
Abstract
Purpose of Review
To review recent surgical advances in the treatment of human papillomavirus (HPV)-related oropharyngeal squamous cell carcinoma (OPSCC), specifically focusing on treatment strategies, patient outcomes, and surgical technologies.
Recent Findings
Transoral robotic surgery (TORS) has become the surgical technique of choice when treating HPV-OPSCC. Patient-reported outcomes and functional outcomes are increasingly becoming drivers of treatment selection given the excellent prognosis of low-risk HPV-OPSCC. Decreased doses of adjuvant radiation therapy for select patients have been shown to be oncologically safe while offering the potential for improved functional outcomes. Neoadjuvant chemotherapy and immunotherapy have been shown to be safe in this patient population and may offer an advantage to up-front surgery. Finally, new data has identified circulating tumor HPV DNA (ctHPVDNA) as a promising biomarker of response to treatment in HPV-OPSCC.
Summary
The treatment of HPV-OPSCC continues to evolve with surgery playing an increasingly important role. De-escalation of adjuvant treatment for select patients provides excellent oncologic control with the potential for decreased long-term toxicity and remains an area of ongoing investigation. Neoadjuvant therapy (chemotherapy and/or immunotherapy) and or biomarker-driven adjuvant therapy may play a significant role in future treatment paradigms using surgery.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The incidence of human papilloma virus (HPV)-related squamous cell carcinoma (SCC) of the head and neck continues to rise in the USA and globally [1]. While HPV-related SCC can affect multiple subsites within the head and neck, the oropharynx is most affected. In addition, oropharyngeal squamous cell carcinoma (OPSCC) is now the most common malignancy caused by HPV in the USA [2, 3]. Patients diagnosed with HPV-OPSCC are typically younger, have fewer medical comorbidities, and enjoy more favorable oncologic outcomes when compared to their HPV-negative counterparts [4]. Collectively, these data prompted a change in the American Joint Committee on Cancer (AJCC) classification of patients with HPV-OPSCC [5].
The treatment landscape for patients with OPSCC has shifted over the last two decades in parallel with the epidemiologic shift from HPV-negative to positive. Surgery re-emerged as an important treatment modality, due primarily to the advent of transoral robotic surgery (TORS) [6, 7]. TORS affords improved access and visualization of the oropharynx, which equates to less surgical morbidity [6, 8]. This technology continues to evolve. The increased use of surgery for low-risk HPV-OPSCC has led to questions about traditional adjuvant radiation therapy (RT) paradigms including delivery technique and dosage de-escalation [9,10,11]. Given the improved prognosis of HPV-OPSCC, and the increased understanding of long-term side effects from treatment, functional and patient reported outcomes (PROs) have become an area of growing interest [12••, 13].
This review aims to discuss recent literature on surgical advances in the treatment of HPV-OPSCC, including the rationale for primary surgery, advanced robotic technology, adjuvant treatment de-escalation, neoadjuvant systemic therapy, the importance of functional outcomes, and the future directions of treatment including biomarker-driven treatment.
Increased Application of TORS
Traditionally, resection of oropharyngeal tumors required extended surgical approaches including mandibulotomy or transcervical lateral pharyngotomy [14, 15]. While these approaches afforded excellent exposure, they also carried substantial morbidity, including fistula formation, malunion, and hardware exposure [16]. In an effort to mitigate morbidity, surgeons advocated for less invasive transoral approaches which were often limited by a lack of exposure [17]. Both TORS and transoral laser microsurgery (TLM) emerged as techniques to gain better access to the upper aerodigestive tract [18]. TORS has emerged as the most widely used approach to resection of oropharyngeal tumors [19] and patients treated with TORS have better overall survival compared to patients treated with non-robotic surgery [20]. Since the Food and Drug Administration (FDA) approval in 2009, TORS has become increasingly popular. A recent National Cancer Database (NCDB) study demonstrated a 31% increase in the use of TORS from 2009 to 2016, with 1045 patients undergoing the procedure in the USA alone in 2016 [21]. Likewise, from 2010 to 2015, the use of TORS for early-stage OPSCC increased from 18 to 36% [22]. Additional data demonstrates that the increased utilization of TORS is not unique to the USA [23, 24], though broader adoption has been tempered by regional treatment differences, cost, and training prohibitions [25].
Rationale for Primary Surgery
The prognosis of early-stage HPV-OPSCC is excellent [26] and comparable between primary surgical and non-surgical approaches [27]. A fundamental goal of a primary surgical approach is to avoid the known long-term sequela from traditional chemoradiation (CRT) [28, 29, 30•, 31]. While some patients treated with primary surgery for HPV-OPSCC can avoid RT altogether, many will require adjuvant therapy. Lower RT doses and the selective application of chemotherapy in the adjuvant setting are intended to help reduce long-term side effects and improve patient functional outcomes [32]. Careful patient selection remains paramount to the application of surgery for HPV-OPSCC and there are many factors involved in determining the appropriate treatment choice for an individual [33].
