
Abstract
Information is needed on implementation processes involved in translating evidence-based interventions (EBIs) into health disparity communities. In an RCT, Nuevo Amanecer, a cognitive-behavioral stress management (CBSM) program delivered by breast cancer survivors (compañeras) in community settings to Spanish-speaking Latina breast cancer survivors, was effective in improving quality of life and decreasing breast cancer concerns and depressive and bodily symptoms. Using mixed methods, we evaluated the processes of implementing Nuevo Amanecer. Program delivery was assessed by direct observation. Treatment receipt was assessed by participants’ mastery and homework completion. Perceived benefits, quality, ease of use, usefulness of components, and suggested improvements were evaluated through participant surveys and semi-structured interviews of participants and compañeras. Eighty percent of women completed six or more of eight sessions. Observer ratings of program delivery indicated compañeras demonstrated fidelity 80–90% of the time for three components (e.g., following the manual), but only 10% for two components (e.g., modeling skills). Regarding treatment receipt, most participants completed all homework. Knowledge and skills mastery was high (mostly >85%). In program evaluations, 93% indicated the program helped them cope with breast cancer “quite a bit/extremely.” Participants reported improved self-management skills and knowledge. Suggested improvements were to add more sessions to practice cognitive-behavioral coping skills and simplify exercises and homework. We conclude that CBSM programs can be delivered in community settings by trained peers with high fidelity, acceptability, and perceived usefulness. Results provided some areas where the program could be improved. Our rigorous evaluation illustrates methods for evaluating processes of translating EBIs for community implementation. Trial registration: NCT01383174 (ClinicalTrials.gov).
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Latina women with breast cancer, especially limited English-proficient (LEP) Latinas, suffer disproportionately higher rates of cancer-related psychosocial morbidity and poorer quality of life than non-Latina white women [1]. The causes are multi-factorial, including limited English fluency, limited health insurance, poverty, immigration stress, poorer understanding of their diagnosis and treatment, and being less likely to participate in treatment decision-making [2–4].
Cognitive-behavioral therapeutic approaches are recommended as part of the National Comprehensive Cancer Network guidelines for the relief of psychosocial distress and fatigue associated with breast cancer and its treatment [5]. Cognitive-behavioral stress management (CBSM) programs provide instruction on mental and behavioral techniques to manage stress and mood and have improved breast cancer patients’ self-efficacy, perceptions of social support, adaptive coping strategies [6], stress and depressive symptoms, treatment side effects, and quality of life [7–9]. Typically, CBSM programs for cancer patients have been offered in cancer centers by mental health professionals, which limits their practicality due to shortages of trained psycho-oncologists. Furthermore, these interventions have not been adapted and tested for cancer patients from diverse ethnic backgrounds, including Latinas. Translation of evidence-based CBSM programs to be appropriate for ethnically diverse groups could help address disparities in cancer-related psychosocial morbidity and quality of life experienced by Latinas and other minority groups.
Translation into diverse populations requires cultural adaptations to improve the fit of the intervention to the new population and usually involves tradeoffs between fit and fidelity [10]. Studying implementation processes when translating interventions can provide valuable information about the core elements of an evidence-based intervention (EBI) that were perceived as most effective, useful, and acceptable. Process evaluation of community-based interventions can identify delivery methods and content that were suboptimal [11] as well as offer valuable insights into why interventions may have been effective and how to improve the program [12, 13]. Process evaluations can also identify problems with implementation that can be addressed prior to broad translation into practice [14].
To develop Nuevo Amanecer, we applied an innovative translational processes model appropriate for minority and underserved populations [10]. The translational process involved integrating an evidence-based intervention, a community “best-practices” program, and our own formative research results. The resulting intervention is a culturally tailored, 8-week CBSM program delivered by trained breast cancer survivors (compañeras) in community settings. In the RCT among Spanish-speaking Latinas with breast cancer, it was found to improve several quality of life domains and decrease breast cancer concerns and depressive and bodily symptoms [15]. Because such translational methods to reach minority populations in community settings, as well as the use of compañeras for program delivery of CBSM interventions, are relatively new, it is important to understand the processes by which it was implemented from the perspective of participants, the compañeras who delivered it, and the community in which it was embedded. This paper reports on a mixed-method evaluation of the implementation of the Nuevo Amanecer program that included observer ratings of program fidelity, participants’ perceived usefulness and ease of use of the program, and participants’ satisfaction with the program, and suggestions for improvement.
