
Abstract
Purpose
There is a lack of consensus about which endocarditis-specific preoperative characteristics have an actual impact over postoperative mortality. Our objective was the identification and quantification of these factors.
Methods
We performed a systematic review of all the studies which reported factors related to in-hospital mortality after surgery for acute infective endocarditis, conducted according to PRISMA recommendations. A search string was constructed and applied on three different databases. Two investigators independently reviewed the retrieved references. Quality assessment was performed for identification of potential biases. All the variables that were included in at least two validated risk scores were meta-analyzed independently, and the pooled estimates were expressed as odds ratios (OR) with their confidence intervals (CI).
Results
The final sample consisted on 16 studies, comprising a total of 7484 patients. The overall pooled OR were statistically significant (p < 0.05) for: age (OR 1.03, 95% CI 1.00–1.05), female sex (OR 1.56, 95% CI 1.35–1.81), urgent or emergency surgery (OR 2.39 95% CI 1.91–3.00), previous cardiac surgery (OR 2.19, 95% CI 1.84–2.61), NYHA ≥ III (OR 1.84, 95% CI 1.33–2.55), cardiogenic shock (OR 4.15, 95% CI 3.06–5.64), prosthetic valve (OR 1.98, 95% CI 1.68–2.33), multivalvular affection (OR 1.35, 95% CI 1.01–1.82), renal failure (OR 2.57, 95% CI 2.15–3.06), paravalvular abscess (OR 2.39, 95% CI 1.77–3.22) and S. aureus infection (OR 2.27, 95% CI 1.89–2.73).
Conclusions
After a systematic review, we identified 11 preoperative factors related to an increased postoperative mortality. The meta-analysis of each of these factors showed a significant association with an increased in-hospital mortality after surgery for active infective endocarditis.
Graphic abstract
Graph summary of the Pooled Odds Ratios of the 11 preoperative factors analyzed after the systematic review and meta-analysis.

Similar content being viewed by others



Avoid common mistakes on your manuscript.
Introduction
The mortality rate in patients operated on after the diagnosis of infective endocarditis (IE) is reported to range from 15% to more than 45%, depending on several factors, such as patient baseline characteristics, preoperative status, offending pathogen, intraoperative difficulties and hospital expertise variations [1]. In spite of the improvement of antimicrobial therapy, the advances in surgical techniques and the shortening of waiting time to surgery, the mortality associated with IE continues to be very high [1, 2]. In that context, although cardiac surgery is an essential procedure in the treatment of IE, a proportion of patients who have surgical indication do not undergo surgical treatment because of their high surgical risk, which could lead to surgery rejection [3,4,5,6]. It is estimated that less than half of the patients who have a surgical indication finally undergo surgical intervention [7,8,9,10]. However, it is well known that patients who have indication for surgery and are not operated on have a dismal prognosis [11], whereas long-term survival in patients who survive the cardiac surgery is acceptable [12].
Therefore, accurate surgical risk estimation is crucial for the surgical decision-making process. In the recent years, several new IE-specific risk scores have been developed. They incorporate some IE-specific factors that are thought to be independent mortality factors [8, 13]. However, the impact of all these specific factors in postoperative mortality continues to be in doubt.
The aim of the present systematic review and meta-analysis was to clarify which are the main pre-operative factors related to in-hospital mortality after valve surgery for active IE. An adequate knowledge of the impact on survival of these factors may help to guide the surgical decision process, through the identification of patients with a higher risk of suffering a poor outcome after surgery.
Methods
Data sources
The systematic review was undertaken in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [14], and it followed the recommendations of Meta-analysis Of Observational Studies in Epidemiology (MOOSE) Group [15]. The literature search was carried out with the help of an experienced librarian. The review question and the complete search strategy [16] are detailed in Fig. 1-1.

Search strategy. 1: Review question and complete search strategy. 2: Flow chart of included/excluded studies
Study selection
The inclusion criteria for the eligible studies were studies whose study population comprised adult subjects with active IE who underwent valve surgery. The investigation of the association between a prognostic factor and in-hospital postoperative mortality was required for inclusion, or raw data from which this association could be determined instead. Active endocarditis was defined as on-going active infection under antimicrobial treatment at the time of surgery [17].
Observational studies, randomized controlled trials, and systematic reviews and meta-analysis were included. Redundancies and overlaps between studies were managed and controlled after quality assessment. Studies that included participants who were managed with medical treatment alone, and those studies focused exclusively on specific subgroups (e.g., valve repair, native valves, congenital diseases, etc.) were excluded. The main reason for exclusion of those specific subgroups publications was the lack of availability of full-sample data, with a high risk of selection bias. The search was limited to articles published in English or Spanish languages, in peer-reviewed journals, involving human subjects. In addition, the bibliographic search was limited to studies published from 2000, because of the change in surgical indications and diagnosis with the development of the IE guidelines [18,19,20]. The selected search string was applied on three databases (Medline, Cochrane and EMBASE). Meeting abstracts, case reports, conference presentations, editorials, and expert opinions were excluded.