Advances in Robotic Technology
The first robotic head and neck surgical procedure in a human was performed in 2005, with the excision of a vallecular cyst at Walter Reed Medical Center [34]. The next year, investigators at the University of Pennsylvania first described the feasibility of TORS for malignant base of tongue tumors [35]. A prospective trial then led to FDA approval in 2009 [36, 37]. The robotic technology used in these early procedures was the da Vinci Surgical System (Intuitive Surgical, Inc., Sunnyvale, California). This device was initially designed for thoracic and abdominal procedures and was FDA approved in 2000 for general laparoscopic surgery before it was utilized in the head and neck. Since then, this technology has continued to evolve. Most recently, the da Vinci SP (single port) was approved for transoral surgery in 2019 and provides a unique advantage: all the components (three robotic arms and camera) are fed through a single 2.5-cm port, with distal articulation, including the camera, creating more favorable operating conditions and visualization [38].
In 2017, the FDA also approved the Flex System (Medrobotics, Raynham, Massachusetts) specifically for use in the head and neck. The main difference between the Flex robot and da Vinci system is that the surgical “arms” are flexible laparoscopic-like arms placed through ports adjacent to a flexible camera system. Studies have shown favorable results when using the Flex System [39], though the future of this device remains uncertain.
Adjuvant Treatment De-escalation
Given the baseline high expectation of cure for HPV-OPSCC, treatment de-escalation has been a heavy area of clinical research in recent years [9, 11, 40]. Recent phase II and phase III randomized trials have explored the role of de-escalated adjuvant RT in patients treated with curative-intent surgery [30•, 41••, 42••].
In 2019, investigators from the Mayo Clinic demonstrated excellent survival outcomes in a phase II trial using de-escalated adjuvant RT (DART), 30–36 Gy with chemotherapy in patients with HPV-OPSCC. To be included, patients had to have < 10 pack-year smoking history and have been treated with curative-intent surgery with negative margins. The study risk stratified patients based on primary tumor features and nodal status: Cohort A (n = 36), the intermediate-risk group, defined as patients with one or more risk factors including lymphovascular invasion, perineural invasion, involvement of 2 or more regional lymph nodes, and a lymph node > 3 cm in size or ≥ T3 primary tumor, and Cohort B (n = 43), the high-risk group, defined as patients with any extranodal extension (ENE). Cohort A patients received 30 Gy with concurrent docetaxel, Cohort B patients received the same treatment plus additional RT boost to the nodal levels with ENE to 36 Gy. The 2-year local regional control rate was 96%, comparable with historical controls treated with higher dose adjuvant RT [43]. Overall, the study showed extremely low rates of high-grade toxicity and favorable functional outcomes [30•].
More recently, investigators from the Mayo clinic reported their phase III results using DART compared to standard of care (SOC) adjuvant (C)RT [42••]. The study stratified patients by smoking status and excluded patients who were pT4 or needed > 2 resections to clear a margin. A total of 194 patients were enrolled: 79 into Cohort A (intermediate-risk) and 115 into Cohort B (high-risk). Patients were randomized 2:1 to DART versus SOC. The primary endpoint was grade ≥ 3 adverse events ≥ 3 months after RT. With a median follow-up of 25 months, the authors report excellent oncologic outcomes for intermediate risk patients: 2-year recurrence-free survival 100% (DART) vs. 93.3% (SOC). Overall, oncologic outcomes were also favorable for high-risk patients with ENE: 2-year recurrence-free survival 92.2% (DART) vs. 100% (SOC). Importantly, the authors identified the patients at greatest risk of failure. Patients with ENE and pN2 disease demonstrated worse progression-free survival at 2 years: 42.9% (DART) vs. 100% (SOC).
The results of ECOG 3311, a multi-site phase II randomized trial of de-escalated adjuvant therapy, were also recently published [41••]. This study included 495 patients who underwent transoral curative-intent surgery for HPV-OPSCC and stratified patients into low-, intermediate-, and high-risk groups for adjuvant therapy de-escalation. The primary outcome was 2-year progression-free survival. In Arm A (n = 38), low-risk patients with negative margins, N0-N1 and no ENE were observed. Intermediate-risk patients with either close margins (< 3 mm), 2–4 positive nodes, ≤ 1 mm ENE, PNI or LVI were randomized to either Arm B (n = 100) and treated with 50 Gy adjuvant RT or Arm C (n = 108) 60 Gy RT. In Arm D (n = 113), high-risk patients with positive margins, > 1 mm ENE or 5 + positive nodes and were treated with 66 Gy cisplatin-based CRT. The authors found no difference in 2-year progression-free survival between intermediate-risk patients who received 50 Gy vs. 60 Gy of adjuvant RT (95% and 96%, respectively). Additionally, there was a trend towards better swallow outcomes using MD Anderson Dysphagia Index (MDADI) in Arm B, though the study was not powered sufficiently to detect a meaningful difference. These data show that reduced-dose adjuvant RT (50 Gy) is oncologically safe in patients with intermediate-risk HPV-OPSCC.
Successful de-escalation of treatment for low-risk HPV-OPSCC includes the judicious use of chemotherapy in the adjuvant setting. The management of “microscopic” ENE (generally defined as ≤ 2 mm) after surgery for HPV-OPSCC remains an area of ongoing debate. In contrast to HPV-negative OPSCC and oral cavity SCC where ENE has been shown to be prognostic, ENE is specifically excluded from the AJCC classification system for HPV-OPSCC. That is because the data supporting the addition of chemotherapy to postoperative RT for patients with either ENE or positive surgical margins was derived in the pre-HPV era, primarily from oral cavity SCC patients and did not distinguish between micro and macroscopic ENE [44,45,46]. Despite the lack of evidence, the use of adjuvant chemoradiation after surgery remains common, and is frequently extrapolated to lower risk HPV-OPSCC [47]. In patients with stage I HPV-OPSCC (AJCC 8) with intermediate-risk (2–4 positive nodes, microscopic ENE, or lymphovascular invasion), overall survival (OS) is similar regardless of whether or not patients receive adjuvant chemotherapy [48].
