
Abstract
Purpose of Review
The main objective in this 2nd part is to highlight comorbidities of great clinical importance such as diabetes, anemia, and chronic renal failure, either because of their high prevalence, or because of their relevance to impact on morbidity and mortality, and directly in the treatment of heart failure.
Recent Findings
The prevalence of heart failure will increase 46% from 2012 to 2030, resulting in > 8 million people ≥ 18 years of age. This disease have a large burden of noncardiovascular comorbidities, which may increase the risk of mortality and decrease quality of life. There is a perception that patients hospitalized for heart failure are also becoming more medically complex. In this review, we highlight important comorbidities often found in patients with heart failure.
Summary
Diabetes mellitus is present in ∼ 40% of patients with heart failure and is associated with an increased risk of morbidity and mortality. Both pathologies present an intriguing pathophysiological overlap, which will be addressed below. Anemia, peripheral artery disease, sarcopenia, cachexia, and chronic kidney disease (CKD) will also be addressed, especially in relation to heart failure.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
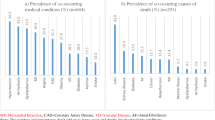
The main objective of this 2nd part is to demonstrate that a better understanding of comorbidities such as sarcopenia, cachexia, diabetes mellitus (DM), and anemia, in addition to their pathophysiological and therapeutic implications, in the modern management of heart failure (HF), as such conditions can interfere with their survival and quality of life of patients (Fig. 1).

Demonstration of comorbidities which can interfere with the survival and quality of life of patients
DM is present in ∼ 40% of patients with heart failure and is associated with an increased risk of morbidity and mortality. Both pathologies present an intriguing pathophysiological overlap, which will be addressed below. Anemia, peripheral artery disease, sarcopenia, cachexia, and chronic kidney disease (CKD) will also be addressed, especially in relation to HF. Interestingly, DM and HF seem to have a bidirectional relationship.
Sarcopenia and Cachexia
Sarcopenia is defined as the loss of muscle mass associated with a loss of muscle function, e.g., walking speed and commonly defined as muscle loss, which reduces subject walking speed = 1 m/s or walking distance < 400 m during a 6-min walking test distance, and was an independent predictor of poor exercise capacity [1]. The prevalence of sarcopenia (muscle wasting) is approximately 19.5%. Management of sarcopenia should consist of resistance exercise in combination with a protein intake of 1 to 1.5 g/kg/day. There is insufficient evidence that vitamin D and anabolic steroids are beneficial [2•].
Cachexia is defined as unintentional non-edematous weight loss of > 5% over at least 6 months. Recently, this definition was improved with the following new criteria: 1) decreased muscle strength, 2) fatigue, 3) anorexia, 4) low fat free mass index, and 5) abnormal biochemistry (anemia (Hb < 120 g/L), low serum albumin (< 32 g/L), increased inflammatory markers (CRP > 5 mg/L, IL-6 > 4 pg/mL)) [3]. Cachexia affects about 10–39% of patients with HF, and it typically occurs in the advanced stages of HF, especially in the presence of congestive right ventricular dysfunction. The prevalence of cachexia among patients with HF ranges between 10 and 39%, depending on the study design, diagnostic criteria of cachexia, and stage of HF. Cachexia is more frequent in patients with advanced disease and HF with reduced ejection fraction (HFrEF) [4]. There is little evidence of the benefit of cachexia-specific treatments, but, undoubtedly, an optimization of HF and, whenever possible, physical exercise to preserve lean muscle mass appear to be beneficial [5].
Diabetes Mellitus
Epidemiologic and clinical data from the last 2 decades have led to the recognition that, in addition to myocardial infarction and other atherosclerosis-related cardiovascular events, HF is a major contributor to cardiovascular morbidity and mortality in patients with DM. Following the first HF hospitalization, the incidence of new-onset diabetes is around 2% per year, increasing to 3% after 5 years of follow-up. New-onset DM was associated with an increased risk of death, compared with HF patients with prevalent diabetes (intermediate risk) and HF patients without DM [6•]. In many patients, the observation that myocardial dysfunction is present in the absence of coronary artery disease has led to the use of the poorly understood term “diabetic cardiomyopathy (DCM)” [7].