Methods
Design
The Nuevo Amanecer program and RCT design are described in detail elsewhere [16]. The program is an individualized Spanish-language 8-week intervention that teaches women cognitive-behavioral coping skills to manage stress and emotions and includes emotional support, informational resources, training in cognitive and behavioral stress management techniques, and modeling. The program is delivered by compañeras (breast cancer survivors trained to deliver the program) who met weekly with participants in their homes. Using structured interventionist and participant manuals, the compañera delivered the following eight modules: Week 1—Managing the initial impact of cancer; Week 2—Finding the cancer information you need; Week 3—Getting the support you need; Week 4—Thoughts and mood, part I; Week 5—Thoughts and mood, part II; Week 6—Stress management; Week 7—Setting goals, part I; and Week 8—Setting goals, part II. Each weekly session was structured to begin with a deep breathing exercise, review of the prior session to reinforce key concepts, review of new week material, hands-on exercises, modeling by the compañera of the skills, role playing, and ending with a recap of the new material covered that session. Key skills/concepts taught included relaxation techniques (e.g., recognizing and managing stress, deep breathing, guided imagery, planning joyful activities), information seeking (communicating with health care professionals and calling the National Cancer Institute Cancer Information Service), communicating with family members and friends about cancer and how to ask for help, cognitive reframing (identification of unhelpful thoughts and techniques for converting them into helpful thoughts), and goal setting for practicing the skills. In the original RCT, 151 women were randomized, 76 to the immediate intervention group and 75 to the wait-list control group who were offered the program after 6 months, henceforth referred to as the intervention and control groups.
Using mixed methods, treatment delivery (extent to which the treatment was delivered as intended) was assessed by direct observation of a sample of intervention sessions. Treatment receipt was assessed by attendance and how well participants learned and understood the intervention components, both reported on tracking forms completed by compañeras. Perceived benefits, quality, ease of use, usefulness of program components, and suggestions for improvements were assessed by participant evaluation surveys and semi-structured interviews of compañeras and participants.
Human Subjects
Written informed consent was obtained from all participants. The University of California San Francisco and the San Mateo Medical Center institutional review boards approved the protocol. The study was performed in accordance with the ethical standards of the 1964 Declaration of Helsinki and its later amendments.
Sample
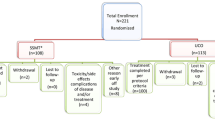
The sample for this study included women who completed the program, defined as having completed at least six of the eight sessions, from either the intervention or control group. Demographic variables consisted of age, educational attainment, health insurance, employment status, financial hardship (problems paying for their monthly expenses in the past month), country of origin, marital status, self-rated health, and any ongoing chronic conditions. The study population for the original study consisted of primarily Spanish-speaking Latinas diagnosed with non-metastatic breast cancer in the previous year living in the 5-county Northern California area targeted by the study. Recruitment was performed in-person by trained bilingual-bicultural recruiters (patient navigators, promotoras, or medical assistants) employed by community-based organizations or clinical partners on the project, occurring mostly in the clinics/hospitals where patients were seen. Recruiters worked closely with health care staff at the clinical sites to identify potentially eligible patients. They offered the program to 195 women meeting eligibility criteria; 151 women were randomized (77%) while 22 were ineligible and 22 refused. Of those randomized, all but one were immigrants, and the majority were of Mexican origin (68%) and had less than a 6th grade level education (66%).
Measures and Analyses
Compañera (Interventionist) Tracking Form
Compañeras completed a structured program tracking form after each of the eight sessions. Data included logistics (session date, location, duration, and round trip travel time and mileage), whether the participant had completed the homework for that week (yes or no), whether the participant reported difficulty in doing the homework (yes or no), and if so, the type of difficulty (open-ended). For sessions 2–8, the compañera assessed whether the participant was able to demonstrate the skill covered in the prior session (yes or no). For sessions 2–4, a few questions assessed knowledge of material presented in the prior session (correct or incorrect).
For program logistics and homework completion data, we calculated descriptive statistics. Qualitative thematic analysis was performed independently by the scientific co-principal investigator (co-PI) and project director on open-ended reports of problems doing homework. For skills demonstration and knowledge, we report the number and percent that successfully demonstrated the skill or answered correctly. We compared skills mastery between the intervention and control groups.
The tracking form also asked women who dropped out at any point their reason for doing so. This information was collected for women in the intervention group and those in the control group who elected to receive the program after the wait period.
