
Abstract
Purpose of Review
Imaging modalities useful in the contemporary evaluation of salivary gland disorders are discussed.
Recent Findings
Salivary gland ultrasound—due to its wide applicability, versatility, availability, and low cost—is supported as a frontline evaluation and is frequently done as an in-office procedure by the treating surgeon. Contrast-enhanced CT may be as accurate as non-contrast CT in detecting sialolithiasis. Although conventional sialography (fluoroscopic salivary gland evaluation with ductal dilation and radiocontrast insufflation) was initially designed as a diagnostic procedure, more recently, reported experience has demonstrated it to result in improved salivary function for several disorders—including its use as treatment of juvenile recurrent parotitis. Conventional sialography remains the most accurate method to assess the full ductal anatomy and is superior to MRI sialography which fails to adequately image the more proximal ducts. For benign salivary tumors, US may obviate the need for further imaging and provide reliable estimation of tumor location.
Summary
Salivary gland disorders are most efficiently imaged with in-office ultrasound. In settings where US cannot be performed, CT (with or without contrast) remains a reliable initial method to detect salivary gland abnormalities including sialolithiasis. MR sialography has become a useful modality for evaluating stenosis and may be considered when conventional sialography is not available.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The diagnostic modalities available for salivary gland imaging include plain radiography, ultrasonography (US), computed tomography (CT), magnetic resonance imaging (MRI), and sialography. The unique physics of each modality and the varied pathologies that affect the salivary gland impact the selection of modality as is determined by the clinical scenario. Although no single salivary imaging modality is superior to another across most clinical scenarios, we emphasize initial screening with ultrasound as the initial method of evaluation in most cases.
Ultrasound
Salivary gland ultrasound (SGUS) as performed by surgeons for the assessment of salivary pathologies outside of the radiology department has increased in recent years. When performed at the initial visit in systematic fashion, US functions as an extension of the physical exam [1]. In many cases, surgeon-performed US may eliminate the need for further imaging studies to reduce the number of clinic visits between initial presentation and definitive treatment and additionally avoid patient exposure to ionizing radiation.
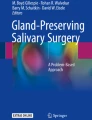
US is a dynamic imaging modality whose performance may be enhanced by examination techniques such as citric acid provocation and sonopalpation. By giving the patient a small amount of citric acid on the tongue, salivation is stimulated to dilate ductal structures which may serve to make obstructive pathology more apparent. Sonopalpation involves the clinician using their non-scanning hand to palpate and maneuver tissues during real-time sonographic examination. This process increases the sensitivity of US for the identification of sialoliths (Fig. 1) [2].

Ultrasound of the right submandibular/floor of the mouth region. Sonopalpation allows for definite characterization of the calculus by both palpation and visualization. The green arrow points to the hyperechoic line of the examiner’s glove. The red arrow points to the deep hyperechoic line of the calculus. Posterior acoustic shadowing is present. The blue arrow points to the dilated Wharton’s duct proximal to the calculus
US also complements other diagnostic methods. For example, the diagnostic yield of fine-needle aspiration biopsies (FNAB) is improved with the addition of US [3]. Salivary US may be used simultaneously with intraductal manipulations including sialendoscopy and duct dilation. This hybrid assessment enables direct visualization and treatment of pathology via the sialendoscope while ultrasound clarifies the location of the sialendoscope relative to anatomic structures not directly visualized on endoscopy (Fig. 2).

Sialendoscope seen within the parotid duct on intraoperative ultrasound
Limitations to US include difficulty in visualizing structures and pathology within the deep lobe of the parotid gland—largely due to shadowing by the mandible. Structures within the superficial floor of the mouth may be difficult to fully assess on external sonography due to the interface between air and soft tissue. This limitation may be overcome through sonopalpation. Enlarged body habitus may be a limitation to the ultrasound examination as the presence of excess subcutaneous fat and subfascial fat can preclude accurate assessment of deeper structures. The presence of facial hair may further degrade imaging despite liberal application of gel.
Salivary US identifies a normal gland as one with hyperechoic and homogeneous echo characteristics and well-defined borders. Stensen’s and Wharton’s ducts are usually not identified in a normal gland unless enhancement with citric acid or another salivary stimulate is used to temporarily increase duct dimensions during salivary. The degree of echogenicity of the gland parenchyma is rated as hyper-, iso-, or hypoechoic relative to the nearby musculature.
A thorough sonographic assessment of the salivary glands should generally note the overall size of the gland, parenchyma echotexture, the absence or presence of ductal dilation, the presence of hyperechoic foci, vascularity, and the presence of lymph nodes or masses within the gland of interest. A critical evaluation of ultrasound reliability by blinded experts assessing normal glands and those affected by Sjogren’s syndrome found consistency only in the reporting of echogenicity (hyper-/hypo-) and homogeneity [4]. These investigators reported “substantial” interobserver reliability for homogeneity and location of hypechoic/anechoic areas and moderate for echogenicity and normal lymph nodes in the parotid. Other “core items” in reporting (hyperechoic bands, calcifications, identified posterior border) were less consistent for the parotid gland but still leading to the “advised diagnosis reliability” as “substantial.” The interobserver consistency in evaluating the submandibular glands was not as good and led to the “advised diagnostic reliability” graded as “moderate.”
It is widely recognized that the quality of salivary gland US is largely dependent on operator technique and that with practice accuracy and consistency will improve. It is possible that for this reason, US is demonstrated in the literature to have a wide range of sensitivity when compared to CT for the detection of sialolithiasis (65–97%) [2, 5, 6].
CT and Cone Beam CT
Standard CT is fast, relatively low cost, widely available throughout the USA, and the most ordered study for evaluation of the sublingual, submandibular, and parotid gland pathology [7]. It is approximately tenfold more sensitive than plain film radiography in the detection of sialoliths and is useful additionally in evaluating the gland parenchyma for other abnormalities including infection, adenopathy, and tumor. However, CT imaging is less sensitive than ultrasound or sialography in detecting ductal dilation or strictures and has been reported to fail to image non-radiopaque stones [8,10,10]. Exposure to ionizing radiation and streak artifact introduced by dental or metallic hardware are other disadvantages [8,10,10].