Cumulatively, current data suggest that de-escalation of adjuvant treatment is oncologically sound for well-selected patients treated surgically for HPV-OPSCC. Careful patient selection and pathologic risk stratification are imperative to the successful application of TORS for HPV-OPSCC. There is more work to be done to further our understanding of which patients can be safely treated with de-escalation strategies.
Neoadjuvant Chemotherapy
The utility of chemotherapy prior to planned surgical resection in HPV-OPSCC is a potentially useful, but largely untested option [49]. While “induction” chemotherapy has never been shown to improve survival in HPV-negative SCC, clinical application varies widely among institutions [50]. Indeed, the very definition of “induction” chemotherapy is not standardized and is often used interchangeably with “neoadjuvant” chemotherapy [51]. Some advocate for the term “neoadjuvant” chemotherapy when used prior to planned definitive surgery, and “induction” chemotherapy when used prior to planned RT.
Proponents of neoadjuvant chemotherapy in patients with HPV-OPSCC note that up to 50% of treatment failures are distant-only [52•]. Importantly, neoadjuvant chemotherapy has been shown to reduce the need for adjuvant RT [29]. In a phase II trial of 55 patients, 72% of patients had a pathologic complete response (pCR) at the primary site, while 44% of patients had a pCR at both the primary site and the neck [52•]. In that study, patients were treated with docetaxel plus cisplatin-based chemotherapy followed by TORS with adjuvant radiotherapy reserved for patients with 4 + positive nodes, positive margins, or “macroscopic” (> 2 mm) ENE on final pathology. Oncologic and functional outcomes compared favorably to CRT; 5-year disease-free survival was 96.1% and no patients required a feeding tube [52•]. Based on these data, there is an ongoing phase II clinical trial (NCT04277858). Neoadjuvant chemotherapy has also been applied to more advanced OPSCC treated surgically with favorable oncologic and functional outcomes [53, 54].
Immunotherapy
In recent years, immunotherapy has been added to the repertoire of treatment for patients with HNSCC and is now the standard of care for patients with recurrent, unresectable and/or metastatic disease [55, 56]. Phase III clinical trials have established the benefit of PD-1 receptor inhibitors as superior to cytotoxic chemotherapy for patients in the advanced unresectable and metastatic setting [57,58,59]. In addition to PD-1 receptor inhibitors, FDA approved since 2016, other immune checkpoint inhibitors including cytotoxic T lymphocyte antigen 4 (CTLA-4) receptor inhibitors have also been shown to play a role in immune response to HNSCC [60].
Given the successes observed in advanced HNSCC, recent work has focused on the application of immunotherapy in earlier stage disease, including HPV-OPSCC [61•]. In CheckMate 358, neoadjuvant nivolumab was well tolerated in previously untreated, resectable OPSCC (30% grade ≥ 3 treatment-related adverse events). Nearly a quarter of patients with HPV-OPSCC experienced a partial pathologic response [61•].
A high density of CD8-positive tumor-infiltrating lymphocytes portends improved prognosis in patients with OPSCC [62]. Based on this principle, combination PD-L1 and CTLA-4 inhibition was applied in the neoadjuvant setting for OPSCC in a recent study [63•]. A total of 28 patients were included and the majority (86%) had HPV-OPSCC. Combination neoadjuvant immunotherapy was found to be well-tolerated and induced a major pathologic response at both the primary site and the neck in 7%, and in the lymph nodes only in 21% [63•]. Additionally, neoadjuvant immunoradiotherapy has been tested in HPV-OPSCC. A recent phase Ib clinical trial evaluated treatment response in patients with locally advanced OPSCC treated with neoadjuvant SBRT with or without nivolumab prior to definitive surgery, followed by adjuvant nivolumab. Investigators found major pathologic responses in 86% and pCR in 67% of patients, respectively [64]. Taken together, these studies indicate that neoadjuvant immunotherapy is safe and feasible in patients with HPV-OPSCC.
Future Directions
Functional Outcomes
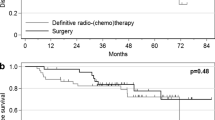
HPV-OPSCC has been shown to affect younger and healthier patients. With a cure rate exceeding 90% in many scenarios regardless of primary treatment modality, focus is shifting towards functional outcomes and PROs [4, 27, 65]. Prior research has demonstrated decreased gastrostomy tube rates in HPV-OPSCC patients treated with TORS [66]. In 2019, a multicenter randomized phase II trial (ORATOR) was the first to compare primary RT versus transoral surgery for OPSCC [12••]. Given previous data that demonstrated similar oncologic outcomes between primary RT and surgery, the authors chose quality of life measures as their primary outcome (MDADI scores at 12 months). A total of 68 patients were randomly assigned to either RT or transoral surgery plus neck dissection. With a median follow-up > 2 years, the RT cohort started with better baseline MDADI scores and demonstrated statistically superior MDADI scores over time, although the differences did not meet the pre-determined 10-point threshold to qualify as a clinically meaningful change and have decreased with long-term follow-up [12••, 67]. Notably in that study, TORS patients routinely underwent prophylactic tracheostomy after a bleeding death was observed. The majority of patients in the trial were treated with multimodality therapy. Nonetheless, the authors conclude that primary RT offers superior swallowing-related QOL.