Over the last few years, this term has been the subject of controversy. However, recently, Kaljda et al. published a community-based cohort matched for age, sex, hypertension, coronary artery disease (CAD), and diastolic function, and participants with DM had an increased incidence of HF over a 10-year follow-up period, even in the absence of underlying diastolic dysfunction. The authors concluded that these findings suggest that DM is an independent risk factor for the development of HF, supporting the concept of DCM [8].
Interest in this association has dramatically increased the number of PubMed publications in the last decade, demonstrating the great relevance of this theme, Fig. 2. A U-shaped relationship between body mass index (BMI) and cardiovascular events among patients with acute HF has been reported. BMI was inversely correlated to the risk of mortality in patients with T2D. Moreover, severe obesity was associated with less mortality risk [9].

Increased number of PubMed publications in the last decade with the term “Diabetes mellitus and heart failure”
There is a strong interrelation between DM and HF. DM is one of the most important risk factors for the development of HF. New treatments for type 2 DM and HF are needed, and rather than considering treatments for these conditions as separate goals, the implication of recent cardiovascular clinical outcomes trials is that targeting shared risk factors and pathophysiologies may allow us to treat and prevent both conditions simultaneously [10].
Peripheral Arterial Disease
PAD and HF have several common risk factors, and each has been associated with increased morbidity and mortality. Patients with PAD have an increased risk of angina, myocardial infarction, stroke, congestive HF, and death compared with patients without PAD. The most frequent PAD symptom is intermittent claudication, defined as muscle pain or weakness induced by exercise and relieved with rest, which occurs distal to the arterial obstruction [11]. There is a positive relationship between PAD and HF. All-cause mortality, hospitalization, and cardiovascular mortality in HF patients with PAD were higher than in those without this comorbidity [12, 13].
PAD often goes undetected, and yet, in spite of the availability of screening tools, this is not commonly considered in HF care [14]. The ankle-brachial index (ABI) is a simple, noninvasive tool for the diagnosis of PAD. In a community cohort of middle-age Americans with up to 22 years of follow-up, Gupta et al. [15] found that a low ABI (≤ 1.00) from a single randomly chosen lower extremity was significantly associated with an increased risk for the development of HF. Patients who are symptomatic, smokers, and those with diagnosed coronary heart disease and diabetes should be targeted for the screening of PAD [16].
Anemia
Iron deficiency is an extremely common comorbidity in patients with HF, affecting up to 50% of all ambulatory patients. Since it contributes to cardiac and peripheral muscle dysfunction, it is associated with poorer clinical outcomes and a greater risk of death, independent of hemoglobin level. Therefore, iron deficiency emerges as a new comorbidity and a therapeutic target of chronic HF [77–80]. Laboratory parameters of serum ferritin < 100 μg/l or 100 to 300 μg/ l, with transferrin saturation < 20%, are established to define the diagnosis of iron deficiency in patients with HFREF [17, 18].
In a series of placebo-controlled, randomized studies in patients with HF and iron deficiency, intravenous iron had a favorable effect on exercise capacity, functional class, LVEF, renal function, and quality of life [19, 20]. During the past 10 years, knowledge about the transport, storage, and homeostasis of iron has improved dramatically, and new molecules involved in iron metabolism have been described (e.g., hepcidin, ferroportin, divalent metal transporter).
Oral iron products have been shown to have little efficacy in patients with HF, where the preference is intravenous iron products. The Iron Repletion Effects on Oxygen Uptake in Heart Failure (IRONOUT-HF) trial previously demonstrated that oral iron supplementation minimally increased iron stores and did not improve exercise capacity in patients with HF, with a reduced ejection fraction and iron deficiency [21]. Most clinical studies have been performed using ferric carboxymaltose, with good efficacy in terms of improvements in a 6-min walk test distance, peak oxygen consumption, quality of life, and improvements in New York Heart Association functional class. The data from meta-analyses also suggest beneficial effects in terms of hospitalization rates for patients with HF and reductions in cardiovascular mortality rates [19].
Recent European guidelines recommend the monitoring of iron parameters (i.e., serum ferritin, transferrin saturation) for all patients with HF. Ongoing clinical trials will explore the benefits of iron deficiency correction on various HF parameters. A class I recommendation based on meta-analysis (level of evidence: A, because two large trials, ferinject assessment in patients with iron deficiency and chronic heart failure (FAIR-HF) and ferric carboxymaltse evaluation on performance in patients with iron deficiency in combination with chronic heart failure (CONFIRM-HF), published positive results) [22].
