
Abstract
Purpose
Mucormycosis encompasses a group of opportunistic fungal infections caused by Zygomycetes, order Mucorales. Mucormycosis can manifest as rhino-orbito-cerebral, pulmonary, gastrointestinal, cutaneous, and disseminated infections. Pulmonary mucormycosis is the second most common presentation. This manuscript characterizes the demographics, clinical presentation, diagnostic procedures, radiologic findings, therapeutic interventions, and outcome in pulmonary mucormycosis.
Methods
We retrospectively reviewed clinical data of 35 patients with pulmonary mucormycosis from 2000 to 2015. Microbiologic diagnosis was based on positive culture from a sterile site or findings on histopathology consistent with mucormycosis. Independent predictors of 28-day mortality were assessed using logistic regression. Survival curves were estimated using Kaplan–Meier method.
Results
There was male predominance with a mean age of 55 ± 15 years. Analysis of predisposing conditions revealed the prevailing presence of malignancy. Sixty-six percent of patients were receiving immunosuppressive agents. Common presenting clinical findings were fever, neutropenia, dyspnea, and cough. Radiologic findings included pleural effusion and nodules. All patients received medical therapy and 43% underwent additional surgical intervention. Twenty eight day mortality was 29% with concurrent bacteremia found as the sole independent predictor. Similar survival from pulmonary mucormycosis was noted over time.
Conclusions
Pulmonary mucormycosis is an opportunistic angioinvasive fungal infection. Physicians must have a high level of suspicion in immunocompromised patients with fever and respiratory symptoms refractory to antibiotics. A low threshold should be had for performing an invasive procedure to gain reliable diagnosis, as early, aggressive medical and surgical interventions are needed for successful treatment.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Mucormycosis encompasses a group of opportunistic infections caused by fungi in the class Zygomycetes, order Mucorales. Mucormycosis manifests in a variety of organs including rhino-orbito-cerebral, pulmonary, gastrointestinal, cutaneous, as well as disseminated disease. Pulmonary mucormycosis is the second most common presentation, representing up to 58% of infections [1], and is known for its aggressive clinical course with a mortality rate of up to 80% [2].
Although the condition is relatively rare, recent studies suggest that the overall incidence has increased over the past two decades [3–5]. While epidemiologic studies are challenging to conduct, available literature suggests multiple reasons for this increase including rising prevalence of hematologic disorders, changes in immunosuppressive therapy and transplant practices, and earlier recognition due to increased awareness [3, 4]. As a result, mucormycosis has emerged as a clinically significant angioinvasive fungal infection, where recent changes in practice prompt an updated review. The purpose of this study is to further characterize the presentation, management, and outcome of patients with pulmonary mucormycosis over a 15-year period at a single tertiary referral institution.
Materials and methods
Study population
IRB approval was obtained (IRB #12-000207). Consecutive patients hospitalized at Mayo Clinic, Rochester with pulmonary mucormycosis between January 1, 2000 and July 31, 2015 were reviewed for study inclusion. Pulmonary mucormycosis was defined as pulmonary or combined sino-pulmonary disease, with the exclusion of lone rhino-orbito-cerebral involvement and disseminated disease. Disseminated disease was defined as microbiologically confirmed mucormycosis in two or more non-contiguous organs. Microbiologic diagnosis was based on positive culture from a normally sterile site or findings on histopathology from biopsied samples. Patients were excluded if their clinical presentation was not consistent with infection, but more suspected colonization. Demographics, predisposing conditions, clinical presentation, diagnostic procedures, radiologic findings, therapeutic interventions, and in-hospital mortality were collected from the electronic medical record. We defined a cutoff for symptom onset as within 2 weeks of diagnosis. Radiologic imaging obtained within that 2-week time frame including computed tomography (CT) and X-rays of the chest were reviewed.
Statistical analysis
Statistical analysis was performed using JMP Software (Version 10.0, SAS Corporation 2012). Continuous variables were expressed as mean ± standard deviation, and qualitative variables as counts and percentage. Independent predictors of 28-day mortality were assessed using univariable and multivariable logistic regression, adjusting for a priori covariables of age, neutropenia, and chronic kidney disease. Survival curves were estimated using Kaplan–Meier method, stratified into two groups (first 17 consecutively diagnosed patients vs. last 18) to better elucidate survival over time. Two-sided P values <0.05 were considered statistically significant.
