
Abstract
Relevance
Proteasome, a cylindrical complex containing 19S regulatory particle lid, 19S regulatory particle base, and 20S core particle, acted as a major mechanism to regulate the levels of intracellular proteins and degrade misfolded proteins, which involved in many cellular processes, and played important roles in cancer biological processes. Elucidation of proteasome alterations across multiple cancer types will directly contribute to cancer medical services in the context of predictive, preventive, and personalized medicine (PPPM / 3P medicine).
Purpose
This study aimed to investigate proteasome gene alterations across 33 cancer types for discovery of effective biomarkers and therapeutic targets in the framework of PPPM practice in cancers.
Methods
Proteasome gene data, including gene expression RNAseq, somatic mutation, tumor mutation burden (TMB), copy number variant (CNV), microsatellite instability (MSI) score, clinical characteristics, immune phenotype, 22 immune cells, cancer stemness index, drug sensitivity, and related pathways, were systematically analyzed with publically available database and bioinformatics across 11,057 patients with 33 cancer types.
Results
Differentially expressed proteasome genes were extensively found between tumor and control tissues. PSMB4 occurred the top mutation event among proteasome genes, and those proteasome genes were significantly associated with TMB and MSI score. Most of proteasome genes were positively related to CNV among single deletion, control copy number, and single gain. Kaplan–Meier curves and COX regression survival analysis showed proteasome genes were significantly associated with patient survival rate across 33 cancer types. Furthermore, the expressions of proteasome genes were significantly different among different clinical stages and immune subtypes. The expressions of proteasome genes were correlated with immune-related scores (ImmuneScore, StromalScore, and ESTIMATEScore), 22 immune cells, and cancer stemness. The sensitivities of multiple drugs were closely related to proteasome gene expressions. The identified proteasome and proteasome-interacted proteins were significantly enriched in various cancer-related pathways.
Conclusions
This study provided the first landscape of proteasome alterations across 11,057 patients with 33 cancer types and revealed that proteasome played a significant and wide functional role in cancer biological processes. These findings are the precious scientific data to reveal the common and specific alterations of proteasome genes among 33 cancer types, which benefits the research and practice of PPPM in cancers.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The structure and functions of ubiquitin–proteasome system
The proteasome was an abundant multi-enzyme complex that is located both in the nucleus and cytoplasm of eukaryotic cells [1]. The ubiquitin–proteasome system provided the main approach to degrade intracellular proteins. Before the discovery of the ubiquitin–proteasome system, it was commonly thought that protein degradation mainly depended on lysosomes [2]. The proteasome was named as 26S proteasome in mammals and contained 19S regulatory particle lid (Rpn3, Rpn10, Rpn7, Rpn8, Rpn12, Rpn6, Rpn5, Rpn9, Rpn11, Rpn4, Rpn15, PA28α, PA28β, and PA28r), 19S regulatory particle base (Rpn2, Rpn1, Rpn13, Rpt2, Rpt1, Rpt5, Rpt3, Rpt6, Rpt4, and PA200), and 20S core particle (inner two rings, β1, β2, β3, β4, β5, β6, and β7; outer two rings, α1, α2, α3, α4, α5, α6, and α7). Additionally, β1, β2, and β5 in the standard 20S core particle were replaced with β1i, and β2i, and β5i to form immunoproteasome, and β5 in the standard 20S core particle was replaced with β5t to form thymoproteasome [3]. When proteins were tagged for degradation with a single ubiquitin molecule, this signal activated other ubiquitin ligases to form a polyubiquitin chain binding with proteasome to degrade the tagged proteins [4]. The 19S regulatory subunit contained ATPase active sites and ubiquitin-binding sites to recognize polyubiquitinated proteins. The 20S core particle was hollow and allowed the tagged protein with ubiquitin to be degraded [5]. The proteasome was responsible for the degradation of most proteins and involved in almost all life activities. Abnormal functions of the proteasome could cause many diseases [6]. The scientists—Aaron Ciechanover, Avram Hershko, and Irwin Rose—who discovered ubiquitin–proteasome pathway-mediated protein degradation were awarded the Nobel Prize for Chemistry in 2004 [7]. Although structure of the proteasome became clear with the development of electron microscopy, X-ray crystallography [8], and cryogenic electron microscopy [9], it was essential to systematically analyze proteasome and reveal the deubiquitylated, unfolded, and degraded mechanisms in human diseases.
Proteasome dysfunctions in cancers
Proteasome was involved in virtually most cell processes, including cell cycle, cell growth, apoptosis, immune system, cancer stemness, oxidative stress, gene transcription, signal transduction, and differentiation [10]. Subsequently, dysfunctional proteasome can lead to various diseases, such as neurodegenerative diseases, cardiovascular diseases, inflammatory responses and autoimmune diseases, and malignancies [11]. The accumulating evidence demonstrated that these proteasome-related processes were closely associated with cancers, so proteasome was one of key protein machines for carcinogenesis and development [12]. For example, the proteasome showed diverse roles in the process of apoptosis. In advance of apoptosis, increased protein ubiquitination and the related ubiquitin ligases (E1, E2, E3) were observed [13]. During apoptosis, many proteasomes in nucleus tended to translocate from nucleus to outer membrane bleb [14]. Proteasome inhibition was also observed to have different effects on apoptosis among different disease models. In general, when proteasome was inhibited, pro-apoptotic status would be occurred in most cell types [15]. However, cells in quiescent states or primary cultured cells were quite insensitive to proteasome inhibitions [16]. In terms of cellular stresses, proteasomal degradation pathway responded in time to degrade misfolded or unfolded proteins. When cells were subjected to stresses, such as heat shock, infection, or oxidative damage, heat shock proteins identified misfolded proteins and increased the activities of ubiquitin–proteasome system [17]. In particular, inappropriately oxidized histones could be degraded directly by the 20S core particle of proteasome in the nucleus [18]. The proteasome played a critical and straightforward role in the adaptive immune system [19]. When pathogens invaded the organism, proteasome monitored them and activated proteasomal degradation to produce peptide antigens, which were displayed by the major histocompatibility complex class I (MHC) proteins on the surface of antigen-presenting cells [20]. During the immune response, immunoproteasome was formed with immunoproteasomal subunits (β1i, β2i, and β5i). Those specialized β subunits had physiological characteristics of altered substrate specificity [21]. Cell cycle progression was controlled by cyclin-dependent kinases (CDKs) and specific cyclins. When a CDK-cyclin complex completed its function, the specific CDKs were polyubiquitinated and degraded by proteasome to mediate directionality of cell cycle [22]. All those biological processes were involved in important mechanisms of tumorigenesis and progression. Proteasome showed a decreased function in the cellular processes of cancer stem cells compared to the rest of cancer cells [23]. To study transcriptional regulation of proteasome subunit proteins, complex assembly, and pluripotency of proteasome would develop more therapeutic opportunities targeted proteasome for target therapeutics in cancers [24]. Even some studies found circulating proteasomes, which indicated that proteasome had potentiality to be clinical biomarkers [25] for cancers.
Working hypothesis
We hypothesized that proteasome genes played important roles in cancers, and the altered proteasome genes were the potential targets to develop therapeutic drugs for targeted prevention and personalized therapy and construct biomarkers for predictive diagnostics, patient stratification, and personalized medical services in cancers [26, 27].
Study design
The data of proteasome genes from The Cancer Genome Atlas (TCGA) database, including gene expression RNAseq, somatic mutation, tumor mutation burden (TMB), copy number variant (CNV), microsatellite instability (MSI) score, clinical characteristics, immune phenotype, 22 immune cells, and cancer stemness index, were systematically analyzed across 11,057 patients with 33 cancer types. The widespread genetic alterations (including gene expressions, somatic mutations, and CNVs) were found in proteasome genes across 11,057 patients with 33 cancer types. The close correlations between proteasome gene expressions and TMB, MSI, immunity system, cancer stemness, and clinical relevance were also assessed. The proteasome-related activated and inhibited pathways help to further study the molecular mechanism of proteasome in the context of PPPM in cancers. This study highlighted the importance of proteasome in cancers and provided some potential targets on the ubiquitin–proteasome system to develop target therapeutic strategies for cancers.
Expected impacts in the framework of predictive, preventive, and personalized medicine
We expect the altered proteasome genes and pathways will be the important targets to develop effective therapeutic drugs for targeted prevention and personalized therapy and clinical biomarkers for predictive diagnosis or disease prognosis, patient stratification, and guiding clinical therapy to personalize management of cancer patients in the framework of predictive, preventive, and personalized medicine (PPPM / 3P medicine) [24, 26, 27].