As a follow-up to the ORATOR trial, results from the ORATOR 2 trial were recently presented [68••]. This follow-up prospective randomized trial was designed to test the contemporary non-surgical and surgical de-intensification strategies in low-risk HPV-OPSCC. The results were presented early after two treatment-related deaths in the surgical arm led to premature closure of the trial. The primary endpoint of the study was overall survival, compared separately for each arm against historical controls. While ORATOR2 planned to accrue 140 patients, the study was stopped early after enrolling just 61 patients. There was 1 death due to bleeding 4 days after surgery despite prophylactic tracheostomy and ipsilateral external carotid artery ligation, and 1 death due to cervical vertebral osteomyelitis approximately one month after completion of adjuvant RT. The unfortunate early closure of this trial underscores the importance of careful patient selection and rigorous surgical quality for HPV-OPSCC.
In contrast to ORATOR, a prospective cohort study including 257 TORS-eligible patients with low to intermediate risk HPV-OPSCC offered a more nuanced perspective [69]. In this study, objective functional swallowing outcomes (as measured by dynamic imaging grade of swallowing toxicity [DIGEST] scores) were compared between surgical and non-surgical patients in addition to subjective outcomes (MDADI). At 3–6 months post-treatment, the prevalence of moderate-severe dysphagia (DIGEST ≥ 2) among the TORS cohort was nearly half that of patients treated with primary RT. Patients treated with TORS alone demonstrated the best subjective and objective swallowing outcomes. In a separate prospective cohort study of 215 TORS-eligible patients treated with either intensity-modulated proton therapy (IMPT) or TORS for HPV-OPSCC, the authors similarly found that patients treated with TORS had better swallowing outcomes as measured by MDADI and DIGEST [70•]. The results held true for patients regardless of the number of treatment modalities. Taken together, these data demonstrate that careful patient selection and surgical quality can yield favorable swallowing outcomes for HPV-OPSCC patients treated with TORS.
Swallow outcomes are an incomplete measure of symptom burden for HPV-OPSCC patients, and thus far little attention has been given to long-term toxicity after treatment. In a study of longitudinal PROs (using MD Anderson Symptom Inventory – Head and Neck [MDASI-HN]) among patients treated surgically versus non-surgically, all patients were found to have improvements over time regardless of primary treatment modality. After 6 months, there was a marked improvement in MDASI-HN scores across the entire population. This study did shed light on different toxicity profiles between patients treated surgically (worse numbness, voice, choking and sleep symptoms) versus non-surgically (worse dry mouth, taste disturbances) in the acute post-treatment period [71]. Patients treated with multi-modality therapy had worse PROs. As such, adjuvant treatment de-escalation for postoperative patients plays a vital role in functional outcomes.
Biomarkers
A robust biomarker for HPV-OPSCC would have great clinical utility, and recent advances point towards a future using “liquid biopsy” techniques to assess treatment response and improve early detection. Circulating tumor DNA has been shown to assist in early detection of cancer recurrence in other sites [72, 73]. Recently, a prospective clinical trial monitoring for circulating tumor HPV DNA (ctHPVDNA) was conducted for patients with HPV-OPSCC. The authors found that for patients with undetectable ctHPVDNA, the negative predictive value for developing recurrence was 100%. Furthermore, in patients with 2 consecutive positive ctHPVDNA tests, the positive predictive value was 94%. These patients on average developed recurrence 4 months after the DNA was found circulating in the bloodstream [74]. Furthermore, next-generation DNA sequencing techniques have been applied to circulating tumor DNA detection in this setting and have been shown to outperform traditional digital polymerase chain reaction (PCR) techniques [75]. As this field evolves, earlier detection of recurrence is likely to result in improved survival outcomes [76, 77].
Conclusions
Surgery has made a resurgence as a viable primary treatment option for HPV-OPSCC and is increasingly utilized in part due to the continued evolution of TORS. In addition, adjuvant treatment de-escalation for select HPV-OPSCC patients has been shown to offer favorable oncologic and functional outcomes. With expected high cure rates regardless of primary treatment modality, PROs and functional outcomes play an increasingly important role in selecting the optimal treatment for individual patients. Neoadjuvant strategies have emerged with hopes of further de-escalation. Finally, HPV biomarkers will likely play a key role in the future direction of the field as the data expands.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Näsman A, Du J, Dalianis T. A global epidemic increase of an HPV-induced tonsil and tongue base cancer – potential benefit from a pan-gender use of HPV vaccine. J Intern Med. 2019;287(2):134–52.
HPV and Oropharyngeal Cancer. Division of Cancer Prevention and Control [Internet]. 2021. Available from: https://www.cdc.gov/cancer/hpv/basic_info/hpv_oropharyngeal.htm.
Van Dyne EA HS, Saraiya M, Thomas CC, Markowitz LE, Benard VB. Trends in human papillomavirus-associated cancers - United States, 1999–2015. MMWR Morb Mortal Wkly Rep [Internet]. 2018;67:[918–24 pp.].