Figure 1-2 shows the flow chart of the process of selection of the eligible references, and the reasons for inclusion/exclusion at each step are summarized.
Data extraction and quality assessment
Two reviewers (JLM and LVB) independently reviewed the full-text articles of the remaining references, and eligibility against the predefined criteria was evaluated. Discrepancies between the two reviewers were resolved by discussion and consensus. Complete References list of the eligible studies was checked for possible additional unidentified references. Finally, information was extracted from article text, tables, and figures of each selected study (Table 2).
The methodological quality of the selected studies was assessed using the Quality in Prognostic Studies tool (QuIPS), using the criteria previously published by Hayden et al. [21]. Studies with an unacceptable risk of bias were excluded, considered as those with more than one aspect classified as “high risk of bias”.
Prognostic factor selection and definitions
Through the systematic review of the literature, we identified the most common IE-specific variables (Table 1). All those variables that were considered as risk factors for mortality in two or more IE-specific scores were included in the meta-analysis. Therefore, a total of 11 possible pre-operative prognostic factors related to pre-surgical conditions were identified:
-
1.
Age (considered as a continuous variable, expressed in years).
-
2.
Female sex.
-
3.
Urgent surgery: surgery required within 24 h of its indication [22].
-
4.
Emergency surgery: surgery required on the day of admission [22].
-
5.
Previous cardiac surgery: previous surgical procedure with opening of the pericardium.
-
6.
Functional class ≥ III before valve surgery, according to New York Heart Association (NYHA) classification [23].
-
7.
Cardiogenic shock: acute myocardial dysfunction, with systolic pressure < 90 mmHg, tissue hypoperfusion and low cardiac output [24].
-
8.
Prosthetic valve IE: IE affecting a previous prosthetic valve.
-
9.
Multivalvular involvement: IE affecting more than one heart valve.
-
10.
Renal failure: presence of a serum creatinine concentration > 2 mg/dl before surgery.
-
11.
Paravalvular abscess: purulent cavity with necrosis and capacity to invade adjacent structures [25].
-
12.
Staphylococcus aureus as the causative agent of the IE episode.
The analyzed outcome was postoperative death, considered as in-hospital mortality and/or death in the first 30 days after surgery [26, 27].
Statistical analysis
All statistical analyses were performed using Stata/IC 14.2 (Stata Statistical Software: Release 14. College Station, TX: StataCorp LP), implemented with the meta-analysis OR, RR, RD, IR, ID, B, MD & R Combined: User-written command [28].
The meta-analysis was performed pooling all the data of reported in hospital mortality in every study, stratified by each of the previously identified IE-specific prognostic factors.
The calculated univariate OR for in-hospital mortality of each of the selected studies were used as the individual summary statistic to obtain the pooled estimation. Heterogeneity across the studies was assessed using the I2 statistic. An I2 greater than 25% was considered as substantial heterogeneity [29, 30]. The weighting method used was the inverse of variance fixed-effects model (FEM), if there was no significant heterogeneity across the studies, or random-effects model (REM) if substantial heterogeneity was observed [31].
Forest plot graphs were used to graphically depict the association between early mortality and each of the analyzed factors. Empirical correction of zeros methodology was used if zero mortality events were observed in 1 group. However, forest plot graphs were presented after excluding studies with zero mortality for graphical quality improvement.
Publication bias was assessed using Egger method [32] and Funnel plot graphs [33]. All p values were two-sided. In addition, to assess the influence of each individual study on the pooled estimates, we performed an influence analysis by sequentially removing each individual study, to analyze the robustness of the estimated ORs.
Results
Description of included studies and patients
Figure 1-2 shows the flow chart for study selection. After full-text review, 18 observational studies were included [9, 10, 34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49]. The demographic details, distribution, methods and designs of these studies are shown in Table 2.
Four of the initially selected studies analyzed the same multipurpose database, in three different time periods [2, 9, 50, 51]. Therefore, to avoid selection bias because of repeated studies from the same cohort, only one study of these series was included [9].
Quality assessment
To assess the potential biases in the included studies, QuIPS [21] was employed by two reviewers independently in the selected references (Fig. 2-1). Two studies were excluded from the meta-analysis due to a moderate to severe risk of bias [34, 38]. Rob summary table [52] adapted to observational studies was used to show overall risk of bias (Fig. 2-2).

Quality assessment. 1: Risk of bias table and 2: Rob summary
Outcomes
-
1.
Age
Age was analyzed in 15 of the included studies; however, the pooled estimation was only possible in five of them, where age was considered as a continuous variable, comprising a total of 1393 patients. Significant heterogeneity was found across the studies (I2 53.10%; p = 0.07). The overall REM pooled OR (Fig. 3-1) was statistically significant (OR 1.03, 95% CI 1.00–1.05, p < 0.01).
-
2.
