
Abstract
Purpose of Review
Emergency departments (EDs) are facing an epidemic of overcrowding and ED boarding, particularly of older adults who often present with, or develop, delirium in the ED. Delirium is associated with increased complications, longer hospital length of stay, mortality, and costs to the healthcare system. However, we only have limited knowledge of how to successfully prevent and treat delirium in the ED in a pragmatic, sustainable, and cost-effective way. We present a narrative review of recent literature of delirium prevention and treatment programs in the ED. We aim to describe the components of successful delirium management strategies to be used by EDs in building delirium management programs.
Recent Findings
We reviewed 10 studies (2005-2023) that report delirium interventions in the ED, and describe the different components of these interventions that have been studied. These interventions included: optimizing hemodynamics and oxygenation, treating pain, hydration and nutrition support, avoiding sedative hypnotics, antipsychotics and anticholinergics, promoting sleep, sensory stimulation, limiting the time spent in the ED, educating providers and staff, and developing multidisciplinary delirium protocols integrated into the electronic health record.
Summary
Through our narrative review of the recent literature on delirium prevention and treatment programs in the ED, we have identified nine components of successful delirium prevention strategies in the ED. We also discuss three high priority areas for further research including identification of most effective components of delirium prevention strategies, conduct of additional high-quality trials in non-hip
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Addressing the unique challenges of older adults admitted to the hospital as part of the Age-Friendly Health System is a pivotal and urgent challenge [1]. Older adults, particularly those with frailty, experience higher rates of poor hospital outcomes, including in-hospital complications such as delirium, functional decline, longer length of stay, discharge to locations other than home, higher health-care expenditures, and mortality [2,3,4,5,6]. Delirium, an acute alteration in attention and cognition, is a common complication for older adults, and is independently associated with increased rates of the aforementioned poor clinical outcomes [4, 7].
Delirium often manifests early in an older adult’s hospital journey, when it is evident in the Emergency Department (ED) [8]. The prevalence of delirium in the ED has been reported as high as 38%, and yet we have only limited knowledge of how to successfully prevent and treat delirium in the ED in a pragmatic, sustainable, and cost-effective way [8]. It is therefore essential to understand how to build programs to prevent and treat delirium in the ED, as the current epidemic of overcrowding—necessitating prolonged ED boarding—leads to increased delirium in the ED, as well as delays in care, increased medical errors, readmissions, mortality, and health-care cost [9,10,11,12,13,14].
The most recent review on delirium management in older adults in the ED, was published by Lee et al. in 2022; their systematic review focused on identifying strategies to prevent and treat delirium in the ED [15••]. They reported delirium management strategies ranging from addressing medications to multi-component interventions. Of the four peer-reviewed studies of delirium management interventions included in the systematic review, three showed reductions of delirium via melatonin or via multi-component, non-pharmacologic interventions [15••, 16,17,18]. In 2023, published delirium practice guidelines were reviewed by Filiatreault et al. who reported an absence of high-quality guidelines specifically addressing management of delirium in the ED. They also noted that very few guidelines included data from the ED [19•]. They concluded that most general guidelines recommended a multi-component intervention through a multi-disciplinary team, which could be applicable to the ED setting [19•].
Given the urgent need to better understand ways to prevent and treat delirium in the ED, we present an updated narrative review of recent literature for the development of delirium prevention and treatment programs in the ED. We aim to describe the components of successful delirium management strategies to be used by EDs in building delirium management programs.
Methods
We reviewed the very recent literature focused on the management of delirium for older adults in the ED, by covering the period starting immediately after the date of the search performed by Lee et al. and thereafter spanning 2 years and 1 month, i.e. we searched reports published between September 1, 2021, and October 16, 2023 [15••]. We used the same robust published MEDLINE search strategy that was used by Lee et al. [15••].