Cone beam CT (CBCT) was introduced in 1998 as a technique based on cone-shaped, rotating X-rays to enhance visualization of bony structures and foreign metal objects [11]. Its main advantages over conventional CT include a lower dose of ionizing radiation, cheaper cost, and reduced image degradation from metallic artifacts [12,14,14]. 3D reconstruction is possible with CBCT and can be viewed in any direction, at various slice thicknesses, and from any cross-sectional orientation [15]. However, CBCT does not adequately visualize glandular parenchyma or soft tissue structures.
Magnetic Resonance Imaging
Magnetic resonance imaging (MRI) is the preferred advanced imaging modality in the evaluation of malignant salivary gland tumors due to the excellent soft tissue contrast it provides in the assessment of deep tissue planes to help identify extra-glandular or perineural spread [7, 16]. Absence of use of ionizing radiation and the capacity to image patients with iodinated contrast allergies are other advantages to MRI. High costs, increased time burden to patients, exam-associated claustrophobia, and inability to perform in selected patients with implanted devices are disadvantages.
Sialography
Conventional Sialography and Digital Subtraction Sialography
Conventional sialography requires the technical ability to dilate and cannulate a salivary duct orifice as well as skill in radiographic assessment with fluoroscopy. Although it is more readily performed than “minimally invasive” diagnostic sialendoscopy, sialography often benefits from a team approach to include a physician skilled in ductal cannulation and a radiologist expert in fluoroscopy. Although some radiologists perform the procedures themselves, the additional expertise of surgeons who routinely perform sialendoscopy usually permits a more sophisticated approach to the process of ductal dilation (often with microscopic control), duct cannulation, and radiocontrast infusion. The technical challenges in coordinating these dual services have been an impediment to wider application of sialography at some institutions.
Sialography may be considered not only diagnostic but also therapeutic in some cases. The process of distal duct dilation with catheter insertion as well as hydro-dilation of the entire system with “flushing out the gland” employs a radiocontrast water-soluble iodinated compound that has bactericidal activity [17]. Tucci et al. in 2019 reported successful treatment of juvenile recurrent parotitis in 89% of 110 patients (all younger than 16 years of age) employing sialography without local anesthesia or sedation [18]. These investigators suggested that sialography “broke the cycle of decreased secretion, stasis and infection” by improving duct patency with cannulation, instilling iodine-based (antiseptic) radiocontrast, and flushing out debris and epithelial plugs in the duct and gland.
Sialography has additionally been useful in guiding procedures performed within the ductal system under fluoroscopic control. These procedures have been reported to include salivary stone lithotripsy, stone extraction, and balloon ductoplasty [19].
Use of subtraction imaging as is commonly applied to digital subtraction angiography (DSA) is designed to highlight perfused vessels and digitally remove the appearance of overlapping structures to improve image interpretation. When applied to sialography, this subtraction imaging requires stabilization of the head to ensure that pre-contrast images (mask images) are taken in the identical position as those following intraductal contrast infusion (live images). Computer processing removes the mask image (subtraction) from the live image(s) in an effort to eliminate the view of soft tissue and bony structures to focus on the detail of ductal anatomy in two dimensions [10, 14, 20, 21]. Unfortunately, there is some degree of “spatial inconsistency between the two images caused by inevitable and complex motion of patient” resulting in blurring from motion artifact [22]. This “interscan motion” is of greater concern in the course of dynamically manipulating the catheterized salivary duct than with the intravascular infusion done during angiography performed in an immobilized patient.
Conventional sialography in the distant past was performed in an “analogue” manner that required “analogue to digital conversion” when subtracting mask images to result in “digital subtraction sialography” [23]. Conventional sialography is now done with enhanced digital recording in a manner that, with the addition of improved (more dense) radiocontrast agents and technical considerations including optimal head positioning, has negated the value in performing subtraction.
Disadvantages to digital subtraction sialography include not only induction of motion artifact but also diminished assessment of spatial relationship of the duct to adjacent structures and limitation in capacity permitting imaging in only one orientation. Some patients will require handheld manipulation of the catheter during infusion to prevent egress of contrast and dislodgement of the catheter. In these cases, the inability to continue imaging impairs the capacity to orient the mask and live images for subtraction. In similar fashion, although CT sialography had found advocates in the past, the loss of detail in ductal definition when compared to contemporary “conventional” sialography—coupled with the increased radiation exposure of CT imaging—has made this imaging option less useful. The capacity to assess ductal changes in an unlimited number of orientations employing the “fourth dimension” (time) that is available with conventional sialography is lost when only several images (usually pre-, intra-, and post-insufflation) are available as with CT sialography [24].
Fluoroscopic salivary duct imaging has additionally been used to direct procedures such as interventional basket retrieval for proximal, mobile stones [25].
Reports of complication from sialography in the past have included concern about extravasation of radiocontrast (“duct rupture”) that has been negated as a concern by use of absorbable water-soluble radiocontrast. Despite employing pliable plastic angiocatheters to cannulate the salivary ducts, Truong et al. still reported a 4.7% radiocontrast ductal extrusion rate among 255 sialograms reviewed [26]. These investigators identified in each case the extravasation was associated with ductal stricture and had no associated complications as the water-soluble contrast material was readily absorbed.
MR Sialography
MR sialography was developed to evaluate the salivary ducts by employing a special technique of heavily T2-weighted rapid acquisition with relaxation enhancement to exploit the imaging potential of the high T2 signal intensity of stationary fluids [7, 27]. The capacity to image the main salivary ducts without instilling contrast (saliva within the ducts acts as the contrast media) makes MR sialography useful for those patients whose ducts cannot be cannulated due to scarring or other reasons. MR sialography has gained support for evaluation of obstructive sialadenitis due to its capacity to image the main salivary ducts [28,29,30,31,32,33,34]. Additional disadvantages to use of MR sialography include the standard general patient contraindications for MRI and image artifact due to dental fillings, implants, or amalgam.
