
Abstract
In the case of mild papilledema, fundoscopy findings may sometimes be insufficient, leading to false and misleading indices in the diagnosis of early-stage idiopathic intracranial hypertension (IIH). This study aims to evaluate these patients through optic coherence tomography (OCT). The study included 54 individuals diagnosed with IIH and 48 healthy individuals in the control group. All patients underwent neurological and ophthalmologic examinations. Opening pressure values of patients’ cerebrospinal fluid (CSF) were recorded. We measured the thickness of the retinal nerve fiber layer (RNFL) and the ganglion cell complex, cup volume, and the optical disc area, as well as the neuroretinal rim in both groups. A total of 108 eyes from the patient group and 96 eyes from the control group were evaluated. It was found that the mean value of the RNFL thickness of the IIH patients was greater than the control group in the following eight segments: superior nasal, superior temporal, inferior nasal, inferior temporal, nasal superior, nasal inferior, temporal superior, and temporal inferior (p < 0.01 for all). In contrast to the control group, the disc and rim area values of the patient group were higher (p < 0.01), while the cup volume was smaller (p < 0.01) than in the control group. In the patient group, a positive correlation was observed between the papilledema grade and the RNFL thickness (r = 0.64, p < 0.01), CSF opening pressure (r = 0.59, p < 0.01), disc area (r = 0.68, p < 0.01), and rim area (r = 0.70, p < 0.01). Furthermore, RNFL thickness, CSF opening pressure (r = 0.61, p < 0.01), disc area (r = 0.71, p < 0.01), and rim area (r = 0.71, p < 0.01) values were determined to be positively correlated to each other. OCT is believed to contribute to the diagnosis of IIH, by providing reliable data on optical cup volume, optical disc and rim area, and a greater RNFL thickness.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Idiopathic intracranial hypertension (IIH) is characterized by an increase in cerebrospinal fluid (CSF) pressure without a space-occupying brain lesion or ventricular dilatation [1, 2]. IIH incidence is 0.03–2/10,000/year, but in obese women of childbearing age, the incidence was reported as 2.7–19/10,0000/year [3]. Headache, papilledema, transient visual obscurations, blurred vision, diplopia, and tinnitus are observed in IIH patients [1,2,3,4,5,6]. The most significant complication associated with IIH is permanent vision loss [7]. As such, it is important to methodically follow and monitor patients with IIH.
Papilledema is the most serious manifestation of IIH [4,5,6,7]. Impaired axoplasmic flow, secondary to increased intracranial pressure and increased perineural pressure, cause optic disc swelling or papilledema [8]; it is generally symmetrical, and rarely observed as asymmetrical or unilateral [4, 5]. Clinical papilledema is not seen in more than 6% of IIH patients, even with cases of optic nerve damage [9]. Several features of pseudo-optic disc edema include optic nerve drusen, tilted optic disc, myelinated fibers, crowded optic disc, and optic nerve hypoplasia, which may be confused with papilledema. These features should be considered in rendering a differential diagnosis during funduscopic examinations, especially if the papilledema is asymmetrical and mild. As funduscopic examinations partly rely on subjective interpretations, patient evaluations may differ. Thus, it is important that experienced physicians perform them [11]. The Frisen Scale is based on a descriptive inspection of various images, monitored by the fundoscopy; thus, difficulties may arise in the evaluation of mild to moderate changes that emerge at a time when the papilledema phase is determined and followed up [12]. Since quantitative data is provided by OCT, it is wise to perform an objective evaluation [12,13,14].
Recently, OCT has become a reliable diagnostic method in neuro-ophthalmologic diseases. It has been reported that OCT is a dependable tool for evaluation of the retinal axonal damage, which is the peripheral reflection of axonal degeneration in the brain for Alzheimer’s, Parkinson’s, Wilson’s, multiple sclerosis (MS), and neuromyelitis optica [14,15,16]. OCT is a non-invasive technique that enables high-resolution visualization of the retina by generating cross-sectional patterns. In monitoring papilledema, effects of intra or extracellular edema, and thinning of peripapillary RNFL associated with axonal loss can be evaluated quantitatively at each phase with a replicable, effortless method [14, 17].