Fakhry C, Westra WH, Li S, Cmelak A, Ridge JA, Pinto H, et al. Improved survival of patients with human papillomavirus-positive head and neck squamous cell carcinoma in a prospective clinical trial. J Natl Cancer Inst. 2008;100(4):261–9.
Amin MB ES, Greene F, Byrd DR, Brookland RK, Washington MK, Gershenwald JE, Compton CC, Hess KR, et al. AJCC Cancer Staging Manual. 8th ed: Springer International Publishing: Am Joint Comm Cancer. 2017.
Schmitt NC, Duvvuri U. Transoral robotic surgery for oropharyngeal squamous cell carcinoma. Curr Opin Otolaryngol Head Neck Surg. 2015;23(2):127–31.
Carnevale C, Ortiz-González I, Ortiz-González A, Bodi-Blanes L, Til-Pérez G. Early T1-T2 stage p16+ oropharyngeal tumours. Role of upfront transoral robotic surgery in de-escalation treatment strategies. A review of the current literature. Oral Oncol. 2021;113:105111.
Golusiński W, Golusińska-Kardach E. Current role of surgery in the management of oropharyngeal cancer. Front Oncol. 2019;9:388.
Iorio GC, Arcadipane F, Martini S, Ricardi U, Franco P. Decreasing treatment burden in HPV-related OPSCC: a systematic review of clinical trials. Crit Rev Oncol Hematol. 2021;160: 103243.
Moore EJ, Van Abel KM, Routman DM, Lohse CM, Price KAR, Neben-Wittich M, et al. Human papillomavirus oropharynx carcinoma: aggressive de-escalation of adjuvant therapy. Head Neck. 2021;43(1):229–37.
Gamez ME, Ma DJ. Deintensification strategies using proton beam therapy for HPV-related oropharyngeal cancer. International Journal of Particle Therapy. 2021;8(1):223–33.
•• Nichols AC, Theurer J, Prisman E, Read N, Berthelet E, Tran E, et al. Radiotherapy versus transoral robotic surgery and neck dissection for oropharyngeal squamous cell carcinoma (ORATOR): an open-label, phase 2, randomised trial. Lancet Oncol. 2019;20(10):1349–59. First randomized control trial to compare TORS vs primary RT and found that patients in the RT arm had better swallow function (though not clinically significant).
Fitzgerald CWR, Long SM, McLean AT, Cracchiolo JR. Patient-reported outcomes in human papillomavirus-related oropharyngeal cancer. J Surg Oncol. 2021;124(6):967–76.
Parsons JT, Mendenhall WM, Stringer SP, Amdur RJ, Hinerman RW, Villaret DB, et al. Squamous cell carcinoma of the oropharynx: surgery, radiation therapy, or both. Cancer. 2002;94(11):2967–80.
Gooris PJ, Worthington P, Evans JR. Mandibulotomy: a surgical approach to oral and pharyngeal lesions. Int J Oral Maxillofac Surg. 1989;18(6):359–64.
Dyalram-Silverberg D, Siavash H, Nasir S, Zhang T, Ord R, Lubek J. Complications of the lip split mandibulotomy: The University of Maryland Experience. Oral Maxillofac Surg. 2011;69(9).
Brickman D, Gross ND. Robotic approaches to the pharynx: tonsil cancer. Otolaryngol Clin North Am. 2014;47(3):359–72.
Holsinger FC, Ferris RL. Transoral endoscopic head and neck surgery and its role within the multidisciplinary treatment paradigm of oropharynx cancer: robotics, lasers, and clinical trials. J Clin Oncol. 2015;33(29):3285–92.
Lang S, Mattheis S, Kansy B. TORS in HPV-positive tumors-the new standard? Recent Results Cancer Res. 2017;206:207–18.
Chillakuru Y, Benito DA, Strum D, Mehta V, Saini P, Shim T, et al. Transoral robotic surgery versus nonrobotic resection of oropharyngeal squamous cell carcinoma. Head Neck. 2021;43(7):2259–73.
Gal TJ, Slezak JA, Kejner AE, Chen Q, Huang B. Treatment trends in oropharyngeal carcinoma: Surgical technology meets the epidemic. Oral Oncol. 2019;97:62–8.
Nguyen AT, Luu M, Mallen-St Clair J, Mita AC, Scher KS, Lu DJ, et al. Comparison of survival after transoral robotic surgery vs nonrobotic surgery in patients with early-stage oropharyngeal squamous cell carcinoma. JAMA Oncology. 2020;6(10).
Pongsapich W, Chongkolwatana C, Chuetnok H, Ratanaprasert N. The implementation of TORS for head and neck surgery in Thailand. J Robot Surg. 2021;15(6):955–61.
Lorincz BB, Jowett N, Knecht R. Decision management in transoral robotic surgery: Indications, individual patient selection, and role in the multidisciplinary treatment for head and neck cancer from a European perspective. Head Neck. 2016;38(Suppl 1):E2190–6.
Mandapathil M, Meyer JE. Acceptance and adoption of transoral robotic surgery in Germany. Eur Arch Otorhinolaryngol. 2021;278(10):4021–6.
Amini A, Jasem J, Jones BL, Robin TP, McDermott JD, Bhatia S, et al. Predictors of overall survival in human papillomavirus-associated oropharyngeal cancer using the National Cancer Data Base. Oral Oncol. 2016;56:1–7.
