
Abstract
Population-based studies report that children with epilepsy have relatively better prognosis than those with an onset at infancy, though studies about this period are limited. We aimed to evaluate the etiology in infant epilepsy less than 2 years of age and foreseeable risk factors for anti-epileptic drug resistance. We evaluated the patients who were presented to the division of pediatric neurology in our university hospital with seizures when they were between 1 and 24 months of age and diagnosed as epilepsy. Two hundred and twenty-nine patients (110 male and 119 female) who were diagnosed between the ages of 1–24 months were included in the study. The etiologies were structural (n = 55;24%), genetic (n = 29;12.7%), metabolic (n = 27;11.7%), and infectious (n = 8;3.5%), and it was unknown in 110 patients (48%). One-hundred and forty (61%) patients met the criteria for drug-resistant epilepsy (DRE). Multivariate logistic regression analysis showed that developmental delay at onset (OR 3.9, 95% CI 1.22, 12.47, p = 0.021), multifocal epileptiform discharges (OR 2.8, 95% CI 1.1, 7.44, p = 0.031), and history of status epilepticus (OR 32.9, 95% CI 3.8, 285.35, p = 0.001) were strong predictive factors for DRE. The epilepsy in children under 2 years of age is highly resistant to the anti-epileptic drugs, which could be related to the history of status epilepticus, developmental delay at onset, and multifocal epileptiform discharges.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Population-based studies report that children with epilepsy have relatively better prognosis than those with an onset at infancy, though studies about this period are limited. Though it has been reported that with proper and adequate treatment, remission is achieved in 60–70% of childhood epilepsy [1], and a group of patients is classified to have pharmacoresistant or intractable epilepsy. Severe epileptic encephalopathies like West and Dravet syndromes, neurometabolic disorders, and cortical dysplasia with resistant epilepsy occurring or becoming symptomatic at infancy result in severe neurodevelopmental delay and worse mortality rates [2, 3].
A widely debated topic is the definition of drug resistance (DR). In 2009, the International League Against Epilepsy (ILAE) suggested that when “a failure of adequate trials of two tolerated and appropriately chosen and used anti-epileptic drug (AED) schedules (whether as monotherapies or in combination) to achieve sustained seizure freedom” occurs, epilepsy should be defined as DR [4]. A lot of research has been done to develop a scoring system that questions risk factors for the purpose of better treatment and follow-up of DR patients. Determinant risk factors for DR are as follows: epileptic seizure onset under age of one, abnormal EEG findings and neurological deficit at the time of diagnosis, symptomatic seizures, high-frequency seizures, non-response to the first AED [4,5,6,7]. We aimed to evaluate the etiology in infant epilepsy less than 2 years of age and foreseeable risk factors for anti-epileptic drug resistance.
Methods
In this retrospective study, we evaluated the patients who presented to the division of pediatric neurology in our university hospital with seizures when they were between 1 and 24 months of age and diagnosed as epilepsy. We included patients with at least 2 years of follow-up period. The experienced pediatric neurologists examined the patients and planned their treatments.
Data for patients age at onset, perinatal risk factors (hypoxia, infection, and metabolic abnormalities requiring at least 5 days of hospitalization), family history, neurological examination at presentation and head circumference, EEG at presentation (epileptiform discharge and background slowing) and cranial MRI findings, history of status epilepticus, and every anti-epileptic drug used were retrieved retrospectively from patient records. The infantile period is arbitrarily defined from 4 weeks (end of neonatal period) to 2 years of life. Patients were divided into three groups as seizure onset in 1–6 months, > 6–12 months, and > 12–24 months of age.
A total of 64 patients whom we were unable to reach via phone and those with bad compliance to medications, incomplete clinic report, and missing follow-ups due to change of address were excluded from the study. Patients with neonatal seizures, febrile seizures, and one acute symptomatic seizure were also excluded from the study.
Drug-resistant epilepsy (DRE) is defined as failure of two or more anti-epileptic drugs (AEDs) with seizure frequency of more than one every 6 months in the year immediately before final follow-up [8]. Drug-responsive epilepsy (control group) is defined as 2 years of seizure control with one or two AEDs. An AED treatment was deemed unsuccessful if seizure control was not achieved with an adequate theuropathic dosage or side effects made the treatment unfeasible to continue. Blood levels of each drug (phenobarbital, valproic acid, carbamazepine, and phenytoin) were monitored in regular intervals.