Fidelity Ratings
Two intervention sessions for each of the five compañeras (ten total sessions) were selected for observation based on convenience. The observer was the community co-PI, a bilingual-bicultural clinical psychologist with extensive experience providing cancer support services to Latinos. Using structured rating scales (1 = not at all, 2 = a fair amount, 3 = a great deal, 4 = constantly), this observer rated interventionist’s compliance with six program components: the extent to which they followed the manual for that session, explained concepts in language the participant understood, checked that the participant understood the material, spoke in a caring/supportive way, modeled the skills, and provided feedback to participants for efforts to practice the skills. Seven additional questions rated the extent to which the counselor encouraged participants to practice seven skills taught (cognitive reframing, good communication, seeking cancer information, practicing stress management, asking for help, increasing helpful activities, and goal setting). Sessions were audiotaped and reviewed independently by two people (co-PI and a trained health education intern). For each fidelity dimension, we report the proportion of the ten sessions that were rated within each response option.
Program Evaluation Survey
Participants were contacted by telephone within a few weeks of completing the program for a 5-min interview about the program. A bilingual-bicultural research associate conducted the interviews and women received $10 in cash. Regarding the program format, we asked them about the timing (how soon after diagnosis would they have liked to have started: sooner/about the same time/later), length (fewer/about the same/more sessions), and delivery format (meetings with compañera/by telephone with compañera/alone using a workbook). Women rated the overall quality of the program, the workbook (written materials), and the compañera’s skills using a 5-level response set of poor/fair/good/very good/excellent. Perceived usefulness was assessed by asking women to rate how much the program helped them cope with their breast cancer (response options were not at all/a little bit/moderately/quite a bit/extremely). They rated the overall usefulness of the workbook and of specific sections on cancer information, communicating with family members, communicating with doctors, managing thoughts and mood, managing stress, and setting goals (not at all/slightly useful/fairly useful/very useful). Ease of use was assessed with three items asking how easy it was to understand the workbook (response options of not at all/slightly easy/fairly easy/very easy), how convenient the program was (not at all/slightly convenient/fairly convenient/very convenient), and how often they continued to practice the skills learned (never/rarely/sometime/often).
We conducted item-level analyses, dichotomizing each item (the lowest three response choices vs. the highest two response choices, e.g., poor/fair/good versus very good/excellent). We tested for differences between the intervention and control groups using chi-square. We performed content analysis of an open-ended question that asked about suggestions for improvement of the program.
Debriefing by Semi-Structured Interviews
We conducted individual semi-structured interviews to debrief compañeras and participants after the randomized trial portion of the study ended. We attempted to interview all five compañeras, but were only able to interview two after the RCT ended, due to their work obligations or travel. We selected ten program participants at random from the intervention arm prior to the start of recruitment and interviewed all of them at the end of the program. Interviews were conducted by a trained bilingual-bicultural interviewer (medical student) who was not directly involved with the main RCT study. An open-ended interview guide was used to query respondents on benefits of the program, suggestions for improvements, cultural factors influencing program participation, and program delivery/attendance challenges. Compañeras were asked also about the manual, program efficacy, acceptability, and training.
Interviews were conducted, audiotaped, and transcribed in Spanish. Two experienced bilingual-bicultural researchers performed content analysis of the transcripts and discussed coding themes with the research team until consensus was reached. Main themes were categorized into subthemes and paired with illustrative quotes. Quotes were translated into English for reporting purposes.
Results
Sample
Of 76 women randomized to the intervention group, 63 completed at least six sessions. Of 74 randomized to the control group, 24 women elected to begin the program, and 17 completed at least six sessions. Thus, a total of 80 women completed the program and are included in these analyses. Time from diagnosis to initiation of the Nuevo Amanecer program was on average 102.6 days (SD 87.7 days) for the intervention group (N = 63) and on average, 326.1 days (SD 85.1 days) for the control group (N = 17). There were no significant differences between the intervention and control groups on sociodemographic variables. The mean age of these 80 women was 49 (SD = 11). Most were born in Mexico (75%) and about 2/3 had less than a 6th grade education (66%). Only 11% had any private health insurance; most (85%) had public health insurance. Only 18% were employed (full or half time) and 78% reported financial hardship in the past year. About half (53%) were married or living with a partner. About half (54%) reported having a chronic medical condition, and 65% reported being in poor or fair health. The type and stage of breast cancer as well as treatment characteristics of these women are summarized elsewhere [15].