CT Sialography and Cone Beam CT Sialography
In a manner similar to conventional sialography, both CT and CBCT sialography are performed after ductal cannulation and contrast injection. However, this modality remains mainly a diagnostic tool to help guide therapeutic procedure, and not used concurrently with intervention [35, 36]. CT sialography is capable of demonstrating both soft tissue and glandular parenchyma in addition to ductal anatomy. Moreover, three-dimensional reconstruction can be performed with CBCT to offer additional perspective in orientation [37].
Obstructive Sialopathy
Sialolithiasis
The most common cause of obstructive sialopathy is sialolithiasis. The evaluation of suspected obstruction should adequately image ductal anatomy and identify the sialolith. It is our approach to begin with surgeon-performed US for suspected sialolith. A sialolith is identified as a hyperechoic focus associated with posterior acoustic shadowing, a finding of signal loss deep to the foci. Indirect signs of associated obstruction include main ductal dilation, intraglandular ductal dilation, and glandular parenchymal changes [38].
Ultrasound has been found to detect stones with a sensitivity ranging from 65 to 95%—with the greatest sensitivity found in the most experienced otolaryngologist examiners and the lowest found when ultrasound was performed by an ultrasound technologist [2, 5, 6, 39, 40, 41•]. This sensitivity increases to as high as 97% when sonopalpation is added [2].
Stones located in the mid floor of the mouth and distal Wharton’s duct are more difficult to image and may be missed on sonographic examination. However, most of these can be detected when combined with sonopalpation. The specificity of ultrasound for detecting sialoliths ranges from 80 to 90% [2, 5, 6, 39, 40]—increased to 90% specificity when sonopalpation techniques are added [2]. This wide range in test characteristics in salivary stone evaluation is hypothesized to be attributable to the low interobserver reliability of ultrasound though well-designed studies examining reliability across a diverse range of examiners have not yet been performed [41•].
CT is considered both sensitive (96–98%) and specific (88–100%) for the detection of sialoliths, though factors such as slice thickness, stone size, and the use of contrast may affect the testing characteristics of this modality [6, 9]. CT is disadvantaged by a lack of visualization of the ducts and related pathologies [39]. Traditionally, non-contrast CT with 1-mm slices has been recommended for the detection of sialoliths as it was thought that a calcified sialolith could easily be mistaken for contrast-enhanced vasculature [42]. However, a recent retrospective case series by Purcell et al. found no difference in sensitivity between contrast and non-contrast-enhanced neck CT in the evaluation of 90 patients presenting with suspected sialolithiasis. With CT, 1 mm slice thickness is preferred for CT evaluation as a thicker slice may fail to detect small stones.
Sialolithiasis: Sialography (DSS, MR, CT)
Sialography is considered both sensitive and specific for the detection of sialolithiasis; however, it has become less common as many surgeons favor ultrasound and sialendoscopy as these interventions can be used across a wide variety of clinical settings ranging from the exam room to the operating room [21, 30, 43]. Other surgeons more liberally employ sialography when sialolithiasis involves the parotid rather than the submandibular gland. Ductal stricture(s) that are commonly associated with parotid sialolithiasis complicate management in a way that assessment with a “road map” (sialogram) to depict the often-multiple narrowed regions associated helps direct counseling and management. The capacity to perform open intraoral ductoplasty with minimal morbidity in the management of submandibular sialolithiasis makes sialography less useful for stones in this location.
Ductal Stricture
Stricture and stenosis will share many findings in common with obstructive sialoliths on ultrasound including common signs of indirect obstruction such as main ductal dilation, intraglandular ductal dilation, and glandular parenchymal changes. A transition from a visibly dilated salivary duct to a collapsed duct without evidence of stone may be observed (Fig. 3). This finding becomes more pronounced with the administration of ascorbic acid [44]. Ductal dilation without direct evidence of stones helps to rule in stenosis (positive predictive value = 93%), but absence of these findings was not sufficient to exclude the diagnosis (negative predictive value = 50%) [45].

Proximal parotid ductal dilation and distal stricture seen on US
CT is not well suited for diagnosing mild to moderate ductal stenosis as it fails to demonstrate the ductal anatomy in all but a few cases. A marked ductal sialectasia (megaduct), however, can be visualized as its size is above the resolution limit for CT. Unlike sialolithiasis, no radiopaque structures are usually seen in association with ductal stenosis.
By nature of sialography’s enhancement of ductal anatomy, sialography offers excellent identification of ductal pathologies. In cases of stenoses, conventional sialography demonstrates a loss of contrast or filling defect in the ductal system proximal to the obstruction. It is ideal for characterizing the extent and number of stenoses present and is more sensitive than ultrasound in this regard [38, 39].
Other Obstructive Causes
Sialolith and ductal stenosis represent the two most common causes of obstructive sialopathy. Less frequent causes include ductal foreign bodies, pneumoparotitis, and external compression of the duct. Ductal foreign bodies reported to include toothbrush bristles, grass, hair, or fish bones are caused by retrograde passage of the foreign body via the mouth [46].
The identification and removal of the foreign body is usually performed by sialendoscopy; however, the ability to view the foreign body on ultrasound or CT largely depends on the physical properties of the offending foreign body. Sialography may be useful. Pneumoparotitis may manifest on US as the presence of air within the parotid gland and duct. Chronic pneumoparotitis may lead to sialectasis and parotid duct dilation visible on CT, sialography, or ultrasound [47]. Though uncommon, external compression of the duct may occur secondary to oral dental appliances or at the anterior masseter secondary to masseter hypertrophy.
Infectious
Infectious pathology may manifest as either unilateral or bilateral sialadenitis. The decision to use one imaging modality usually depends on the severity of the infection and setting of the presentation (clinic or the emergency department). In uncomplicated cases of sialadenitis that present in the office, a surgeon experienced in ultrasound may opt to use this modality as a first diagnostic assessment. Acute bacterial sialadenitis often shows enlarged hypoechoic salivary glands. Ductal dilation can sometimes be seen. Abscesses can be seen on US as relatively anechoic foci with fine and coarse echoes in late stages, along with periglandular inflammatory changes [48]. For complicated infections unrelated to obstructive pathology, or cases where extra-glandular extension is suspected, contrast-enhanced CT is the most sensitive modality for detecting the deep extent of an abscess [49]. Within a bacterially infected gland, diffuse inhomogeneous pattern of contrast enhancement can be seen. When MR is obtained, usually due to contrast-related contraindications, high T2 signal intensity will usually accompany the typically asymmetric, diffuse glandular enlargement and occasionally be associated with a dilated duct on STIR images [48].