Materials and methods
Collection of proteasome genes
The proteasome genes in proteasome complex were 19S regulatory particle lid (n = 14 genes), containing PSMD3, PSMD4, PSMD6, PSMD7, PSMD8, PSMD9, PSMD11, PSMD12, PSMD13, PSMD14, SEM1, PSME1, PSME2, and PSME3; 19S regulatory particle base (n = 10 genes), containing PSMD1, PSMD2, ADRM1, PSMC1, PSMC2, PSMC3, PSMC4, PSMC5, PSMC6, and PSME4; and 20S core particle (n = 14), containing PSMA1, PSMA2, PSMA3, PSMA4, PSMA5, PSMA6, PSMA7, PSMB1, PSMB2, PSMB3, PSMB4, PSMB5, PSMB6, and PSMB7. For immunoproteasome, PSMB1, PSMB2, and PSMB5 were replaced with PSMB8, PSMB9, and PSMB10. For thymoproteasome, PSMB5 was replaced with PSMB11 (Supplementary Table 1).
Genome-wide omics data across 33 cancer types
Genome-wide omics data were based on UCSC Xena datasets (https://xenabrowser.net/datapages/). A total of 11,057 patients (10,327 cancer samples and 730 control samples) with 33 different cancer types were analyzed (Table 1), including adrenocortical carcinoma (ACC; tumor = 79), bladder urothelial carcinoma (BLCA; tumor vs. control = 411 vs. 19), breast cancer (BRCA; tumor vs. control = 1104 vs. 113), cervical squamous cell carcinoma and endocervical adenocarcinoma (CESC; tumor vs. control = 306 vs. 3), cholangiocarcinoma (CHOL; tumor vs. control = 36 vs. 9), colon adenocarcinoma (COAD; tumor vs. control = 471 vs. 41), lymphoid neoplasm diffuse large b-cell lymphoma (DLBC; tumor = 48), esophageal carcinoma (ESCA; tumor vs. control = 162 vs. 11), glioblastoma multiforme (GBM; tumor vs. control = 168 vs. 5), head and neck squamous carcinoma (HNSC; tumor vs. control = 502 vs. 44), kidney chromophobe (KICH; tumor vs. control = 65 vs. 24), kidney renal clear cell carcinoma (KIRC; tumor vs. control = 535 vs. 72), kidney renal papillary cell carcinoma (KIRP; tumor vs. control = 289 vs. 32), acute myeloid leukemia (LAML; tumor = 151), brain lower grade glioma (LGG; tumor = 529), liver hepatocellular carcinoma (LIHC; tumor vs. control = 374 vs. 50), lung adenocarcinoma (LUAD; tumor vs. control = 526 vs. 59), lung squamous cell carcinoma (LUSC; tumor vs. control = 501 vs. 49), mesothelioma (MESO; tumor = 86), ovarian serous cystadenocarcinoma (OV; tumor = 379), pancreatic adenocarcinoma (PAAD; tumor vs. control = 178 vs. 4), pheochromocytoma and paraganglioma (PCPG; tumor vs. control = 183 vs. 3), prostate adenocarcinoma (PRAD; tumor vs. control = 499 vs. 52), rectum adenocarcinoma (READ; tumor vs. control = 167 vs. 10), sarcoma (SARC; tumor vs. control = 263 vs. 2), skin cutaneous melanoma (SKCM; tumor vs. control = 471 vs. 1), stomach adenocarcinoma (STAD; tumor vs. control = 375 vs. 32), testicular germ cell tumors (TGCT; tumor = 156), thyroid carcinoma (THCA; tumor vs. control = 510 vs. 58), thymoma (THYM; tumor vs. control = 119 vs. 2), uterine corpus endometrial carcinoma (UCEC; tumor vs. control = 548 vs. 35), uterine carcinosarcoma (UCS; tumor = 56), and uveal melanoma (UVM; tumor = 80). Genome-wide omics data included gene expression RNAseq (HTSeq-FPKM GDC Hub, Supplementary Table 2), somatic mutation (VarScan2 Variant Aggregation and Masking, Supplementary Table 3), CNV (GISTIC-focal score by gene GDC Hub), clinical characteristics (Curated clinical data by Pan-Cancer Atlas Hub), immune phenotype (Immune subtype by Pan-Cancer Atlas Hub), and cancer stemness index (Stemness score-RNA based by Pan-Cancer Atlas Hub). Maftools R package (https://www.bioconductor.org/packages/release/bioc/html/maftools.html) was used to calculate the TMB distribution according to somatic mutation data, which also generated result for waterfall of mutation genes (Supplementary Table 4). MSI scores were obtained from published data (PMID: 30,211,344, and Supplementary Table 5) that were generated by TCGA Research Network (http://cancergenome.nih.gov/).
Determination of differentially expressed genes (DEGs) between tumors and control tissues in each cancer type
DEGs were determined in tumors compared to control tissues with the ggpubr R package (https://rpkgs.datanovia.com/ggpubr/) across 33 cancer types (adjusted p value < 0.05) (Supplementary Table 6; Supplementary Fig. 1). An empirical Bayesian algorithm approach was used to estimate gene expression alterations with Wilcox test. The Benjamini–Hochberg multiple testing was used to calculate the adjusted p value. The heatmap of DEGs was plotted by pheatmap R package (https://www.rdocumentation.org/packages/pheatmap/versions/1.0.12/topics/pheatmap).
Correlations of proteasome gene expressions with TMB, MSI, or CNV
Corrplot R package (https://cran.r-project.org/web/packages/corrplot/vignettes/corrplot-intro.html) was used to perform the correlation analysis between proteasome gene expression and TMB or MSI with the Spearman method (p < 0.05). The fmsb R package (https://cran.r-project.org/web/packages/fmsb/index.html) was used to plot the correlation between proteasome gene expression and TMB (Supplementary Fig. 2) or between proteasome gene expression and MSI (Supplementary Fig. 3) by radar chart. The correlation between proteasome gene expression and CNV was calculated with Kruskal test (p < 0.05), and boxplots were plotted with barplot R package (https://www.rdocumentation.org/packages/graphics/versions/3.6.2/topics/barplot). The chromosome localization circle was plotted with RCircos R package (https://www.rdocumentation.org/packages/RCircos/versions/1.2.1).
The associations between proteasome gene expressions and clinical features
The samples were divided into high- and low-expression groups of proteasome genes by median value of each proteasome gene across 33 cancer types. The Kaplan–Meier method by survminer R package (https://cran.r-project.org/web/packages/survminer/index.html) was used for overall survival (OS) analysis, which was compared to the log-rank test, with statistical significance of p < 0.05. Cox regression analysis was also performed with survival R package (https://www.rdocumentation.org/packages/survival/versions/3.2-3) to select survival-related proteasome genes. The hazard ratio (HR) was calculated for Cox proportional hazard regression models (Supplementary Table 7), and the survival data of proteasome genes across 33 cancer types (n = 10,121) were listed (Supplementary Table 8). Further, the associations between clinical characteristics and proteasome genes were analyzed across 33 cancer types. The clinical data of 33 cancer types were listed (Supplementary Table 9), including pathologic stage (stages I, II, III, and IV), pathologic metastasis, pathologic node, and pathologic tumor size.
The expressions of proteasome genes among immune phenotypes across 33 cancer types
Samples of TCGA Pan-Cancer data were divided into five clusters, including wound healing (Immune C1), IFN-gamma dominant (Immune C2), inflammatory (Immune C3), lymphocyte depleted (Immune C4), and immunologically quiet (Immune C5) based on subtypes of immune model. The different expressions of proteasome genes among subtypes of immune model with Kruskal test (p < 0.05) were plotted with ggplot2 R package (https://cran.r-project.org/web/packages/ggplot2/index.html).
Estimation of immune-related scores across 33 cancer types
ESTIMATE R package (https://bioinformatics.mdanderson.org/estimate/rpackage.html) was used to estimate the presence of infiltrating stromal and immune cells in malignant tumor tissues with gene expression data. ESTIMATE algorithm based on ssGSEA analysis generated three types of scores: (i) StromalScore that captured the presence of stroma in tumor tissue, (ii) ImmuneScore that represented the infiltration of immune cells in tumor tissue, and (iii) ESTIMATEScore, (Supplementary Table 10), which were positively correlated with the ratio of stromal cells, immune cells, and the sum of both, respectively. Also, for each score, the higher score means the larger ratio of the corresponding component in tumor microenvironment (TME). Corrplot R package (https://cran.r-project.org/web/packages/corrplot/vignettes/corrplot-intro.html) was used to determine the correlations of proteasome gene expression with ImmuneScore, StromalScore, and ESTIMATEScore with the Spearman method (p < 0.05) (Supplementary Fig. 4).