Compañera Tracking Form
Participants’ knowledge was high (>85% correct) for four of five knowledge questions (common reactions to breast cancer, remembered more than one type of professional on her treatment team, could describe ways to help family deal with cancer, and could describe good communication skills). Knowledge was poor (53%) for describing breast cancer. No differences between the intervention and control groups were observed on knowledge. Skill mastery was high with over 90% able to correctly perform 10 of 13 skills evaluated (Table 1). The two skills with the lowest ratings (73 and 84%) were being able to successfully role play asking a doctor or other health professional a question about breast cancer (73%) and being able to describe how to use the Cancer Information Service (84%), but even for these, well over 2/3 of the sample did them correctly. No differences between the groups were observed in skill mastery.
At session 2, 86% of the participants completed the distress thermometer homework, but this increased each session, with 97% completing this homework by session 8. Similarly, the percent completing the deep breathing homework was 76% at session 2, but increased to 88% by session 8. Rates of completion of the other types of homework ranged from 80 to 94% with one exception. Only 67% completed the positive thoughts card (creating an affirmation thought card to help cope with stressful events), suggesting that this was particularly challenging for participants. The most frequently mentioned problems with doing the homework were as follows, from the most to least often cited: did the homework, but did not record answers; unable to do it due to side effects; too busy; and could not read/write. For those unable to read and write, compañeras did the homework with participants.
Compañeras’ mean round trip travel time for sessions was 35 min (SD = 19.1). Mean round trip distance traveled was 21 miles (SD = 15.0). Sessions lasted on average 1 h and 45 min (SD = 19). There were no group differences in these statistics.
The primary reason women in the intervention group did not complete at least six sessions was due to serious treatment side effects, while in the control group, women were more likely to report no longer needing a support program after having waited to receive it or family/work hardships. Overall, of women who completed five or less sessions, most never initiated the program.
Fidelity Ratings
Observer ratings of compañeras’ fidelity were high for all six program components (compañeras complied a “great deal/constantly” for 70% or more of the sessions observed). For three of the six components (following the manual, explaining concepts in language participant could understand, and caring/supportive), observer ratings of compañeras’ fidelity were very high (compañeras did this “constantly” in 80–90% of the sessions). The lowest ratings were for checking that participants understood the material, modeling the skills, and providing feedback to participants (30% of the sessions were rated as having been complied with “a fair amount”).
Ratings of the extent to which the compañeras encouraged the participant to practice the skills were either 3 (a great deal) or 4 (constantly), indicating good fidelity. No ratings of “not at all” or “a fair amount” were given for the extent to which the compañeras encouraged participants to practice seven skills (cognitive reframing, good communication, seeking cancer information, practicing stress management, asking for help, increasing helpful activities, and setting goals for self-care).
Program Evaluation Survey
Of the 80 participants who completed at least six sessions, 76 (95%) completed the program evaluation survey (Table 2), 62 from the intervention group and 14 from the control group. Regarding program timing, most (64%) preferred the program as delivered. About one fourth would have preferred to start sooner (26%) and only 9% would have preferred to start later. More from the intervention group than those from the control group preferred starting the program when delivered (71 versus 36%; p < 0.001). No one reported preferring fewer sessions, about 2/3 (67%) felt that the duration should be about the same, and about 1/3 (33%) would have preferred having more sessions. Almost all (97%) preferred the program as delivered rather than by telephone or workbook alone, with no group differences.
The overall quality of the program was rated as very good/excellent by 89% of respondents. The overall quality of the workbook was rated as very good/excellent by 81%. The highest rating was for the skills of the compañeras (96% reported these as being very good/excellent). There were no group differences in quality ratings.
Regarding the usefulness of the program in terms of how much it helped them cope with breast cancer, 93% of participants responded quite a bit/extremely. The highest ratings (>90% rated the usefulness as fairly/very useful) pertained to the workbook (93%) and sections on cancer information (99%), managing thoughts and mood (95%), managing stress (92%), and setting goals (92%). The lowest rating was for the program in general (76%). Regarding its ease of use, the convenience of the program received the highest rating (99% reported it being fairly/very convenient). The lowest rating was for the ease of understanding the workbook (42% reported it as being fairly/very easy). This rating of the workbook varied by group—50% of those in the intervention group reported it as being fairly/very easy, whereas only 7% of the control group reported this. A majority (61%) reported currently practicing the skills.