Results
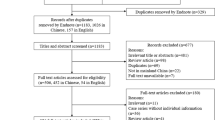
Demographic characteristics of the study population are presented in Table 1. Thirty-five patients fulfilled criteria for diagnosis of pulmonary mucormycosis; 5 were diagnosed in the first 5-year interval of 2000–2005, 12 over 2006–2010, and 18 over 2011–2015. There was a male predominance (69M:31F) with a mean age of 55 ± 15 years (range 22–76). Analysis of predisposing conditions noted extensive presence of malignancy. Of 28 patients with malignancy, the majority were hematologic with 16 cases of leukemia, mostly acute myeloid leukemia, and eight with lymphoma. Only 20% of patients had diabetes mellitus. Of these seven patients, two had poorly controlled disease with hemoglobin A1C above 7.5. Of 13 patients who underwent transplantation, five occurred within a month of mucor infection (Table 2). Sixty-six percent were on immunosuppressive agents at the time of diagnosis. Sixty-eight percent received prophylaxis with anti-fungal agents. Another 20% of patients had concurrent bacteremia. The most common presenting clinical findings were fever, neutropenia, dyspnea, and cough.
Diagnostic procedures included biopsy, bronchoalveolar lavage and sputum/tracheal analysis (Table 2). CT of the chest was obtained in 97% of patients. There was a wide spectrum of radiologic findings (Table 3), with the most common being pleural effusion, followed by nodules, consolidation, and ground glass infiltrates. All patients were medically treated with 17% receiving lone liposomal amphotericin B and 80% receiving combination anti-fungal therapy (Table 4). Mean duration of amphotericin B treatment was 74 ± 90 days (range 2–385 days). Forty-three percent of patients underwent additional surgical interventions, including wedge resection or lobectomy. Thirteen received step down therapy with oral posaconazole. Twenty eight day mortality was 29% with fifty-three percent of deaths attributable to mucormycosis. Cause of death could not be ascertained from the medical record in seven patients. Autopsy was performed in only one patient.
Clinical variables were assessed for their contribution to 28-day mortality (Table 5). Odds ratio for 28-day mortality was statistically significant (OR 17, 95% CI 2.12–369, P value 0.006) only for concurrent bacteremia on univariable analysis. After adjustment for a priori covariables of age, neutropenia, and chronic kidney disease, concurrent bacteremia remained predictive (OR 20.6, 95% CI 1.87–564, P value 0.012). Survival was similar for the first half of consecutive patients compared to the last half (Fig. 1).

Survival curve, stratified by date of diagnosis
Discussion
In our study, pulmonary mucormycosis occurred primarily in middle-aged males with diagnoses of malignancy. The majority of patients presented with neutropenic fever and radiologic findings of pleural effusion and nodules. Eighty percent received multiple anti-fungal agents, and 43% underwent surgical intervention. The 28-day mortality was 29% and concurrent bacteremia was the sole clinical feature associated with mortality. This study suggests increasing frequency of diagnoses over time, yet similar survival when stratified by earlier and more recently diagnosed disease.
Prior reports suggest increasing incidence of mucormycosis over the past few decades [3, 4, 6]. This finding is also supported by our study, with increasing frequency of diagnoses over 5-year intervals. It was previously postulated that the widespread usage of anti-fungal prophylactic agents lacking activity against mucormycosis such as voriconazole may have driven this increase [7], but this association has since been disputed [4]. Of the 35 patients in our study, 24 received prophylaxis with anti-fungal agents with 17 on voriconazole.
Mucormycosis is rarely reported in patients without predisposing conditions. In our study, all patients with pulmonary disease had one or more of these known risk factors. Epidemiologic studies highlight variable distribution of risk factors across geographical regions [6]. For example, mucormycosis is primarily seen in patients with hematologic malignancies in developed nations, in comparison to those with diabetes in developing nations [6]. There may also be an association between underlying disease and the type of mucormycosis presentation, as patients with hematologic malignancy appear more likely to develop pulmonary infection [8, 9], compared to those with diabetes who are more prone to rhino-orbito-cerebral disease [8]. In our study, 80% had a diagnosis of malignancy, predominately hematologic. Of the seven patients with diabetes, only two had poorly controlled disease. These findings suggest weaker association between diabetes mellitus and pulmonary mucormycosis, as compared to other types of mucormycosis presentation.