For each patient, epilepsy classification was made using the new ILAE Commission on Classification and Terminology 2011–2013 Report. Descriptive semiologies from the medical records, EEG, and neuroimaging findings, and for some specific syndromes, age at onset were used to decide the seizure type(s) to be considered in the classification. For each case, epilepsy was classified based on the mode of onset at presentation (generalized, focal, infantile spasms, or unknown) and etiology (genetic, structural, metabolic, infection, or unknown).
For the etiology of the epilepsy, all patients were tested for their blood count, serum levels of glucose, electrolytes, liver, renal and thyroid function tests, and metabolic tests including tandem MS, blood and urine amino acid levels and organic acid profile, biotinidase activity, serum lactate, and very long chain fatty acids. Cranial MRI was also obtained from all the patients. In treatment-resistant patients’ lysosomal screening, CSF evaluation for glucose, lactate levels, and amino acid profiles was performed. For the genetic investigations, karyotype analyses, and array comparative genomic hybridization, epilepsy gen panel and whole exome/genome sequencing were studied if the parents could afford financial burden.
In the treatment of West and Dravet syndromes, we used the standard treatment protocols. However, in the study, the first choice anti-epileptic drug was defined as the agent, which was administered first after the onset of the seizures, in our hospital according to our standard protocol or in other hospitals, where the initial treatments were started according to their own protocols.
Statistical analyses
All statistical analyses were performed with SPSS for Windows version 21.0. Shapiro–Wilk tests and histogram graphics were used to assess normality. Categorical variables between groups were compared with χ 2 (Fisher exact test when the expected cell size was < 5). Normally, distributed continuous variables were compared by Student’s t test. Mann–Whitney U test was used for continuous variables, which are not normally distributed. All p values are based on two-tailed statistical analyses, and p < 0.05 was considered statistically significant. The significant predictors of drug-resistance epilepsy with p ≤ 0.05 in univariate analysis formed a logistic regression analysis model to identify independent risk factors associated with drug-resistance epilepsy occurrence.
Results
Patient population
Two hundred and twenty-nine patients (110 male and 119 female) who were diagnosed between the ages of 1–24 months were included in the study. The median age of patients was 58 months (33–140 months). Median month for the onset of seizure was 6 months (2–23 months). Mean follow-up duration was 57.2 months (25–130 months).
Seizure onset was most frequent between 1 and 6 months (n = 128, 56%) and 143 (62.4%) patients had generalized seizures, while 58 (25.3%) had focal and 25 (11%) had infantile spasm. Perinatal risk factors were present in 44 (19.2%) patients, and 56 (24.5%) had status epilepticus history. At the time of presentation with onset of seizure, 128 (56%) patients had a neurodevelopmental delay, 49 (21.4%) had microcephaly, and for 138 (60.3%) patients, neurological examination was abnormal. Evaluation of seizure etiology of the patients was based on history, physical examination, laboratory tests, imaging techniques, and metabolic screening tests. 55 (24%) patients’ etiology was structural, 29 (12.7%) genetic, 27 (11.7%) metabolic, 8 (3.5%) infectious, and for 110 (48%) of them, etiology was unknown. For those with unknown etiology, cranial MRI and metabolic testing were normal, and genetic testing was done for 32 of the 110. In DRE group with unknown etiology (n = 50), we obtained informed consents of the parents for the genetic tests for 32 patients. In addition, we could make array comparative genomic hybridization or epilepsy panel in only ten patients and whole exome/genome sequencing in two patients because of its financial burden on the families.
154 (67.2%) patients were started on phenobarbital, and 48 (21%) on valproic acid, 7 (3.1%) on levetiracetam, 9 (4%) on vigabatrin, 6 (2.6%) on carbamazepine, 3 (1.3%) on phenytoin, and 2 were on other medicines. In 77 (33.6%) patients, the seizures were controlled using only one anti-epileptic drug. In this study, our first choice was vigabatrin for nine patients and was ACTH for two patients with West syndrome. Unfortunately, 20 patients had been treated initially in other centers by different clinicians using phenobarbital, levetiracetam or valproic acid. In the study, only one out of 20 patients had been treated with other agents for 18 days. However, 19/20 patients had been referred to our hospital even if they started other agents, and we administered vigabatrin/ACTH in less than 1 week (range 2–6 days) after the onset of the seizures.