Granulomatous inflammation due to cat scratch disease is characterized by enlarged lymph nodes within the gland, with often normal-appearing parenchyma on ultrasound. Tuberculosis can also involve the salivary gland and demonstrate either decreased echogenicity or a focal intraparotid hypoechoic zone with an associated cavity [49,50,51]. A “periparotid type” pattern has also been described, appearing as multiple hypoechoic nodules located in a peripheral zone of hyperechoic gland consistent with enlarged periglandular lymph nodes [51]. Necrotic nodes, calcifications, and enlarged lymph nodes are also usually appreciated across both ultrasound and CT. Moreover, atypical mycobacterial infections tend to show extension from cervical adenitis, and are radiologically indistinguishable from tuberculosis [48].
Chronic Sialadenitis
Repeated infections may result in glandular atrophy with focal intraglandular calcifications. Glands affected by chronic inflammation are often characterized by sialectasis and reduced salivary secretions. An obstructive process frequently lays the ground for these repeated bacterial infections. Multiple oval hypoechoic areas, often uniformly distributed in the gland parenchyma, are characteristically found [48, 52]. Doppler US can help demonstrate increased vascularization, and parenchymal fibrosis as well (Fig. 4) [50].

Doppler US of the submandibular gland demonstrating a hypervascular mass found to be a lymphoma
Autoimmune Systemic Disorders
Sjögren’s Syndrome
The salivary gland changes seen in Sjögren’s syndrome (SS) may be assessed by many imaging modalities with recent support for expanded use of ultrasound to quantify findings through scoring systems to assist in confirming the diagnosis [53]. Additional support for expanded use of sialography to identify location and extent of parotid ductal strictures amenable to dilation with steroid infusion has been reported [54].
Sjogren’s syndrome salivary gland ultrasound (SGUS) is characterized by a heterogenous salivary parenchyma (Fig. 5) marked by multiple small round anechoic or hypoechoic foci, sometimes described as resembling a “honeycomb” [55]. This pattern is thought to be caused by fatty infiltration, fibrosis, ductal dilation and lymphoid involvement of the glands [56]. The degree of inhomogeneity may be graded and correlated to the disease severity [57]. These findings have been shown to aid in the diagnosis of primary Sjögren’s syndrome (pSS) with good agreement between sonographic findings and the 2016 American College of Rheumatology (ACR)/European League Against Rheumatism (EULAR) classification criteria [58]. The intense scrutiny of ultrasound scoring systems to help not only with clinical management, but also in establishing the diagnosis of primary Sjogren’s syndrome (pSS) led Jousee-Joulin et al. in 2020 to “strongly suggest that the SGUS score assist in the classification of pSS and deserves inclusion in the next iteration of the ACR-EULAR classification criteria for pSS” [59].

US demonstrating Sjögren’s syndrome: heterogenous parenchyma marked by multiple small round anechoic or hypoechoic foci in a “honeycomb” pattern
MRI will show patterns of parenchymal inhomogeneity similar to those found on ultrasound. T1- and T2-weighted sequencing shows multiple areas of hypo- and hyperintensity ranging in various sizes. MR sialography allows for visualization of ductal structures without the invasive instillation of a contrast agent into the duct [28].
Contrast sialography remains an active criterion in the classification system to establish the diagnosis of Sjogren’s syndrome (SS). Foggia et al. (2020) through a review of 26 parotid sialograms performed to evaluate Sjogren’s syndrome formulated a classification system for ductal involvement identifying cases in which the main duct was unaffected and therefore more likely to benefit from steroid infusion in a clinic setting than full sialendoscopy with duct dilation [54]. These investigators identified a correlation between symptom duration and degree of main ductal stenosis, supporting the contention that SS is a disease that progresses over time from a proximal (terminal ducts and acini) to distal (main duct) fashion “to ultimately involve the entire ductal system in most cases—sparing the main duct in a minority of cases.”
While CT may reveal the inhomogeneity of the parenchyma, it is less often used than ultrasound or MRI in assessing SS due to poorer soft tissue characterization and exposure to ionizing radiation.
IgG4-Related Disease
IgG4-related disease (IgG4-RD) is a chronic fibroinflammatory condition typified by enlargement of the affected gland, elevated serum IgG4 concentrations, and infiltration of abundant IgG4-positive plasma cells into the affected gland [60].
A broad spectrum of radiographic findings have characterized salivary gland involvement with IgG4-RD that may reflect not only different stages in the disease process but also treatment effect [61]. This diversity in presentation is consistent with the multiple differing phenotypes that permitted Wallace et al. to classify IgG4-RD into 4 major groups with further variability identified within each group [62]. IgG4-RD may be characterized on CT and MR imaging by diffuse multiglandular disease or localized disease involving the parotid, submandibular, and sublingual glands. In cases with diffuse multiglandular involvement, the lacrimal glands may also be involved.
Contrast-enhanced CT imaging variably shows either a homogenous enhancement or a heterogenous “crazy-paving” pattern associated with bilateral enlargement of the submandibular glands, parotid glands, or both [63, 64]. This heterogenous “crazy-paving” pattern is thought to be due to sclerosis of the interlobular septa seen on histologic examination of affected glands.
US examination reveals swelling of usually bilateral glands with a rough contour texture. Gland parenchyma generally shows diffuse hypoechoic echotexture or multiple hypoechoic nodule within the affected gland. Increased Doppler signal is also seen within the affected gland [65]. Although the submandibular gland is more commonly affected and may demonstrate ultrasound findings similar to those seen with Sjogren’s syndrome, the less commonly involved parotid gland is identified with unremarkable parenchyma surrounding a dilated ductal system [66,67,68]. MR imaging demonstrates diffuse swelling of the affected salivary glands. Lesions are usually well-defined and demonstrate homogenous signal intensity. T1- and T2-weighted images demonstrate signal hypo-intensity with homogenous enhancement upon contrast injection, though these findings are not specific [60].