We included studies of any delirium prevention or treatment intervention initiated in the ED for older adults ≥ 65 years of age, as compared to either placebo, usual care, or pre-intervention time, that examined the intervention’s impact on delirium incidence, prevalence, severity, or duration. Exclusion criteria included abstracts, case reports, studies focused on delirium from substance use, and studies not published in English. Two authors performed title, abstract, and then full text review for inclusion and exclusion criteria. Disagreements were solved by adjudication between the two reviewers.
Our search strategy identified only 2 new original studies [20, 21]. Thus, we chose to evaluate any recent review studies meeting our search criteria published between September 1, 2021 and October 16, 2023 for additional original studies or meta-analyses meeting our criteria. We identified three recent reviews [22,23,24] that resulted in the inclusion of 4 additional studies [25,26,27,28••] meeting our criteria. Because these studies were identified by reviews, they span the years from 2011 to 2022. This resulted in a total of 6 studies. Due to the limited available research in this area and the goal of describing successful delirium management strategies to be used by EDs in building delirium management programs, we decided to also include in this review four original studies meeting our search criteria [16,17,18, 29] identified by Lee et al. [15••] spanning the years of 2005-2018.
This search strategy resulted in a total of 10 original studies or meta-analysis meeting our inclusion criteria for review (Table 1) [16,17,18, 20, 21, 25, 26, 27, 28••, 29].
Additional supporting information included in our present narrative review comes from recent literature and published guidelines on the prevention and treatment of delirium in other settings, that may be applicable to the ED setting.
Results
We reviewed 10 studies examining delirium management strategies in the ED (Table 1). Eight of these studies are considered entirely delirium prevention studies, only the two pharmacotherapy studies also assessed the ability of interventions (melatonin and haloperidol) to treat delirium; neither was a successful treatment. [16, 29] Six prevention studies significantly reduced delirium [16,17,18, 21, 25, 26] while three resulted in non-significant delirium reductions [20, 27, 28•]. One study resulted in a non-significant increase in delirium [29]. It is important to note that four of the six successful prevention strategies were multi-component interventions [17, 18, 21, 25]. We summarize the components separately in Table 2.
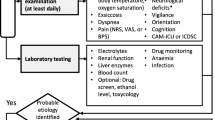
A visual mnemonic of ED delirium management strategies, “MENTATION”, is represented as a figure (Fig. 1). The following represent “MENTATION”: M Multidisciplinary processes, E Educate providers, N Nutrition and hydration, T Treat pain, A Avoid deliriogenic medications, T Time limit, I Investigate underlying cause, O Optimize hemodynamics and oxygenation, N Nurture sleep.

Mnemonic illustration of delirium prevention strategies or components of multi-component strategies for the prevention of delirium in the ED identified in this review
Optimizing Hemodynamics and Oxygenation
Two successful multi-component delirium prevention studies specific to older adults with hip fracture in ED, by Björkelund et al. and Larsson and Holgers, included optimization of hemodynamics and/or oxygenation as part of their delirium interventions [17, 25]. Both studies provided empiric supplemental oxygen [17, 25]. The oxygen protocol by Björkelund et al. targeted oxygenation saturation of ≥ 95% on room air [17]. Björkelund et al. also included protocols to avoid hypotension with a goal of maintaining a systolic blood pressure of ≥ 90–100 mmHg, transfuse at a more liberal hemoglobin cut off of 10g/dL, and maintain normothermia [17].
However, it is important to note that the protocol by Björkelund et al. did not examine possible adverse events related to liberal transfusion such as transfusion reaction or volume overload in older adults with cardiovascular disease. Thus, caution must be exercised when applying these delirium management strategies in the ED; patient specific comorbidities must be considered. Although these two studies were specific to hip fracture populations, and the particular protocols have limitations, facilitating optimal cerebral oxygenation is recommended as part of the management of delirium, and is included in intervention strategies used in other hospitalized settings [30, 31].