Female sex
Fourteen studies reported enough data to estimate the association of sex with the event of interest, comprising a total of 6326 patients (Fig. 3-2). I2 was 3.96% (p = 0.41). The overall FEM pooled OR was 1.56 (95% CI 1.35–1.81, p < 0.001).
-
3.
Urgent or emergency surgery
9 studies analyzed the relation between urgent/emergent surgery and in-hospital mortality (2809 patients). I2 resulted 38.27% (p = 0.12). The overall pooled OR after zero correction was statistically significant (OR 2.39, 95% CI 1.91–3.00, p < 0.001) (Fig. 3-3).
-
4.
Previous cardiac surgery
It was analyzed in 8 of the included studies (4796 patients). I2 was 24.90%, (p = 0.23). The overall pooled OR was 2.19 (95% CI 1.84–2.61, p < 0.001) (Fig. 3-4).
-
5.
NHYA functional class ≥ III
NHYA ≥ III was considered in 10 studies (5119 patients). I2 resulted 32.90% (p = 0.15). The REM pooled OR, adjusted for zero correction, was 1.84 (95% CI 1.33–2.55, p = 0.002) (Fig. 3-5).
-
6.
Cardiogenic shock
Acute circulatory failure was analyzed in 6 studies, comprising a total of 4627 patients. There was significant heterogeneity across the studies (I2 = 43.82%, p = 0.11). REM pooled estimation resulted in a significant association (OR 4.15, 95% CI 3.06–5.64, p < 0.001) (Fig. 3-6).
-
7.
Prosthetic valve IE
Among the 16 studies included in the analysis, 11 analyzed prosthetic valve IE comprising a total of 5857 patients. No heterogeneity was observed across the studies (I2 0%, p = 0.89). The overall pooled OR was 1.98 (95% CI 1.68–2.33, p < 0.001) (Fig. 3-7).
-
8.
Multivalvular involvement
Multivalvular IE was analyzed in 12 studies (5750 patients). The meta-analysis showed a significant heterogeneity (I2 37.92%, p = 0.11). REM pooled estimation (after zero correction) showed a significant association (OR 1.35, 95% CI 1.01–1.82, p = 0.003) (Fig. 3-8).
-
9.
Renal failure
9 studies analyzed the relation between renal failure and in-hospital mortality, comprising a total of 5267 patients. The overall pooled OR was statistically significant (OR 2.57, 95% CI 2.15–3.06, p < 0.001) without heterogeneity across the studies (I2 0%, p = 0.87) (Fig. 3-9).
-
10.
Paravalvular abscess
Figure 3-10 shows the estimated OR of in-hospital mortality and abscess formation. Twelve analyzed paravalvular abscess, comprising a total of 6422 patients. The pooled OR was statistically significant (OR 2.39, 95% CI 1.77–3.22, p < 0.001) using REM (I2 64.68%, p = 0.001).
-
11.
Staphylococcus aureus infection
Staphylococcus aureus as the causative agent of the IE episode was analyzed in 11 studies (5759 patients). No heterogeneity was observed across the studies (I2 0%, p = 0.48). The overall pooled OR was statistically significant (OR 2.27, 95% CI 1.89–2.73, p < 0.001) (Fig. 3-11).
Fig. 3 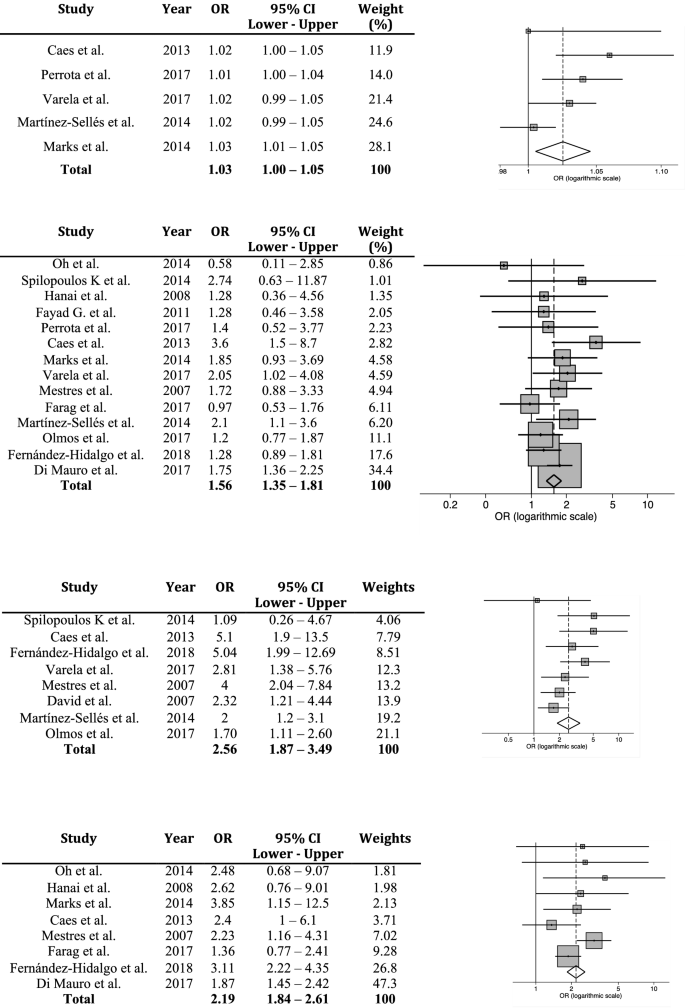


Forest plot graphs. 1: Age, 2: Female sex, 3: Urgent surgery, 4: Previous cardiac surgery, 5: NYHA ≥ III, 6: Cardiogenic shock, 7: Prosthetic valve IE, 8: Multivalvular IE, 9: Renal failure, 10: Paravalvular abscess, 11: S. aureus. *OR odds ratio; CI confidence interval



Other data
There was a possible publication bias, according to Egger’s method in 7 of the analyzed variables; however, no important asymmetries were observed regarding Funnel plots (Fig. 4).