A prospective trial to investigate the effects on morbidity and mortality is currently ongoing. Since no validations exist for HF with preserved ejection fraction, it should be regarded with caution in this population [the FAIR HFPEF study addresses whether treatment with IV iron (ferric carboxymaltose) in patients with HF with preserved ejection fraction and iron deficiency can improve exercise capacity and symptoms while being safe (NCT03074591)].
Coronary Artery Disease
CAD is the most common etiology of HFrEF, with about 2/3 of cases [23]. Older patients with HF more commonly have CAD as the cause of their HF than younger patients. The presence of left ventricular dysfunction yields a worse prognosis for patients with CAD. More than 70% of patients with ischemic cardiomyopathy (ICM) severe left ventricular dysfunction have a great burden of comorbidities, associated with greater functional limitations and decreased survival rates [24,25,26].
One of the goals of coronary artery bypass surgery (CABS) for this group of patients is contractile recovery after the procedure, with improvement of symptoms, functional capacity, and reduction in mortality. In a sub-analysis of the STICH (Surgical Treatment for Ischemic Heart Failure) study, three predictors of good prognosis with CABS were three-vessel disease, ejection fraction below 27%, and indexed end-systolic volume greater than 79 mL/m2. If the patient has two or more of these factors, benefits more when submitted to CABS than the patient that have just one. The results of the long-term follow-up of the STICH study corroborate this indication for surgical revascularization for ICM instead of OMT alone [27].
Nevertheless, controversy exists over the patient selection for CABS because of the surgical risk. However, for patients who are young with few comorbidities, CABS is low risk, with a great improvement in cardiovascular and all-cause morbidity and mortality [28]. Guidelines provide evidence of myocardial viability prior to CABS. Among all non-invasive methods, positron emission tomography (PET) using 18F-fluorodeoxyglucose (FDG) has the highest sensitivity and is considered the gold standard for the detection of hibernating myocardium.
Viability imaging should be limited to situations in which revascularization decisions are most difficult. Viability imaging should be used when it will favor decision-making [29]. However, it is important to remember that subjects with myocardial viability have increased mortality if they do not receive revascularization in addition to medical treatment. Many issues related to myocardial viability remain. Hopefully, they will soon be answered with prospective, randomized trials using state of the art imaging modalities [30]. In this matter, there is one currently in progress evaluating the role of advanced imaging in the management of ischemic cardiomyopathy [31, 32]. Another point is whether coronary percutaneous intervention (PCI) has the same advantages as those seen with CABS. There is a lack of strong evidence. In fact, in this regard, some studies have shown inferiority of PCI compared with CABS [33]. The ongoing REVIVED-BCIS2 (Study of Efficacy and Safety of Percutaneous Coronary Intervention to Improve Survival in Heart Failure) trial will test the hypothesis that PCI plus OMT will improve event-free survival in subjects with ICM and viable myocardium compared to OMT alone [34].
Chronic Kidney Disease
HF and CKD are diseases that have increased prevalence and incidence in the world population [35, 36]. Kidney dysfunction may cause HF, and HF may induce kidney disfunction, creating a vicious cycle of interdependence [37]. Some of the factors that contribute to HF and CKD are DM, systemic arterial hypertension, association of comorbidities, and, the most important, aging of the population [35].
The coexistence of CKD and HF is notorious; although, in patients classified as HFPEF, it is less frequent than in patients with HFREF. Half of patients have HFPEF, and this percentage is projected to increase over the next few years [38]. Approximately 30% of patients admitted for acute HF have acute or CKD, and about 50% of HF patients have CKD [39], defined as a glomerular filtration rate (GFR) of less than 60 ml/min/1.73 m2. The real prevalence of this situation is still a matter of investigation. It occurs because most studies present CKD as exclusion criteria, especially advanced stages of the disease.
The worse the kidney function, the worse the prognosis of the individual with or without HF. Due to the high morbidity and mortality and the high costs of this association, it is necessary to create protocols that include these entities. CKD patients have very high mortality rates, and about 50% of deaths are related to cardiovascular disease [40]. Among those with advanced CKD, especially patients on renal replacement therapy such as dialysis, rates are even more significant, with HF and coronary disease predominating [40]. Mortality is independent of the ejection fraction of these individuals. In patients with HFREF, in which drug treatment has been shown to reduce mortality and hospitalizations, current evidence recommends the use of these drugs despite the limited information available. In patients with HFPEF, in which there is no drug treatment that has been shown to reduce mortality, treatment is based on the treatment of underlying pathologies with greater restrictions in CKD populations. Interestingly, this population has the highest association with CKD.
