauvaget C, Nagano J, Allen N, Grant EJ, Beral V. Intake of animal products and stroke mortality in the Hiroshima/Nagasaki Life Span Study. Int J Epidemiol. 2003;32(4):536–43. https://doi.org/10.1093/ije/dyg151.
Bernstein AM, Pan A, Rexrode KM, Stampfer M, Hu FB, Mozaffarian D, et al. Dietary protein sources and the risk of stroke in men and women. Stroke. 2012;43(3):637–44. https://doi.org/10.1161/strokeaha.111.633404.
Abdollahi AM, Virtanen HEK, Voutilainen S, et al. Egg consumption, cholesterol intake, and risk of incident stroke in men: the Kuopio Ischaemic Heart Disease Risk Factor Study. Am J Clin Nutr. 2019;110(1):169–76. https://doi.org/10.1093/ajcn/nqz066.
• Djousse L, Gaziano JM. Egg consumption and risk of heart failure in the Physicians’ Health Study. Circulation. 2008;117(4):512–6. https://doi.org/10.1161/circulationaha.107.734210. Findings from this study suggest that infrequent egg consumption is not associated with the risk of heart failure.
Nettleton JA, Steffen LM, Loehr LR, Rosamond WD, Folsom AR. Incident heart failure is associated with lower whole-grain intake and greater high-fat dairy and egg intake in the Atherosclerosis Risk in Communities (ARIC) study. J Am Diet Assoc. 2008;108(11):1881–7. https://doi.org/10.1016/j.jada.2008.08.015.
MacDonald CJ, Madika AL, Bonnet F, Fagherazzi G, Lajous M, Boutron-Ruault MC. Cholesterol and egg intakes, and risk of hypertension in a large prospective cohort of French women. Nutrients. 2020;12(5). https://doi.org/10.3390/nu12051350.
Zhang Y, Zhang DZ. Red meat, poultry, and egg consumption with the risk of hypertension: a meta-analysis of prospective cohort studies. J Hum Hypertens. 2018;32(7):507–17. https://doi.org/10.1038/s41371-018-0068-8.
Wang MX, Wong CH, Kim JE. Impact of whole egg intake on blood pressure, lipids and lipoproteins in middle-aged and older population: a systematic review and meta-analysis of randomized controlled trials. Nutr Metab Cardiovasc Dis. 2019;29(7):653–64. https://doi.org/10.1016/j.numecd.2019.04.004.
Kolahdouz-Mohammadi R, Malekahmadi M, Clayton ZS, et al. Effect of egg consumption on blood pressure: a systematic review and meta-analysis of randomized clinical trials. Curr Hypertens Rep. 2020;22(3):24. https://doi.org/10.1007/s11906-020-1029-5.
Author information
Authors and Affiliations
Contributions
All authors had access to the data and contributed significantly to the work and a role in writing the manuscript.
Corresponding author
Ethics declarations
Conflict of Interest
Dr. Krittanawong discloses the following relationships – Member of the American College of Cardiology Solution Set Oversight Committee and the American College of Cardiology/American Heart Association (ACC/AHA) Task Force on Performance Measures, The Lancet Digital Health (Advisory Board), European Heart Journal Digital Health (Editorial board), Journal of the American Heart Association (Editorial board), JACC: Asia (Section Editor), and The Journal of Scientific Innovation in Medicine (Associate Editor). Dr. Virani discloses the following relationships: Grant support: Department of Veterans Affairs, World Heart Federation, and Tahir and Jooma Family; Honorarium: American College of Cardiology (Associate Editor for Innovations, acc.org).
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Cardiovascular Care
Rights and permissions
About this article

Cite this article
Hahn, J., Dehghan, M., Drouin-Chartier, JP. et al. Egg Consumption and Risk of Cardiovascular Disease: a Critical Review. Curr Emerg Hosp Med Rep 9, 25–37 (2021). https://doi.org/10.1007/s40138-021-00225-w
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40138-021-00225-w