Calculation of the proportions of immune cells across 33 cancer types
The CIBERSORT algorithm and LM22 gene signature were used to determine the proportions of immune cells across 33 cancer types. This algorithm can discriminate 22 human immune cell phenotypes with high sensitivity and high specificity. Gene expression profiles in the format of standard annotation files were input to the CIBERSORT web portal (http://cibersort.stanford.edu/), and its algorithm was run with LM22 signature and 1,000 permutations (Supplementary Table 11). Corrplot R package (https://cran.r-project.org/web/packages/corrplot/vignettes/corrplot-intro.html) was used to determine the correlation of proteasome gene expressions with different immune cells with the Spearman method (p < 0.05) (Supplementary Fig. 4), including B cells naïve, B cells memory, plasma cells, T cells CD8, T cells CD4 naïve, T cells CD4 memory resting, T cells CD4 memory activated, T cells follicular helper, T cells regulatory (Tregs), T cells gamma delta, NK cells resting, NK cells activated, monocytes, macrophages M0, macrophages M1, macrophages M2, dendritic cells resting, dendritic cells activated, mast cells resting, mast cells activated, eosinophils, and neutrophils.
The associations of proteasome gene expression with cancer stemness, and with drug sensitivity
RNA expression-based (all sets of available genes) stemness scores (RNAss) were derived from the stemness group based on epigenetically regulated RNA expression of 103 stemness-related genes. Corrplot R package (https://cran.r-project.org/web/packages/corrplot/vignettes/corrplot-intro.html) was used to determine the correlation between proteasome gene expression and RNAss with the Spearman method (p < 0.05). The CellMiner (https://discover.nci.nih.gov/cellminer/) was a web-based genomic and pharmacologic tool to explore transcript and drug patterns in the NCI-60 cell line set. The NCI-60 cell set was used to effectively screen anti-cancer drug efficacy, which was developed by the Developmental Therapeutics Program (DTP), US National Cancer Institute (NCI). The NCI-60 cell set has been used to screen many thousands of compounds. The association between proteasome gene expression and drug sensitivity was performed with Corrplot R package plus Spearman method (p < 0.05) based on the corresponding data from CellMiner (Supplementary Table 12).
Functional characteristics and pathways of proteasome and its interacted proteins
The co-expressions between proteasome genes were plotted with Corrplot R package plus Spearman method (p < 0.05). The interactions between proteasome proteins and non-proteasome proteins were analyzed with String website (https://string-db.org/) to obtain proteasome-interacted proteins with combined score more than 0.9 (Supplementary Table 13). Gene Set Variation Analysis (GSVA) is a non-parametric, unsupervised method to estimate variation of gene set enrichment via the samples of an expression dataset. Proteasome proteins and proteasome-interacted proteins were used to enrich statistically significant Kyoto Encyclopedia of Genes and Genomes (KEGG) pathways (p < 0.05 and FDR < 0.05), and these KEGG pathways were further analyzed with GSVA to compare the pathway difference between tumor and control tissues across 33 cancer types (Supplementary Table 14). Also, proteasome proteins and proteasome-interacted proteins were used to enrich statistically significant Gene Ontology (GO) terms with Cytoscape ClueGO (two-sided hypergeometric test, adjusted p value < 0.05 corrected with Benjamini–Hochberg multiple testing), including cellular components (CCs), molecular functions (MFs), and biological processes (BPs) (Supplementary Table 15).
Results
Proteasome genes expressed differentially between tumor and control tissues across different cancer types
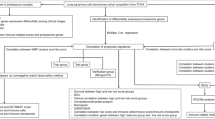
The proteasome was named as 26S proteasome in mammals, which contained 19S regulatory particle lid, 19S regulatory particle base, and 20S core particle. Additionally, proteasomal subunits β1, β2, and β5 in 20S core particle were replaced with β1i, β2i, and β5i for immunoproteasome, and β5 in 20S core particle was replaced with β5t for thymoproteasome (Fig. 1A and Supplementary Table 1). The mRNA expression levels of each proteasome gene were analyzed between tumor and control tissues in each cancer. For example, PSMA5 was differentially expressed between tumor and control tissues across 21 cancer types (Fig. 1B), and the mRNA differential expressions of the rest 41 proteasome genes between tumor and control tissues across 21 cancer types were collected (Supplementary Table 6 and Supplementary Fig. 1), and these 21 cancer types included BLCA, BRCA, CESC, CHOL, COAD, ESCA, GBM, HNSC, KICH, KIRC, KIRP, LIHC, LUAD, LUSC, PAAD, PCPG, PRAD, READ, STAD, THCA, and UCEC (Fig. 1C), while mRNA differential expressions of each proteasome gene were not analyzed in the other 11 cancer types without the corresponding control tissues. Most of proteasome genes were significantly down-regulated in KICH and PCPG (p < 0.05), for example, PSMA5, PSMD4, PSMC5, PSMB1, PSMB6, PSMB3, and PSMB2 in KICH, and PSMA5, PSME2, PSMB7, PSMD7, PSMD6, PSME1, PSMD2, PSME4, ADRM1, and PSMA6 in PCPG. Some of proteasome genes were significantly up-regulated in various cancer types (p < 0.05), for example, PSMD14 in cancer types STAD, READ, COAD, CESC, HNSC, BLCA, BRCA, UCEC, ESCA, LUAD, LUSC, CHOL, and LIHC; SEM1 in cancer types CHOL, READ, COAD, STAD, HNSC, LUAD, KICH, UCEC, LIHC, BLCA, KIRP, GBM, ESCA, and LUSC; PSMA5 in cancer types STAD, READ, HNSC, LUAD, KIRP, BRCA, LIHC, LUSC, CHOL, CESC, GBM, BLCA, UCEC, and ESCA; PSMB3 in cancer types STAD, READ, HNSC, LUAD, KIRP, BRCA, LIHC, LUSC, CHOL, CESC, GBM, BLCA, UCEC, and ESCA; PSMB4 in cancer types READ, HNSC, BRCA, UCEC, BLCA, LUAD, GBM, ESCA, LUSC, LIHC, and CHOL; PSMB8 in cancer types LIHC, UCEC, THCA, STAD, BLCA, HNSC, CESC, ESCA, KIRP, KIRC, CHOL, and GBM; and PSMB9 in cancer types BLCA, LIHC, STAD, READ, KIRP, CESC, HNSC, CHOL, ESCA, KIRC, and GBM.

Pan-cancer expression and mutation alterations of proteasome genes. A The components of proteasome. B The expressions of PMSA5 between tumor and control tissues across 21 cancer types. C The expression alterations of proteasome genes across 21 cancer types. The heat map shows the fold changes, with red representing up-regulated genes and green representing down-regulated genes. D The mutation frequency of proteasome genes across 33 cancer types. E The association between PSMA5 expression and TMB across 33 cancer types. TMB, tumor mutation burden. BLCA, bladder urothelial carcinoma. BRCA, breast cancer. CESC, cervical squamous cell carcinoma and endocervical adenocarcinoma. CHOL, cholangiocarcinoma. COAD, colon adenocarcinoma. ESCA, esophageal carcinoma. GBM, glioblastoma multiforme. HNSC, head and neck squamous carcinoma. KICH, kidney chromophobe. KIRC, kidney renal clear cell carcinoma. KIRP, kidney renal papillary cell carcinoma. LIHC, liver hepatocellular carcinoma. LUAD, lung adenocarcinoma. LUSC, lung squamous cell carcinoma. PAAD, pancreatic adenocarcinoma. PCPG, pheochromocytoma and paraganglioma. PRAD, prostate adenocarcinoma. READ, rectum adenocarcinoma. STAD, stomach adenocarcinoma. THCA, thyroid carcinoma. UCEC, uterine corpus endometrial carcinoma. *p < 0.05, **p < 0.01, and ***p < 0.001
The overall average mutation frequency of proteasome genes across 33 cancer types
The overall average mutation frequency of proteasome genes was low, ranging from 0.01 to 20%. The proteasome genes PSME4, PSMD1, PSMD2, PSMC2, PSMC4, PSMB11, PSMC6, PSMD12, PSMA2, PSMD11, PSMD3, PSMC5, PSMB4, PSMA1, PSMA4, PSMD6, and PSMB8 were identified to have higher mutation frequencies (more than 5%) across 33 cancer types (Fig. 1D and Supplementary Table 3). Moreover, the correlations between proteasome gene expressions and TMB score (Supplementary Table 4) were evaluated across 33 cancer types (Supplementary Fig. 2); for example, the expression of PSMA5 was significantly negatively correlated with TMB scores of cancer types PCPG and THYM and positively correlated with TMB scores of cancer types ESCA, KIRC, BLCA, COAD, LIHC, PRAD, SARC, UCEC, BRCA, KIRP, LGG, LUAD, PAAD, SKCM, and STAD (Fig. 1E). Similarly, the correlations of the other proteasome genes and TMB scores were collected in Supplementary Fig. 2.
