
Abstract
Understanding disease burden is necessary to optimally distribute resources, direct research efforts, and prioritize healthcare interventions. The Global Burden of Disease (GBD) Study was established in 1990 with the goal of providing accurate, transparent data for all diseases across the globe. In order to measure disease burden, this study employs disability-adjusted life years (DALYs), a metric which incorporates mortality and burden of living with a disease into a single unit. This open access database includes data from 2010 covering 291 conditions, 1160 sequelae, and 67 risk factors across 187 countries, allowing a comprehensive assessment of the world’s health as a whole and evaluation of potential regional differences in disease burden. Overall, GBD 2010 demonstrated that skin conditions rank fourth in terms of non-fatal disease burden. Additionally, 8 skin disorders rank in the top 50 most prevalent diseases worldwide. This resource highlights the importance of skin disease internationally and serves as an important resource for further refining our understanding the role of cutaneous disorders in across diverse societal, cultural, and environmental contexts.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Optimized allocation and delivery of healthcare resources require identification and evaluation of those diseases causing the greatest impact on patient health. Ongoing advances in disease prevention, diagnosis, and treatment have resulted in overall improved patient outcomes and survival across a spectrum of disorders in both developed and developing countries, and many diseases once considered fatal are now managed as chronic conditions. Accordingly, accurate assessments of disease burden must increasingly account for disease-related sequelae in addition to disease-specific mortality. This article briefly reviews the history of disease burden measures and describes in detail the recent development and implementation of the Global Burden of Disease Study, an ongoing project to provide comprehensive, high-fidelity information regarding disease-specific burden across the world.

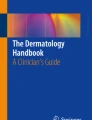
Square pie chart demonstrating global DALYs due to skin conditions in 2010. Red, blue, and green colors correspond to infective or parasitic skin disease, non-infective skin disease, and skin neoplasm, respectively. Color gradation demonstrates annual percent change of DALYs per 100,000 from 1990 to 2010

Square pie chart demonstrating US DALYs due to skin conditions in 2010. Red, blue, and green colors correspond to infective or parasitic skin disease, non-infective skin disease, and skin neoplasm, respectively. Color gradation demonstrates annual percent change of DALYs per 100,000 from 1990 to 2010
Background: Early Measure Development for Disease Burden
The need to measure burden of disease has led to the development of many tools, each with important limitations. Initial attempts to develop composite measures of fatal and non-fatal disease burden began in the 1960s with the creation of population-based indices that reflected the morbidity and mortality across entire populations [1, 2]. These measures provided a generalized assessment of population health as a whole, rather than attribution to particular conditions. This initial work led to the creation of the Gross National Health Product (GHNP) in 1979, which also combined population-level morbidity and mortality information, reported as disability-free years of life expected per 100,000 persons [2]. Data used to calculate GNHP were readily available from the United States (US) National Center for Health Statistics and included age-stratified total population, age-stratified total number of disability days for acute and chronic diseases, age-stratified total all-cause mortality, and age-stratified life expectancies [2]. The GNHP was designed to enable improved monitoring of aggregate health system performance, with the ultimate aim of informing healthcare policy and decision-making.
Similarly, in 1976, the quality-adjusted life years (QALY) metric was created to evaluate specific health outcomes within a single, unified unit [3]. The QALY uniquely incorporated patient ideas about quality of life in various health states. This novel metric was used primarily in economic studies examining the cost-effectiveness of health interventions to increase years of healthy life [3]. The calculation of QALY was performed using elaborate quality of life profiles that allowed for health status changes over time [3]. A major limitation of this metric was the implicit discrimination against the elderly and chronically ill. Nevertheless, the QALY set the stage for a transition in health metrics to include patient-centered opinions by implementing a quality of life profile into the statistical calculations [3].
Regardless of the measurement tool, the role of collecting and analyzing data on global disease prevalence and burden has historically fallen to the World Health Organization (WHO). This is largely due to the lack of another credible or willing organization [4] to assume this responsibility. For an organization with so many important functions in global health, including but not limited to coordinating global health efforts, disease advocacy, and promoting research efforts, the collection of prevalence data failed to be a major priority among these competing agendas [5]. In addition, WHO data is generally reported by United Nations member states. This is despite the fact that reported region disease prevalence is often not related to published regional data and occasionally reported data that could not reflect the actual disease burden. For instance, the WHO reported positive tuberculosis smear rates as greater than 100 % in Oman, Chile, Honduras, and Algeria in 2004. An alternative agency and more accurate measurement tool were needed to assume this responsibility [5].