Treating Pain
Severe pain has been identified as a significant risk factor for delirium in the ED in a recent meta-analysis, suggesting that incorporating pain control will be beneficial [32••]. We identified five studies, one of which was a meta-analysis, that evaluated addressing pain as a strategy for managing delirium in the ED, all of which were studies in the hip fracture population [17, 25,26,27, 28•]. Two of these studies reported success in reducing incident delirium when there was a focus on addressing pain, either without a specific recommended medication, or recommending opioids and acetaminophen [17, 25]. The three other studies sought to assess whether a nerve block would be less deliriogenic than routine pain control; [26, 27, 28•] two studies showed less incident delirium using a nerve block for pain control than when using NSAIDs or placebo [23, 26, 27], whereas the third study, a meta-analysis by Kim et al., showed no significant difference between a nerve block for pain control and control (IV opioids, IV acetaminophen, or placebo) for pain control [28•]. The latter study did however note a significant decrease in the odds of incident delirium by 56% in a subgroup analysis of adults with underlying cognitive impairment [28•]. We identified no studies examining the treatment of pain in managing delirium for non-hip fracture diagnoses.
Thus, current literature suggests treating pain from hip fracture is an important component of delirium management in the ED, but there is little evidence to support a specific pain treatment approach in the ED for older adults at risk for delirium. In general, there is strong evidence that treatment of older adults should avoid medications such as meperidine, skeletal muscle relaxants, opioids, and the combination of any psychoactive medications with gabapentinoids [33]. However, we recognize that often some of these medications are needed for adequate pain control. A conservative approach favoring scheduled acetaminophen, lower doses of opioids, and minimizing co-administration with additional psychoactive medications like gabapentin and muscle relaxants may be a reasonable middle ground to help control severe pain while also reducing medication side effects.
Hydration and Nutritional Support
Dehydration and malnutrition are risk factors for delirium [30, 32••]. Two studies specific to older adults with hip fracture that were successful in reducing delirium in the ED included fluid resuscitation [17, 25]. One study also included enhanced nutrition support [17]. However, when considering hydration protocols in the general ED population, caution needs to be exercised in giving IV fluids empirically. Neither study assessed potential adverse events (e.g., congestive heart failure) that may occur if an older adult’s volume status is not carefully monitored during fluid administration. More conservative hydration protocols for older adults with laboratory evidence of dehydration have been successfully incorporated into delirium management programs on medicine floors [34]. Similarly, when considering nutrition protocols, the best approach for nutrition supplementation has not been identified. However, a recent review of malnutrition by Dent et al. suggests the management of malnutrition should focus on providing nutritional support through conservative and tailored multidisciplinary nutritional plans, focusing on education, oral supplementation, and mealtime assistance, if necessary [35].
Avoiding Sedative Hypnotics, Antipsychotics and Anticholinergics
Use of sedative hypnotics, antipsychotics, and anticholinergics increases the risk for developing delirium [30]. The successful delirium prevention intervention in the ED reported by Björkelund et al. included avoidance of these medications [17]. Only one study from our review, by Schrijver et al., analyzed the effect of using the antipsychotic, haloperidol, to prevent delirium in the ED which resulted in a non-significant increase in delirium (OR 1.43 [0.72, 2.78]) [29]. This outcome is not surprising, given several recent systematic reviews, including a large Cochrane review, showing that antipsychotics do not reduce the severity of, or resolve, inpatient delirium, with no difference between typical or atypical antipsychotics [36, 37]. In addition, antipsychotics carry significant risk in older adults, including an increased risk for mortality for adults with dementia [33]. Current guidelines suggest antipsychotics should be reserved for cases where the patient may be harmful to themselves or others, utilizing the lowest dose and shortest duration necessary [38]. To meet this recommendation, these medications should be ordered at time of need by the prescriber, and not ordered to be given as needed for agitation, as this can lead to overuse. Quetiapine 12.5 mg oral and Olanzapine 2.5 mg oral or intramuscular are examples of low dose antipsychotics. Once again, co-administering antipsychotics with other psychoactive medication such as diphenhydramine or benzodiazepines should be avoided [33].