OCT facilitates the evaluation of macular and RNFL thickness, and particularly determining the quantitative axonal loss in cases of optic neuropathy. Since the ganglion cell complex (GCC) plays a strong role in the thickness of the macular area, the measured loss of GCC highlights the estimate of macular thickness in the event of optic neuropathy [18]. Changes in OCT parameters, such as optical disc area, neuro-rim thickness, and cup volume have been reported in cases of IIH, cup/disc area, cup /disc volume, and cup/disc height; however, they have not been thoroughly investigated in IHH [19].
The aim of this study was to evaluate changes in the optic nerve head and macula of IIH patients by OCT and to then compare the relevant data with the control group.
Methods
Subjects
We prospectively recruited 67 consecutive patients, who were suspected of having IIH. Thirteen of the 67 patients were not appropriate for this study. Fifty-four study patients had recently been diagnosed with IIH, according to the International Classification of Headache Disorders (ICHD) version beta-3 [20]. Forty-eight healthy individuals were also included in the control group.
Inclusion criteria: age > 18, high CSF opening pressure (ICP ≥ 250 mm/CSF), normal MRI and MRI venography, normal CSF composition and cytology, normal neurological examination except for papilledema. Patients who had other ocular or neurological diseases, or other medical diseases, were excluded from the study.
All patients and controls were informed about the details of the study. The study was approved by the Local Ethics Committee of the Diskapi Yildirim Beyazit Training and Research Hospital. All investigators confirmed the ethical standards as described in the Declaration of Helsinki.
Neurological and ophthalmologic evaluation
Patients with papilledema who were clinically assessed to have IIH were subjected to evaluation by the same neurologists and ophthalmologists. The ophthalmologic examination included the best corrected visual activity, biomicroscopy of the anterior and posterior segment, and standard automated perimetry. Perimetric measurements were made using a Humphrey Field Analyzer. Reliability in visual field testing is assessed by parameters such as fixation losses (FL), false negatives (FN), and false positives (FP). According to Humphrey Field Analyzer software, the visual field is considered to be reliable at values below 33% for FP and FN and below 20% for fixation loss [21, 22]. Mean deviation (MD) and pattern standard deviation (PSD) were recorded. Severity of papilledema was graded with the Frisen Scale.
Cerebrospinal fluid
Every patient underwent a lumbar puncture within 24 h of the OCT evaluation, and were not medicated prior to undergoing it. Situated in the left lateral decubitus position, patients were sterilized locally, and the subarachnoid space was reached at the L3–4 or L4–5 interspace. The opening pressure was measured using an 18- or 20-gauge spinal needle with a monometer positioned at a 90° angle. The CSF analyses included glucose, lactate, total protein, and cell count. The biochemical composition was consistently normal. Cells were not observed in CSF. Normal values for CSF were glucose 40–85 mg/dL (two-thirds of the blood glucose), lactate less than 35 mg/dL, protein (total) 15–45 mg/dL, and leukocytes 0–5/µL.
OCT
This manuscript follows the Advised Protocol for OCT Study Terminology and Elements Recommendations for reporting quantitative OCT studies [23]. A total of 108 eyes from the patient group and 96 eyes from the control group were evaluated. OCT scanning was performed on the same day as the qualifying ophthalmological examination by experienced operators, using the RTVue SD-OCT system (RTVue-XR 100 Avanti software v.6.1, Optovue, Inc., Fremont, CA, USA). OCT was performed on both eyes after the pupils underwent dilatation in a dark room. The macula and optic nerve head were evaluated, while the RNFL and GCC thicknesses were measured separately. Measurements were repeated three times for each eye to reduce measurement errors.
The RNFL 3.45 protocol was used for peripapillary RNFL analysis, with the thickness measured at a diameter of 3.45 mm around the center of the optic disc. The total number of A-scans with the circumference was 2225. Results were displayed on a color map with customized software, with normative data adjusted for age and optic disc size. A peripapillary RNFL thickness map was expressed as a numerical value, and the color code in each of the eight segments for the four quadrants was: superior (46°–135°), nasal (316°–45° for the right and 136°–225° for the left), inferior (226°–315°), and temporal (136°–225° for the right and 316°–45° for the left) (Fig. 1).

Peripapillary RNLF thickness map. a Superior temporal. b Superior nasal. c Nasal superior. d Nasal inferior. e İnferior nasal. f İnferior temporal. g Temporal inferior. h Temporal superior
Ganglion cell complex thickness was measured using the GCC protocol, composed of 15 vertically oriented B scans of 7.0 mm in length (800 A scans each), separated by 0.50 mm, along with a single horizontally oriented B scan of 7.0 mm in length (12,934 A-scans), all centered on the macula by the operator (the center of the GCC scan was shifted 1.0 mm temporally to better sample the temporal peripheral macula with the nasal visual field).