In a study of patients referred for dialysis, 74% had left ventricular hypertrophy (LVH) [41]. Patients undergoing repetitive dialysis have progression of myocardial fibrosis and increased left ventricular mass indices. Of these, a significant percentage have worsened ventricular function and manifest HF. However, in patients with stage-V CKD, the dialytic process does not modify LVH but worsens ejection fraction. In CKD patients, morpho-structural changes and ventricular function alterations are present even in early stages of the disease. Most patients with advanced CKD do not die from kidney causes but from cardiovascular disease, especially HF.
About 94% of patients hospitalized for HF are so-called “wet and warm.” The treatment aims to reduce pulmonary and systemic congestion. The latter plays an essential role in organ dysfunction, being more relevant than the reduction of cardiac output in the pathophysiology of renal injury. The interrelationship between HF and CKD involves neurohormonal, hemodynamic mechanisms, anemia, inflammation, electrolyte changes [42], and the creation of arteriovenous short circuit through the hemodialysis fistula (which initially leads to overload to the right ventricle and later to the left ventricle). The interrelationship between these diseases is so complex that the term cardio renal syndrome was introduced and divided into five subtypes, depending on the initial factor of decompensation [43, 44].
Whether due to initial HF and after kidney disease or vice versa, if decompensation is acute or chronic and if it is for another predominant non cardiorenal cause, HF drugs may affect CKD in different ways. For decongestion of the patient, the furosemide or torsemide loop diuretics are usually used. Their chronic administration in HF can cause diuretic resistance [45, 46]. In advanced CKD, loop diuretic doses should be high. Sometimes, concomitant use of thiazides, acetazolamide, or spironolactone/eplerenone is required for so-called nephron sequential blockade [43]. A new study using data from several beta blocker trials showed that they are effective in reducing mortality in HFREF individuals with moderate to severe renal impairment [47].
Beta blockers can be used in CKD. Carvedilol is poorly dialyzable, but it has benefits in this population, with a study showing favorable remodeling even in dialysis patients. Metoprolol is dialyzable, and bisoprolol is not.
Regarding the use of angiotensin converting enzyme inhibitors (ACEI), there is evidence of beneficial effects [39] even in patients with severe CKD [48]. There is an ongoing study testing this hypothesis [49]. Angiotensin II receptor blockers (ARBs) have studies in moderate renal dysfunction, but with little evidence of severe dysfunction. Mineralocorticoid blockers are routinely used in CKD, except when glomerular filtration rate (GFR) is below 30 mL/min/1.73 m2. There are few studies with dialysis patients using (ACEI)/ARB + spironolactone that show promising results. Sacubitril valsartan, which is an angiotensin/neprilysin inhibitor, has been shown to reduce mortality and hospital readmissions in patients with HFREF [50] and to improve quality of life in HFPEF patients, but it has not been tested in patients with GFR below 30 mL/min/1.73 m2 [51, 52]. A new study focusing on renal protection was conducted with this drug in CKD patients with proteinuria and GFR between 20 and 60 ml/min/1.73 m2, and it showed no difference between sacubitril-valsartan and irbersartan on GFR or in proteinuria results [53].
Regarding the current treatment of HFREF with sodium-glucose cotransporter-2 (SGLT2) inhibitors, although it has not been tested on GFR below 30 mL/min/1.73 m2, there was evidence that in the primary outcome (hospitalization for HF, death from cardiovascular cause, or use of venous therapy for HF) the drug did work in subjects with rates of less than 60 mL/min/1.73 m2 [54••].
Limitations
It is a narrative (non-systematic) review of the literature on the topic addressed, and thus, although we have expressed the search methodology in the first part of this review, it is subject to conscious and unconscious bias due to the selection and construction of this text by the authors themselves, making reproducibility difficult. However, this narrative are useful for educational purpose since they pull many pieces of information together into a readable format addressing several complex topics concentrated in 2 papers (part 1 and 2).