Regarding open-ended feedback to improve the program, the following themes emerged: (1) make the program more than eight sessions; (2) skip sections that are not relevant (e.g., family section if living alone); (3) add more relaxation and positive thinking skills practice; (4) add group sessions to practice relaxation, meditation, or yoga; (5) accommodate the inability to read/write; and (6) eliminate having to wait for the program (control group only). Apparently, even though compañeras were instructed to skip material that was not relevant for specific women, this did not occur in some cases. Women rated strengths of the program as the information on cancer, personal contact with a survivor, and coping skills training. Stress management skills that participants identified as the most important for their quality of life were as follows: walking, breathing techniques, coping mechanisms, spending time with family and friends, and being more proactive during doctor visits. The majority of participants’ goals focused on healthy lifestyles (exercising and eating better), losing weight, finding a job, going back to school to finish college or learn English, and continuing breathing techniques. An important source of chronic stress that came up frequently was financial hardships because many participants had to quit working in order to focus on their cancer treatment.
Debriefing by Semi-Structured Interviews
We completed debriefing interviews with ten participants and two compañeras. Participants’ mean age was 53 years (SD = 13). Most participants had less than a 6th grade education (50%), and 90% reported financial hardship in the past year. Compañeras were 65 and 59 years old; one was a college graduate and the other had a high school diploma; both had invasive breast cancer and were diagnosed 3+ years prior to the study.
Four major themes emerged from the semi-structured interviews, each with subthemes: benefits of the program, cultural factors that affected the success of the program, suggestions for improving the program, and challenges in delivering the program (Table 3). Pertaining to the benefits mentioned, these included improvements in (1) self-management skills (healthy lifestyles, self-esteem, and ability to cope with stress); (2) knowledge about cancer, cancer treatments, and how to engage more with clinicians and their care; (3) communication skills with family and the interventionist; and (4) mood and sense of hope. Participants described a sense of mastery and self-efficacy to manage their distress, general mood, and other self-care behaviors.
Cultural factors that emerged included the trust that participants had in their compañera due to their shared cultural background, language, and cancer experience. The shared culture and language resulted in one participant expressing that she viewed the compañera as a family member, reflecting the strong bond that developed between them.
Suggestions for improving the program included making the sessions a bit longer and developing a program for participants’ family members. Lengthening the session to allow for time for socializing was recommended by a few participants. Also, several participants indicated they would have liked it if the program had offered some kind of support for family members, especially their children.
Finally, challenges associated with delivery of the program that were voiced in the interviews included limited literacy of some participants and the complexity of the medical terminology related to the sections that describe cancer and cancer treatments. To address issues of limited literacy, compañeras commented that they would do the homework during the sessions with women if needed, which extended the length of these meetings. Several participants expressed having difficulty doing the homework on their own and understanding some of the terminology associated with the side effects of chemotherapy and other treatments.
Discussion
Using mixed methods, we evaluated the processes of implementing a new 8-week CBSM program for Spanish-speaking Latina breast cancer survivors. Program delivery by peers was very good in terms of fidelity. Treatment receipt was successful as evidenced by participants’ ability to demonstrate successfully the skills imparted by the program, e.g., cognitive reframing, stress management, and goal setting. The program was acceptable, useful, and fairly easy to use among this population. In the interviews, participants reported an improved ability to manage stress and mood, greater engagement in their health care, a sense of hope, and trust in the interventionist. Suggested improvements to the program include more sessions to practice skills and simpler exercises and homework that do not require reading and writing.
Participants rated the sections of the program that offered information on cancer, mood management, stress management, and goal setting as the most useful, indicating that cognitive-behavioral approaches are culturally relevant for Latinas. Through the Nuevo Amanecer program, we were able to address effectively the dominant psychosocial issues identified in our prior formative work that affect Latinas with breast cancer: helplessness, lack of control, fear and anxiety, and the need for more information on breast cancer [17]. Also, by delivering this program in community settings, we addressed barriers associated with lack of transportation and limited access to and awareness of cancer psychosocial support programs. The convenience of the program was viewed very favorably and may be an especially critical factor among vulnerable women who face daily hardships. In spite of the convenience, women who dropped out of the program or never started it cited treatment side effects and family or work hardships as reasons. About half of women had some difficulty using the workbook, problems also noted in the qualitative interviews. Most problems had to do with the complexity and literacy level of some of the exercises and homework. Although we made extensive efforts to simplify exercises and language, further simplification and supplementation with audiovisual materials would be helpful. Our results indicate that delivery in-person rather than by phone or the manual alone was preferred and may be necessary to reinforce key skills. In fact, many women suggested including more sessions to have additional opportunities to practice the skills and socialize with the compañeras.