Statistics
Data were evaluated with the SPSS 22 program (Statistical Package for the Social Sciences Inc., Chicago, IL, USA). Descriptive values were presented as “number” and “percentage”. The variables were identified as mean ± standard deviation or median (minimum–maximum) according to the distribution of data. The Student’s t test or the Mann–Whitney U test demonstrated distributions of the paired comparison of the numerical data, with significance levels at p < 0.05. The relationship between variables was tested with Spearman’s rank correlation coefficient, and the significance level at p < 0.05.
Results
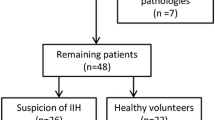
Sixty-seven consecutive patients suspected of having IIH were evaluated. Six patients with pseudopapilledema (two had optic disc drusen, one had tilted optic disc, and three had crowded disc), with seven patients with ocular pathology due to systemic disease (two were found to have diabetic retinopathy, two had hypertensive retinopathy, and three had optic neuritis) were excluded (Fig. 2).

The distribution of papillary edema, pseudopapillary edema and other pathologies in patients with suspected IHH
Fifty-four IIH patients (50 females, 4 males; mean age 35.51 ± 11.52) and 45 healthy individuals as the control group were included in the study (41 females, 4 males; mean age 35.10 ± 10.49). Demographical and clinical patient findings can be seen in Table 1.
The mean RNFL thickness of the patient group showed a statistically significant increase compared to the control group (p < 0.01). After evaluating the eyes of both group members in eight quadrants, the patient group’s RNFL thickness in all segments was found to be statistically greater in contrast to the control group (p < 0.01 for all segments). There was no statistical difference in the mean GCC thickness between the patient and control group. Compared to the control group, the disc and rim area values of the patient group were higher, whereas their cup volume was smaller than the control group (p < 0.01 for all). Subsequently, it was found that the cup/disc area, cup/disc volume, and the cup/disc height of the patient group were statistically smaller than the control group (p < 0.01 for all); see Table 2.
Correlation
In the patient group, a positive correlation was determined between the grade of papilledema and the CSF opening pressure (r = 0.59, p < 0.01), the mean RNFL thickness (r = 0.64, p < 0.01), (r = 0.68, p < 0.01), and the rim area (r = 0.70, p < 0.01). RNFL thickness was positively correlated with the grade of papilledema (r = 0.64, p < 0.01), (r = 0.61, p < 0.01), the disc area (r = 0.71, p < 0.01), and the rim area (r = 0.71, p < 0.01). A positive correlation was detected between the CSF opening pressure, the RNFL thickness (Fig. 3), the disc and rim area (r = 0.59, p < 0.01), (r = 0.54, p < 0.01), and (r = 0.52, p < 0.01). Forty patients who met the criteria for visual field results were appropriate for perimetric evaluation criteria. The disc and rim area were positively correlated (r = 0.98, p < 0.01); see Table 3.

Correlation of CSF opening pressure between RNLF thickness. CSF cerebrospinal fluid (mmH2O), RNLF retinal nerve layer fiber (µm)
Discussion
In our study, it was found that the RNFL thickness measured in IIH patients with papilledema was above normal in all segments. These findings led us to conclude that OCT could be a useful tool in determining the diagnosis of IIH earlier.
It has been reported in other studies that RNFL thickness of newly diagnosed IIH patients was increased in four quadrants: superior, inferior, nasal, and temporal [24,25,26,27]. Moreover, the mean RNFL thickness and the temporal and superior quadrants in children’s newly diagnosed IIH were found to be increased [28]. However, in several studies, evaluating a limited number of IIH patients experiencing acute and chronic stages in combination, it was reported that the RNFL thickness resembled that of the control group [19, 29]. Similar to results reported in the literature, our study determined a positive correlation between CFS opening pressure and peripapillary RNFL thickness [21, 27] and the grade of papilledema [24, 27, 30]. These findings indicate that OCT may help detect the severity of the intracranial pressure increase, as well as diagnosing papilledema in the acute period. Contradictory results were reported by several studies investigating the relationship between CSF opening pressure and RNFL thickness [27]. These conflicting results are likely associated with whether the disease is in the acute or chronic stage, as well as the interval of time between the performance of lumbar puncture and OCT.