Tumors
Differentiating benign from malignant tumors on US has been shown with an association of deep or distal acoustic enhancement, with a sensitivity of 53% and specificity of 89% [69]. Malignant tumors have consistently been shown to be associated with extra-parenchymal extension, irregular borders, hypervascularity, infiltration and lack of deep enhancement [70, 7172•]. Centrally located cystic components have also been found to be significantly more frequent in malignant tumors, both in CT and MRI [16, 73]. A recent meta-analysis found the diagnostic sensitivity and specificity of ultrasound to be 63% and 92% respectively in differentiating malignant from benign salivary gland tumors [74]. In contrast, CT and MRI demonstrated sensitivities and specificities of 83% and 85%, and 81% and 89%, respectively, in that same analysis [74]. Among series with surgeon-performed ultrasound, hypervascularity, infiltration and increased heterogenicity have been found to be significantly associated with malignant tumors with high specificity and positive predictive values [71, 72•]. Moreover, determining the depth of tumor and its relation to the facial nerve by way of either measuring the distance between the skin and deep aspect of mass, or the minimal fascia-tumor distance (with cut-off points between 2.4 and 3.0 mm described in the literature) can help localize benign parotid tumors to either superficial or deep lobes (Fig. 6) [75,76,77]. These techniques can aid in operative planning and patient counseling, especially in benign cases. In cases of malignancy or in deep lobe tumors whose margins are not assessable through US, obtaining further cross-sectional imaging, usually an MRI, is warranted.

A well-circumscribed parotid mass with an anechoic center suggestive of a cystic component
Conclusion
Various imaging modalities are at the disposal of the otolaryngologist in the workup of salivary gland disorders. The value of surgeon-performed ultrasound continues to be demonstrated throughout numerous studies, largely due to its wide applicability, versatility, availability, and low cost. In settings where US cannot be performed, CT remains an easy, reliable method for detecting radiopaque sialoliths. Conventional sialography remains an important diagnostic option and an increasingly valuable therapeutic option. For benign salivary tumors, US may obviate the need for further imaging and provide reliable estimation of tumor location and relationship to the facial nerve.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance
Hoffman HT, Pagedar NA. Ultrasound-guided salivary gland techniques and interpretations. Atlas Oral Maxillofac Surg Clin North Am. 2018;26(2):119–32. https://doi.org/10.1016/j.cxom.2018.04.001.
Patel NJ, Hashemi S, Joshi AS. Sonopalpation: a novel application of ultrasound for detection of submandibular calculi. Otolaryngol - Head Neck Surg (United States). 2014;151(5):770–5. https://doi.org/10.1177/0194599814545736.
Khan N, Afroz N, Agarwal S, Khan M, Ahmad I, Ansari H. Comparison of the efficacy of the palpation versus ultrasonography-guided fine-needle aspiration cytology in the diagnosis of salivary gland lesions. Clin Cancer Investig J. 2015;4(2):134.
Jousse-Joulin S, Nowak E, Cornec D, Brown J, Carr A, Carotti M, et al. Salivary gland ultrasound abnormalities in primary Sjögren’s syndrome: consensual US-SG core items definition and reliability. RMD Open. 2017;3:e000364. https://doi.org/10.1136/rmdopen-2016-000364.
Gritzmann N. Sonography of the salivary glands. Am J Roentgenol. 1989;153(1):161–6. https://doi.org/10.2214/ajr.153.1.161.
Thomas WW, Douglas JE, Rassekh CH. Accuracy of ultrasonography and computed tomography in the evaluation of patients undergoing sialendoscopy for sialolithiasis. Otolaryngol - Head Neck Surg (United States). 2017;156(5):834–9. https://doi.org/10.1177/0194599817696308.
Atkinson C, Fuller J, Huang B. Cross-sectional imaging techniques and normal anatomy of the salivary glands. Neuroimaging Clin N Am. 2018;28(2):137–58. https://doi.org/10.1016/j.nic.2018.01.001.
Som PM, Curtin HD. Salivary glands. In: Head and neck imaging. 4th ed. St Louis: Elsevier; 2003.
Purcell YM, Kavanagh RG, Cahalane AM, Carroll AG, Khoo SG, Killeen RP. The diagnostic accuracy of contrast-enhanced CT of the neck for the investigation of sialolithiasis. Am J Neuroradiol. 2017;38(11):2161–6. https://doi.org/10.3174/ajnr.A5353.
Sobrino-Guijarro B, Cascarini L, Lingam RK. Advances in imaging of obstructed salivary glands can improve diagnostic outcomes. Oral Maxillofac Surg. 2013;17(1):11–9. https://doi.org/10.1007/s10006-012-0327-8.
Schwarz D, Kabbasch C, Scheer M, Mikolajczak S, Beutner D, Luers JC. Comparative analysis of sialendoscopy, sonography, and CBCT in the detection of sialolithiasis. Laryngoscope. 2015;125(5):1098–101. https://doi.org/10.1002/lary.24966.
Mozzo P, Procacci C, Tacconi A, Tinazzi Martini P, Bergamo Andreis IA. A new volumetric CT machine for dental imaging based on the cone-beam technique: preliminary results. Eur Radiol. 1998;8(9):1558–64. https://doi.org/10.1007/s003300050586.
van der Meij EH, Karagozoglu KH, de Visscher JGAM. The value of cone beam computed tomography in the detection of salivary stones prior to sialendoscopy. Int J Oral Maxillofac Surg. 2018;47(2):223–7. https://doi.org/10.1016/j.ijom.2017.07.022.
Jadu FM, Lam EWN. A comparative study of the diagnostic capabilities of 2D plain radiograph and 3D cone beam CT sialography. Dentomaxillofacial Radiol. 2013;42(1):1–8. https://doi.org/10.1259/dmfr.20110319.
Drage N, Rogers S, Greenall C, Playle R. Incidental findings on cone beam computed tomography in orthodontic patients. J Orthod. 2013;40(1):29–37. https://doi.org/10.1179/1465313312Y.0000000027.