Global Disease Burden 1990 Study
The 1990 Global Burden of Disease (GBD) Study was initiated at the request of the World Bank in collaboration with the World Health Organization (WHO) to provide information about non-fatal disease burden to create global epidemiologic disease assessments using a metric that would quantify disease burden for cost-effectiveness analysis and inform international health policy [6]. The 1990 iteration of GBD estimated disease burden for 107 causes of death, 483 sequelae of these conditions and 10 major risk factors, across 8 global regions and 14 age-sex groups [6]. Diseases were grouped into 3 broad categories for purposes of comparative evaluation: communicable/maternal/neonatal/nutritional disorders, non-communicable diseases, and injuries [9•].
The 1990 GBD Study introduced a new measure for disease burden—the disability-adjusted life year (DALY) [7]. The DALY, a modification of the QALY, is a comprehensive, unified metric for comparing disease burden associated with various disease states that can be used to prioritize healthcare resource distribution (particularly among underserved patient populations), serving as a common quantitative unit for both public health research and health program evaluation [7]. The DALY combines years of life lost (YLL) and years of life lived with disability (YLD) such that one DALY is synonymous to 1 year of healthy life lost [8]. YLL measures burden of disease caused by premature death before the average life expectancy, while YLD is the combination of years lived with sequelae of disease and a severity factor [8]. Combining the two metrics of morbidity and mortality, the DALY allows for a disease with short duration and severe disability comparable to a disease with longer duration but more mild disability. For diseases that are not fatal, particularly skin conditions, the DALY accounts for the significant impact on patients’ lives across decades. The severity scale also allows investigators to incorporate the human element and social preferences into the analysis of the impact of disease sequelae on individuals [7]. DALY calculation provides a standardized approach for assessing the health impact of a large number of diverse diseases and their outcomes [7].
In 1990, 90 % of global DALYs were concentrated in the developing world, largely sub-Saharan Africa and India, which correlated with only 10 % of total global healthcare spending [7]. The high-income Western Europe and the USA accounted for 7.2 % of disease burden but 87.3 % of health care spending, while the region including Eastern and Central Europe accounted for 4.5 % of disease burden and only 2.9 % of health care spending [7]. The majority (80 %) of DALYs in developed countries were caused by non-communicable diseases [7]. Childhood diseases accounted for 25 % of total disease burden in developing regions [7]. The two most important risk factors contributing to increased mortality in developing regions were pediatric malnutrition and poor water, sanitation, and hygiene [7]. Injuries accounted for approximately 10 % of global mortality, suggesting a potentially under-recognized cause of significant disease burden, while neuropsychiatric conditions contributed 22 % of disease burden in developed countries and 9 % in developing regions, with unipolar depression representing the fourth largest cause of disease-specific DALYs [6, 7]. Skin disorders collectively caused only 0.1 % of total disease burden in 1990, ranking 11 out of 14 categories of non-communicable diseases [7]. Finally, the GBD 1990 Study suggested that future trends and changes in global disease burden would be primarily driven by aging populations, peak and decline of the HIV epidemic, increases in tobacco-related disorders, and decreasing incidence of communicable and maternal/neonatal/nutritional diseases [6].
Global Burden of Disease 2010 Study
The landmark update of the GBD 2010 Study was the result of collaboration between hundreds of investigators evaluating 291 conditions, 1160 sequelae, and 67 risk factors across 187 countries over the two decades from 1990 to 2010 [9••]. Researchers revised calculations on 1990 data to enhance accuracy with new data sources [8]. Calculation of the DALY for GBD 2010 was also improved by basing the disease severity factor, also known as the disability weight, on population and Internet surveys rather than on individual health care professionals as had been done by GBD 1990 [9••].
Results from GBD 2010 show that disability now causes a much larger proportion of disease burden than premature mortality [9••]. Number of DALYs and overall prevalence rates have decreased for communicable and maternal/neonatal/nutritional disorders and increased for non-communicable disorders, with the largest DALY increase in diabetes [10]. This suggests that improvements in education, access to healthcare, preventative care measures, and increased income may positively impact burden from infectious conditions [10]. Despite this trend, GBD 2010 reported a disproportionate rise in HIV and malaria DALYs. Expected changes in the global age-structure correlate with the increased burden from non-communicable chronic disorders [7]. This also correlates with a greater proportion of total disease burden caused by disability than from premature death [7]. The large quantity of data collected and synthesized by GBD 2010 and now readily accessible allows continuing interpretation and further review of any subcategory or group of interest by outside investigators.