Future Directions
Despite the pharmacological arsenal available for the treatment of patients with HF, the progressive global population aging, technological advances that collaborate with the maintenance of life, the concomitance of several comorbidities, making the interrelation between pathologies and treatments a complex level of interactions that require a holistic view from the clinical physician and joint monitoring with several other specialties.
For the future, we will have new monitoring devices that added to artificial intelligence will bring detailed information to individualize the treatment of each patient.
Conclusion
With population aging and increased survival, chronic diseases stand out with high prevalence. Especially in the elderly, the presence of simultaneous and complex comorbidities, such as HF and DM, require knowledge and contact with various specialties from the attending physician. Thus, it is essential to deepen our knowledge in a multidisciplinary way, offering the HF patient a more holistic and functional view.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Morley JE. Hormones and sarcopenia. Curr Pharm Des. 2017;23(30):4484–92. https://doi.org/10.2174/1381612823666161123150032.
• Bauer J, Morley JE, Schols A, Ferrucci L, Cruz-Jentoft AJ, Dent E, et al. Sarcopenia: a time for action. An SCWD position paper. J Cachexia Sarcopenia Muscle. 2019;10(5):956–61. https://doi.org/10.1002/jcsm.12483. This position statement provides recommendations on the management of sarcopenia and how to progress the knowledge and recognition of sarcopenia.
Correale M, Paolillo S, Mercurio V, Limongelli G, Barilla F, Ruocco G, et al. Comorbidities in chronic heart failure: an update from Italian Society of Cardiology (SIC) Working Group on Heart Failure. Eur J Intern Med. 2019. https://doi.org/10.1016/j.ejim.2019.10.008.
Valentova M, Anker SD, von Haehling S. Cardiac cachexia revisited: the role of wasting in heart failure. Heart Fail Clin. 2020;16(1):61–9. https://doi.org/10.1016/j.hfc.2019.08.006.
Gielen S, Sandri M, Kozarez I, Kratzsch J, Teupser D, Thiery J, et al. Exercise training attenuates MuRF-1 expression in the skeletal muscle of patients with chronic heart failure independent of age: the randomized Leipzig Exercise Intervention in Chronic Heart Failure and Aging catabolism study. Circulation. 2012;125(22):2716–27. https://doi.org/10.1161/CIRCULATIONAHA.111.047381.
• Zareini B, Rorth R, Holt A, Mogensen UM, Selmer C, Gislason G, et al. Heart failure and the prognostic impact and incidence of new-onset of diabetes mellitus: a nationwide cohort study. Cardiovasc Diabetol. 2019;18(1):79. https://doi.org/10.1186/s12933-019-0883-4. New-onset diabetes was associated with an increased risk of death, compared to HF patients with prevalent diabete.
Lehrke M, Marx N. Diabetes mellitus and heart failure. Am J Med. 2017;130(6S):S40–50. https://doi.org/10.1016/j.amjmed.2017.04.010.
Klajda MD, Scott CG, Rodeheffer RJ, Chen HH. Diabetes mellitus is an independent predictor for the development of heart failure: a population study. Mayo Clin Proc. 2020;95(1):124–33. https://doi.org/10.1016/j.mayocp.2019.07.008.
Abi Khalil C, Sulaiman K, Singh R, Jayyousi A, Asaad N, AlHabib KF, et al. BMI is inversely correlated to the risk of mortality in patients with type 2 diabetes hospitalized for acute heart failure: findings from the Gulf aCute heArt failuRE (Gulf-CARE) registry. Int J Cardiol. 2017;241:262–9. https://doi.org/10.1016/j.ijcard.2017.02.119.
Wilkinson MJ, Zadourian A, Taub PR. Heart failure and diabetes mellitus: defining the problem and exploring the interrelationship. Am J Cardiol. 2019;124(Suppl 1):S3–S11. https://doi.org/10.1016/j.amjcard.2019.10.024.
Newman AB, Shemanski L, Manolio TA, Cushman M, Mittelmark M, Polak JF, et al. Ankle-arm index as a predictor of cardiovascular disease and mortality in the cardiovascular health study. The cardiovascular health study group. Arterioscler Thromb Vasc Biol. 1999;19(3):538–45. https://doi.org/10.1161/01.atv.19.3.538.
Wei B, Qian C, Fang Q, Wang Y. The prognostic value of peripheral artery disease in heart failure: insights from a meta-analysis. Heart Lung Circ. 2016;25(12):1195–202. https://doi.org/10.1016/j.hlc.2016.04.002.