Yeh DH, Tam S, Fung K, MacNeil SD, Yoo J. Winquist E et al Transoral robotic surgery vs radiotherapy for management of oropharyngeal squamous cell carcinoma a systematic review of the literature. Eur J Surg Oncol. 2015;41(12):1603–14.
Feng AL, Holcomb AJ, Abt NB, Mokhtari TE, Suresh K, McHugh CI, et al. Feeding tube placement following transoral robotic surgery for oropharyngeal squamous cell carcinoma. Otolaryngol Head Neck Surg. 2021:1945998211020302.
Sadeghi N, Li NW, Taheri MR, Easley S, Siegel RS. Neoadjuvant chemotherapy and transoral surgery as a definitive treatment for oropharyngeal cancer: a feasible novel approach. Head Neck. 2016;38(12):1837–46.
• Ma DJ, Price K, Moore EJ, Patel SH, Hinni ML, Chintakuntlawar AV, et al. Two-year results for MC1273, a phase 2 evaluation of aggressive dose de- escalation for adjuvant chemoradiation in HPV+ oropharynx squamous cell carcinoma (OPSCC). Int J Radiat Oncol *Biology*Phys. 2017;99(5):1320. Found that reduced-dose adjuvant CRT demonstrated locoregional control rate similar to historical controls while improving quality of life.
Machtay M, Moughan J, Trotti A, Garden AS, Weber RS, Cooper JS, et al. Factors associated with severe late toxicity after concurrent chemoradiation for locally advanced head and neck cancer: an RTOG analysis. J Clin Oncol. 2008;26(21):3582–9.
Zakeri K, Dunn L, Lee N. HPV-associated oropharyngeal cancer de-escalation strategies and trials: Past failures and future promise. J Surg Oncol. 2021;124(6):962–6.
Berger MH, Yasaka TM, Haidar YM, Kuan EC, Tjoa T. Insurance status as a predictor of treatment in human papillomavirus positive oropharyngeal cancer. Laryngoscope. 2021;131(4):776–81.
McLeod IK, Melder PC. Da Vinci robot-assisted excision of a vallecular cyst: a case report. Ear Nose Throat J. 2005;84(3):170–2.
O’Malley BW Jr, Weinstein GS, Snyder W, Hockstein NG. Transoral robotic surgery (TORS) for base of tongue neoplasms. Laryngoscope. 2006;116(8):1465–72.
Weinstein GS, O’Malley BW Jr, Snyder W, Sherman E, Quon H. Transoral robotic surgery: radical tonsillectomy. Archives of Otolaryngology-Head & Neck Surgery. 2007;133(12):1220–6.
Weinstein GS, O’Malley BW Jr, Magnuson JS, Carroll WR, Olsen KD, Daio L, et al. Transoral robotic surgery: a multicenter study to assess feasibility, safety, and surgical margins. Laryngoscope. 2012;122(8):1701–7.
Intuitive Surgical Announces Innovative Single Port Platform - the da Vinci SP Surgical System. 2018. https://isrg.gcs-web.com/news-releases/news-release-details/intuitive-surgical-announces-innovative-single-port-platform-da
Lang S, Mattheis S, Hasskamp P, Lawson G, Güldner C, Mandapathil M, et al. A european multicenter study evaluating the flex robotic system in transoral robotic surgery. Laryngoscope. 2017;127(2):391–5.
Ma DJ, Van Abel KM. Treatment de-intensification for HPV-associated oropharyngeal cancer: a definitive surgery paradigm. Semin Radiat Oncol. 2021;31(4):332–8.
•• Ferris RL, Flamand Y, Weinstein GS, Li S, Quon H, Mehra R, et al. Transoral robotic surgical resection followed by randomization to low- or standard-dose IMRT in resectable p16+ locally advanced oropharynx cancer: A trial of the ECOG-ACRIN Cancer Research Group (E3311). J Clin Oncol. 2020;38(15_suppl):6500. Demonstrated that reduced-dose adjuvant RT to 50Gy is oncologically safe in intermediate-risk patients with HPV-OPSCC.
•• Ma DM, Price K, Moore EJ, Patel SH, Hinni ML, Fruth B, et al. MC1675, a phase III evaluation of de-escalated adjuvant radiation therapy (DART) vs. standard adjuvant treatment for human papillomavirus associated oropharyngeal squamous cell carcinoma. Int J Radiat Oncol *Biology*Physics. 2021;111(5):1324. Showed that patients with ENE and pN2 disease had worse progression-free survival.
Harari PM, Harris J, Kies MS, Myers JN, Jordan RC, Gillison ML, et al. Postoperative chemoradiotherapy and cetuximab for high-risk squamous cell carcinoma of the head and neck: Radiation Therapy Oncology Group RTOG-0234. J Clin Oncol. 2014;32(23):2486–95.
Bernier J, Domenge C, Ozsahin M, Matuszewska K, Lefèbvre JL, Greiner RH, et al. Postoperative irradiation with or without concomitant chemotherapy for locally advanced head and neck cancer. N Engl J Med. 2004;350(19):1945–52.
Cooper JS, Pajak TF, Forastiere AA, Jacobs J, Campbell BH, Saxman SB, et al. Postoperative concurrent radiotherapy and chemotherapy for high-risk squamous-cell carcinoma of the head and neck. N Engl J Med. 2004;350(19):1937–44.
