
Abstract
Background
The continuing migration of individuals from geographic areas with high/medium endemicity has determined the arrival of new chronic hepatitis B virus (HBV) carriers in Italy. The magnitude of this phenomenon and clinical/virological features of HBsAg-positive migrants remain not very well defined.
Aims
To evaluate the proportion of HBsAg-positive immigrants enrolled in this multicenter Società Italiana di Malattie Infettive e Tropicali (SIMIT) cross-sectional study and to compare the characteristics of chronic hepatitis B infection in migrants to those of Italian carriers.
Methods
From February 1 to July 31 2008, anonymous data were obtained from all HBsAg-positive patients aged ≥18 years observed at 74 Italian centers of infectious diseases.
Results
Of the 3,760 HBsAg-positive subjects enrolled, 932 (24.8 %) were immigrants, with a prevalent distribution in central to northern Italy. The areas of origin were: Far East (37.1 %), Eastern Europe (35.4 %), Sub-Saharan Africa (17.5 %), North Africa (5.5 %), and 4.5 % from various other sites. Compared to Italian carriers, migrants were significantly younger (median age 34 vs. 52 years), predominantly female (57.5 vs. 31 %), and most often at first observation (incident cases 34.2 vs. 13.3 %). HBeAg-positives were more frequent among migrants (27.5 vs. 14 %). Genotype D, found in 87.8 % of Italian carriers, was present in only 40 % of migrants, who were more frequently inactive HBV carriers, with a lower prevalence of chronic hepatitis, cirrhosis, and hepatocellular carcinoma (HCC). Only 27.1 % of migrants received antiviral treatment compared to 50.3 % of Italians.
Conclusions
Twenty-five percent of all HBV carriers examined at Italian centers was composed of immigrants with demographic, serological, and virological characteristics that differed from those of natives and appeared to have an inferior access to treatment.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The epidemiology of hepatitis B virus (HBV) infection in Italy has changed remarkably in the last 30 years, due to the introduction of mandatory anti-HBV vaccination in 1991 and the overall improvement of socio-economic and health conditions. Currently, the incidence of acute HBV hepatitis is <1 case/100,000 inhabitants, with new cases almost exclusively involving adults for whom the infection is mainly transmitted by a sexual route [1]. The reduced HBV circulation in the population and the lower rate of evolution to chronic disease in adults, when compared to young people, has progressively decreased the reservoir of HBV chronic carriers. Consequently, this factor has also led to a reduction in HBsAg prevalence, which is now <2 %, thus, permitting the inclusion of Italy among countries with a low endemicity [2].
However, since the end of the 1970s, Italy, together with other European countries, has become one of the main destinations of migratory flows from poverty-stricken countries. The available statistics, regarding only the proportion of legal immigrants and, thus, underestimating the real number of immigrants entering the country, evidenced that they represented 7 % of the entire population resident in Italy in 2010 [3]. This figure indicates an increasing trend over time during the last several decades, as the estimated rate of immigrants compared to the entire population was only 1.7–1.9 % in 1995–1996.
This constant migration of people from regions with an intermediate (HBsAg carriers prevalence 2–8 %) or high (>8 %) HBV endemicity implies a presumable increase in the number of HBV carriers in Italy, whose actual size is difficult to establish because of the limited number of studies on HBsAg prevalence in the migrant population. A large cohort study of pregnant women evidenced a 5.9 % prevalence of HBsAg among non-Europeans versus 1.4 % among Italian women [4]. These results are similar to those obtained by the Italian Society of Infectious Diseases in 2002, which recorded a 5.4 % prevalence of HBsAg among hospitalized immigrant patients [5], 12.5 % of whom had a diagnosis of hepatitis (acute or chronic), mainly due to HBV, and, only in a minority of cases, to hepatitis C virus (HCV). This pattern is in contrast to the current low level of HBV-related hepatitis in the Italian population, in which acute forms have become very rare and chronic disease has dramatically decreased [6]. More recently, a lower prevalence for HBsAg has been reported in both Italian and immigrant women (0.4 vs. 2.5 %) [7].