Different results regarding GCC thickness of IIH patients were obtained. It has been reported that secondary macular edema or hemorrhage could develop in the acute period due to increased intracranial pressure, which may lead to confusion for the measurement of macular thickness [18]. Because the macular area contains RNFL, some fibers may swell in the acute period and affect the measurement. On the other hand, several cases in which GCC thickness decreased as RNFL thickness increased were identified among IIH patients. It has been argued that this might be associated with early retrograde optic atrophy. A decrease in macular thickness in the chronic period is related to axonal loss [9, 26]. Our findings show that the GCC thickness of both groups were similar, which can be attributed to the absence of macular edema and optic atrophy among the patients.
The neuroretinal rim refers to the intrapapillary extensions of retinal and optic nerve fibers, which suggests that intracranial pressure initially affects it [19]. It was found that the retinal rim area of the patient group was greater than the control group. Another study evaluated the neuroretinal rim with similar findings [19]. Our study indicated the optic disc area of IIH patients was greater than the control group, and a parallel increase in optic disc area showed an increase in the neuroretinal rim.
The cup volume values of the IIH patients were lower than those of the control group, with most values measured as zero. The zero cup volume, reported to be a remarkable phenomenon in IIH, may be affected by different segmentations of the swelled optic nerve head [19]. We detected that the cup/disc area, cup/disc volume, and cup/disc height ratios of both eyes of the patient group were lower than the control group; this finding prompted us to consider that the increased edema may result from a decrease in area, volume, and cup height. Although a reduced cup/disc area was reported, there were no OCT data regarding cup/disc volume and cup/disc height of IIH patients.
The limitation of our study is that patients were evaluated 2D in the spectral domain OCT device. This examination may lead to measurement errors in moderate or severe papilledema (Friedsen grade 3 or more), and significant thickening of the RNLF (mean RNFL > 200 µm) [6]. We think that the rate of error is low because the majority of our patient had mild papilledema.
Our results demonstrated that OCT can be a reliable alternative analysis in early-stage IIH patients, for whom papilledema is mild and may lead to a fundoscopy. Data on the parameters, such as the optic cup volume, optic disc and rim area, along with an increase in RNFL thickness, was determined by OCT, thereby contributing to the diagnosis of early-stage IIH.
References
De Simone R, Ranieri A, Montella S et al (2014) Revised diagnostic criteria for the pseudotumor cerebri syndrome in adults and children. Neurology 18(11):1011–1012
Fraser C, Plant GT (2011) The syndrome of pseudotumour cerebri and idiopathic intracranial hypertension. Curr Opin Neurol 24(1):12–17
Julayanont P, Karukote A, Ruthirago D, Panikkath D,et al. Idiopathic intracranial hypertension: ongoing clinical challenges and future prospects. J Pain Res. 2016;9:87–99
Friedman DI (2014) The pseudotumor cerebri syndrome. Neurol Clin 32(2):363–396
Thurtell MJ, Bruce BB, Newman NJ, et al. An update on idiopathic intracranial hypertension. Rev Neurol Dis. 2010;7(2–3):e56–e68
Chan JW (2017) Current concepts and strategies in the diagnosis and management of idiopathic intracranial hypertension in adults. J Neurol 264(8):1622–1633
Chen JJ, Thurtell MJ, Longmuir RA et al (2015) Causes and prognosis of visual acuity loss at the time of initial presentation in idiopathic intracranial hypertension. Invest Ophthalmol Vis Sci 56(6):3850–3859
Passi N, Degnan AJ, Levy LM (2013) MR imaging of papilledema and visual pathways: effects of increased intracranial pressure and pathophysiologic mechanisms. AJNR Am J Neuroradiol 34(5):919–924
Marzoli SB, Ciasca P, Curone M et al (2013) Quantitative analysis of optic nerve damage in idiopathic intracranial hypertension (IIH) at diagnosis. Neurol Sci 34(Suppl 1):S143–S145
Carta A, Favilla S, Prato M et al.Accuracy of funduscopy to identify true edema versus pseudoedema of the optic disc. Invest Ophthalmol Vis Sci. 2012;53(1):1–6