Promoting Sleep
Disruption of the sleep wake cycle is commonly associated with delirium, and efforts to promote quality sleep have been recommended as part of the management of delirium [30]. One study which started in the ED, assessed the use of low dose nightly melatonin (0.5 mg) for the prevention of delirium, resulting in a significant decrease in incident delirium [16]. However, recent RCTs and meta-analyses from other hospitalized settings have shown mixed results when evaluating the efficacy of melatonin for the management of delirium [39, 40]. Thus, it is unclear who may benefit. In addition, other sleep medications such as sedative hypnotics increase the risk for delirium and other adverse effects in older adults [33]. However, non-pharmacologic approaches to enhancing sleep quality have been suggested for the multi-component management of delirium, including avoiding waking the patient overnight and noise reduction [7].
Sensory Stimulation
The ED is an overstimulating environment with loud background noise which can be particularly concerning for older adults at risk for delirium. One study piloted music and light therapy in the ED for adults at risk for delirium, yet did not find any significant change in the incidence of delirium in the treatment group verses control [20]. This finding is consistent with other studies outside of the ED environment, showing limited evidence for the efficacy of music or light for the management of delirium [7, 30]. However, we know that vision and hearing impairment are risk factors for delirium, and so it is generally recommended that adequate lighting should be provided, and older adults should have access to vision and hearing aids if necessary [7, 30].
Limiting Time Spent in the Emergency Department
Longer duration in the ED is associated with higher risk of developing delirium [32••]. Thus, two successful ED interventions included protocols to reduce the length of stay in the ED, with one bypassing the ED all together through a partnership with emergency medical services to begin triage in the field [17, 25].
It is hypothesized that a delay in diagnosis of the underlying precipitating condition leading to delirium occurs when older adults have an extended stay in the ED. Thus, it may be prudent to evaluate for underlying causes early in an older adult’s ED stay. A recent international panel of delirium experts described common diagnoses considered as possible underlying causes of delirium to evaluate as part of delirium management protocols [41••]. Although none of the protocols described in the management algorithms focus on delirium management in the ED, the information on assessing the precipitating cause of delirium is foundational to treating delirium in any setting.
Educating Providers and Staff
The successful multi-component ED delirium intervention by Naughton et al. included educating the multidisciplinary stakeholders involved in their program, including both physicians and nurses [18]. Delirium is often underrecognized, and a recent root cause analysis evaluating the reason why many adults are not screened for delirium in the ED, identified lack of delirium education as a key cause [42]. This is not surprising because delirium can present as hyperactive, hypoactive, or both. Unfortunately, hypoactive can be even more difficult to diagnose since it is often confused with drowsiness or depression, and yet hypoactive delirium carries a poorer prognosis than its hyperactive counterpart [30].
Multidisciplinary Protocols and Electronic Health Record Integration
All four of the successful multi-component delirium interventions in the ED that were identified by our review incorporated a multidisciplinary approach (Table 2) [17, 18, 21, 25]. Participating stakeholders included: emergency medical services, the ED, orthopedics, trauma, anesthesia, geriatrics, radiology, nursing, social work, case management, physical and occupational therapy, speech-language pathology, pain management, and volunteers [17, 18, 21, 25]. In addition, the successful intervention by Park et al. incorporated their protocol and algorithms into the electronic health record, including a delirium management order set which automatically triggered in the ED [21].
Discussion
We have summarized the evidence behind nine components, studied either alone or as part of multi-component interventions to manage delirium in the ED. These interventions were: optimizing hemodynamics and oxygenation, treating pain, hydration and nutrition support, avoiding sedative hypnotics, antipsychotics and anticholinergics, promoting sleep, sensory stimulation, limiting the time spent in the ED, educating providers and staff, and developing multidisciplinary delirium protocols integrated into the electronic health record.