In addition, it must be considered that HBV-carrier immigrants present demographical, serological, and virological characteristics differing from those of autochthonous carriers. Among these features, the HBV genotype might play an important role, even if it is not yet completely understood, as an increasing amount of reports in the literature suggests that genotype might influence disease progression in terms of the rate of seroconversion to anti-HBe, core promoter and pre-core mutations, severity of liver damage, and response to antiviral therapy, including interferon [8–14]. An accurate knowledge of the epidemiology and clinical characteristics of HBV infection among immigrants in Italy is required in order to empower screening programs, improve access to care, and facilitate management of the disease in this special population. Furthermore, recently, it has been demonstrated that the evaluation of the prevalence of viral infectious diseases among immigrants is likely to be cost-effective and necessary for the planning of health control strategies [15, 16].
The aim of our study was to evaluate the proportion of migrants in a large cohort of HBsAg-positive subjects enrolled in the SIMIT (Società Italiana di Malattie Infettive e Tropicali) multicenter study regarding chronic HBV infection in Italy and then compare the characteristics of the chronic HBV infection in migrants with respect to native patients.
Patients and methods
This study is a portion of a large, cross-sectional observational study on the characteristics of HBV infection in the Italian population which, from February 1st to July 31st 2008, recruited patients in 74 infectious disease centers throughout the Italian regions.
The inclusion criteria included: age ≥18 years, chronic HBV infection defined as HBsAg positivity for at least 6 months, and at least one visit to one of the participating centers during the study period. For patients at first observation, chronic HBV infection was diagnosed if the documentation of a previous HBsAg positivity (at least 6 months previously) was available. For each enrolled patient, the following data were recorded: gender, year of birth, country of origin, alcohol intake (defined as previous and/or current consumption >12.5 g/dL alcohol/day), date of first HBsAg-positive test, alanine transaminase (ALT) levels (IU/ml), other hepatitis markers (HBeAg, anti-HBe, HBV genotype, anti-HCV, anti-HDV), anti-human immunodeficiency virus (HIV) testing, and HBV-DNA IU/ml (with indication of the method used and corresponding detection limits). In addition, based on medical history, physical examination, laboratory parameters, and abdominal ultrasonography, patients were classified by clinicians into three categories: chronic inactive carriers (HBV-DNA levels persistently below 2,000 IU/ml and continually normal ALT levels), active carriers with chronic hepatitis, and active carriers with cirrhosis (including the Child–Pugh score in the latter category). However, due to an inadequate length of follow-up, the diagnosis of inactive carrier for immigrants should be presumed, especially for those at first diagnosis. In patients for whom a liver biopsy had been performed, grading, staging, and the method used for histology classification were recorded. When present, the diagnosis of hepatocellular carcinoma (HCC) had to be indicated. Lastly, the type and duration of all anti-HBV treatments, previously or currently administered, were registered.
The study did not require approval from the ethics committee, since it was performed as an observational study in the context of normal clinical routine and according to the Helsinki Declaration principles. However, all patients provided informed consent for the use of their data for research purposes. Data were collected on an anonymous form at each participating center and sent to the coordinating center.
Results
During the study period, 3,760 HBsAg-positive carriers were enrolled, 932 of whom (24.8 %) were immigrants born outside Italy. The demographical, serological, and virological features of HBV infection in the foreign-born population compared to natives are shown in Table 1, while the differential characteristics of migrant patients according to their region of origin are presented in Table 2.
Demographical characteristics
Migrant patients were not uniformly distributed throughout the national territory, as 55.9 % visited the infectious disease units in central Italy, 36.1 % in the north, and only 8 % in southern Italy. Their region of origin was Asia in 37.1 % of cases, Eastern Europe in 35.4 %, Sub-Saharan Africa in 17.5 %, and North Africa in 5.5 %, while the remaining 4.5 % included patients from other countries (Western Europe, South America, and Middle East).
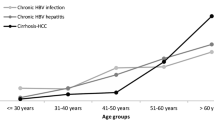
The HBsAg-positive immigrants were significantly younger than natives, with a median age of 34 (range 18–77) versus 52 years (range 18–93), respectively (p < 0.001). The majority of immigrants from all areas were included in the age level ranging between 30 and 49 years. However, the greatest difference between the two groups was observed in the proportion of patients ≥60 years of age, representing 29.4 % in the Italian population versus only 1.6 % in the migrant group, independent of the country of origin. Moreover, the migrant HBsAg-positive population included a greater proportion of women than the Italian population (57.5 vs. 31.0 %, respectively, p < 0.001). When considering the gender distribution, this appeared to be correlated to the region of origin. In fact, the higher prevalence of females in the immigrant group was mainly due to the large number of Asiatic and Eastern European women, while the proportion of males was higher than females among Northern and Sub-Saharan Africans, and did not differ from the Italian population.