Funnel plots and results in each of the meta-analysis conducted. *Nº number, Stud ad. data studies with adequate data for pooled calculations, FIM fixed effects model, REM random effects model, OR odds ratio, CI confidence interval, Zero c zero correction needed. OR change ^ after influence analysis, maximum change in the pooled OR
Regarding the influence analysis, the pooled estimates were robust and independent of the deletion of any individual study.
Discussion
We performed a systematic review of all the studies that reported factors related to in-hospital mortality after cardiac surgery for IE, trying to address which of those previously described factors are related to poor prognosis. After the development of 11 independent meta-analysis, in order to assess the relative influence of each one on mortality, we found that the 11 possible pre-operative prognostic factors analyzed were associated with poor outcome after surgery.
In the last years, some new endocarditis specific scores have been published [8, 9, 41, 45, 48, 53,54,55] trying to improve prognostic accuracy. And, at the same time, a lot of retrospective and prospective observational studies with limited sample sizes were published describing independent factors for mortality. Several IE-specific factors have been previously defined as independent mortality predictors in patients with IE [8,9,10, 47, 56]. However, the impact of these specific factors on postoperative mortality is debated, since the ones considered in each study are different, and with varied effect-sizes.
Regarding age, although it is one of the most important factors employed in risk calculation [41, 44, 47], it was only considered as a continuous variable in 5 of the included studies. There is an important lack of consensus when categorizing this variable, with different cut-off points when age was considered as a categorical variable. Therefore, it is not possible to combine every study´s individual results. Nevertheless, we observed the huge importance that age has in the prognosis after cardiac surgery, with a 3% of increase in mortality for each additional year.
Several studies found that although women suffered from IE less frequently than men, females have more severe manifestations and are more likely to have worse outcomes [57]. Although female sex is considered as a risk factor in the majority of cardiac surgery scores, it is only present in half of the IE-specific scores [47]. The individual studies included in our systematic review did not find female sex as a significant mortality factor, probably because of a relatively small sample size. Therefore, the pooled estimation found that female sex had a significant association with mortality (OR 1.56).
Both IE-specific scores and classic cardiac surgery risk scores take into account the priority of the surgical intervention to estimate mortality risk [47]. Urgent or emergency surgeries had a significant association with mortality in almost every individual study; consequently, the pooled OR was also statistically significant. Similarly, a history of previous cardiac surgery also increases the difficulty of the surgical approach and increases the mortality risk. Probably for that reason, it also showed a significant association with mortality.
Regarding the clinical presentation of IE, a poor preoperative hemodynamic condition is the greatest predictor of mortality, therefore, it is present in all the published risk models [8, 47]. Cardiogenic shock showed the strongest association with mortality in our meta-analysis (OR 4.15). Likewise, in patients without a critical hemodynamic condition, the presence of heart failure also was an indicator of worse prognosis after surgery [5], with a pooled OR for NYHA ≥ III of 1.84. Regarding valvular invasion, on the one hand, the prognostic implications of prosthetic valve IE have been reported elsewhere [58, 59]. On the other hand, the involvement of more than one cardiac valve has been described as a marker of non-controlled infection and greater severity of IE [8]. Although few studies analyzed the risk of death in multivalvular IE, high mortality rates were reported [60, 61]. Our pooled estimations confirmed an association with mortality of both prosthetic valve IE and multivalvular invasion.
Preoperative renal insufficiency is associated with poor prognosis [62, 63] and longer hospitalization in patients with IE [64]. Nine articles considered renal failure as a prognostic factor, and their results were consistent. Paravalvular abscess increases complexity of the procedure and complications associated with IE surgery and mortality [13]. It is probably associated with higher microorganism virulence, poor prognosis and a delay in the surgical treatment [65]. Twelve studies analyzed paravalvular abscesses, and the pooled OR was 2.39, which agrees with the studies that specifically analyzed outcomes in IE complicated with paravalvular abscesses [13, 65]. Staphylococcus aureus is being recognized as the most common cause of IE [1, 66] and also has been shown to be an independent predictor of mortality. Staphylococcus aureus is related to severity of the local invasion, with increased likelihood of abscesses formation, fistulae and prosthesis dehiscence. Our results confirmed a significant relation with mortality of this etiologic agent.