Nakamura Y, Kunii H, Yoshihisa A, Takiguchi M, Shimizu T, Yamauchi H, et al. Impact of peripheral artery disease on prognosis in hospitalized heart failure patients. Circ J. 2015;79(4):785–93. https://doi.org/10.1253/circj.CJ-14-1280.
Inglis SC, Hermis A, Shehab S, Newton PJ, Lal S, Davidson PM. Peripheral arterial disease and chronic heart failure: a dangerous mix. Heart Fail Rev. 2013;18(4):457–64. https://doi.org/10.1007/s10741-012-9331-1.
Gupta DK, Skali H, Claggett B, Kasabov R, Cheng S, Shah AM, et al. Heart failure risk across the spectrum of ankle-brachial index: the ARIC study (Atherosclerosis Risk In Communities). JACC Heart Fail. 2014;2(5):447–54. https://doi.org/10.1016/j.jchf.2014.05.008.
Jankowska EA, Kasztura M, Sokolski M, Bronisz M, Nawrocka S, Oleskowska-Florek W, et al. Iron deficiency defined as depleted iron stores accompanied by unmet cellular iron requirements identifies patients at the highest risk of death after an episode of acute heart failure. Eur Heart J. 2014;35(36):2468–76. https://doi.org/10.1093/eurheartj/ehu235.
Zhang H, Zhabyeyev P, Wang S, Oudit GY. Role of iron metabolism in heart failure: from iron deficiency to iron overload. Biochim Biophys Acta Mol basis Dis. 2019;1865(7):1925–37. https://doi.org/10.1016/j.bbadis.2018.08.030.
Qian C, Wei B, Ding J, Wu H, Wang Y. The efficacy and safety of Iron supplementation in patients with heart failure and Iron deficiency: a systematic review and meta-analysis. Can J Cardiol. 2016;32(2):151–9. https://doi.org/10.1016/j.cjca.2015.06.009.
Klip IT, Comin-Colet J, Voors AA, Ponikowski P, Enjuanes C, Banasiak W, et al. Iron deficiency in chronic heart failure: an international pooled analysis. Am Heart J. 2013;165(4):575–82 e3. https://doi.org/10.1016/j.ahj.2013.01.017.
Ebner N, von Haehling S. Iron deficiency in heart failure: a practical guide. Nutrients. 2013;5(9):3730–9. https://doi.org/10.3390/nu5093730.
von Haehling S, Ebner N, Evertz R, Ponikowski P, Anker SD. Iron deficiency in heart failure: an overview. JACC Heart Fail. 2019;7(1):36–46. https://doi.org/10.1016/j.jchf.2018.07.015.
Ebner N, Jankowska EA, Ponikowski P, Lainscak M, Elsner S, Sliziuk V, et al. The impact of iron deficiency and anaemia on exercise capacity and outcomes in patients with chronic heart failure. Results from the studies investigating co-morbidities aggravating heart failure. Int J Cardiol. 2016;205:6–12. https://doi.org/10.1016/j.ijcard.2015.11.178.
Bekfani T, Pellicori P, Morris D, Ebner N, Valentova M, Sandek A, et al. Iron deficiency in patients with heart failure with preserved ejection fraction and its association with reduced exercise capacity, muscle strength and quality of life. Clin Res Cardiol. 2019;108(2):203–11. https://doi.org/10.1007/s00392-018-1344-x.
Lewis GD, Malhotra R, Hernandez AF, McNulty SE, Smith A, Felker GM, et al. Effect of oral iron repletion on exercise capacity in patients with heart failure with reduced ejection fraction and Iron deficiency: the IRONOUT HF randomized clinical trial. JAMA. 2017;317(19):1958–66. https://doi.org/10.1001/jama.2017.5427.
McDonagh T, Damy T, Doehner W, Lam CSP, Sindone A, van der Meer P, et al. Screening, diagnosis and treatment of iron deficiency in chronic heart failure: putting the 2016 European Society of Cardiology heart failure guidelines into clinical practice. Eur J Heart Fail. 2018;20(12):1664–72. https://doi.org/10.1002/ejhf.1305.
Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, et al. 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2016;37:2129–200. https://doi.org/10.1093/eurheartj/ehw128.