It is important to recognize that there is limited evidence for many of the components that have been studied for delirium in the ED. These limitations can be considered in three categories: (1) The paucity of rigorous studies on the management of delirium in the ED. Of the 10 studies we included in our review, eight were entirely delirium prevention strategies [17, 18, 20, 21, 25,26,27, 28•]. The two studies assessing pharmacotherapy for delirium prevention and treatment (melatonin and haloperidol) did not show a benefit from medication verses placebo for the treatment of delirium, measured by either delirium severity or delirium duration [16, 29]. (2) Many studies are specific to a certain patient population, possibly limiting generalizability. Half of the studies were specific to geriatric hip fracture patients, which may limit generalizability [17, 25,26,27, 28•]. (3) It is difficult to determine efficacy of individual elements of interventions. The multi-component delirium interventions were studied as bundles, therefore we were not able to determine to what degree—if any—each individual component plays in reducing delirium risk [17, 18, 21, 25]. It is important to note that although the multi-component delirium interventions were implemented in different care settings, we chose to highlight only the components that were implemented in the ED.
We have identified three areas that should be a high priority for further research of delirium management in the ED: (1) identification of which components of multi-component interventions are most impactful, to guide formation of parsimonious delirium prevention protocols in the ED, (2) performance of additional high quality randomized trials and prospective cohort studies examining multi-component interventions for the management of delirium in the ED, particularly for non-hip fracture populations, and (3) identification and evaluation of delirium treatment strategies in the ED.
Despite the limited evidence, the nine components of interventions discussed here may be beneficial starting points when designing delirium prevention protocols in the ED. We have discussed the evidence supporting each component from the ED literature, as well as the relationship to the larger body of evidence for delirium management beyond the ED that may be applicable in the ED setting. This review should provide a fundamental framework for key stakeholders in the ED to begin developing successful multidisciplinary delirium management programs in the ED.
Conclusion
Emergency departments are facing an epidemic of overcrowding and ED boarding, particularly of older adults who often present with or develop delirium in the ED. This situation is of considerable consequence as delirium is associated with poor outcomes. However, delirium research in the ED is still in its early stages, and we have only limited knowledge of how to successfully prevent and treat delirium in the ED in a pragmatic, sustainable, and cost-effective way. Through our narrative review of the recent literature on delirium prevention and treatment programs in the ED, we have identified nine components of successful delirium prevention strategies in the ED and three high priority areas for further research including identification of most efficacious delirium prevention strategic components, performing additional high-quality trials in non-hip fracture populations, and identifying and evaluating delirium treatment strategies in the ED.
Data Availability
There were no primary data for this narrative review.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Institute for Healthcare Improvement. Age-Friendly Health Systems. [Internet]. [cited 2024 March 5]. Available from https://www.ihi.org/initiatives/age-friendly-health-systems.
Hoogendijk EO, Afilalo J, Ensrud KE, Kowal P, Onder G, Fried LP. Frailty: Implications for clinical practice and public health. Lancet. 2019;394(10206):1365–75. https://doi.org/10.1016/S0140-6736(19)31786-6.
Nidadavolu LS, Ehrlich AL, Sieber FE, Oh ES. Preoperative evaluation of the frail patient. Anesth Analg. 2020;130(6):1493–503. https://doi.org/10.1213/ANE.0000000000004735.
Sieber F, Gearhart S, Bettick D, Wang N. Edmonton frailty scale score predicts postoperative delirium: A retrospective cohort analysis. BMC Geriatr. 2022;22(1):585–8. https://doi.org/10.1186/s12877-022-03252-8.
Muscedere J, Waters B, Varambally A, et al. The impact of frailty on intensive care unit outcomes: A systematic review and meta-analysis. Intensive Care Med. 2017;43(8):1105–22. https://doi.org/10.1007/s00134-017-4867-0.
Imam T, Konstant-Hambling R, Fluck R, Hall N, Palmer J, Conroy S. The hospital frailty risk score-outcomes in specialised services. Age Ageing. 2021;50(2):511–8. https://doi.org/10.1093/ageing/afaa156.
Oh ES, Fong TG, Hshieh TT, Inouye SK. Delirium in older persons: Advances in diagnosis and treatment. JAMA. 2017;318(12):1161–74. https://doi.org/10.1001/jama.2017.12067.