The CNV and MSI alterations of proteasome genes across different cancer types
CNV was the repeated sections of the genome that varied between individuals. Whether the CNV affected the expression of proteasome genes, the expression perturbations of proteasome genes were therefore explored across 33 cancer types. The CNV alteration frequencies of proteasome genes were widespread positively correlated with the expressions of proteasome genes, which were prevalent in cancer types BLCA, BRCA, CESC, HNSC, COAD, ESCA, LGG, LIHC, LUAD, LUSC, OV, PAAD, PRAD, SARC, SKCM, STAD, and UCEC (Fig. 2A). CNV alterations were likely one of the gene-driving mechanisms leading to perturbations in the expressions of proteasome genes. For example, PSMA5 was significantly down-regulated in single deletion CNV group and up-regulated in single gain CNV group, compared to control CNV group in BRCA (Fig. 2B). PSMA5 also showed the same positive correlation results in other cancer types, such as LUSC (Fig. 2C), BLCA, BRCA, CESC, CHOL, COAD, DLBC, ESCA, GBM, HNSC, KICH, KIRC, KIRP, LAML, LGG, LIHC, LUAD, LUSC, MESO, OV, PAAD, PCPG, PRAD, READ, SARC, SKCM, STAD, TGCT, THCA, THYM, and UCEC (Fig. 2A). Moreover, the proteasome genes are mainly located in chromosome (chr)1, chr2, chr3, chr6, chr7, chr9, chr11, chr12, chr14, chr15, chr16, chr17, chr19, and chr20 (Fig. 2D). Microsatellites were the repeated DNA sequences, and MSI indicated dysfunction of DNA mismatch repair (MMR) [28]. The correlations between proteasome genes expressions and MSI score (Supplementary Table 5) were evaluated across 33 cancer types, which showed the widespread positive correlations between the expression and MSI of proteasome genes. Here showed the correlations between PSMA5 expression and MSI across 33 cancer types (Fig. 2E), and the significant correlations between PSMA5 expression and MSI were presented in cancer types BRCA, LUAD, SARC, UCEC, CESC, KIRC, KIRP, OV, THCA, COAD, DLBC, HNSC, LUSC, and STAD. The correlations of all other proteasome gene expressions and MSI were listed (Supplementary Fig. 3).

Pan-cancer CNV and MSI alterations of proteasome genes. A The correlations between mRNA expressions and CNV alteration frequency of proteasome genes across 33 cancer types. B The correlations between mRNA expression and CNV alteration frequency of PSMA5 in BRCA. C The correlations between mRNA expression and CNV alteration frequency of PSMA5 in LUSC. D The chromosome localization of proteasome genes. E The associations between PSMA5 mRNA expression and MSI across 33 cancer types. CNV, copy number variant. MSI, microsatellite instability. *p < 0.05, **p < 0.01, and ***p < 0.001
Clinical relevance of proteasome genes across different cancer types
Overall survival of each proteasome gene was analyzed across 33 cancer types, and many of them were significantly related to patient survival rates (Fig. 3A). (i) The high expressions of proteasome genes showed as consistent risky factors in some cancer types. For example, the high expressions of proteasome genes PSMD4, PSMD11, PSMD13, PSMD14, PSME2, PSMC1, PSMC3, PSMC4, PSMC6, PSME4, PSMA1, PSMA2, PSMA4, PSMA5, PSMA7, PSMB1, PSMB2, PSMB4, PSMB5, and PSMB7 showed a poor survival in ACC. The high expressions of proteasome genes PSMD3, PSMD7, PSME1, PSME3, PSMD1, PSMC2, PSMB3, PSMB8, PSMB10, PSMD4, PSMD13, PSMD14, PSME2, PSMC4, PSMA4, PSMA7, PSMB1, PSMB2, and PSMB5 showed a poor survival in LAML. The high expressions of proteasome genes PSMD6, PSMD8, PSMD2, PSMC5, PSMA3, PSMD11, PSMC1, PSMC3, PSMC6, PSME4, PSMA1, PSMA2, PSMA5, PSMB4, PSMD3, PSMD1, PSMD4, PSMD13, PSMD14, PSMA7, PSMB2, and PSMB5 showed a poor survival in LICH. The high expressions of proteasome genes PSMD2, PSMC1, PSMC6, PSMA1, PSMA2, PSMA5, PSMD1, PSMB5, PSMB6, PSMB7, PSME3, and PSMC4 showed a poor survival in LUAD. (ii) The high expression of proteasome genes showed as consistent protective factors in some cancer types. For example, the high expressions of proteasome genes PSMA5, PSMB6, PSMD6, PSMD14, PSMB2, ADRM1, PSMA6, PSMB9, PSMD12, PSMB3, PSME2, and PSMA4 showed a better survival in OV. The high expressions of proteasome genes PSME2, SEM1, PSME1, and PSMB8 showed a better survival in BRCA. Here, we also provided Kaplan–Meier survival analysis curves of PSMA5 in ACC (Fig. 3B), ESCA (Fig. 3C), KIRC (Fig. 3D), LGG (Fig. 3E), LIHC (Fig. 3F), LUAD (Fig. 3G), OV (Fig. 3H), and PAAD (Fig. 3I), as an example, which clearly demonstrated that the high expressions of PSMA5 in these cancers showed a poor survival.

Overall survival-related proteasome genes across 33 cancer types. A Summary of the correlations between proteasome gene expressions and patient overall survival across 33 cancer types. Red represents a higher expression of proteasome genes associated with worse survival, and green represents an association with better survival. Only p values < 0.05 are shown. B Kaplan–Meier survival curve of PSMA5 expression in ACC. C Kaplan–Meier survival curve of PSMA5 expression in ESCA. D Kaplan–Meier survival curve of PSMA5 expression in KICR. E Kaplan–Meier survival curve of PSMA5 expression in LGG. F Kaplan–Meier survival curve of PSMA5 expression in LIHC. G Kaplan–Meier survival curve of PSMA5 expression in LUAD. H Kaplan–Meier survival curve of PSMA5 expression in OV. I Kaplan–Meier survival curve of PSMA5 expression in PAAD. The patients were grouped by median value of global expression pattern of proteasome genes. ACC, adrenocortical carcinoma. ESCA, esophageal carcinoma. KICR, kidney renal clear cell carcinoma. LGG, brain lower grade glioma. LIHC, liver hepatocellular carcinoma. LUAD, lung adenocarcinoma. OV, ovarian serous cystadenocarcinoma. PAAD, pancreatic adenocarcinoma
Further, the expressions of proteasome genes were acted as continuous variable for Cox regression analysis to obtain hazard ratio (HR) across 33 cancer types (risky factor: HR > 1 and protective factor: HR < 1). Most of the results were consistent with Kaplan–Meier survival analysis (Fig. 4 and Supplementary Table 7). For example, except for PSMB10, all other proteasome genes acted as risky factors (HR > 1) in ACC. Most of proteasome genes acted as risky factors (HR > 1) in KICH, including PSMA1, PSMA3, PSMA4, PSMA5, PSMA6, PSMA7, PSMB1, PSMB2, PSMB3, PSMB4, PSMB5, PSMB6, PSMB8, PSMB9, PSMC2, PSMC3, PSMC4, PSMC5, PSMC6, PSMD1, PSMD3, PSMD4, PSMD9, PSMD11, PSMD12, PSMD13, PSMD14, PSME2, PSME3, and PSME4. All other Cox regression analysis of proteasome genes in other cancers was listed (Fig. 4 and Supplementary Table 7).