Global Burden of Disease 2010 Study and Dermatologic Disorders
The GBD 2010 Study included 15 categories of skin conditions [11•] (Figs. 1 and 2). Although individual skin disease categories were not associated with a significant disease burden, the combination of all skin diseases ranked eighteenth in DALY rate among all disorders [11•,12]. Moreover, analyzing only the morbidity component of diseases without mortality, the combination of all skin conditions ranked fourth in terms of YLD [11•]. Three skin condition categories were ranked in the top 10 most prevalent diseases worldwide: fungal diseases, acne vulgaris, and other skin conditions combined (an aggregate of 22 less common skin disorders). An additional 5 skin conditions were in the top 50, including pruritus, eczema, impetigo, scabies, and molluscum contagiousum [11•]. These results indicate a widespread burden caused by dermatologic conditions. Skin disorders demonstrated a bimodal distribution, with a peak during adolescence (related to the high prevalence of acne) and a second peak in the elderly (related to increases in skin cancers and other skin conditions) [11•].
Geographic variation in cutaneous disease burden was also observed. In the tropical areas of Oceania, sub-Saharan Africa, Southeast Asia, and tropical Central/South Americas, skin infections accounted for a much higher proportion of the overall disease burden compared to the global mean. Conversely, there was a lower proportion of the total disease burden related to skin infections in high-income regions of Asia. These variations highlight the combination of environmental and socioeconomic factors, including access to healthcare, which contribute to regional differences in disease burden [11•].
There are several major limitations to GDB 2010, including categorization methods of diseases, sequelae, and risk factors. GBD 2010 assigns each individual disease to a single category. For example, melanoma is included under “cancers” and is thus not included under “skin conditions” [11•]. Another source of error was the combination of eczema with other forms of dermatitis, collectively mislabeled as “eczema” [11•]. As a result of this classification error, the data suggests that eczema peaks at age 5, but remains a constant major cause of DALY disease burden related to eczema from age 20 to 80 [11•]. This is more likely the result of disease burden caused by other forms of dermatitis.
Although incorporating over 1000 categorized sequelae into the burden caused by each condition, the true magnitude of disease burden is likely underestimated. Sequelae of skin conditions are limited to itch and disfigurement only, discounting the emotional and financial burden that may be related to dermatologic conditions. For example, the arthritic and cardiovascular effects of psoriasis and the emotional impact of alopecia areata are not accounted for by the current GBD model. Finally, risk factors for skin disease are extremely narrow and particularly do not include UV exposure [9••]. These limitations are areas of potential improvement in future updates of the GBD.
Research Prioritization
Burden of disease measured by GBD 2010 has been used to investigate research prioritization [12, 13•]. In a comparison between skin condition DALYs and the number of systematic reviews and protocols published by the Cochrane Database of Systematic Reviews (CDSR), the number of reviews/protocols was well matched with DALYs for only 5 of the 15 skin conditions included in GBD [13•]. Dermatitis was both the largest source of skin disease burden and had the most CDSR review/protocol representation. Other conditions with disease burden were equally matched with the current research efforts were melanoma, non-melanoma skin cancer, viral skin diseases, and fungal skin diseases. Decubitus ulcers, psoriasis, and leprosy had higher rates of reviews/protocols compared to their relative disease burden [13•]. This may be related to the previously mentioned limitations in sequelae calculated by GBD. Acne, bacterial diseases, urticaria, pruritus, and scabies had proportionally fewer reviews/protocols when compared to their significant global disease burden. The pathology of these common conditions is generally understood, and there are many effective treatment options, possibly explaining the disparity between research efforts and a large disease burden. This approach is broadly applicable to other fields of medicine [14]. In addition, future investigations will allow investigation of priority-setting methods for various additional research databases.