Mollan SP, Markey KA, Benzimra JD et al (2014) A practical approach to, diagnosis, assessment and management of idiopathicintracranial hypertension. Pract Neurol 14(6):380–390
Kardon R.Optical coherence tomography in papilledema: what am I missing? J Neuroophthalmol. 2014;34 Suppl:S10–S17
Heidary G, Rizzo JF III. Use of optical coherence tomography to evaluate papilledema and pseudopapilledema. Semin Ophthalmol. 2010;25(5–6):198–205
Rebolleda G, Diez-Alvarez L, Casado A et al. OCT: new perspectives in neuro-ophthalmology. Saudi J Ophthalmol. 2010;29(1):9–25
Langwińska-Wośko E, Litwin T, Dzieżyc K et al (2017) Optical coherence tomography as a marker of neurodegeneration in patients with Wilson’s disease. Acta Neurol Belg 117(4):867–871
Noval S, Contreras I, Muñoz S (2011) Optical coherence tomography in multiple sclerosis and neuromyelitis optica: an update. Mult Scler Int 2011:472790
Optical Coherence Tomography Substudy Committee; NORDIC Idiopathic Intracranial Hypertension Study Group. Auinger P, Durbin M, Feldon S et al. Papilledema outcomes from the optical coherence tomography substudy of the idiopathic intracranial hypertension treatment trial. Ophthalmology. 2015;122(9):1939.e2–1945.e2
Monteiro ML, Afonso CL (2014) Macular thickness measurements with frequency domain-OCT for quantification of axonal loss in chronic papilledema from pseudotumor cerebri syndrome. Eye (Lond) 28(4):390–398
Huang-Link YM, Al-Hawasi A, Oberwahrenbrock T et al (2015) OCT measurements of optic nerve head changes in idiopathic intracranial hypertension. Clin Neurol Neurosurg 130:122–127
Headache Classification Committee of the International Headache Society (IHS) (2013) The international classification of headache disorders, 3rd edition (beta version). Cephalalgia 33(9):629–808
Yohannan J, Wang J, Brown J et al (2017) Evidence-based criteria for assessment of visual field reliability. Ophthalmology 124(11):1612–1620
Heijl A, Patella VM, Bengstsson B (2012) The field analyzer primer: effective perimetry, 4th edn. Carl Zeiss Meditec, Dublin
Cameron JR, Albrecht P, Cruz-Herranz A et al. The APOSTEL recommendations for reporting quantitative optical coherence tomography studies. Neurology. 2016;87(18):1960
Skau M, Yri H, Sander B et al (2013) Diagnostic value of optical coherence tomography for intracranial pressure idiopathic intracranial hypertension. Graefes Arch Clin Exp Ophthalmol 251(2):567–574
Rebolleda G, Muñoz-Negrete FJ (2009) Follow-up of mild papilledema in idiopathic intracranial hypertension with optical coherence tomography. Invest Ophthalmol Vis Sci 50(11):5197–5200
Labib DM. Abdel Raouf DH (2015) Diagnostic value of optic coherans tomography in patients with idiopathic intracranial hypertension. Egypt J Neurol Psychiatry Neurosurg 52(4):249–253
Waisbourd M, Leibovitch I, Goldenberg D et al (2011) OCT assessment of morphological changes of the optic nerve head and macula inidiopathic intracranial hypertension. Clin Neurol Neurosurg 113(10):839–843
El-Dairi MA, Holgado S, O’Donnell T et al (2007) Optical coherence tomography as a tool for monitoring pediatric pseudotumor cerebri. J AAPOS 11(6):564–570
Kaufhold F, Kadas EM, Schmidt C et al (2012) Optic nerve head quantification in idiopathic intracranial hypertension by spectral domain OCT. PLoS One 7(5):e36965
OCT Sub-Study Committee for NORDIC Idiopathic Intracranial Hypertension Study Group, Auinger P, Durbin M, Feldon S, Garvin M et al (2014) Baseline OCT measurements in the idiopathic intracranial hypertension treatment trial, part II: correlations and relationship to clinical features. Invest Ophthalmol Vis Sci. 55(12):8173–8179
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
The study was carried out according to 1964 Helsinki Declaration and was approved by the Institutional Ethics Committee.
Informed consent
All patients participating in the study provided informed consent.
Rights and permissions
About this article

Cite this article
Eren, Y., Kabatas, N., Guven, H. et al. Evaluation of optic nerve head changes with optic coherence tomography in patients with idiopathic intracranial hypertension. Acta Neurol Belg 119, 351–357 (2019). https://doi.org/10.1007/s13760-018-1000-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13760-018-1000-2