The distribution of hazard ratios (HR) of proteasome genes across different cancer types using COX regression survival analysis. HR > 1: risk factor. HR < 1: protective factor
Moreover, the associations between pathologic stages (stages I, II, III, and IV) and proteasome genes were analyzed across 33 cancer types (Fig. 5A). Many proteasome genes were significantly expressed differentially among different pathologic stages in the same cancer; for example, the significantly differential expressions of proteasome genes PSMD13, PSMA4, PSMA1, ADRM1, PSME2, PSMB4, PSMB3, PSMA5, PSMB10, PSMC4, PSMB2, PSMB9, SEM1, PSMC3, PSMD4, PSMB8, PSMC1, PSMD14, PSMD8, PSMA7, PSMA2, PSMC5, PSMB6, PSMB1, PSMD11, PSMC2, PSMD3, PSMD2, PSMB5, and PSMC6 among different pathological stages in KIRC. The same proteasome gene was significantly expressed differentially among different pathological stages in various cancers; for example, PSMD8 was significantly expressed differentially among pathological stages in cancer types ACC, BLCA, BRCA, CESC, CHOL, COAD, DLBC, ESCA, GBM, HNSC, KICH, KIRC, KIRP, LIHC, LUAD, LUSC, MESO, OV, PAAD, READ, SKCM, STAD, TGCT, THCA, THYM, and UCEC. PSMD11 was significantly expressed differentially among pathological stages in cancer types ACC, BLCA, BRCA, CESC, CHOL, COAD, DLBC, ESCA, GBM, HNSC, KICH, KIRC, KIRP, LIHC, LUAD, LUSC, MESO, OV, PAAD, READ, SKCM, STAD, TGCT, THCA, THYM, and UCEC. SEM1 was significantly expressed differentially among pathological stages in cancer types BLCA, BRCA, CESC, CHOL, COAD, DLBC, ESCA, GBM, HNSC, KICH, KIRC, KIRP, LIHC, LUAD, LUSC, MESO, OV, PAAD, READ, SKCM, STAD, TGCT, THCA, THYM, and UCEC. Here, we also provided an example to present the associations between pathologic stages and proteasome gene expressions in KICH, which clearly showed that proteasome genes PSMA5, PSMD11, PSMB2, PSMB5, PSMD14, PSMD3, PSME4, PSMD8, PSMD12, PSMC2, PSMA1, and SEM1 were significantly expressed differentially among pathologic stages in KICH (Fig. 5B).

The proteasome genes expressed differentially among clinical stages across 33 cancer types. A Summary of the correlations between proteasome gene expressions and clinical stages. Only p values < 0.05 are shown in blue. B Box plots showing the expression distribution of proteasome genes among different clinical stages in KICH. KICH, kidney chromophobe. *p < 0.05 and **p < 0.01
Association of proteasome gene expressions with immune microenvironment
To explore associations of proteasome gene expressions with immune microenvironment, an overall analysis showed that all proteasome gene expressions were significantly related to immune subtypes C1, C2, C3, C4, and C5 (Fig. 6A). For further detailed analysis of associations of proteasome gene expressions with immune microenvironment, the associations of proteasome gene expressions with immune-related sores (ImmuneScore, StromalScore, and ESTIMATEScore) (Supplementary Table 10) and immune cells (Supplementary Table 11) were analyzed. Some results were obvious and consistent; for example, PSME1, PSME2, PSMB8, PSMB9, and PSMB10 were positively related to ESTIMATEScore (Fig. 6B), ImmuneScore, CD8 T cell (Fig. 6C), macrophages M1, NK cells activated, and T cells CD4 memory activated in various cancer types (Supplementary Fig. 4). Most of proteasome genes showed widespread negative associations with B cells naïve, mast cells activated, mast cells resting, and T cells CD4 memory resting (Supplementary Fig. 4). In addition, some cancer types showed different trends from others in the same association plot. For example, most of proteasome genes in ACC group were negatively associated with ESTIMATEScore, including PSMA6, PSMC6, PSMB5, PSMC1, PSMB7, PSME2, PSMD6, PSMD12, PSMD14, PSMB11, PSMD8, PSMC4, PSMA3, PSMD1, PSME1, PSMD11, PSMA4, PSMD3, PSME4, and PSMC (Fig. 6B), while most of proteasome genes in UVM group were positively associated with ESTIMATEScore, including PSMB4, PSMB1, PSMA6, PSMA3, PSMA5, PSMD13, PSMB6, PSME3, SEM1, PSMC5, PSMD11, PSMB5, PSMD3, PSMB2, PSME1, PSMC3, PSMB3, PSMD8, PSMC4, PSME2, PSMB8, PSMB10, and PSMB9 (Fig. 6B). The consistent phenomenon was also observed in association plot of immune cells, such as CD8 T cell (Fig. 6C; Supplementary Fig. 4).

The immune relevance of proteasome genes across 33 cancer types. A Box plots showing the expression distribution of proteasome genes among different immune subtypes (C1, C2, C3, C4, C5, and C6) across 33 cancer types. B The correlations between proteasome gene expressions and ESTIMATEScore across 33 cancer types. C The correlations between proteasome gene expressions and CD8 T cells across 33 cancer types. Red dots represent positive correlation, and blue dots represent negative correlation. ***p < 0.001
Associations of proteasome gene expressions with stemness score RNAss, and with drug sensibility
Most of proteasome genes showed widespread positive associations with stemness score RNAss in many kinds of cancers; for example, the expressions of proteasome genes PSMD9, PSMB11, PSMC5, PSMA3, PSMD3, PSMA6, PSMB9, PSMD6, PSMD2, PSMB1, PSMA2, PSMD14, PSME2, SEM1, PSMD7, PSMB6, PSMC4, PSMB10, PSMB8, PSMB4, PSMA7, PSMB7, PSME1, PSMD4, PSMC3, PSMB3, PSMD8, PSMA1, PSMD13, PSMA4, PSMA5, and PSMB2 were significantly positively related to RNAss in THYM (Fig. 7A). PSMB9 and PSMB10 showed significantly negatively associations with RNAss in various cancer types; for example, PSMB9 was significantly negatively related to RNAss in cancer types KICH, LGG, PRAD, and TGCT; and PSMB10 was significantly negatively related to RNAss in cancer types LGG, ACC, PRAD, TGCT, KICH, PCPG, LUSC, and LAML (Fig. 7A).

Pan-cancer analysis of RNAss and drug sensitivity associations with proteasome genes. A The correlations between proteasome gene expressions and RNAss across 33 cancer types. Red dots represent positive correlation, and blue dots represent negative correlation. RNAss means RNA expression-based stemness scores. B The drug sensitivity relevance of proteasome gene expression
Moreover, the associations of proteasome gene expressions with drug sensibility were investigated. Some proteasome genes showed positive associations with drug sensibility, including PSMB10 and hydroxyurea, PSMA6 and chelerythrine, PSMB10 and asparaginase, PSMB10 and pipobroman, PSMB10 and uracil mustard, PSMB10 and thiotepa, PSMB10 and triethylenemelamine, PSMB10 and chlorambucil, PSMB10 and cyclophosphamide, PSMB10 and melphalan, PSMB10 and LMP-400, PSMB10 and chelerythrine, PSMB9 and hydroxyurea, PSMB9 and asparaginase, PSMB9 and chlorambucil, PSMB9 and LMP-400, PSMD3 and 5-fluoro deoxy uridine 10mer, PSMB10 and cladribine, PSMB10 and nitrogen mustard, PSMB7 and chelerythrine, PSME1 and chelerythrine, PSMB10 and nelarabine, PSMB10 and cytarabine, PSMB9 and uracil mustard, PSMA6 and nelarabine, PSMB1 and chelerythrine, PSMD9 and hydroxyurea, PSMB10 and imexon, PSMB10 and carmustine, PSMB10 and XK-469, PSMD7 and chelerythrine, PSMB10 and idarubicin, PSMB10 and bendamustine, PSMA7 and chelerythrine, PSME1 and hydroxyurea, and PSME1 and nelarabine (Fig. 7B and Supplementary Table 12). The expression of PSMB10 showed negative association with kahalide f (Supplementary Table 12). These findings indicated that those drug sensibility-associated proteasome genes were the potential drug therapeutic targets.
Functional characteristics and signaling pathways of proteasome-interacted proteins revealed the crucial mechanisms of proteasome
The co-expression network of proteasome genes showed that they worked together well and existed widespread positive correlations (Fig. 8A). To explore potential mechanism of proteasome, protein–protein interaction (PPI) network was constructed to obtain proteasome-interacted proteins with combined score more than 0.9 (Fig. 8B and Supplementary Table 13). Those identified proteasome-interacted proteins (n = 165) and proteasome proteins (n = 42) across 33 cancer types were used to enrich statistically significant KEGG pathways, and these KEGG pathways were further analyzed with GSVA to obtain altered KEGG pathways between tumor and control tissues (Fig. 8C). A total of 31 altered significant KEGG pathways was identified across 33 cancer types between tumor and control tissues; 9 of them were inhibited (ECM receptor interaction, GAP junction, p53 signaling pathway, cell cycle, regulation of autophagy, natural killer cell-mediated cytotoxicity, antigen processing and presentation, apoptosis, and VEGF signaling pathway), and 22 of them were activated (B cell receptor signaling pathway, intestinal immune network for IgA production, WNT signaling pathway, leukocyte transendothelial migration, notch signaling pathway, T cell receptor signaling pathway, ubiquitin-mediated proteolysis, TGF beta signaling pathway, focal adhesion, cell adhesion molecules cams, chemokine signaling pathway, ABC transporters, hedgehog signaling pathway, tight junction, NOD-like receptor signaling pathway, endocytosis, proteasome, dorso ventral axis formation, inositol phosphate metabolism, and phosphatidylinositol signaling system) (Fig. 8D and Supplementary Table 14).