We believe that an adequate knowledge of the impact on survival of the analyzed risk factors may help to guide the surgical decision process in IE patients. Some meta-analyses were developed to assess the optimal time to surgery, compared biological versus mechanical prosthesis, or compared valve replacement versus valve repair in IE patients. But to our knowledge, our study is the first meta-analysis of prognostic factors in IE surgery in which 11 factors associated with poor outcome were assessed. Recently, Wang et al. published a meta-analysis of risk-scores in surgery for IE [67], comparing the prognostic utility of EuroSCORE I and II, which included 8 studies (1743 patients), and they calculated pooled c-statistics for operative mortality for both scores. They concluded that EuroSCORE had a trend to over-estimate mortality, and suggested that EuroSCORE II would be a better estimator, but in addition, the authors made great emphasis on the need to develop new endocarditis-specific risk scores. One possible future study, after identification of these preoperative factors related to in-hospital mortality, could be the use of the obtained regression coefficients in the development of a new specific-IE score derived from the literature search.
Study limitations
The major limitation of this report is that our meta-analysis included both prospective and retrospective observational studies, with a small to moderate number of patients. Therefore, because of their observational nature, there could be some unidentified differences between the studies, regarding different disease spectrum, referring population size, epidemiological factors, hospital differences, referral bias [68] or surgical indications. For example, the aggressiveness of endocarditis could be different between the included studies, since some of them included only left site IE; whereas other studies included also right side IE. In addition, some studies considered in-hospital mortality as their main outcome, whereas other calculated 30-day mortality. However, predefined criteria insured the inclusion of exclusively active IE. Unfortunately, the results of the individual studies included were not adjusted for baseline differences, since we reported the OR from the univariate analysis or the ones obtained from raw data calculations; so there is risk of bias because of unknown confounders. Of the 16 studies finally included in the meta-analysis, it is important to note that none of them included as much as these 11 factors altogether.
Statistical analysis revealed a possible publication bias in some of the analyzed factors. In addition, some of the funnel plot showed slight asymmetries. The role of chance is critical for interpretation of funnel plots because most of our meta-analyses contained few studies. Relations across studies in meta-analysis are seriously prone to false positive findings when there is heterogeneity and a few numbers of studies are included, which may affect funnel plot symmetry [33].
In reference to age, as we previously mentioned, there is an important lack of consensus in the cut-off points for categorization of age across the studies. Categorization of continuous variables carries a loss of information, and it is not recommended. Therefore, it could only be analyzed when continuous age OR were reported.
All those variables that were considered as risk factors for mortality in two or more IE-specific scores were included in the meta-analysis; however, some other possible risk factors were not analyzed, such as vegetations, thrombocytopenia, LVEF, stroke or embolism. We tried to follow a strict criterion to choose the most studied variables in risk assessment by reviewing previously published IE-specific scores; however the analysis of those other risk factors could be performed to further improve mortality risk prediction.
Conclusions
After a systematic review, we identified 11 preoperative factors related with an increased postoperative mortality: Cardiogenic shock, urgent surgery, paravalvular abscess, preoperative renal failure, previous cardiac surgery, S. aureus, female sex, age, NHYA class ≥ III, prosthetic valve IE, and multivalvular involvement.
The meta-analysis of each of these factors showed a significant association with an increased in-hospital mortality after surgery for active infective endocarditis.
Change history
24 September 2019
The original version of this article unfortunately contained a mistake.
References
Murdoch DR, Corey GR, Hoen B, Miró JM, Fowler VG, Bayer AS, et al. Clinical presentation, etiology, and outcome of infective endocarditis in the 21st century: the International Collaboration on Endocarditis-Prospective Cohort Study. Arch Intern Med. 2009;169:463–73.
San Román JA, López J, Vilacosta I, Luaces M, Sarriá C, Revilla A, et al. Prognostic stratification of patients with left-sided endocarditis determined at admission. Am J Med. 2007;120:369.e1–7.
Rasmussen RV, Bruun LE, Lund J, Larsen CT, Hassager C, Bruun NE. The impact of cardiac surgery in native valve infective endocarditis: can euroSCORE guide patient selection? Int J Cardiol. 2011;149:304–9.
Chu VH, Park LP, Athan E, Delahaye F, Freiberger T, Lamas C, et al. Association between surgical indications, operative risk, and clinical outcome in infective endocarditis a prospective study from the international collaboration on endocarditis. Circulation. 2015;131:131–40.
Prendergast BD, Tornos P. Surgery for infective endocarditis: who and when? Circulation. 2010;121:1141–52.