Howlett JG, Stebbins A, Petrie MC, Jhund PS, Castelvecchio S, Cherniavsky A, et al. CABG improves outcomes in patients with ischemic cardiomyopathy. JACC: Heart Fail. 2019;7:878–87. https://doi.org/10.1016/j.jchf.2019.04.018.
Hassanabad AF, MacQueen KT, Ali I. Surgical treatment for ischemic heart failure (STICH) trial: a review of outcomes. J Card Surg. 2019;34:1075–82. https://doi.org/10.1111/jocs.14166.
Ambrosy AP, Stevens SR, Al-Khalidi HR, Rouleau JL, Bouabdallaoui N, Carson PE, et al. Burden of medical co-morbidities and benefit from surgical revascularization in patients with ischaemic cardiomyopathy. Eur J Heart Fail. 2019;21:373–81. https://doi.org/10.1002/ejhf.1404.
Kandolin RM, Wiefels CC, Mesquita CT, Chong AY, Boland P, Glineur D, et al. The current role of viability imaging to guide revascularization and therapy decisions in patients with heart failure and reduced left ventricular function. Can J Cardiol. 2019;35:1015–29. https://doi.org/10.1016/j.cjca.2019.04.029.
Patel H, Mazur W, Williams KA, Kalra DK. Myocardial viability–state of the art: is it still relevant and how to best assess it with imaging? Trends Cardiovasc Med. 2018;28:24–37. https://doi.org/10.1016/j.tcm.2017.07.001.
O'Meara E, Mielniczuk LM, Wells GA, de Kemp RA, Klein R, Coyle D, et al. Alternative Imaging Modalities in Ischemic Heart Failure (AIMI-HF) IMAGE HF Project I-A: study protocol for a randomized controlled trial. Trials. 2013;14:1–12. https://doi.org/10.1186/1745-6215-14-218.
Beanlands R. IMAGE-HF Project I-A: Cardiac Imaging in Ischemic Heart Failure (AIMI-HF) - Full Text View - ClinicalTrials.gov. 2019.
Hage F, Hage A, Haddad H, Kiaii B. Update on revascularization in patients with heart failure and coronary artery disease. Curr Opin Cardiol. 2018;33:232–6. https://doi.org/10.1097/HCO.0000000000000483.
Perera D, Clayton T, Petrie MC, Greenwood JP, O’Kane PD, Evans R, et al. Percutaneous revascularization for ischemic ventricular dysfunction: rationale and design of the REVIVED-BCIS2 trial. JACC: Heart Fail. 2018;6:517–26. https://doi.org/10.1016/j.jchf.2018.01.024.
Smith GL, Lichtman JH, Bracken MB, Shlipak MG, Phillips CO, DiCapua P, et al. Renal impairment and outcomes in heart failure: systematic review and meta-analysis. J Am Coll Cardiol. 2006;47(10):1987–96. https://doi.org/10.1016/j.jacc.2005.11.084.
Boudoulas KD, Triposkiadis F, Parissis J, Butler J, Boudoulas H. The cardio-renal interrelationship. Prog Cardiovasc Dis. 2017;59(6):636–48. https://doi.org/10.1016/j.pcad.2016.12.003.
Gheorghiade M, Filippatos G. Reassessing treatment of acute heart failure syndromes: the ADHERE Registry. Eur Heart J Suppl. 2005;7(suppl_B):B13–B9. https://doi.org/10.1093/eurheartj/sui008.
Kim H-J, Lee M-H, Jo S-H, Seo W-W, Kim SE, Kim K-J, et al. Effects of angiotensin-converting enzyme inhibitors and angiotensin-receptor blockers in heart failure with chronic kidney disease ― propensity score matching analysis ―. Circ J. 2019. https://doi.org/10.1253/circj.CJ-19-0782.
Bansal N, Katz R, Robinson-Cohen C, Odden MC, Dalrymple L, Shlipak MG, et al. Absolute rates of heart failure, coronary heart disease, and stroke in chronic kidney disease: an analysis of 3 community-based cohort studies. JAMA Cardiol. 2017;2(3):314–8. https://doi.org/10.1001/jamacardio.2016.4652.
Foley RN, Curtis BM, Randell EW, Parfrey PS. Left ventricular hypertrophy in new hemodialysis patients without symptomatic cardiac disease. Clin J Am Soc Nephrol. 2010;5(5):805–13. https://doi.org/10.2215/cjn.07761109.