Carpenter CR, Hammouda N, Linton EA, et al. Delirium prevention, detection, and treatment in emergency medicine settings: A geriatric emergency care applied research (GEAR) network scoping review and consensus statement. Acad Emerg Med. 2021;28(1):19–35. https://doi.org/10.1111/acem.14166.
Kenny JF, Chang BC, Hemmert KC. Factors affecting emergency department crowding. Emerg Med Clin North Am. 2020;38(3):573–87. https://doi.org/10.1016/j.emc.2020.04.001.
Kelen GD, Wolfe R, Gail D’Onofrio, et al. Emergency department crowding: The canary in the health care system. Catalyst non-issue content. 2021;2(5). https://doi.org/10.1056/CAT.21.0217.
Ma IC, Chen KC, Chen WT, et al. Increased readmission risk and healthcare cost for delirium patients without immediate hospitalization in the emergency department. Clin Psychopharmacol Neurosci. 2018;16(4):398–406. https://doi.org/10.9758/cpn.2018.16.4.398.
Elder NM, Mumma BE, Maeda MY, Tancredi DJ, Tyler KR. Emergency department length of stay is associated with delirium in older adults. West J Emerg Med. 2023;24(3):532–7. https://doi.org/10.5811/westjem.59383.
Moura Junior V, Westover MB, Li F, et al. Hospital complications among older adults: Better processes could reduce the risk of delirium. Health Serv Manage Res. 2022;35(3):154–63. https://doi.org/10.1177/09514848211028707.
Ehrlich A, Erickson M, Oh E, James T, Saxena S. Prioritizing care of older adults in times of emergency department overcrowding. JGEM. 2023;4(3):1–6. https://institutionalrepository.aah.org/cgi/viewcontent.cgi?article=1067&context=jgem. https://doi.org/10.17294/2694-4715.1067.
•• Lee S, Chen H, Hibino S, et al. Can we improve delirium prevention and treatment in the emergency department? A systematic review. J Am Geriatr Soc. 2022;70(6):1838–49. https://doi.org/10.1111/jgs.17740. Initial systematic review of delirium management in the emergency department.
Al-Aama T, Brymer C, Gutmanis I, Woolmore-Goodwin SM, Esbaugh J, Dasgupta M. Melatonin decreases delirium in elderly patients: A randomized, placebo-controlled trial. Int J Geriatr Psychiatry. 2011;26(7):687–94. https://doi.org/10.1002/gps.2582.
Bjorkelund KB, Hommel A, Thorngren K, Gustafson L, Larsson S, Lundberg D. Reducing delirium in elderly patients with hip fracture: A multi-factorial intervention study. Acta Anaesthesiol Scand. 2010;54(6):678–88. https://doi.org/10.1111/j.1399-6576.2010.02232.x.
Naughton BJ, Saltzman S, Ramadan F, Chadha N, Priore R, Mylotte JM. A multifactorial intervention to reduce prevalence of delirium and shorten hospital length of stay. J Am Geriatr Soc. 2005;53(1):18–23. https://doi.org/10.1111/j.1532-5415.2005.53005.x.
• Filiatreault S, Grimshaw JM, Kreindler SA, et al. A critical appraisal and recommendation synthesis of delirium clinical practice guidelines relevant to the care of older adults in the emergency department: An umbrella review. J Eval Clin Pract. 2023;29(6):1039–53. https://doi.org/10.1111/jep.13883. Outlines and discusses current delirium clinical practice guidelines that may be relevant to the emergency department setting.
Keene S, Balasundaram A, Cameron-Comasco L, Otero R. Feasibility of light and music therapy in the elderly for the prevention of hospital-associated delirium. R I Med J (2013). 2023;106(4):35–9.
Park C, Bharija A, Mesias M, et al. Association between implementation of a geriatric trauma clinical pathway and changes in rates of delirium in older adults with traumatic injury. JAMA Surg. 2022;157(8):676–83. https://doi.org/10.1001/jamasurg.2022.1556.