Future
The GBD aims to release updated data on an annual basis. GBD 2013 was partially released in May 2014, and the remainder is scheduled for release in the fall of 2014, after which updates will be released annually [15••]. Frequent updates will allow policy makers and researchers to make informed decisions about allocation of resources including information about effectiveness of current policies. The GBD Study is also providing new insights to the field of dermatoepidemiology and has the potential to promote high-quality studies to better inform the burden of various skin diseases worldwide [16]. The GBD Study is a rich source of information with the potential to inform epidemiological assessments and, ultimately, improve global health.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Chiang CL. An index of health: mathematical models. Vital Health Stat. 1965;1(94):1–19.
Chen MK. The gross national health product: a proposed population health index. Public Health Rep. 1979;94(2):119–23.
Sassi F. Calculating QALYs, comparing QALY and DALY calculations. Health Policy Plan. 2006;21(5):402–8.
Murray CL, Lopez AD, editors. Summary: Global Burden of Disease—a comprehensive assessment of mortality and disability from diseases, injuries, and risk factors in 1990 and projected to 2020. Boston: Harvard School of Public Health; 1996.
Murray CJ, Lopez AD, Wibulpolprasert S. Monitoring global health: time for new solutions. BMJ. 2004;329(7474):1096–100.
Murray CJ, Lopez AD. Mortality by cause for eight regions of the world: Global Burden of Disease Study. Lancet. 1997;349(9061):1269–76.
Murray CJ, Lopez AD. Global mortality, disability, and the contribution of risk factors: Global Burden of Disease Study. Lancet. 1997;349(9063):1436–42.
Murray CJ. Quantifying the burden of disease: the technical basis for disability-adjusted life years. Bull World Health Organ. 1994;72(3):429–45.
Murray CJ, Vos T, Lozano R, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2197–223. Crucial landmark update of the original GBD study, which increased the number of conditions, sequelae, risk factors and countries included. This study also reanalyzed the original data from 1990 to allow more accurate comparison with new data.
Murray CJ, Lopez AD. Measuring the global burden of disease. N Engl J Med. 2013;369(5):448–57.
Hay RJ, Johns NE, Williams HC, Bolliger IW, Dellavalle RP, Margolis DJ, et al. The global burden of skin disease in 2010: an analysis of the prevalence and impact of skin conditions. J Invest Dermatol. 2014;134(6):1527–34. First study to look more critically and specifically at the dermatologic conditions included in the mass of GBD data.
Karimkhani C, Boyers LN, Margolis DJ, Naghavi M, Hay RJ, Williams HC, et al. Comparing cutaneous research funded by the national institute of arthritis and musculoskeletal and skin diseases with 2010 global burden of disease results. PLoS One. 2014;9(7):e102122.
Karimkhani C, Boyers LN, Prescott L, Welch V, Delamere FM, Nasser M, et al. Global burden of skin disease as reflected in Cochrane database of systematic reviews. JAMA Dermatol. 2014. doi:10.1001/jamadermatol.2014.709. Comparison of the burden of skin disease with the current research efforts using Cochrane reviews as a way to quantify research efforts. Allows comparison between what is causing people problems and what investigators are doing to fix these problems.
Boyers LN, Karimkhani C, Hilton J, Richheimer W, Dellavalle RP. Global burden of eye and vision disease as reflected in the Cochrane database of systematic reviews. JAMA Ophthalmol. 2014. doi:10.1001/jamaophthalmol.2014.3527.
About GBD. Institute for Health Metrics and Evaluation Web site. http://www.healthdata.org/gbd/about. Accessed July 14, 2014. Website contains open access to all GBD data and comparison of any subset of the data. This allows researchers or individuals access to their wealth of data to promote new interpretations of the data.
Karimkhani C, Boyers LN, Naghavi M, Coffeng LE, Lott JP, Wulf S, et al. The global burden of disease associated with alopecia areata. Br J Dermatol. 2014. doi:10.1111/bjd.13559.
Compliance with Ethics Guidelines
Conflict of Interest
K Goff, LN Boyers, C Karimkhani, JP Lott, and RP Dellavalle all declare no conflicts of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Author information
Authors and Affiliations
Corresponding author
Additional information
This article is part of the Topical Collection on Epidemiology
Rights and permissions
About this article

Cite this article
Goff, K., Boyers, L.N., Karimkhani, C. et al. Disease Burden Measures: a Review. Curr Derm Rep 4, 30–35 (2015). https://doi.org/10.1007/s13671-014-0094-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13671-014-0094-x