Schefold JC, Filippatos G, Hasenfuss G, Anker SD, von Haehling S. Heart failure and kidney dysfunction: epidemiology, mechanisms and management. Nat Rev Nephrol. 2016;12(10):610–23. https://doi.org/10.1038/nrneph.2016.113.
Arrigo M, Cippà PE, Mebazaa A. Cardiorenal interactions revisited: how to improve heart failure outcomes in patients with chronic kidney disease. Curr Heart Fail Rep. 2018;15(5):307–14. https://doi.org/10.1007/s11897-018-0406-8.
Cowger JA, Radjef R. Advanced heart failure therapies and cardiorenal syndrome. Adv Chronic Kidney Dis. 2018;25(5):443–53. https://doi.org/10.1053/j.ackd.2018.08.012.
Rangaswami J, Bhalla V, Blair JEA, Chang TI, Costa S, Lentine KL, et al. Cardiorenal syndrome: classification, pathophysiology, diagnosis, and treatment strategies: a scientific statement from the American Heart Association. Circulation. 2019;139(16):e840–e78. https://doi.org/10.1161/CIR.0000000000000664.
Ellison DH, Felker GM. Diuretic treatment in heart failure. N Engl J Med. 2017;377(20):1964–75. https://doi.org/10.1056/NEJMra1703100.
Kotecha D, Gill SK, Flather MD, Holmes J, Packer M, Rosano G, et al. Impact of renal impairment on beta-blocker efficacy in patients with heart failure. J Am Coll Cardiol. 2019;74(23):2893–904. https://doi.org/10.1016/j.jacc.2019.09.059.
Rangaswami J, McCullough PA. Heart failure in end-stage kidney disease: pathophysiology, diagnosis, and therapeutic strategies. Semin Nephrol. 2018;38(6):600–17. https://doi.org/10.1016/j.semnephrol.2018.08.005.
Bhandari S, Ives N, Brettell EA, Valente M, Cockwell P, Topham PS, et al. Multicentre randomized controlled trial of angiotensin-converting enzyme inhibitor/angiotensin receptor blocker withdrawal in advanced renal disease: the STOP-ACEi trial. Nephrol Dial Transplant. 2016;31(2):255–61. https://doi.org/10.1093/ndt/gfv346.
McMurray JJ, Packer M, Desai AS, Gong J, Lefkowitz MP, Rizkala AR, et al. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N Engl J Med. 2014;371(11):993–1004. https://doi.org/10.1056/NEJMoa1409077.
McMurray JJV, Jackson AM, Lam CSP, Redfield MM, Anand IS, Ge J, et al. Effects of sacubitril-valsartan, versus valsartan, in women compared to men with heart failure and preserved ejection fraction: insights from PARAGON-HF. Circulation. 2019. https://doi.org/10.1161/CIRCULATIONAHA.119.044491.
Solomon SD, McMurray JJV, Anand IS, Ge J, Lam CSP, Maggioni AP, et al. Angiotensin–neprilysin inhibition in heart failure with preserved ejection fraction. N Engl J Med. 2019;381(17):1609–20. https://doi.org/10.1056/NEJMoa1908655.
Haynes R, Judge PK, Staplin N, Herrington WG, Storey BC, Bethel A, et al. Effects of sacubitril/valsartan versus Irbesartan in patients with chronic kidney disease. Circulation. 2018;138(15):1505–14. https://doi.org/10.1161/CIRCULATIONAHA.118.034818.
•• McMurray JJV, Solomon SD, Inzucchi SE, Kober L, Kosiborod MN, Martinez FA, et al. Dapagliflozin in patients with heart failure and reduced ejection fraction. N Engl J Med. 2019;381(21):1995–2008. https://doi.org/10.1056/NEJMoa1911303. Among patients with heart failure and a reduced ejection fraction, the risk of worsening heart failure or death from cardiovascular causes was lower among those who received dapagliflozin than among those who received placebo, regardless of the presence or absence of diabetes.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors of this article declare that they have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Cardiovascular Care
Rights and permissions
About this article

Cite this article
Duraes, A.R., da Silva, W.A.P., Filho, C.R.H. et al. Heart Failure and Comorbidities—Part 2. Curr Emerg Hosp Med Rep 8, 69–75 (2020). https://doi.org/10.1007/s40138-020-00211-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40138-020-00211-8