Compañeras demonstrated good fidelity in their ability to impart the information in a way that could be understood by participants and being supportive and encouraging of participants’ use of the coping skills. Training of compañeras may need to place greater emphasis on modeling of desired behaviors, checking in frequently with participants to ensure their comprehension, and providing specific feedback to participants as they practice the skills. In a current study in which the program is being tested with Spanish-speaking Latinas in rural communities, we are monitoring the modeling and reinforcement of the behaviors by the compañeras and how often they observe and provide feedback to participants on the skills performance through site visits, technical assistance, and reminders on monthly conference calls. In preparation for disseminating the program, a program implementation guide for community organizations is under development and training materials are being refined. These materials will emphasize the importance of ensuring fidelity to program delivery and the important role of the peer.
We devoted significant resources to conduct a rigorous implementation evaluation because our study was a first attempt to culturally adapt a CBSM program for delivery by trained peers to low-SES Latinas in community-based settings. Such rigorous implementation studies that utilize mixed methods are critical for assessing fidelity and fit of translated interventions in community-based settings [18]. Our evaluation methods can serve as a model to guide other health disparities researchers in evaluating similar intervention studies.
Through the evaluation, we learned much to inform further testing and dissemination of Nuevo Amanecer and similar programs to reduce psychosocial health disparities in vulnerable groups. We learned that cognitive reframing and behavioral approaches to managing stress are culturally relevant and particularly useful for Latinas with breast cancer. These elements of the program were among the most critical from the perspectives of participants. The women in this study faced chronic stress. They were extremely vulnerable, with most having less than a 6th grade education and almost all having faced financial hardships in the past year. The program we offered helped them increase their sense of control and mastery over their daily lives in spite of such hardships, easing their cancer distress and improving their overall well-being. These types of stress management interventions could be used to improve quality of life in other vulnerable populations, including those with other chronic conditions. Future dissemination efforts will involve development of supplemental audiovisual materials to reinforce key skills, further simplification of exercises, and more demonstration by compañeras and practice by participants of the stress management skills, given that these appear to be key to achieving program effectiveness.
Implications for Cancer Education
A similar pilot study of a peer-delivered breast cancer treatment decision support intervention among Latina breast cancer patients improved women’s involvement with their physicians in treatment decision-making, feelings of low self-efficacy and fatalism [4]. This other intervention has three elements in common with Nuevo Amanecer: (1) delivery in-person by a trained Latina breast cancer survivor; (2) a focus on skills building; and (3) incorporation of Latino cultural values, e.g., personalismo (preference for positive interpersonal relations) and confianza (trust). Incorporation of these three elements is recommended when developing interventions among vulnerable Latina cancer patients.
Conclusions
Our results suggest that this program is feasible and acceptable for use among Spanish-speaking Latina breast cancer survivors, a vulnerable group who is at disproportionately higher risk of psychosocial morbidity following breast cancer, compared to white women [1]. We demonstrated that cognitive-behavioral stress management programs that have been offered typically by mental health professionals in cancer centers can be offered by peers in community settings with good results. Our evaluation results have implications for other investigators seeking to develop psychosocial support programs for low-income, limited English-speaking populations. Results support the use of peer-delivered, evidence-based programs as culturally relevant approaches that may help reduce disparities in distress due to breast cancer and other chronic conditions. This type of approach builds community capacity for delivery of CBSM programs to address the chronic stress faced by vulnerable cancer patients. Employing community-based, trained peer support counselors to deliver CBSM programs will be an important strategy to address shortages of culturally appropriate psycho-oncology services for the growing population of limited English-proficient cancer patients.