Alcohol intake was more frequently reported for natives than for migrant people in our cohort (60.0 vs. 41.4, respectively, p < 0.001).
Immigrants were more likely to be at their first observation for HBV infection, with a significantly higher proportion of incident cases, 34.2 %, compared to 13.3 % in Italians (p < 0.001).
Serological and virological characteristics
A higher prevalence of patients with HBeAg-positive chronic hepatitis was observed in immigrants when compared to natives (27.5 vs. 14.0 %, respectively, p < 0.001); 46.1 % of immigrants of Asian origin were HBeAg-positive.
Overall, the migrant subjects presented a lower probability of co-infection with other hepatitis viruses, such as HDV (4.6 vs. 7.6 % in Italians, p = 0.003), HCV (3.2 vs. 9.7 %, respectively, p < 0.001), as well as HIV (8.6 vs. 15.5 %, p < 0.001). However, when considering the country of origin, as expected, an elevated prevalence of HDV co-infection was observed in the group of Eastern European patients (8.7 %). In addition, HIV–HBV co-infection was more frequently recorded among Sub-Saharan African patients (26.3 %) (Table 2). HIV–HBV co-infected immigrants were less likely to present undetectable HIV-RNA levels than co-infected Italian patients (30.9 vs. 51.5 %, respectively, p = 0.014) and presented a significantly lower median CD4 count (355 cells/mm3, range 8–1,280 vs. 441.5 cells/mm3, range 11–4216, p < 0.001).
Serum HBV-DNA levels were detectable (>400 IU/ml) more frequently in the migrant (59.1 % of cases) than in the autochthonous population (46.2 %) (p < 0.001); this difference remained significant (p < 0.001) even when considering only the proportion of patients who were not receiving treatment at the time of analysis.
The HBV genotype was available for 226 patients (45 immigrants and 181 Italians). A wider diversification and a higher frequency of non-D genotypes was found among immigrants; in fact, while genotype D was responsible for 87.8 % of infections in Italian patients, it was observed in only 40 % of immigrants. The distribution of the main non-D genotypes in the two groups is shown in Fig. 1.

Hepatitis B virus (HBV) genotype distribution in the native and foreign-born populations
Diagnosis and antiviral treatment
According to clinical and histological criteria, HBV carriers were classified into three categories: inactive carriers, active carriers with chronic hepatitis, and cirrhosis (Table 3). Despite the greater number of HBV-DNA-positive patients, immigrants seemed to have less severe hepatic damage, with an overall higher prevalence of inactive carriers (37.8 vs. 15.8 % in natives), and a smaller proportion of patients with chronic hepatitis (55.6 vs. 72.0 % in the two groups, respectively) and cirrhosis (6.7 vs. 12.2 %, respectively) (p < 0.001). However, when analyzing the severity of liver cirrhosis according to the Child–Pugh classification, no remarkable differences were observed between cirrhotic immigrants and cirrhotic Italians.
A liver biopsy had been performed at a certain time during the patient’s history in 16.2 % of immigrant patients and in 35.3 % of Italians (p < 0.001). According to histological examination, no significant differences were observed in the relative proportion of patients classified as inactive carrier (7.3 vs. 3.8 %), chronic hepatitis (78.8 vs. 82.4 %), and cirrhosis patients (13.9 vs. 13.8 %) in the two groups.
A diagnosis of HCC was recorded in 2.4 % of Italians and in 0.3 % of immigrants, corresponding to 18.5 and 4.8 % of all patients with cirrhosis, respectively.
Lastly, the history of previous and/or current antiviral treatment against HBV was analyzed. A significantly higher percentage of immigrants (71.2 %) reported that they had never received previous antiviral therapies compared to natives (50.1 %) (p < 0.001). Also, the proportion of patients being treated with any antiviral regimen at the time of the survey was slightly lower for immigrants (27.1 %) than for Italians (50.3 %) (p = 0.08). The type of antiviral regimen (both in the past and at the time of analysis) chosen by clinicians for the two groups of patients is reported in Fig. 2.