Maher S, Moore Z, Avsar P, Patton D. What is the impact of a fast-track pathway on length of stay for adult patients with a hip fracture? A systematic review. Arch Orthop Trauma Surg. 2022;142(12):3803–16. https://doi.org/10.1007/s00402-021-04248-6.
Makkar JK, Singh NP, Bhatia N, Samra T, Singh PM. Fascia iliaca block for hip fractures in the emergency department: Meta-analysis with trial sequential analysis. Am J Emerg Med. 2021;50:654–60. https://doi.org/10.1016/j.ajem.2021.09.038.
Simic A, Nesek Adam V, Rosic D, et al. Peripheral nerve blocks for hip fractures in emergency medicine. Acta Clin Croat. 2022;61(Suppl 1):78–83. https://doi.org/10.20471/acc.2022.61.s1.13.
Larsson G, Holgers K. Fast-track care for patients with suspected hip fracture. Injury. 2011;42(11):1257–61. https://doi.org/10.1016/j.injury.2011.01.001.
Hao J, Dong B, Zhang J, Luo Z. Pre-emptive analgesia with continuous fascia iliaca compartment block reduces postoperative delirium in elderly patients with hip fracture. A randomized controlled trial. Saudi Med J. 2019;40(9):901–6. https://doi.org/10.15537/smj.2019.9.24483.
Monzon D, Iserson K, Vasquez J. Single fascia iliaca compartment block for post-hip fracture pain relief. J Emerg Med. 2007;32(3):257–62.
• Kim C, Yang JY, Min CH, Shon H, Kim JW, Lim EJ. The effect of regional nerve block on perioperative delirium in hip fracture surgery for the elderly: A systematic review and meta-analysis of randomized controlled trials. Orthop Traumatol Surg Res. 2022;108(1):103151. https://doi.org/10.1016/j.otsr.2021.103151. Meta-analysis of delirium incidence following regional nerve blocks for hip fracture pain.
Schrijver EJM, de Vries OJ, van de Ven PM, et al. Haloperidol versus placebo for delirium prevention in acutely hospitalised older at-risk patients: A multi-centre double-blind randomised controlled clinical trial. Age Ageing. 2018;47(1):48–55. https://doi.org/10.1093/ageing/afx124.
Hshieh TT, Inouye SK, Oh ES. Delirium in the elderly. Psychiatr Clin North Am. 2018;41(1):1–17. https://doi.org/10.1016/j.psc.2017.10.001.
Burton JK, Craig L, Yong SQ, et al. Non-pharmacological interventions for preventing delirium in hospitalised non-ICU patients. Cochrane Database Syst Rev. 2021;11(11):CD013307. https://doi.org/10.1002/14651858.CD013307.pub3.
•• Oliveira JE, Silva L, Berning MJ, Stanich JA, et al. Risk factors for delirium in older adults in the emergency department: A systematic review and meta-analysis. Ann Emerg Med. 2021;78(4):549–65. https://doi.org/10.1016/j.annemergmed.2021.03.005. Outlines risk factors for incident delirium in the emergency department which may benefit from targeted interventions.
American Geriatrics Society Beers Criteria(R) Update Expert Panel. American geriatrics society 2023 updated AGS beers criteria(R) for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2023;71(7):2052–81.
Inouye SK, Bogardus STJ, Charpentier PA, et al. A multicomponent intervention to prevent delirium in hospitalized older patients. N Engl J Med. 1999;340(9):669–76. https://doi.org/10.1056/NEJM199903043400901.
Dent E, Wright ORL, Woo J, Hoogendijk EO. Malnutrition in older adults. Lancet. 2023;401(10380):951–66. https://doi.org/10.1016/S0140-6736(22)02612-5.
Burry L, Mehta S, Perreault MM, et al. Antipsychotics for treatment of delirium in hospitalised non-ICU patients. Cochrane Database Syst Rev. 2018;6(6):CD005594. https://doi.org/10.1002/14651858.CD005594.pub3.