We found the most common presenting clinical features were fever, neutropenia, dyspnea, and cough, which is in agreement with prior studies [7, 10]. Further complicating early diagnosis is the frequent co-existence of other infections with rates as high as 39% [2, 11]. In our study, 20% of patients had concurrent bacteremia, which in our study was independently associated with 28-day mortality.
In our study, 71% were diagnosed via bronchoscopy; thus, healthcare providers must have a low threshold for performing invasive procedures when indicated. The importance of early diagnosis has led to the development of other diagnostic tests including microbe specific polymerase chain reaction (PCR) [12]. Most cases of pulmonary mucormycosis are caused by fungi in the genus Rhizopus and Mucor, which are susceptible to amphotericin B [13]. While we were unable to ascertain species identification for all specimens, there was a predominance of isolates belonging to both Rhizopus and Mucor in our series.
Previously reported radiologic findings associated with pulmonary mucormycosis include consolidation, opacity, nodules, and cavitation [2, 7, 10, 14]. Although abnormal imaging was present in most patients in our study, these findings were non-specific for fungal infection. Pleural effusion and pulmonary nodules were the more frequent findings. The presence of pleural effusion or multiple nodules were independent predictors of pulmonary mucormycosis in one series [7].
Current guidelines recommend a combined medical and surgical approach to management [5], as anti-fungal agents may have poor penetration at the site of infection. Little evidence exists regarding the increased efficacy of combination anti-fungal agents, compared to monotherapy, outside of animal subjects [5]. Despite this gap in the literature, our observation reveals that combination therapy is often pursued in clinical practice with liposomal amphotericin B and a second anti-fungal agent, primarily posaconazole or caspofungin. There are no current guidelines regarding duration of treatment [5], which remains variable. Unfortunately, operative resection is often precluded in patients who are critically ill. Less than half of our patients underwent additional surgical intervention. After initial infection is stabilized, posaconazole is often used as step down therapy [15], a practice that has become more common in the past 5 years. Recently, isavuconazole was approved for treatment of mucormycosis, typically as an alternative to posaconazole while amphotericin B remains first line therapy [16]. None of our patients received this new agent.
Our study reported a 28-day mortality of 29%, in comparison to a previously reported in-hospital mortality of 80% [2]. Of the 15 patients with a confirmed cause of death secondary to infection, 11 received medical intervention alone and 4 underwent both medical and surgical intervention. These findings suggest overall improved mortality with combination anti-fungal therapy and operative resection, although a combined treatment approach was not associated with improved survival in our study. Analysis revealed only concurrent bacteremia as an independent predictor of 28-day mortality. Interestingly, our study showed no statistically significant association between mortality and recent chemotherapy, neutropenia, or need for mechanical ventilation.
Our study has limitations that merit discussion. This is a single-center study reviewing patients diagnosed and treated over a number of years, reflecting local practices and their evolution over time. Patients referred to a tertiary care center may also have more advanced or refractory disease, and thus may not be fully representative of the general population. As a retrospective study, exact circumstances involved in decision making are difficult to determine. Despite being one of the larger retrospective studies on pulmonary mucormycosis, the absolute number of patients limited more robust statistical analyses.
Conclusion
In conclusion, pulmonary mucormycosis is a life-threatening opportunistic angioinvasive fungal infection with increasing incidence over the past few decades. Because of its non-specific presentation, healthcare providers must have a high level of suspicion in any immunocompromised host with persistent fever and respiratory symptoms refractory to initial antibiotic therapy. Aggressive medical and surgical interventions are the cornerstone of successful treatment.
Author contribution:
All authors contributed substantially to the literature search, study design, data collection, data analysis, data interpretation, writing, and revision of the manuscript.
References
Danion F, Aguilar C, Catherinot E, Alanio A, DeWolf S, Lortholary O, et al. Mucormycosis: new developments into a persistently devastating infection. Semin Respir Crit Care Med. 2015;36:692–705. doi:10.1055/s-0035-1562896.
Tedder M, Spratt JA, Anstadt MP, Hegde SS, Tedder SD, Lowe JE. Pulmonary mucormycosis: results of medical and surgical therapy. Ann Thorac Surg. 1994;57:1044–50.