Drug-resistant epilepsy group
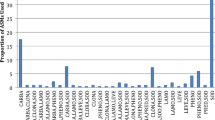
Based on the response to AED treatment, 140 (61%) patients met the criteria for DRE (Table 1). Seizure etiology for these patients was as follows: 21 (15%) genetic, 47 (33.6%) structural, 15 (10.7%) metabolic, 7 (5%) infectious, and 50 (35.7%) unknown. While for DRE patients, structural etiology was a significant risk factor (p < 0.001); the control group had a significantly higher number of patients with unknown etiology. Amongst the 47 patients with structural etiology, 21 had a brain injury in perinatal period, 19 had malformations of cortical development, 3 had vascular pathologies, and 4 had neurocutaneous syndrome. In the genetic etiology group, 11 patients were diagnosed with Dravet syndrome (SCN1A mutation), one had SCN2A mutation, two were diagnosed as Down syndrome, four had chromosome abnormality (duplication or deletion) and three patients had multiple congenital anomalies with normal chromosomes.
Ninety (64.3%) patients of the DRE group had an onset of seizure between 1 and 6 months (p = 0.005). Focal seizure (77.6%, p = 0.003) and infantile spasm (96%, p < 0.001) patients were significantly higher in DRE group than the control group. Other potential risk factors for DRE were perinatal risk factors (p = 0.002), developmental delay at onset (p < 0.001), microcephaly (at presentation) (p = 0.001), abnormal neurologic exam (p < 0.001), abnormal neuroimaging (p < 0.001), history of status epilepticus (p < 0.001), EEG pattern of epileptiform discharges, those with multifocal discharges (p = 0.008), hypsarrhythmia (p < 0.001), and both focal and generalized background slowing (p < 0.001).
All variables that had significance for DRE development in univariate analysis were used in our logistic regression model. Multivariate logistic regression analysis showed that developmental delay at onset (OR 3.9, 95% CI 1.22, 12.47, p = 0.021), multifocal epileptiform discharges (OR 2.8, 95% CI 1.1, 7.44, p = 0.031), and history of status epilepticus (OR 32.9, 95% CI 3.8, 285.35, p = 0.001) were strong predictive factors for DRE (Table 2).
Discussion
Two-thirds (61%) of our study population met the criteria for DRE. In similar studies, seizure onset age range was wider, and early onset of seizure was found to be a strong predictive factor for DRE [6, 7, 9,10,11]. In this study, onset of seizure was under the age of 2 years (neonatal seizures were excluded) and the mean of follow-up period was 57 months. Wirrell et al. studied risk factors for medical-resistance development in 127 epilepsy patients diagnosed under age of 36 months and a follow-up of 78 months showed that 35% of patients had DRE [14]. These rates being much higher than those in population-based studies could be the result of specific etiologies with resistant epileptic seizures occurring in infancy. Another reason for high percentage of DRE in the current study was that our institution is one of the reference hospitals for refractory epilepsy patients and neonates with high risks, in the country. In this study, children with cerebral anomalies had a significantly higher risk for DR and poor prognosis which was also shown in lots of other studies [6, 8, 12, 13]. Casetta et al. described perinatal brain injury as the leading cause for DR patients, while Othuska et al. found it to be CNS infection and perinatal hypoxic–ischemic injury [11]. This supports the poor prognosis of early childhood brain lesions on neurological functions. We consider that high percentage of DR patients in our series, in contrast to the literature, could be caused by the age of seizure onset, which was determined as the first 2 years of age.
Several studies have found infantile spasms and focal onset seizures as risk factors for resistant epilepsy [9, 14]. Similarly, in this study, infantile spasms (96%, p < 0.001) and focal onset seizures (77.6%, p = 0.003) were both significant risk factors for DR. In contrast, Berg et al. reported that 40% of children with focal epilepsy presented with delayed intractability (more than 3 years after onset of epilepsy) [15]. Patients’ age range being much higher than our study and focal epilepsies (rolandic epilepsy, occipital epilepsy) at school-age being of benign character may have resulted in this difference.
Few studies are done on assessment of EEG findings, based on drug response. Focal slowing being a strong predictive factor was shown by Berg et al. and Wirrell et al. [14, 15]. This study also showed that EEG pattern of focal slowing was a significant risk factor for DR. Consistent with a study done in a similar age group [14], this study found that multifocal epileptiform discharges on EEG were an independent risk factor using multivariate logistic regression.
History of status epilepticus is shown to have an association with DR in many studies [14,15,16], though there are a few studies in the literature showing otherwise. Our multivariate logistic regression model showed history of status epilepticus as the leading significant independent risk factor (n = 56). In some studies, etiology was found to be effective in prognosis after status epilepticus and this poor prognosis was strongly related to structural epilepsy. In this study, one-third of our status epilepticus patients had structural etiology, and another one-third was of unknown etiology. The unknown group may have had resistant epilepsies of neurometabolic or genetic etiology, which we could not diagnose with the available methods.