Nikooie R, Neufeld KJ, Oh ES, et al. Antipsychotics for treating delirium in hospitalized adults: A systematic review. Ann Intern Med. 2019;171(7):485–95. https://doi.org/10.7326/M19-1860.
American Geriatrics Society Expert panel on postoperative delirium in older adults. American geriatrics society abstracted clinical practice guideline for postoperative delirium in older adults. J Am Geriatr Soc. 2015;63(1):142–50. https://doi.org/10.1111/jgs.13281.
Oh ES, Leoutsakos J, Rosenberg PB, et al. Effects of ramelteon on the prevention of postoperative delirium in older patients undergoing orthopedic surgery: The RECOVER randomized controlled trial. Am J Geriatr Psychiatry. 2021;29(1):90–100. https://doi.org/10.1016/j.jagp.2020.05.006.
Khaing K, Nair BR. Melatonin for delirium prevention in hospitalized patients: A systematic review and meta-analysis. J Psychiatr Res. 2021;133:181–90. https://doi.org/10.1016/j.jpsychires.2020.12.020.
•• Ottens T, Hermes C, Page V, et al. The delphi delirium management algorithms. A practical tool for clinicians, the result of a modified delphi expert consensus approach. Delirium. 2024. https://deliriumjournal.com/article/90652-the-delphi-delirium-management-algorithms-a-practical-tool-for-clinicians-the-result-of-a-modified-delphi-expert-consensus-approach. https://doi.org/10.56392/001c.90652. Discusses expert consensus for how to manage delirium including useful mnemonics for diagnosing the underlying cause of delirium.
Martin L, Lyons M, Patton A, et al. Implementing delirium screening in the emergency department: A quality improvement project. BMJ Open Qual. 2022;11(2):e001676. https://doi.org/10.1136/bmjoq-2021-001676.
Acknowledgements
We would like to acknowledge and thank Dr. Sarah Poynton for her thoughtful edits of this work. We would also like to thank and acknowledge Jennifer Fairman for her outstanding assistance with creating our mnemonic illustration. We would also like to thank and acknowledge our sources of support including NIH/NIA grant number T32AG066576 [AE] and grant numbers R01AG076525, R01AG057667, R01AG057725, P30AG021334, P30AG073104 [EO], the Richman Family Precision Medicine Center of Excellence in AD [EO], and the Sarah Miller Coulson Human Aging Program [EO].
Funding
April Ehrlich is supported by NIH/NIA [grant number T32AG066576]. Esther Oh is supported by NIH/NIA [grant numbers R01AG076525, R01AG057667, R01AG057725, P30AG021334, P30AG073104], the Richman Family Precision Medicine Center of Excellence in Alzheimer’s Disease, and Sarah Miller Coulson Human Aging Program Scholar.
Author information
Authors and Affiliations
Contributions
AE reviewed literature, wrote the main manuscript, created the mnemonic, participated in draft reviews, approved the final version, and agrees to be accountable for all aspects of work. ' EO reviewed literature, made substantial contributions to the conception or design of the work, participated in draft reviews, approved the final version, and agrees to be accountable for all aspects of work. SA reviewed literature, made substantial contributions to the conception or design of the work, participated in draft reviews, approved the final version, and agrees to be accountable for all aspects of work.
Corresponding author
Ethics declarations
Conflict Interests
The authors declare that they have no competing interests.
Human and Animal Right and Informed Concent
All reported studies/experiments with human or animal subjects performed by the authors have been previously published, and complied with all applicable ethical standards (including the Helsinki declaration and its amendments, institutional/national research committee standards, and international/national/institutional guidelines).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Ehrlich, A., Oh, E. & Ahmed, S. Managing Delirium in the Emergency Department: An Updated Narrative Review. Curr Geri Rep 13, 52–60 (2024). https://doi.org/10.1007/s13670-024-00413-y
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13670-024-00413-y