Bitar D, Van Cauteren D, Lanternier F, Dannaoui E, Che D, Dromer F, et al. Increasing incidence of zygomycosis (mucormycosis), France, 1997–2006. Emerg Infect Dis. 2009;15:1395–401. doi:10.3201/eid1509.090334.
Saegeman V, Maertens J, Meersseman W, Spriet I, Verbeken E, Lagrou K. Increasing incidence of mucormycosis in University Hospital Belgium. Emerg Infect Dis. 2010;16:1456–8. doi:10.3201/eid1609.100276.
Cornely OA, Arikan-Akdagli S, Dannaoui E, Groll AH, Lagrou K, Chakrabarti A, et al. ESCMID and ECMM joint clinical guidelines for the diagnosis and management of mucormycosis 2013. Clin Microbiol Infect. 2014;20:5–26. doi:10.1111/1469-0691.12371.
Chakrabarti A, Das A, Mandal J, Shivaprakash MR, George VK, Tarai B, et al. The rising trend of invasive zygomycosis in patients with uncontrolled diabetes mellitus. Med Mycol. 2006;44:335–42. doi:10.1080/13693780500464930.
Chamilos G, Marom EM, Lewis RE, Lionakis MS, Kontoyiannis DP. Predictors of pulmonary zygomycosis versus invasive pulmonary aspergillosis in patients with cancer. Clin Infect Dis. 2005;41:60–6. doi:10.1086/430710.
Chakrabarti A, Das A, Sharma A, Panda N, Das S, Gupta KL, et al. Ten yearsʼ experience in zygomycosis at a tertiary care centre in India. J Infect. 2001;42:261–6. doi:10.1053/jinf.2001.0831.
Pagano L, Ricci P, Tonso A, Nosari A, Cudillo L, Montillo M, et al. Mucormycosis in patients with haematological malignancies: a retrospective clinical study of 37 cases. GIMEMA Infection Program (Gruppo Italiano Malattie Ematologiche Maligne dellʼAdulto). Br J Haematol. 1997;99:331–6.
McAdams HP, Rosado de Christenson M, Strollo DC, Patz EF Jr. Pulmonary mucormycosis: radiologic findings in 32 cases. AJR Am J Roentgenol. 1997;168:1541–8. doi:10.2214/ajr.168.6.9168721.
Saegeman V, Maertens J, Ectors N, Meersseman W, Lagrou K. Epidemiology of mucormycosis: review of 18 cases in a tertiary care hospital. Med Mycol. 2010;48:245–54. doi:10.1080/13693780903059477.
Hammond SP, Bialek R, Milner DA, Petschnigg EM, Baden LR, Marty FM. Molecular methods to improve diagnosis and identification of mucormycosis. J Clin Microbiol. 2011;49:2151–3. doi:10.1128/jcm.00256-11.
Alvarez E, Sutton DA, Cano J, Fothergill AW, Stchigel A, Rinaldi MG, et al. Spectrum of zygomycete species identified in clinically significant specimens in the United States. J Clin Microbiol. 2009;47:1650–6. doi:10.1128/jcm.00036-09.
Marchiori E, Zanetti G, Escuissato DL, Souza AS Jr, Meirelles GS, Fagundes J, et al. Reversed halo sign: high-resolution CT scan findings in 79 patients. Chest. 2012;141:1260–6. doi:10.1378/chest.11-1050.
Greenberg RN, Mullane K, van Burik JA, Raad I, Abzug MJ, Anstead G, et al. Posaconazole as salvage therapy for zygomycosis. Antimicrob Agents Chemother. 2006;50:126–33. doi:10.1128/aac.50.1.126-133.2006.
Marty FM, Ostrosky-Zeichner L, Cornely OA, Mullane KM, Perfect JR, Thompson GR 3rd, et al. Isavuconazole treatment for mucormycosis: a single-arm open-label trial and case-control analysis. Lancet Infect Dis. 2016;16:828–37. doi:10.1016/s1473-3099(16)00071-2.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors report no proprietary or commercial interest in any product mentioned or concept discussed in this article. This research received no grant from any funding agency in the public, commercial or non-profit sectors.
Rights and permissions
About this article

Cite this article
Lin, E., Moua, T. & Limper, A.H. Pulmonary mucormycosis: clinical features and outcomes. Infection 45, 443–448 (2017). https://doi.org/10.1007/s15010-017-0991-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s15010-017-0991-6