Neurodevelopmental delay at onset had a significant relation with DRE in previous studies [14,15,16]. This study, consistent with the literature, showed that neurodevelopmental delay at presentation might be an independent risk factor.
We had some limitations in this study and many of them were related to its retrospective design. First, because the time intervals between the onset of the seizures and onset of the treatments were not definitely noted in the files of about one-fourth of the patients, instead, they were written as approximate time, so we could not use this data in the study, which may have importance in the drug resistance and prognosis. Second, we could not give the data about cognitive prognosis, because range of ages of the patients in the study was wide and we could not make a standardized neuropsychological test. Further prospective studies in patients with similar ages are needed.
Conclusion
Two-thirds of our epileptic patients with onset of it under age of 2 years were DR. These patients should be closely monitored using the parameters found in our multivariate analysis (history of status epilepticus, developmental delay at onset, and EEG pattern of multifocal epileptiform discharges). Considering the negative neurocognitive effects of resistant seizures, these patients should be referred to non-medical treatment (epileptic surgery for seizures, ketogenic diet, and adequate physiotherapy) at the early stages and multidisciplinary approach should be provided.
References
Kwan P, Brodie MJ (2000) Early identification of refractory epilepsy. N Engl J Med 342:314–319
Camfield C, Camfield P (2008) Twenty years after childhood-onset symptomatic generalized epilepsy the social outcome is usually dependency or death: a population-based study. Dev Med Child Neurol 50:859–863
Berg AT, Smith SN, Frobish D, Beckerman B, Levy SR, Testa FM et al (2004) Longitudinal assessment of adaptive behavior in infants and young children with newly diagnosed epilepsy: influences of etiology, syndrome, and seizure control. Pediatrics 114:645–650
Kwan P, Arzimanoglou A, Berg AT, Brodie MJ, Allen Hauser W, Mathern G et al (2010) Definition of drug resistant epilepsy: consensus proposal by the ad hoc Task Force of the ILAE Commission on Therapeutic Strategies. Epilepsia 51:1069–1077
Shahar E, Genizi J (2008) Predictive factors of seizure control in childhood onset epilepsy. J Pediatr Neurosci 3:117–120
Sillanpää M, Schmidt D (2009) Early seizure frequency and aetiology predict long-term medical outcome in childhood-onset epilepsy. Brain 132:989–998
Camfield C, Camfield P, Gordon K, Smith B, Dooley J (1993) Outcome of childhood epilepsy: a population-based study with a simple predictive scoring system for those treated with medication. J Pediatr 122:861–868
Wirrell EC (2013) Predicting pharmacoresistance in pediatric epilepsy. Epilepsia 54 (s2):19–22
Kwong KL, Sung WY, Wong SN (2003) Early predictors of medical intractability in childhood epilepsy. Pediatr Neurol 29:46–52
Berg AT, Levy SR, Novotny EJ, Shinnar S (1996) Predictors of intractable epilepsy in childhood: a case-control study. Epilepsia 37:24–30
Ohtsuka Y, Yoshinaga H, Kobayshi K, Murakami N, Yamatogi Y, Oka E et al (2001) Predictors and underlying causes of medically intractable localization-related epilepsy in childhood. Pediatr Neurol 24:209–213
Casetta I, Granieri E, Monetti VC, Gilli G, Tola MR, Paolino E et al (1999) Early predictors of intractability in childhood epilepsy: a community-based case-control study in Copparo, Italy. Acta Neurol Scand 99:329–333
Chawla S, Aneja S, Kashyap R, Mallika V (2002) Etiology and clinical predictors of intractable epilepsy. Pediatr Neurol 27:186–191
Wirrell E (2012) Predictors and course of medically ıntractable epilepsy in young children presenting before 36 months of age: a retrospective, population-based study. Epilepsia 53:1563–1569
Berg AT, Vickrey BG, Testa FM, Levy SR, Shinnar S, DiMario F et al (2006) How long does it take for epilepsy to become intractable? A prospective investigation. Ann Neurol 60:73–79
Seker Yilmaz B, Okuyaz C, Komur M (2013) Predictors of intractable childhood epilepsy. Pediatr Neurol 48:52–55
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
The study was reviewed and approved by the Institutional Ethics Committee at Istanbul Faculty of Medicine. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Yildiz, E.P., Gunes, D., Bektas, G. et al. Predictive factors of drug-resistant epilepsy in children presenting under 2 years of age: experience of a tertiary center in Turkey. Acta Neurol Belg 118, 71–75 (2018). https://doi.org/10.1007/s13760-017-0850-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13760-017-0850-3