Gatti G, Chocron S, Obadia J-F, Duval X, Iung B, Alla F, et al. Using surgical risk scores in nonsurgically treated infective endocarditis patients. Hell J Cardiol HJC Hell Kardiologike Epitheorese. 2019. https://doi.org/10.1016/j.hjc.2019.01.008(Epub ahead of print).
Iung B, Doco-Lecompte T, Chocron S, Strady C, Delahaye F, Le Moing V, et al. Cardiac surgery during the acute phase of infective endocarditis: discrepancies between European Society of Cardiology guidelines and practices. Eur Heart J. 2016;37:840–8.
Gaca JG, Sheng S, Daneshmand MA, O’Brien S, Rankin JS, Brennan JM, et al. Outcomes for endocarditis surgery in North America: a simplified risk scoring system. J Thorac Cardiovasc Surg. 2011;141:98–106.
Olmos C, Vilacosta I, Habib G, Maroto L, Fernández C, López J, et al. Risk score for cardiac surgery in active left-sided infective endocarditis. Heart. 2017;103:1435–42.
Farag M, Borst T, Sabashnikov A, Zeriouh M, Schmack B, Arif R, et al. Surgery for infective endocarditis: outcomes and predictors of mortality in 360 consecutive patients. Med Sci Monit Int Med J Exp Clin Res. 2017;23:3617–26.
Ramos-Martínez A, Calderón-Parra J, Miró JM, Muñoz P, Rodríguez-Abella H, Valerio M, et al. Effect of the type of surgical indication on mortality in patients with infective endocarditis who are rejected for surgical intervention. Int J Cardiol. 2019. https://doi.org/10.1016/j.ijcard.2019.01.014(Epub ahead of print).
Varela Barca L, López-Menéndez J, Navas Elorza E, Moya Mur JL, Centella Hernéndez T, Redondo Palacios A, et al. Long-term prognosis after surgery for infective endocarditis: distinction between predictors of early and late survival. Enfermedades Infecc Microbiol Clín. 2018. https://doi.org/10.1016/j.eimc.2018.10.017(Epub ahead of print).
Varela Barca L, López Menéndez J, Martín García M, Redondo Palacios A, Centella Hernández T, Miguelena Hycka J, et al. Absceso paravalvular en la endocarditis bacteriana: influencia en el pronóstico postoperatorio. Circ Cardiovasc. 2017;24:2–7.
Moher D, Liberati A, Tetzlaff J, Altman DG, Group TP. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLOS Med. 2009;6:e1000097.
Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA. 2000;283:2008–12.
Debray TPA, Damen JAAG, Snell KIE, Ensor J, Hooft L, Reitsma JB, et al. A guide to systematic review and meta-analysis of prediction model performance. BMJ. 2017;356:i6460.
Amilivia G. Infective endocarditis: a better outcome after surgery during the active phase. Crit Care. 2000;2:6339.
Horstkotte D, Follath F, Gutschik E, Lengyel M, Oto A, Pavie A, et al. Guidelines on prevention, diagnosis and treatment of infective endocarditis executive summary; the task force on infective endocarditis of the European society of cardiology. Eur Heart J. 2004;25:267–76.
Pettersson GB. Surgical treatment of endocarditis. Tex Heart Inst J. 2011;38:667–8.
Sexton DJ, Spelman D. Current best practices and guidelines. Assessment and management of complications in infective endocarditis. Cardiol Clin. 2003;21:273–82.
Hayden JA, van der Windt DA, Cartwright JL, Côté P, Bombardier C. Assessing bias in studies of prognostic factors. Ann Intern Med. 2013;158:280–6.
Clark RE. Definitions of terms of the society of thoracic surgeons national cardiac surgery database. Ann Thorac Surg. 1994;58:271–3.
Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016;37:2129–200.
Hollenberg SM, Kavinsky CJ, Parrillo JE. Cardiogenic shock. Ann Intern Med. 1999;131:47–59.
Thomas D, Desruennes M, Jault F, Isnard R, Gandjbakhch I. Cardiac and extracardiac abscesses in bacterial endocarditis. Arch Mal Coeur Vaiss. 1993;86:1825–35.
Edmunds LH, Clark RE, Cohn LH, Grunkemeier GL, Miller DC, Weisel RD. Guidelines for reporting morbidity and mortality after cardiac valvular operations. The American Association for Thoracic Surgery, Ad Hoc Liaison Committee for Standardizing Definitions of Prosthetic Heart Valve Morbidity. Ann Thorac Surg. 1996;62:932–5.
Akins CW, Miller DC, Turina MI, Kouchoukos NT, Blackstone EH, Grunkemeier GL, et al. Guidelines for reporting mortality and morbidity after cardiac valve interventions. Ann Thorac Surg. 2008;85:1490–5.
Doménech JM (2018) Meta-analysis OR, RR, RD, IR, ID, B, MD & R combined: user-written command mar for Stata [computer program]. V1.4.1. Barcelona: Graunt 21.
Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557–60.
Riley RD, Higgins JPT, Deeks JJ. Interpretation of random effects meta-analyses. BMJ. 2011;342:d549.
Barili F, Parolari A, Kappetein PA, Freemantle N. Statistical primer: heterogeneity, random- or fixed-effects model analyses? Interact Cardiovasc Thorac Surg. 2018;27:317–21.
Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315:629–34.
Sterne JAC, Sutton AJ, Ioannidis JPA, Terrin N, Jones DR, Lau J, et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ. 2011;343:d4002.
Rostagno C, Rosso G, Puggelli F, Gelsomino S, Braconi L, Montesi GF, et al. Active infective endocarditis: clinical characteristics and factors related to hospital mortality. Cardiol J. 2010;17:566–73.
Mestres CA, Castro MA, Bernabeu E, Josa M, Cartaná R, Pomar JL, et al. Preoperative risk stratification in infective endocarditis. Does the EuroSCORE model work?Preliminary results. Eur J Cardio-Thorac Surg. 2007;32:281–5.
Hanai M, Hashimoto K, Mashiko K, Sasaki T, Sakamoto Y, Shiratori K, et al. Active infective endocarditis: management and risk analysis of hospital death from 24 years’ experience. Circ J. 2008;72:2062–8.
Fayad G, Leroy G, Devos P, Hervieux E, Senneville E, Koussa M, et al. Characteristics and prognosis of patients requiring valve surgery during active infective endocarditis. J Heart Valve Dis. 2011;20:223–8.
Meszaros K, Nujic S, Sodeck GH, Englberger L, König T, Schönhoff F, et al. Long-term results after operations for active infective endocarditis in native and prosthetic valves. Ann Thorac Surg. 2012;94:1204–10.
Caes F, Bove T, Van Belleghem Y, Vandenplas G, Van Nooten G, Francois K. Reappraisal of a single-centre policy on the contemporary surgical management of active infective endocarditis. Interact Cardiovasc Thorac Surg. 2014;18:169–76.
Hussain ST, Shrestha NK, Gordon SM, Houghtaling PL, Blackstone EH, Pettersson GB. Residual patient, anatomic, and surgical obstacles in treating active left-sided infective endocarditis. J Thorac Cardiovasc Surg. 2014;148:981–8.
Martínez-Sellés M, Muñoz P, Arnáiz A, Moreno M, Gálvez J, Rodríguez-Roda J, et al. Valve surgery in active infective endocarditis: a simple score to predict in-hospital prognosis. Int J Cardiol. 2014;175:133–7.
Spiliopoulos K, Giamouzis G, Haschemi A, Karangelis D, Antonopoulos N, Fink G, et al. Surgical management of infective endocarditis: early and long-term mortality analysis. Single-center experience and brief literature review. Hellenic J Cardiol. 2014;55:462–74.
Marks DJB, Hyams C, Koo CY, Pavlou M, Robbins J, Koo CS, et al. Clinical features, microbiology and surgical outcomes of infective endocarditis: a 13-year study from a UK tertiary cardiothoracic referral centre. QJM Mon J Assoc Physicians. 2015;108:219–29.
Oh T, Voss J, Gamble G, Kang N, Pemberton J. Comparison of contemporary risk scores for predicting outcomes after surgery for active infective endocarditis. Heart Vessels. 2015;30:227–34.
Di Mauro M, Dato GMA, Barili F, Gelsomino S, Sante P, Corte AD, et al. A predictive model for early mortality after surgical treatment of heart valve or prosthesis infective endocarditis. The EndoSCORE. Int J Cardiol. 2017;241:97–102.
Perrotta S, Jeppsson A, Frojd V, Svensson G. Surgical treatment for infective endocarditis: a single-centre experience. Thorac Cardiovasc Surg. 2017;65:166–73.
Varela L, López-Menéndez J, Redondo A, Fajardo ER, Miguelena J, Centella T, et al. Mortality risk prediction in infective endocarditis surgery: reliability analysis of specific scores. Eur J Cardio-Thorac Surg. 2018;53:1049–54.
Fernández-Hidalgo N, Ferreria-González I, Marsal JR, Ribera A, Aznar ML, de Alarcón A, et al. A pragmatic approach for mortality prediction after surgery in infective endocarditis: optimizing and refining EuroSCORE. Clin Microbiol Infect. 2018;24:1102.
David TE, Gavra G, Feindel CM, Regesta T, Armstrong S, Maganti MD. Surgical treatment of active infective endocarditis: a continued challenge. J Thorac Cardiovasc Surg. 2007;133:144–9.
Ferrera C, Vilacosta I, Fernández C, López J, Sarriá C, Olmos C, et al. Early surgery for acute-onset infective endocarditis. Eur J Cardio-Thorac Surg. 2018;54:1060–6.