Relative proportions of migrant and native patients treated with an antiviral therapy in the past (a) or at the time of study (b)
Correlation of patient characteristics with stage of infection
In order to individuate factors independently associated with the presence of liver cirrhosis as determined by histology, two models of univariate and multivariate analysis were performed, including the following patient characteristics: gender, age, nationality, alcohol intake, HBV genotype, HBeAg status, HBV-DNA positivity, and previous and current antiviral therapy. No association was found between viral genotype (D vs. non-D) and liver cirrhosis; due to the limited number of viral genotypes tested, this variable was not included in the multivariate analysis.
Detectable viremia (HBV-DNA >400 IU/ml), age >50 years, and previous/current antiviral therapy were associated with liver cirrhosis at univariate analysis; however, only viremia [odds ratio (OR) 0.46, 95 % confidence interval (CI) 0.28–0.74, p = 0.001), age (OR 2.74, 95 % CI 1.68–4.45, p < 0.001), and nationality (OR 0.52, 95 % CI 0.28–0.98, p = 0.044), remained independently associated with outcome at multivariate analysis (Table 4).
Discussion
The migratory flow of individuals from countries with intermediate/high HBV endemicity has determined the arrival of new HBV chronic carriers in Italy, which, nevertheless, still remains a country with low endemicity for HBV infection. In this SIMIT multicenter, cross-sectional study on chronic HBV infection in Italy, 3,760 HBsAg-positive carriers were consecutively enrolled, 932 of whom (24.8 %) were immigrants. This study reveals important findings of epidemiological and public health interest, as it contributes to a better characterization of HBV infection in immigrants living in Italy, whose features are not well defined due to the extensive number of illegal immigrants, the rapid dynamics of migratory flows, and the lack of effective surveillance tools.
In 2006–2007, a previous cross-sectional multicenter study was conducted in Italy which enrolled 1,396 HBsAg chronic carriers, but only 104 (7.4 %) of those were immigrants [17]. In our study, for the first time in a large cohort of immigrants, the epidemiological, virological, and clinical characteristics of HBV infection were compared with those of the native HBV carriers.
The majority of our migrant patients came from Asia (37.1 %) and from Eastern Europe (35.4 %), followed by Sub-Saharan Africa (17.5 %), thus, reflecting the actual migratory flow to Italy [3]. The geographic distribution of these HBsAg-positive migrants was not uniform throughout the national territory; in fact, more than 80 % resided in central to northern Italy. The high percentage of migrant patients recorded from sites in central Italy could depend on a bias, due to the presence of a large group of Chinese migrants living in Tuscany. This bias might also explain the higher frequency of females among migrant HBsAg-positive patients (57.5 vs. 31 % among Italians). This fact does not reflect a different gender distribution of HBV in the country of origin, but is simply due to the prevalence of females among immigrants in these areas due to work possibilities.
As expected, migrant HBV chronic carriers were younger than Italian carriers due to the higher rate of vertically transmitted HBV infection and decreased HBV vaccination in their country of origin, thus, determining the greater frequency of HBeAg-positive carriers among immigrants (27.5 vs. 14 % in natives). Overall, co-infections with HCV, HDV, and HIV were also less frequent among HBsAg-positive migrants compared to Italians. Interestingly, anti-HDV antibodies were found in 190 of 2,501 (7.6 %) HBsAg-positive tested Italian carriers, thereby, confirming the downtrend of HDV co-infection reported in past several years [18]. A higher frequency of non-D genotypes was found among immigrants. Recently, there have been several studies reporting the influence of HBV genotypes on the clinical features and on the response to antiviral treatment [8–14]. Therefore, the different genotypes might require a different clinical and therapeutic approach.
Based on the clinical classification, a diagnosis of inactive carrier was formulated by clinicians more frequently for migrants than nationals; however, no significant differences between the two groups were observed if a histological criterion was used. This discrepancy is probably due to the fact that a greater number of first diagnoses was recorded for immigrants compared to Italians. Consequently, a precise diagnostic allocation for immigrants at first diagnosis, particularly for those with an inactive carrier state, was not possible, since it is well known that serum ALT and HBV-DNA levels may fluctuate over time [19], thus, requiring an adequate follow-up.
Although marked differences were not noted for liver disease severity, a smaller proportion of migrant patients were treated with antiviral drugs, both in the past and at the time of study, a result which leads to considerations regarding present barriers to the access of medical care by this high-risk population.
In conclusion, our study demonstrates that immigrants represent an increasing segment of patients who refer to our centers. Chronic HBV immigrant carriers have demographic, serological, and virological characteristics differing from those of native carriers. Therefore, a more profound knowledge of the epidemiology and clinical characteristics of HBV infection among immigrants in Italy is required in order to empower screening programs, improve access to care, and facilitate management of the disease in this population.