Bernier J, Cooper JS, Pajak TF, van Glabbeke M, Bourhis J, Forastiere A, et al. Defining risk levels in locally advanced head and neck cancers: a comparative analysis of concurrent postoperative radiation plus chemotherapy trials of the EORTC (#22931) and RTOG (# 9501). Head Neck. 2005;27(10):843–50.
Trifiletti DM, Smith A, Mitra N, Grover S, Lukens JN, Cohen RB, et al. Beyond positive margins and extracapsular extension: evaluating the utilization and clinical impact of postoperative chemoradiotherapy in resected locally advanced head and neck cancer. J Clin Oncol. 2017;35(14):1550–60.
Cramer JD, Hicks KE, Rademaker AW, Patel UA, Samant S. Validation of the eighth edition American Joint Committee on Cancer staging system for human papillomavirus associated oropharyngeal cancer. Head Neck. 2018;40(3):457–66.
Sher DJ, Schwartz DL, Nedzi L, Khan S, Hughes R, Fidler MJ, et al. Comparative effectiveness of induction chemotherapy for oropharyngeal squamous cell carcinoma: a population-based analysis. Oral Oncol. 2016;54:58–67.
Strohl MP, Wai KC, Ha PK. De-intensification strategies in HPV-related oropharyngeal squamous cell carcinoma-a narrative review. Ann Transl Med. 2020;8(23):1601.
Devisetty K, Wong SJ. Neoadjuvant versus induction chemotherapy: more than semantics. J Clin Oncol. 2013;31(23):2971–2.
• Sadeghi N, Khalife S, Mascarella MA, Ramanakumar AV, Richardson K, Joshi AS, et al. Pathologic response to neoadjuvant chemotherapy in HPV-associated oropharynx cancer. Head Neck. 2020;42(3):417–25. Demonstrated success with neoadjuvant chemotherapy followed by TORS with avoidance of adjuvant RT in select patients, resulting in excellent DFS and swallowing outcomes.
Park YM, Jung CM, Cha D, Kim DH, Kim HR, Keum KC, et al. A new clinical trial of neoadjuvant chemotherapy combined with transoral robotic surgery and customized adjuvant therapy for patients with T3 or T4 oropharyngeal cancer. Ann Surg Oncol. 2017;24(11):3424–9.
Lee E, Gorelik D, Crowder HR, Badger C, Schottler J, Li NW, et al. Swallowing function following neoadjuvant chemotherapy and transoral robotic surgery for oropharyngeal carcinoma: a 2-year follow-up. Otolaryngol Head Neck Surg. 2021:1945998211057430.
Cramer JD, Burtness B, Ferris RL. Immunotherapy for head and neck cancer: recent advances and future directions. Oral Oncol. 2019;99: 104460.
Nanda R, Chow LQ, Dees EC, Berger R, Gupta S, Geva R, et al. Pembrolizumab in patients with advanced triple-negative breast cancer: phase Ib KEYNOTE-012 Study. J Clin Oncol. 2016;34(21):2460–7.
Yen CJ, Kiyota N, Hanai N, Takahashi S, Yokota T. Iwae S et al Two-year follow-up of a randomized phase III clinical trial of nivolumab vs the investigator’s choice of therapy in the Asian population for recurrent or metastatic squamous cell carcinoma of the head and neck (CheckMate 141). Head Neck. 2020;42(10):2852–62.
Cohen EEW, Machiels J-PH, Harrington KJ, Burtness B, Shin SW, Gause CK, et al. KEYNOTE-040: a phase III randomized trial of pembrolizumab (MK-3475) versus standard treatment in patients with recurrent or metastatic head and neck cancer. Journal of Clinical Oncology. 2015;33(15_suppl):TPS6084-TPS.
Burtness B, Harrington KJ, Greil R, Soulières D, Tahara M, de Castro Jr G, Psyrri A, Basté N, Neupane P, Bratland Å, Fuereder T. Pembrolizumab alone or with chemotherapy versus cetuximab with chemotherapy for recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-048): a randomised, open-label, phase 3 study. Lancet. 2019;394(10212):1915–28.
Hecht M, Gostian AO, Eckstein M, Rutzner S, von der Grün J, Illmer T, et al. Safety and efficacy of single cycle induction treatment with cisplatin/docetaxel/ durvalumab/tremelimumab in locally advanced HNSCC: first results of CheckRad-CD8. J Immunother Cancer. 2020;8(2).
• Ferris RL, Spanos WC, Leidner R, Gonçalves A, Martens UM, Kyi C, et al. Neoadjuvant nivolumab for patients with resectable HPV-positive and HPV-negative squamous cell carcinomas of the head and neck in the CheckMate 358 trial. J Immunother Cancer. 2021;9(6):e002568. Found that neoadjuvant immunotherapy was safe in HPV-OPSCC.
Solomon B, Young RJ, Bressel M, Urban D, Hendry S, Thai A, et al. Prognostic significance of PD-L1(+) and CD8(+) immune cells in HPV(+) oropharyngeal squamous cell carcinoma. Cancer Immunol Res. 2018;6(3):295–304.