Garcia-Granja PE, Lopez J, Vilacosta I, Ortiz-Bautista C, Sevilla T, Olmos C, et al. Polymicrobial infective endocarditis: clinical features and prognosis. Medicine. 2015;94:e2000. https://doi.org/10.1097/md.0000000000002000.
Higgins JPT, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928.
De Feo M, Cotrufo M, Carozza A, De Santo LS, Amendolara F, Giordano S, et al. The need for a specific risk prediction system in native valve infective endocarditis surgery. Sci World J. 2012;2012:307571. https://doi.org/10.1100/2012/307571.
Gatti G, Perrotti A, Obadia J-F, Duval X, Iung B, Alla F, et al. Simple scoring system to predict in-hospital mortality after surgery for infective endocarditis. J Am Heart Assoc. 2017;6:e004806.
da Costa MAC, Wollmann DR, Campos ACL, da Cunha CLP, de Carvalho RG, de Andrade DF, et al. Risk index for death by infective endocarditis: a multivariate logistic model. Rev Bras Cir Cardiovasc. 2007;22:192–200.
Nunes MCP, Guimarães-Júnior MH, Murta Pinto PHO, Coelho RMP, Souza Barros TL, de Faleiro Maia NPA, et al. Outcomes of infective endocarditis in the current era: early predictors of a poor prognosis. Int J Infect Dis. 2018;68:102–7.
Sambola A, Fernández-Hidalgo N, Almirante B, Roca I, González-Alujas T, Serra B, et al. Sex differences in native-valve infective endocarditis in a single tertiary-care hospital. Am J Cardiol. 2010;106:92–8.
Nagy M, Alkady H, Abo Senna W, Abdelhay S. Predictors of surgical outcome in isolated prosthetic mitral valve endocarditis. Asian Cardiovasc Thorac Ann. 2018;26:517–23.
Lopez J, Sevilla T, Vilacosta I, Garcia H, Sarria C, Pozo E, et al. Clinical significance of congestive heart failure in prosthetic valve endocarditis. A multicenter study with 257 patients. Rev Espanola Cardiol. 2013;66:384–90.
Mueller XM, Tevaearai HT, Stumpe F, Fischer AP, Hurni M, Ruchat P, et al. Multivalvular surgery for infective endocarditis. Cardiovasc Surg. 1999;7:402–8.
Kim N, Lazar JM, Cunha BA, Liao W, Minnaganti V. Multi-valvular endocarditis. Clin Microbiol Infect. 2000;6:207–12.
Chen C-H, Lo M-C, Hwang K-L, Liu C-E, Young T-G. Infective endocarditis with neurologic complications: 10-year experience. J Microbiol Immunol Infect. 2001;34:119–24.
Liu Y, Zhang H, Liu Y, Han Q, Tang Y, Zhao L, et al. Risk factors and short-term prognosis of preoperative renal insufficiency in infective endocarditis. J Thorac Dis. 2018;10:3679–88.
Tamura K, Arai H, Yoshizaki T. Long-term outcome of active infective endocarditis with renal insufficiency in cardiac surgery. Ann Thorac Cardiovasc Surg. 2012;18:216–21.
David TE, Regesta T, Gavra G, Armstrong S, Maganti MD. Surgical treatment of paravalvular abscess: long-term results. Eur J Cardio-Thorac Surg. 2007;31:43–8.
Fernández-Hidalgo N, Ribera A, Larrosa MN, Viedma E, Origüen J, de Alarcón A, et al. Impact of Staphylococcus aureus phenotype and genotype on the clinical characteristics and outcome of infective endocarditis. A multicentre, longitudinal, prospective, observational study. Clin Microbiol Infect. 2018;24:985–91.
Wang TKM, Wang MTM, Pemberton J. Risk scores and surgery for infective endocarditis: a meta-analysis. Int J Cardiol. 2016;222:1001–2.
Kanafani ZA, Kanj SS, Cabell CH, Cecchi E, de Oliveira Ramos A, Lejko-Zupanc T, et al. Revisiting the effect of referral bias on the clinical spectrum of infective endocarditis in adults. Eur J Clin Microbiol Infect Dis. 2010;29:1203–10.
Acknowledgements
The present authors sincerely thank Noelia Álvarez for his contribution to the literature search.
Funding
This research received no specific grant from any funding agency, commercial or non-profit.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
There was no conflict of interest.
Ethical approval
The Ethical Review Board (ERB) of the Hospital approved the implementation of this study (ERB number 313/2016, approved on November 28, 2016).
Informed consent
The requirement for informed written consent was waived. Patient identification was encoded, complying with the requirements of the Organic Law on Data Protection 15/1999.
Additional information
The original version of this article was revised: The spelling of the name “Nuria Fernández-Hidalgo” was incorrect.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Varela Barca, L., Navas Elorza, E., Fernández-Hidalgo, N. et al. Prognostic factors of mortality after surgery in infective endocarditis: systematic review and meta-analysis. Infection 47, 879–895 (2019). https://doi.org/10.1007/s15010-019-01338-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s15010-019-01338-x