Abdel Razek AAK, Mukherji SK. State-of-the-art imaging of salivary gland tumors. Neuroimaging Clin N Am. 2018;28(2):303–17. https://doi.org/10.1016/j.nic.2018.01.009.
Lee C, Kim JE, Huh KH, Yi WJ, Heo MS, Lee SS, et al. Therapeutic effect of intraductal irrigation of the salivary gland: a technical report. Imaging Sci Dent. 2017;47:123–7. https://doi.org/10.5624/isd.2017.47.2.123.
Tucci FM, Roma R, Bianchi A, De Vincentiis GC, Bianchi PM. Juvenile recurrent parotitis: diagnostic and therapeutic effectiveness of sialography. Retrospective study on 110 children. Int J Pediatr Otorhinolaryngol. 2019;124:179. https://doi.org/10.1016/j.ijporl.2019.06.007.
Brown JE. Interventional sialography and minimally invasive techniques in benign salivary gland obstruction. Semin Ultrasound, CT MRI. 2006;27(6):465–75. https://doi.org/10.1053/j.sult.2006.09.003.
Kelly IMG, Dick R. Technical report: interventional sialography: Dormia basket removal of Wharton’s duct calculus. Clin Radiol. 1991;43(3):205–6. https://doi.org/10.1016/S0009-9260(05)80480-5.
Kalinowski M, Heverhagen JT, Rehberg E, Klose KJ, Wagner HJ. Comparative study of MR sialography and digital subtraction sialography for benign salivary gland disorders. Am J Neuroradiol. 2002;23(9):1485–92.
Lightfoote JB, Friedenberg RM, Smolin MF. Digital subtraction ductography. Am J Roentgenol. 1985;144:635–8. https://doi.org/10.2214/ajr.144.3.635.
Gao Y, Song Y, Yin X, Wu W, Zhang L, Chen Y, et al. Deep learning-based digital subtraction angiography image generation. Int J Comput Assist Radiol Surg. 2019;14:1775–84. https://doi.org/10.1007/s11548-019-02040-x.
Blake Sullivan C, Hoffman H. Dynamic imaging with sialography combined with sialendoscopy to manage a foreign body in Stensen’s duct. Am J Otolaryngol - Head Neck Med Surg. 2018;39:349–51. https://doi.org/10.1016/j.amjoto.2018.03.001.
Brown JE, Drage NA, Escudier MP, Wilson RF, McGurk M. Minimally invasive radiologically guided intervention for the treatment of salivary calculi. Cardiovasc Intervent Radiol. 2002;25(5):352–5. https://doi.org/10.1007/s00270-002-1950-9.
Truong K, Hoffman HT, Policeni B, Maley J. Radiocontrast dye extravasation during sialography. Ann Otol Rhinol Laryngol. 2018;127(3):192–9. https://doi.org/10.1177/0003489417752711.
Lomas DJ, Carroll NR, Johnson G, Antoun NM, Freer CEL. MR sialography: work in progress. Radiology. 1996;200(1):129–33. https://doi.org/10.1148/radiology.200.1.8657900.
Jungehulsing M, Fischbach R, Schroder U, Kugel H, Damm M, Eckel HE. Magnetic resonance sialography. Otolaryngol Head Neck Surg. 1999;121(4):488–94. https://doi.org/10.1016/S0194-5998(99)70243-3.
Gadodia A, Seith A, Sharma R, Thakar A, Parshad R. Magnetic resonance sialography using CISS and HASTE sequences in inflammatory salivary gland diseases: comparison with digital sialography. Acta Radiol. 2010;51(2):156–63. https://doi.org/10.3109/02841850903376306.
Becker M, Marchal F, Becker CD, Dulguerov P, Georgakopoulos G, Lehmann W, et al. Sialolithiasis and salivary ductal stenosis: diagnostic accuracy of MR sialography with a three-dimensional extended-phase conjugate-symmetry rapid spin-echo sequence. Radiology. 2000;217(2):347–58. https://doi.org/10.1148/radiology.217.2.r00oc02347.
Capaccio P, Cuccarini V, Ottaviani F, Minorati D, Sambataro G, Cornalba P, et al. Comparative ultrasonographic, magnetic resonance sialographic, and videoendoscopic assessment of salivary duct disorders. Ann Otol Rhinol Laryngol. 2008;117(4):245–52. https://doi.org/10.1177/000348940811700402.
Izumi M, Eguchi K, Ohki M, Uetani M, Hayashi K, Kita M, et al. MR imaging of the parotid gland in Sjögren’s syndrome: a proposal for new diagnostic criteria. Am J Roentgenol. 1996;166(6):1483–7. https://doi.org/10.2214/ajr.166.6.8633469.
De Ren Y, Li XR, Zhang J, Long LL, Li WX, Han YQ. Conventional MRI techniques combined with MR sialography on T2-3D-DRIVE in Sjögren syndrome. Int J Clin Exp Med. 2015;8(3):3974–82.
Lee LIT, Pawar RR, Whitley S, Makdissi J. Incidence of different causes of benign obstruction of the salivary glands: retrospective analysis of 493 cases using fluoroscopy and digital subtraction sialography. Br J Oral Maxillofac Surg. 2015;53:54–7. https://doi.org/10.1016/j.bjoms.2014.09.017.
Bertin H, Bonnet R, Delemazure AS, Mourrain-Langlois E, Mercier J, Corre P. Three-dimensional cone-beam CT sialography in non tumour salivary pathologies: procedure and results. Dentomaxillofacial Radiol. 2016;46(1). https://doi.org/10.1259/dmfr.20150431.
Kroll T, May A, Wittekindt C, Kähling C, Sharma SJ, Howaldt HP, et al. Cone beam computed tomography (CBCT) sialography - an adjunct to salivary gland ultrasonography in the evaluation of recurrent salivary gland swelling. Oral Surg Oral Med Oral Pathol Oral Radiol. 2015;120(6):771–5. https://doi.org/10.1016/j.oooo.2015.09.005.