The functional characteristics and signaling pathways enriched with proteasome genes and their interacted genes. A The co-expression network of proteasome genes. Blue dots represent positive correlation, and red dots represent negative correlation. B Protein–protein interaction (PPI) networks based on proteasome genes and proteasome-interacted genes (combined score > 0.9). C The heat map of proteasome-related pathway alterations between tumor and control tissues across 21 cancer types. Red represents activated pathways, and green represents inhibited pathways. D The volcano plot presented the activation and inhibition of signaling pathways. Red represents activated pathways, and green represents inhibited pathways. E BP analysis of proteasome genes and proteasome-integrated genes. F CC analysis of proteasome genes and proteasome-interacted genes. G MF analysis of proteasome genes and proteasome-interacted genes. BP, biological process. CC, cellular component. MF, molecular function
GO enrichment analysis revealed the functional characteristics of those proteasome-interacted proteins and proteasome proteins, including 57 statistically significant BPs, 47 CCs, and 75 MFs (Supplementary Table 15). Those proteasome proteins and their interacted proteins were further clustered into 8 groups according to BPs (Fig. 8E), including endopeptidase regulator activity, transcription initiation from RNA polymerase II promoter, ubiquitin-protein transferase activity, regulation of protein serine/threonine kinase activity, regulation of mitotic sister chromatid separation, regulation of ubiquitin-dependent protein catabolic process, cyclin-dependent protein serine/threonine kinase activity, and anaphase-promoting complex-dependent catabolic process; 11 groups according to CCs (Fig. 8F) including spermatoproteasome complex, PML body, SCF ubiquitin ligase complex, centrosome, cullin-RING ubiquitin ligase complex, P-body, spindle, proteasome complex, proteasome accessory complex, cyclin-dependent protein kinase holoenzyme complex, and chromosomal region; and 13 groups according to MFs (Fig. 8G), including protein phosphatase binding, ubiquitin protein ligase binding, histone kinase activity, regulation of DNA binding, tumor necrosis factor receptor superfamily binding, thiol-dependent ubiquitin-specific protease activity, telomerase activity, ubiquitin protein ligase activity, threonine-type endopeptidase activity, regulation of protein kinase activity, endopeptidase activity, protein serine/threonine kinase activity, and regulation of protein serine/threonine kinase activity.
Discussion
The role of proteasome in cancers
Proteins could keep dynamic balance in the protein synthesis and degradation system. In terms of degradation, the assembly, activity, and abundance of proteasome were essential [11]. The ubiquitin–proteasome system mediated degradation of thousands of half-life of short-lived, damaged, aged, and misfolded proteins, to regulate various cellular processes, including cell cycle, cell survival, apoptosis, cellular metabolism, and protein quality control [29]. The involved proteins contained cancer-related ones, such as transcription factors, oncogenes, tumor suppressor proteins, and signaling molecules [30]. Many previous studies have shown that the levels of proteasome in cancer cells were higher compared to their normal counterparts because of high oxidative stress levels [31]. For example, the total chymotrypsin-like activity of proteasomes in colon cancer patients with metastasis was 1.6-fold higher compared to those in patients without metastasis. The high level of chymotrypsin-like proteasome activity was unfavorable factor in terms of metastasis-free survival [32]. The 20S and 26S proteasome activities were also shown to be significantly higher in tumors of female reproductive system than control tissues. The increasing activities of total proteasome and 20S proteasome were observed as the depth of myometrial invasion in endometrial cancer tissues. Those data clearly demonstrate that proteasome is significantly involved in the process of carcinogenesis [33]. The dysregulated proteasome in human cancer cells played a crucial role in the growth and development of cancer cells. Therefore, the study of proteasome targets for the treatment of various cancer types has been one of the major focuses in the PPPM practice of cancer research. For example, bortezomib, a proteasome inhibitor, was approved for the treatment of multiple myeloma in clinical practice, and various preclinical and clinical models has been studied on lung cancer [34]. A potent proteasome inhibitor, marizomib, showed the strong inhibitory effect on multiple proteasome catalytic activities and induced a better anti-tumor response in triple-negative breast cancer cell lines and patient-derived xenografts alone in breast cancer [35]. Therefore, exploration of the functions and underlying mechanisms of proteasome would contribute more well-identified therapeutic targets for personalized cancer treatment.
The associations between proteasome gene expression and different altered parameters (TMB, CNV, and MSI)
In this study, the data of proteasome genes, including gene expression RNAseq, somatic mutation, TMB, CNV, MSI, immune phenotype, 22 immune cells, cancer stemness index, drug sensitivity, and signaling pathways across 33 cancer types, were systematically analyzed. Some of the obtained results were consistent with the previous studies. (i) In terms of proteasome gene expressions, PSMD9 was analyzed with immunohistochemistry in 102 patients with cervical cancer [36], which found that PSMD9 was overexpressed in tumor tissues compared to the adjacent peritumoral tissues, and was significantly correlated with proliferation. PSMD9 expression correlated significantly with the expression of the proliferation marker MIB-1. Patients with higher PSMD9 expression tended to poor survival rate and more recurrence diseases [36]. ADRM1 was up-regulated in various cancers. The potential prognostic and predictive values of ADRM1 expression have been evaluated on 19 independent breast cancer microarray datasets. The mRNA expression of ADRM1 was significantly associated with tumor size, histologic grade, survival rate, lymph node status, and molecular subtypes (estrogen receptor status and progesterone receptor status) in patients with breast cancer [37]. So many differentially expressed proteasome genes identified in our study were consistent with previously reported literature, and some new changes were also identified, which provided proteasome gene expression profile across 33 cancer types to help further studies. (ii) In terms of somatic mutation of proteasome genes, like the importance of BRCA2 depletion in breast cancer, SEM1 depletion also led to hypersensitivity to DNA damage. It was proved that nearly all BRCA2 in human cell lines was associated with SEM1, which indicated the stability of BRCA2 protein in mammalian cells depended on the presence, deletion, or mutation of SEM1 [38]. PSMB5 Q62P, as a novel mutation form, induced bortezomib resistance in acute myeloid leukemia cells and was associated with the proteasome β5 subunit high expression [39]. The crystal structure of the PSME1 subunit heptamer occurred a mutation site (N146Y) binding with proteasome as tightly as wild-type; however, the mutate PSME1 subunit inhibited proteasome activation and could not activate peptide hydrolysis [40]. Many mutations of proteasome genes influenced the functions and activation of proteasome. Thus, all the information we provided in the study would be meaningful for proteasome. Recent discoveries have observed that patients with the higher number of tumor mutations might have better outcome. The TMB may be a good predictor for cancer therapy, especially for patients treated with immune checkpoint inhibitors [41]. In the present study, the expressions of many proteasome genes were significantly correlated with TMB across different cancer types. Those TMB-related proteasome genes might be useful in the field of predictor for cancer therapy. (iii) In terms of CNV, genetic amplification was also one kind style of identified driver gene among genetic disorder. Copy number gained always proved to be positively related to elevated expression in cancer. PSMB4 amplification elevated expression of PSMB4, which was identified to be the first oncogenic proteasomal subunit that associated with cancer cell survival, tumor growth, and poor prognosis [42]. The association of PSMB9 genetic variability with the metastasis risk of ovarian cancer was investigated in the Chinese population. The results showed that the sequence variants in PSMB9 would increase the risk of the lymph node metastasis and tumor distant metastasis in ovarian cancer [43]. In this study, a lot of CNV-driving proteasome genes were identified. Those would be one of potential mechanisms that result in dysfunction of proteasome. (iv) In terms of MSI, microsatellites were the repeated DNA sequences (one to six base pairs). Microsatellite variation contributes to the individual DNA “fingerprint.” MSI resulted from impaired DNA mismatch repair (MMR), which indicated dysfunction of MMR [28]. In the present study, the expressions of many proteasome genes were significantly correlated with MSI across various cancer types. Those MSI-related proteasome genes might be useful in the field of predictor for cancer therapy.