References
Stroffolini T, Mele A, Tosti ME, et al. The impact of hepatitis B mass immunization campaign on the incidence and risk factors of acute hepatitis B in Italy. J Hepatol. 2000;33:980–5.
Stroffolini T. The changing pattern of hepatitis B virus infection over the past three decades in Italy. Dig liver Dis. 2005;37:622–627.
Caritas Italiana/Migrantes. Dossier Statistico Immigrazione 2011. XXI Rapporto. Edizioni Idos Roma. http://www.dossierimmigrazione.it/libro.php?cid=47_52&pid=145.
Stroffolini T, Bianco E, Szklo A, et al. Factors affecting the compliance of the antenatal hepatitis B screening programme in Italy. Vaccine. 2003;21:1246–9.
Scotto G, Saracino A, Pempinello R, et al.; Gruppo Italiano per lo Studio delle Malattie Infettive negli Immigrati. Epidemiologic multicenter study of the prevalence of hepatitis in hospitalised immigrants in Italy in the year 2002. Ann Ig. 2005;17:11–8.
Da Villa G, Romanò L, Sepe A, et al. Impact of hepatitis B vaccination in a highly endemic area of south Italy and long-term duration of anti-HBs antibody in two cohorts of vaccinated individuals. Vaccine. 2007;25:3133–6.
Spada E, Tosti ME, Zuccaro O, Stroffolini T, Mele A; Collaborating Study Group. Evaluation of the compliance with the protocol for preventing perinatal hepatitis B infection in Italy. J Infect. 2011;62:165–71.
Sánchez-Tapias JM, Costa J, Mas A, Bruguera M, Rodés J. Influence of hepatitis B virus genotype on the long-term outcome of chronic hepatitis B in western patients. Gastroenterology. 2002;123:1848–56.
Yuen MF, Sablon E, Yuan HJ, et al. Significance of hepatitis B genotype in acute exacerbation, HBeAg seroconversion, cirrhosis-related complications, and hepatocellular carcinoma. Hepatology. 2003;37:562–7.
Sumi H, Yokosuka O, Seki N, et al. Influence of hepatitis B virus genotypes on the progression of chronic type B liver disease. Hepatology. 2003;37:19–26.
McMahon BJ. The influence of hepatitis B virus genotype and subgenotype on the natural history of chronic hepatitis B. Hepatol Int. 2009;3:334–42.
Cao GW. Clinical relevance and public health significance of hepatitis B virus genomic variations. World J Gastroenterol. 2009;15:5761–9.
Kurbanov F, Tanaka Y, Mizokami M. Geographical and genetic diversity of the human hepatitis B virus. Hepatol Res. 2010;40:14–30.
Lin CL, Kao JH. The clinical implications of hepatitis B virus genotype: recent advances. J Gastroenterol Hepatol. 2011;26:123–30.
Almasio PL, Babudieri S, Barbarini G, et al. Recommendations for the prevention, diagnosis, and treatment of chronic hepatitis B and C in special population groups (migrants, intravenous drug users and prison inmates). Dig Liver Dis. 2011;43:589–95.
Veldhuijzen IK, Toy M, Hahné SJ, et al. Screening and early treatment of migrants for chronic hepatitis B virus infection is cost-effective. Gastroenterology. 2010;138:522–30.
Stroffolini T, Almasio PL, Sagnelli E, et al. Evolving clinical landscape of chronic hepatitis B: a multicenter Italian study. J Med Virol. 2009;81:1999–2006.
Gaeta GB, Stroffolini T, Chiaramonte M, et al. Chronic hepatitis D: a vanishing disease? An Italian multicenter study. Hepatology. 2000;32:824–7.
Fattovich G, Bortolotti F, Donato F. Natural history of chronic hepatitis B: special emphasis on disease progression and prognostic factors. J Hepatol. 2008;48:335–52.
Acknowledgments
The authors are grateful to Ms. Paulene Butts for her assistance in the preparation of the manuscript.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Fasano, M., Saracino, A., Carosi, G. et al. Hepatitis B and immigrants: a SIMIT multicenter cross-sectional study. Infection 41, 53–59 (2013). https://doi.org/10.1007/s15010-012-0384-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s15010-012-0384-9