Drage NA, Brown JE. Cone beam computed sialography of sialoliths. Dentomaxillofacial Radiol. 2009;38(5):301–5. https://doi.org/10.1259/dmfr/90784441.
Goncalves M, Schapher M, Iro H, Wuest W, Mantsopoulos K, Koch M. Value of sonography in the diagnosis of sialolithiasis: comparison with the reference standard of direct stone identification. J Ultrasound Med. 2017;36(11):2227–35. https://doi.org/10.1002/jum.14255.
Marchal F, Dulguerov P. Sialolithiasis management: the state of the art. Arch Otolaryngol Head Neck Surg. 2003;129(9):951–6. https://doi.org/10.1001/archotol.129.9.951.
Jager L, Menauer F, Holzknecht N, Scholz V, Grevers G, Reiser M. Sialolithiasis: MR sialography of the submandibular duct - an alternative to conventional sialography and US? Radiology. 2000;216(3):665–71. https://doi.org/10.1148/radiology.216.3.r00se12665.
• Goncalves M, Mantsopoulos K, Schapher ML, et al. Interrater reliability of ultrasound in the diagnosis of sialolithiasis. Ultraschall Med. 2019;40(4):481–7. https://doi.org/10.1055/a-0837-0712Large retrospective study supporting ultrasound as a first-line study for diagnosing sialolithiasis by experienced otolaryngologists, with high sensitivity, specificity, and positive predictive value.
Avrahami E, Englender M, Chen E, Shabtay D, Katz R, Harell M. CT of submandibular gland sialolithiasis. Neuroradiology. 1996;38(3):287–90. https://doi.org/10.1007/BF00596550.
Pniak T, Štrympl P, Staníková L, Zeleník K, Matoušek P, Komínek P. Sialoendoscopy, sialography, and ultrasound: a comparison of diagnostic methods. Open Med. 2016;11(1):461–4. https://doi.org/10.1515/med-2016-0081.
Bozzato A, Hertel V, Bumm K, Iro H, Zenk J. Salivary simulation with ascorbic acid enhances sonographic diagnosis of obstructive sialadenitis. J Clin Ultrasound. 2009;37(6):329–32. https://doi.org/10.1002/jcu.20595.
Larson AR, Aubin-Pouliot A, Delagnes E, Zheng M, Chang JL, Ryan WR. Surgeon-performed ultrasound for chronic obstructive sialadenitis helps predict sialendoscopic findings and outcomes. Otolaryngol Head Neck Surg. 2017;157(6):973–80. https://doi.org/10.1177/0194599817728867.
Levine G, Clark M, Mandel L. Obstructive parotitis from extraorally introduced foreign body in the stensen duct. J Oral Maxillofac Surg. 2013;71(12):2087–91. https://doi.org/10.1016/j.joms.2013.06.211.
McGreevy AE, O’Kane AM, McCaul D, Basha SI. Pneumoparotitis: a case report. Chen A, ed Head Neck. 2013;35(2):E55-E59. doi:https://doi.org/10.1002/hed.21873.
Abdel Razek AAK, Mukherji S. Imaging of sialadenitis. Neuroradiol J. 2017;30(3):205–15. https://doi.org/10.1177/1971400916682752.
Ugga L, Ravanelli M, Pallottino AA, Farina D, Maroldi R. Work-up diagnostico nella patologia ostruttiva e infiammatoria delle ghiandole salivari. Acta Otorhinolaryngol Ital. 2017;37(2):83–93. https://doi.org/10.14639/0392-100X-1597.
Orlandi MA, Pistorio V, Guerra PA. Ultrasound in sialadenitis. J Ultrasound. 2013;16(1):3–9. https://doi.org/10.1007/s40477-013-0002-4.
Koç A, Cengíz K, Şengör A, Han T. Tuberculosis of the parotid gland. Otolaryngol Head Neck Surg. 2005;133(4):640. https://doi.org/10.1016/j.otohns.2004.09.056.
Yousem DM, Kraut MA, Chalian AA. State of the art major salivary gland imaging 1.
Jousse-Joulin S, D’Agostino MA, Nicolas C, et al. Video clip assessment of a salivary gland ultrasound scoring system in Sjögren’s syndrome using consensual definitions: an OMERACT ultrasound working group reliability exercise. Ann Rheum Dis. 2019;78:967–73. https://doi.org/10.1136/annrheumdis-2019-215024.
Foggia MJ, Peterson J, Maley J, Policeni B, Hoffman HT. Sialographic analysis of parotid ductal abnormalities associated with Sjogren’s syndrome. Oral Dis. 2020. https://doi.org/10.1111/odi.13298.
Jecker P, Geisthoff U, Meyer J, Orloff L. Salivary gland ultrasonography. In: Orloff LA, ed. Head and neck ultrasonography: essential and extended applications. Second. San Diego, CA: Plural Publishing; 2017:155–188.
Niemelä RK, Takalo R, Pääkkö E, Suramo I, Päivänsalo M, Salo T, et al. Ultrasonography of salivary glands in primary Sjögren’s syndrome. A comparison with magnetic resonance imaging and magnetic resonance sialography of parotid glands. Rheumatology. 2004;43(7):875–9. https://doi.org/10.1093/rheumatology/keh187.
Hočevar A, Ambrožič A, Rozman B, Kveder T, Tomšič M. Ultrasonographic changes of major salivary glands in primary Sjögren’s syndrome. Diagnostic value of a novel scoring system. Rheumatology. 2005;44(6):768–72. https://doi.org/10.1093/rheumatology/keh588.
Mossel E, Delli K, Van Nimwegen JF, et al. Ultrasonography of major salivary glands compared with parotid and labial gland biopsy and classification criteria in patients with clinically suspected primary Sjögren’s syndrome. Ann Rheum Dis. 2017;76(11):1883–9. https://doi.org/10.1136/annrheumdis-2017-211250.
Jousse-Joulin S, Gatineau F, Baldini C, Baer A, Barone F, Bootsma H, et al. Weight of salivary gland ultrasonography compared to other items of the 2016 ACR/EULAR classification criteria for primary Sjögren’s syndrome. J Intern Med. 2020;287(2):180–8. https://doi.org/10.1111/joim.12992.