The associations between proteasome gene and immune
This study also found that proteasome genes were universally associated with immune subtypes and immune-related scores across different cancers. Furthermore, the associations between proteasome gene expressions and immune cells were significant and meaningful. PSMB8 (β5i), PSMB9 (β1i), and PSMB10 (β2i) were important subunits of immunoproteasome and increased in most cancer types. The expressions of immunoproteasome genes were proved to be related to the abundance of tumor infiltrating lymphocytes and protective survival rate [44]. This study found that PSMB8, PSMB9, and PSMB10 were positively related to ESTIMATEScore, ImmuneScore, CD8 T cell, macrophages M1, NK cells activated, and T cells CD4 memory activated, in various cancer types. Those results were consistent with previous studies. For example, a total of 668 breast cancers were retrospectively analyzed to test immunoproteasome subunit PSMB8 (β5i), which showed that high level of PSMB8 had more tumor-infiltrating lymphocytes and had better disease-free survival outcomes [45]. PSMB9 (β1i) performed a critical role in the antigen processing via the major histocompatibility complex-I (MHC-I) complex CD8( +) cytotoxic T lymphocytes (CTL) pathway [46]. Importantly, one study also found that mRNA expression levels of PSMB8 (β5i) and PSMB9 (β1i) were much better predictors of immune response to checkpoint inhibitors than the TMB in melanoma patients [47].
The associations between proteasome gene and stemness
The hypothesis of cancer stem cells (CSC) proposed that CSC was small population but most important contributors in development and propagation of tumor. CSCs contain some essential properties to keep cancer development and maintenance, such as resistance to apoptosis, dormant invasion and metastasis potential, avoidance of immune recognition, evasion from growth suppressors, genome instability, induction of angiogenesis, and destruction and metabolism adjustments [23]. The previous findings suggested that proteasome could mediate stem cell-like phenotype; for example, proteasome β2 (PSMB2) and β5 (PSMB5) subunit activities were down-regulated during epithelial-mesenchymal transition (EMT), and the selective down-regulation could help mammary epithelial cells acquire a cancer stem cell-like phenotype. As proteasome inhibitors become widely studied in cancer treatment, it was suggested that targeting proteasome might be a possible mechanism to solve sluggishness CSCs in treatment of cancer. For example, the overexpression of PSME3 induced the process of EMT and contributed to increase the expression of cancer stem cell markers of the MDA-MB-231 breast cell line, thus enhancing the migration and invasion of cancer cells [48]. The deubiquitinase PSMD14 took part in PSMD14-ALK2-BMP6 signaling pathway axis to contribute to the decreased tumorigenesis of HCT116 colorectal cancer cells and cancer stemness of colorectal cancers [49].
The associations between proteasome gene and drug sensitivity
This study also explored the associations between proteasome gene expressions and drug sensitivity, and some drugs were significantly related to proteasome genes, including drugs hydroxyurea, chelerythrine, asparaginase, pipobroman, uracil mustard, thiotepa, triethylenemelamine, chlorambucil, cyclophosphamide, melphalan, LMP-400, 5-fluoro deoxy uridine 10mer, cladribine, nitrogen mustard, nelarabine, cytarabine, imexon, carmustine, XK-469, idarubicin, bendamustine, triapine, and kahalide f. Some of the drugs have been proven to have contributions in proteasome pathway. For example, hydroxyurea could inhibit protein degradation in purified 20S proteasome lysates in dose-dependent manner. In this process, the induced nitric oxide (NO) in endothelial cells might be mediated by inhibition of the proteasome activity [50]. Recent phase 2 clinical study on the efficacy of combination chemotherapeutic agents l-asparaginase with bortezomib (a proteasome inhibitor) for acute lymphoblastic leukemia demonstrated favorable clinical outcomes. Bortezomib showed only marginal cross-resistance when combined with l-asparaginase. It indicated that the study of association between proteasome gene expressions and drug sensitivity would be applied to guide drug combination [51]. Some emerging new drugs were based on similar mechanisms or pathways; for example, proteasome inhibitors and bendamustine were based on the control of cell cycle and apoptotic pathways. The monotherapy of those agents had been demonstrated to be as safe and effective, but combination strategies were being investigated in clinical trials [52]. The association between the expression of proteasome genes and drug sensitivity might systematically provide some clues for cancer therapy based on proteasome or guidance for drug combination.
The potential mechanisms of proteasome in cancers
To clarify the potential mechanisms of proteasome in cancers, a total of 31 cancer-related activated and inhibited KEGG pathways were analyzed between tumor and control tissues across 33 cancer types; and of them, 9 pathways were inhibited, and 22 pathways were activated. Actually, the functions of proteasome were profoundly influenced in cancer development, and various pathways would be changed according to proteasome and proteasome-interacted genes. For example, there was a certain cooperation and crosstalk between ubiquitin–proteasome system and autophagy-lysosome pathway, and some molecules might act as initiate compensatory effects to prevent cancer progression. Sometimes ubiquitin–proteasome system and autophagy-lysosome pathway worked hand-in-hand to degrade a common substrate. For instance, monomeric and soluble substrates could be degraded by the ubiquitin–proteasome system, whereas their aggregates and insoluble complexes should depend on autophagy to remove [53]. The p53 tumor suppressor protein and its oncoproteins (MDM2 and MDMX) could form MDM2/MDMX-p53 circuitry that had an important function in cancer malignant behaviors, such as angiogenesis, growth and proliferation, cell cycle progression, senescence, apoptosis, and immune response. Recent studies have shown that the stabilities of MDM2/MDMX-p53 circuitry were tightly mediated by the ubiquitin–proteasome system through the degradation of oncoproteins to activate the p53 signaling and induce cell cycle arrest and apoptosis [54]. In this direction, proteasome inhibition received very good results to cause apoptosis in various tumor cell types, including ovarian cancer, leukemia, lung cancer, Hodgkin’s and non-Hodgkin’s, colorectal cancer, gastric cancer, glioblastoma, pancreatic cancer, lymphoma, and prostate cancer [55]. The essential steps for antigen processing for direct presentation on MHC class I molecules involved the concerted activity of several cellular complexes, such as protein synthesis via the ribosome and protein degradation via the proteasome [56]. Most of MHC class I alleles preferred hydrophobic C-terminal residues, which had a better interaction with hydrophobic C-termini that is generated by immunoproteasome complex [57]. The proteasome degradation machinery was also essential for cellular process of T-cell immunity. Proteasome dysfunction induced senescence-associated phenotypes of CD4 + T cells by T-cell receptor signaling via IKK-, MEK-, and calcineurin-dependent pathways. The hallmark of CD4 + T-cell senescence included damaged cytokine production, defective proliferation, and increased biomarker of PD-1+ CD44High CD4 + T cells [58]. The clinical responses of expanded activated autologous lymphocyte treatment depended on the levels of high-affinity-specific T-cell receptors to recognize tumor cells in patients and contribute to CTL-delivered apoptotic death signals. The proteasome inhibitor bortezomib could restore some high-affinity-specific T-cell receptor expression by decreasing phospho-ERK1/2, inhibiting NF-κB activity, and increasing phospho-c-jun-NH(2)-kinase(p-JNK) levels. These findings suggested that proteasome inhibition might have ability to improve cancer-related antigen expression and restore pro-apoptotic pathway [59]. The Wnt, Notch signaling, and TGF-β signaling pathways were essential for the regulation of proliferation, cellular polarity, differentiation, invasion, and migration. These pathways were vulnerable to somatic mutations to initiate cell proliferation and precancerous condition, which ultimately induced the development into cancer in the mutation-accumulation process [60]. Wnt signaling pathway was initially identified for the development of cancers. The expressions of key signaling molecule CTNNB1 (β-catenin) and Wnt ligand-proteins (Wnt1, Wnt2, and Wnt7A) were universally tested in various cancers, such as breast cancer, esophageal cancer, melanoma, ovarian cancer, prostate cancer, colorectal cancer, glioblastoma, and lung cancer [61]. The key proteins in the Wnt signaling pathway, including β-catenin and GSK3, were identified to be regulated by the proteasome under the condition of the endoplasmic reticulum stress using label-free quantitative proteomics [62]. Axin protein contributed to the formation of the β-catenin destruction complex in Wnt/β-catenin signaling pathway. The ubiquitin–proteasome system also proved to have a profound effect on Wnt/β-catenin signaling through regulating stability and cellular concentration of Axin protein [63]. Role of Notch signaling was a driver of some kinds of cancer types, and many notch inhibitors as cancer treatments, which were currently in different phases of clinical trials; for example, MK-0752, one of notch inhibitors, has obtained promising results in an early clinical trial for breast cancer [64]. Notch signaling pathway could be activated by Notch gene mutation itself and inactivated by gene mutations of FBXW7. FBXW7 was one of the most important tumor suppressors in deregulated ubiquitin–proteasome system and controlled proteasome-mediated degradation of oncoproteins, including Notch [65]. The positive and negative of TGF-beta signaling mainly relied on several key components of TGF-beta receptors and ligands. The degradation of those receptors could be mediated by the ubiquitin–proteasome system in a gene-specific and time-dependent way in various cancers. These findings indicated that dysregulated proteasomal degradation would take part in silencing TGF-beta signaling [66]. For example, the TGF-beta family ligands-Smad proteins, as crucial signal transducers, were commonly interacted with various subunits of the 26S proteasome system with different ubiquitin E3 ligases, such as APC complex, HECT family, and SCF; thereby forming an extremely TGF-beta pathway-related complex signaling network to regulate multiple biological activities [67].