References
Ashing-Giwa KT, Lim JW (2011) Examining emotional outcomes among a multiethnic cohort of breast cancer survivors. Oncol Nurs Forum 38(3):279–288
Ashing-Giwa K, Rosales M, Lai L, Weitzel J (2013) Depressive symptomatology among Latina breast cancer survivors. Psychooncology 22(4):845–853
Napoles-Springer AM, Livaudais JC, Bloom J, Hwang S, Kaplan CP (2007) Information exchange and decision making in the treatment of Latina and white women with ductal carcinoma in situ. J Psychosoc Oncol 25(4):19–36
Sheppard VB, Figueiredo M, Canar J, Goodman M, Caicedo L, Kaufman A, Norling G, Mandelblatt J (2008) Latina a Latina: developing a breast cancer decision support intervention. Psychooncology 17(4):383–391
National Comprehensive Cancer Network, Inc. (2013) NCCN Clinical Practice Guidelines in Oncology-Distress Management Version 2.2013. https://www.nccn.org/professionals/physician_gls/f_guidelines.asp#supportive. Accessed June 26, 2016
Antoni MH (2003) Stress management intervention for women with breast cancer. United Book Press, Baltimore
Antoni MH, Lechner S, Diaz A, Vargas S, Holley H, Phillips K, McGregor B, Carver CS, Blomberg B (2009) Cognitive behavioral stress management effects on psychosocial and physiological adaptation in women undergoing treatment for breast cancer. Brain Behav Immun 23(5):580–591
Antoni MH, Lehman JM, Kilbourn KM, Boyers AE, Culver JL, Alferi SM, Yount SE et al (2001) Cognitive-behavioral stress management intervention decreases the prevalence of depression and enhances benefit finding among women under treatment for early-stage breast cancer. Health Psychol 20(1):20–32
Strain JJ, Loigman M (2007) Quick reference for oncology clinicians: the psychiatric and psychological dimensions of cancer symptom management. Edited by Holland JC, Greenberg DB, Hughes MK. Charlottesville, VA: International Psycho-Oncology Society (IPOS) Press
Napoles AM, Santoyo-Olsson J, Stewart AL (2013) Methods for translating evidence-based behavioral interventions for health-disparity communities. Prev Chronic Dis 10:E193
Schneider MW, Hall J, Hernandez AE, Hindes K, Montez G, Pham T, Rosen L et al (2009) Rationale, design and methods for process evaluation in the HEALTHY study. Int J Obes 33(Suppl 4):S60–S67
Hulscher ME, Laurant MG, Grol RP (2003) Process evaluation on quality improvement interventions. Qual Saf Health Care 12(1):40–46
Lavinghouze SR, Snyder K (2013) Developing your evaluation plans: a critical component of public health program infrastructure. Am J Health Educ 44(4):237–243
Linnan L, Steckler A (2002) Process evaluation for public health interventions and research. Jossey-Bass, San Francisco
Napoles AM, Ortiz C, Santoyo-Olsson J, Stewart AL, Gregorich S, Lee HE, Duron Y, McGuire P, Luce J (2015) Nuevo Amanecer: results of a randomized controlled trial of a community-based, peer-delivered stress management intervention to improve quality of life in Latinas with breast cancer. AJPH 105(Suppl 3):e55–e63
Napoles AM, Santoyo-Olsson J, Ortiz C, Gregorich S, Lee HE, Duron Y, Graves K et al (2014) Randomized controlled trial of Nuevo Amanecer: a peer-delivered stress management intervention for Spanish-speaking Latinas with breast cancer. Clin Trials 11(2):230–238
Napoles-Springer AM, Ortiz C, O'Brien H, Diaz-Mendez M (2009) Developing a culturally competent peer support intervention for Spanish-speaking Latinas with breast cancer. J Immigr Minor Health 11(4):268–280
Hawe P, Shiell A, Riley T (2004) Complex interventions: how “out of control” can a randomised trial be? BMJ 328(7455):1561–1563
Acknowledgements
This research was supported by the California Breast Cancer Research Grants Program Office of the University of California (15BB-1300 and 15BB-1301), National Cancer Institute (1U54CA153511), and National Institute on Aging (1 P30 AG15272).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The protocol was approved by the University of California San Francisco and San Mateo Medical Center institutional review boards. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Conflict of Interest
The authors declare that they have no conflict of interest.
Informed Consent
Written informed consent was obtained from all individual participants included in the study. The study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Rights and permissions
About this article

Cite this article
Nápoles, A.M., Santoyo-Olsson, J., Stewart, A.L. et al. Evaluating the Implementation of a Translational Peer-Delivered Stress Management Program for Spanish-Speaking Latina Breast Cancer Survivors. J Canc Educ 33, 875–884 (2018). https://doi.org/10.1007/s13187-017-1202-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13187-017-1202-y