Fujita A. Imaging of Sjögren syndrome and immunoglobulin G4-related disease of the salivary glands. Neuroimaging Clin N Am. 2018;28(2):183–97. https://doi.org/10.1016/j.nic.2018.01.003.
Marcus K, Rajan A, Maley J, Hoffman H. Multimodal imaging using ultrasound and sialography to identify IgG4-related disease involving the parotid gland. In: Combined Otolaryngology Spring Meeting 2020.
Wallace ZS, Zhang Y, Perugino CA, Naden R, Choi HK, Stone JH. Clinical phenotypes of IgG4-related disease: an analysis of two international cross-sectional cohorts. Ann Rheum Dis. 2019;78:406–12. https://doi.org/10.1136/annrheumdis-2018-214603.
Wang Z, Feng R, Chen Y, et al. CT features and pathologic characteristics of IgG4-related systemic disease of submandibular gland. Int J Clin Exp Pathol. 2015;8(12):16111–6.
Ferreira da Silva RC, Lieberman SM, Hoffman HT, Policeni B, Bashir A, Smith RJH, et al. IgG4-related disease in an adolescent with radiologic-pathologic correlation. Radiol Case Reports. 2017;12(1):196–9. https://doi.org/10.1016/j.radcr.2016.10.008.
Omotehara S, Nishida M, Satoh M, Inoue M, Kudoh Y, Horie T, et al. Sonographic findings of immunoglobulin G4-related sclerosing sialadenitis. J Med Ultrason. 2016;43(2):257–62. https://doi.org/10.1007/s10396-015-0693-6.
Wang ZJ, Zheng LY, Pu YP, et al. Clinical features and treatment outcomes of immunoglobulin g4-related sclerosing sialadenitis. J Craniofac Surg. 2014;25:2089. https://doi.org/10.1097/SCS.0000000000001016.
Shimizu M, Okamura K, Kise Y, Takeshita Y, Furuhashi H, Weerawanich W, et al. Effectiveness of imaging modalities for screening IgG4-related dacryoadenitis and sialadenitis (Mikulicz’s disease) and for differentiating it from Sjögren’s syndrome (SS), with an emphasis on sonography. Arthritis Res Ther. 2015;17:223. https://doi.org/10.1186/s13075-015-0751-x.
Li W, Xie XY, Su JZ, Hong X, Chen Y, Gao Y, et al. Ultrasonographic features of immunoglobulin G4-related sialadenitis. Ultrasound Med Biol. 2016;42(1):167–75. https://doi.org/10.1016/j.ultrasmedbio.2015.09.014.
Kovačević DO, Fabijanić I. Sonographic diagnosis of parotid gland lesions: correlation with the results of sonographically guided fine-needle aspiration biopsy. J Clin Ultrasound. 2010;38(6):294–8. https://doi.org/10.1002/jcu.20704.
Białek EJ, Jakubowski W, Karpińska G. Role of ultrasonography in diagnosis and differentiation of pleomorphic adenomas: work in progress. Arch Otolaryngol Head Neck Surg. 2003;129(9):929–33. https://doi.org/10.1001/archotol.129.9.929.
Rzepakowska A, Osuch-Wójcikiewicz E, Sobol M, Cruz R, Sielska-Badurek E, Niemczyk K. The differential diagnosis of parotid gland tumors with high-resolution ultrasound in otolaryngological practice. Eur Arch Oto-Rhino-Laryngology. 2017;274(8):3231–40. https://doi.org/10.1007/s00405-017-4636-2.
• Zheng M, Plonowska KA, Strohl MP, Ryan WR. Surgeon-performed ultrasound for the assessment of parotid masses. Am J Otolaryngol - Head Neck Med Surg. 2018;39(5):467–71. https://doi.org/10.1016/j.amjoto.2018.04.011Findings from this study suggest that surgeon-performed US can help predict parotid mass benignity or malignancy, margin risk and relation of tumor to facial nerve.
Kato H, Kanematsu M, Watanabe H, Mizuta K, Aoki M. Salivary gland tumors of the parotid gland: CT and MR imaging findings with emphasis on intratumoral cystic components. Neuroradiology. 2014;56(9):789–95. https://doi.org/10.1007/s00234-014-1386-3.
Liu Y, Li J, Tan YR, Xiong P, Zhong LP. Accuracy of diagnosis of salivary gland tumors with the use of ultrasonography, computed tomography, and magnetic resonance imaging: a meta-analysis. Oral Surg Oral Med Oral Pathol Oral Radiol. 2015;119(2):238–245.e2. https://doi.org/10.1016/j.oooo.2014.10.020.
Cheng PC, Chang CM, Huang CC, Lo WC, Huang TW, Cheng PW, et al. The diagnostic performance of ultrasonography and computerized tomography in differentiating superficial from deep lobe parotid tumours. Clin Otolaryngol. 2019;44(3):286–92. https://doi.org/10.1111/coa.13289.
Higashino M, Kawata R, Haginomori S-I, Lee K, Yoshimura K, Inui T, et al. Novel differential diagnostic method for superficial/deep tumor of the parotid gland using ultrasonography. Head Neck. 2013;35(8):1153–7. https://doi.org/10.1002/hed.23103.
Brennan PA, Herd MK, Howlett DC, Gibson D, Oeppen RS. Is ultrasound alone sufficient for imaging superficial lobe benign parotid tumours before surgery? Br J Oral Maxillofac Surg. 2012;50(4):333–7. https://doi.org/10.1016/j.bjoms.2011.01.018.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Daniel A. Benito, Christopher Badger, and Arjun Joshi declare that they have no conflict of interest.
Henry Hoffman is an author for UpToDate, a research consultant for Cook Medical and iotamotion, and a section editor for the journal Current Otorhinolaryngology Reports.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical collection on Salivary Gland Disorders
Rights and permissions
About this article

Cite this article
Benito, D.A., Badger, C., Hoffman, H.T. et al. Recommended Imaging for Salivary Gland Disorders. Curr Otorhinolaryngol Rep 8, 311–320 (2020). https://doi.org/10.1007/s40136-020-00299-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40136-020-00299-2