• Ferrarotto R, Bell D, Rubin ML, Hutcheson KA, Johnson JM, Goepfert RP, et al. Impact of neoadjuvant durvalumab with or without tremelimumab on CD8(+) tumor lymphocyte density, safety, and efficacy in patients with oropharynx cancer: CIAO Trial Results. Clin Cancer Res. 2020;26(13):3211–9. Demonstrated that neoadjuvant immunotherapy was safe in HPV-OPSCC.
Leidner R, Crittenden M, Young K, Xiao H, Wu Y, Couey MA, et al. Neoadjuvant immunoradiotherapy results in high rate of complete pathological response and clinical to pathological downstaging in locally advanced head and neck squamous cell carcinoma. J Immunother Cancer. 2021;9(5): e002485.
Ang KK, Harris J, Wheeler R, Weber R, Rosenthal DI, Nguyen-Tan PF, et al. Human papillomavirus and survival of patients with oropharyngeal cancer. N Engl J Med. 2010;363(1):24–35.
Heah H, Goepfert RP, Hutcheson KA, Garden AS, Gunn GB, Fuller CD, et al. Decreased gastrostomy tube incidence and weight loss after transoral robotic surgery for low- to intermediate-risk oropharyngeal squamous cell carcinoma. Head Neck. 2018;40(11):2507–13.
Hutcheson KA, Barrow MP, Lisec A, Barringer DA, Gries K, Lewin JS. What is a clinically relevant difference in MDADI scores between groups of head and neck cancer patients? Laryngoscope. 2016;126(5):1108–13.
•• Palma D NA. A phase II randomized trial of treatment de-escaation for HPV associated oropharyngeal squamous cell carcinoma: radiotherapy vs. trans-oral surgery (ORATOR 2). 2021. Demonstrated that reduce-dose primary RT demonstrated better OS when compared to patients treated with TORS + reduced-dose RT.
Hutcheson KA, Warneke CL, Yao C, Zaveri J, Elgohari BE, Goepfert R, et al. Dysphagia after primary transoral robotic surgery with neck dissection vs nonsurgical therapy in patients with low- to intermediate-risk oropharyngeal cancer. JAMA Otolaryngol Head Neck Surg. 2019;145(11):1053–63.
• Barbon CE, Peterson CB, Dirba DD, Gunn GB, Frank SJ, Ferrarotto R, et al. Comparison of prospective, longitudinal swallowing function after primary intensity-modulated proton therapy (IMPT) or transoral robotic surgery (TORS) for oropharyngeal squamous cell carcinoma. Int J Radiat Oncol *Biology* Phys. 2020;108(3, Supplement):S160. Demonstrated improved swallowing outcomes in patients treated with TORS versus IMPT.
Amit M, Hutcheson K, Zaveri J, Lewin J, Kupferman ME, Hessel AC, et al. Patient-reported outcomes of symptom burden in patients receiving surgical or nonsurgical treatment for low-intermediate risk oropharyngeal squamous cell carcinoma: a comparative analysis of a prospective registry. Oral Oncol. 2019;91:13–20.
Cullinane C, Fleming C, O’Leary DP, Hassan F, Kelly L, O’Sullivan MJ, et al. Association of circulating tumor DNA with disease-free survival in breast cancer: a systematic review and meta-analysis. JAMA Network Open. 2020;3(11):e2026921.
Zhang J, Dai D, Tian J, Li L, Bai J, Xu Y, et al. Circulating tumor DNA analyses predict disease recurrence in non-muscle-invasive bladder cancer. Front Oncol. 2021;11.
Chera BS, Kumar S, Shen C, Amdur R, Dagan R, Green R, et al. Plasma circulating tumor HPV DNA for the surveillance of cancer recurrence in HPV-associated oropharyngeal cancer. J Clin Oncol. 2020;38(10):1050–8.
Rungkamoltip P, Temisak S, Piboonprai K, Japrung D, Thangsunan P, Chanpanitkitchot S, et al. Rapid and ultrasensitive detection of circulating human papillomavirus E7 cell-free DNA as a cervical cancer biomarker. Exp Biol Med. 2021;246(6):654–66.
Routman DM, Kumar S, Chera BS, Jethwa KR, Van Abel KM, Frechette K, et al. Detectable Postoperative circulating tumor human papillomavirus (HPV) DNA and association with recurrence in patients with HPV-associated oropharyngeal squamous cell carcinoma. Int J Radiat Oncol *Biology* Phys. 2022.
O'Boyle CJ, Siravegna G, Varmeh S, Queenan N, Michel A, Pang KCS, et al. Cell-free human papillomavirus DNA kinetics after surgery for human papillomavirus–associated oropharyngeal cancer. Cancer.n/a(n/a).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Dr. Mulcah declares no conflicts of interest. Dr. Gross reports grants and personal fees from Regeneron, personal fees from Sanofi-Genzyme (Ad hoc Scientfic Advisory Board), personal fees from Shattuck Labs (Ad hoc Scientfic Advisory Board), personal fees from PDS Biotechnology (Scientfic Advisory Board), personal fees from Intuitive Surgical, and personal fees from DragonFly Therapeutics, outside the submitted work.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Head and Neck: Human Papilloma Virus Associated Head and Neck Squamous Cell Carcinoma
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Mulcahy, C.F., Gross, N.D. Advances in Surgical Therapy for HPV-Associated Squamous Cell Carcinoma. Curr Otorhinolaryngol Rep 10, 475–482 (2022). https://doi.org/10.1007/s40136-022-00421-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40136-022-00421-6