In summary, the prevalent genetic and expression alterations of proteasome genes across 11,057 patients with 33 cancer types were presented in this study. The proteasome genes were demonstrated to closely associate with immunity, stemness, and survival of cancers. The activation and inhibition of pathway alterations gave promising clues for further mechanism study underlying proteasome. This systematic landscape of genetic alterations and clinical relevance of proteasome genes laid a basic foundation to explore the dysregulation of cellular biological process. However, more general mechanisms underlying proteasome dysregulation should be further studied, such as epigenetic regulation and post-translational modifications in proteasome self-proteins. This study would also provide great advance to our understanding in the development of proteasome-based combination treatment for various kinds of cancers in the context of PPPM practice.
Conclusions and expert recommendations in the framework of 3P medicine
Proteasome machinery was the major mechanism to degrade proteins and regulate the levels of intracellular proteins and closely associated with different cancers. This study provided the first landscape of proteasome alterations across 11,057 patients with 33 cancer types, with systematic analysis of proteasome genes in these aspects, including differential expressions, somatic mutation, copy number variant, microsatellite instability, clinical characteristics, tumor immunity, cancer stemness, drug sensitivity, and the related pathways. This pan-cancer analysis of proteasome alterations provided the scientific evidence to comprehensively reveal the important roles and mechanisms of proteasome machinery in cancer pathogenesis and its clinically relevant outcomes and systematically reveal the scientific merit of proteasome machinery as drug targets in cancer treatment.
We strongly recommend to strengthen pan-cancer studies of proteasome machinery for discovery of the common and different alterations of proteasome genes among 33 cancer types in the framework of 3P medicine. (i) This study just focused on the analysis of proteasome genes at the levels of DNAs and RNAs, including gene expression RNA data, somatic mutation, tumor mutation burden (TMB), copy number variant (CNV), microsatellite instability (MSI) score, clinical characteristics, immune phenotype, 22 immune cells, cancer stemness index, drug sensitivity, and related pathways. The findings provide the scientific data to systematically in-depth understand the common and specific molecular mechanisms and functional roles of proteasome genes in different types of cancers, which will be helpful for targeted therapeutic and personalized medical services of different types of cancers. (ii) Alternative RNA splicing is an important molecular event and is extensively associated with different disease including cancers. The alternative splicing status of proteasome genes remains unclear among different cancer types. In future, it is necessary to investigate the alternative splicing of proteasome genes across different cancer types to discover alternative splicing-related biomarkers of proteasome genes for personalized medical services of different cancer types. (iii) Proteins, exactly proteoforms, are the final functional performer of genes; also post-translational modifications (PTM) are one of major factors to cause the diversity of proteins—proteoforms. We should integrate proteomics data and PTMomics data to completely understand molecular mechanisms and biological functions of proteasome genes in different types of cancers. PTMs and proteoforms of proteasome will be an important aspect in precise regulation of proteasome functions. (iv) Proteasome machinery-based therapeutic targets and drugs for cancers are a very promising area; especially studies on PTMs and proteoforms of proteasome protein machinery might lead to more precise and reliable biomarkers and new effective therapeutic targets/drugs for PPPM practice in cancers.
Actually, proteasome alterations are involved in the entire healthcare process of a cancer patient, including prediction/prevention, early-stage diagnosis/therapy, late-stage diagnosis/therapy, and prognostic assessment [27, 68]. Proteasome alterations across different cancer types are the promising source to develop effective biomarkers and proteasome-based drugs for individualized predictive diagnosis, targeted prevention, patient stratification, targeted therapy, and individualized prognostic diagnosis for healthy individuals and pre-cancer and cancer patients in the framework of PPPM/3P medicine [27, 68].
Data accessibility
All data and materials were provided in this manuscript and supplementary materials.
Abbreviations
- ACC:
-
Adrenocortical carcinoma
- ADRM1:
-
Proteasome 26S subunit, non-ATPase 13
- BLCA:
-
Bladder urothelial carcinoma
- BP:
-
Biological process
- BRCA:
-
Breast cancer
- CC:
-
Cellular component
- CDKs:
-
Cyclin-dependent kinases
- CESC:
-
Cervical squamous cell carcinoma and endocervical adenocarcinoma
- CHOL:
-
Cholangiocarcinoma
- CNV:
-
Copy number variant
- COAD:
-
Colon adenocarcinoma
- DEGs:
-
Differentially expressed genes
- DLBC:
-
Lymphoid neoplasm diffuse large b-cell lymphoma
- DTP:
-
Developmental therapeutics program
- ESCA:
-
Esophageal carcinoma
- GBM:
-
Glioblastoma multiforme
- GO:
-
Gene Ontology
- GSVA:
-
Gene set variation analysis
- HNSC:
-
Head and neck squamous carcinoma
- HR:
-
Hazard ratio
- KEGG:
-
Kyoto Encyclopedia of Genes and Genomes
- KICH:
-
Kidney chromophobe
- KIRC:
-
Kidney renal clear cell carcinoma
- KIRP:
-
Kidney renal papillary cell carcinoma
- LAML:
-
Acute myeloid leukemia
- LGG:
-
Brain lower grade glioma
- LIHC:
-
Liver hepatocellular carcinoma
- LUAD:
-
Lung adenocarcinoma
- LUSC:
-
Lung squamous cell carcinoma
- MESO:
-
Mesothelioma
- MF:
-
Molecular function
- MHC:
-
Major histocompatibility complex class I
- MMR:
-
DNA mismatch repair
- mRNA:
-
Messenger RNA
- MSI:
-
Microsatellite instability
- OV:
-
Ovarian serous cystadenocarcinoma
- PAAD:
-
Pancreatic adenocarcinoma
- PCPG:
-
Pheochromocytoma and paraganglioma
- PRAD:
-
Prostate adenocarcinoma
- PSMA1:
-
Proteasome 20S subunit alpha 1
- PSMA2:
-
Proteasome 20S subunit alpha 2
- PSMA3:
-
Proteasome 20S subunit alpha 3
- PSMA4:
-
Proteasome 20S subunit alpha 4
- PSMA5:
-
Proteasome 20S subunit alpha 5
- PSMA6:
-
Proteasome 20S subunit alpha 6
- PSMA7:
-
Proteasome 20S subunit alpha 7
- PSMB1:
-
Proteasome 20S subunit beta 1
- PSMB10:
-
Proteasome 20S subunit beta 10
- PSMB11:
-
Proteasome subunit beta 11
- PSMB2:
-
Proteasome 20S subunit beta 2
- PSMB3:
-
Proteasome 20S subunit beta 3
- PSMB4:
-
Proteasome 20S subunit beta 4
- PSMB5:
-
Proteasome 20S subunit beta 5
- PSMB6:
-
Proteasome 20S subunit beta 6
- PSMB7:
-
Proteasome 20S subunit beta 7
- PSMB8:
-
Proteasome 20S subunit beta 8
- PSMB9:
-
Proteasome 20S subunit beta 9
- PSMC1:
-
Proteasome 26S subunit, ATPase 1
- PSMC2:
-
Proteasome 26S subunit, ATPase 2
- PSMC3:
-
Proteasome 26S subunit, ATPase 3
- PSMC4:
-
Proteasome 26S subunit, ATPase 4
- PSMC5:
-
Proteasome 26S subunit, ATPase 5
- PSMC6:
-
Proteasome 26S subunit, ATPase 6
- PSMD1:
-
Proteasome 26S subunit, non-ATPase 1
- PSMD11:
-
Proteasome 26S subunit, non-ATPase 11
- PSMD12:
-
Proteasome 26S subunit, non-ATPase 12
- PSMD13:
-
Proteasome 26S subunit, non-ATPase 13
- PSMD14:
-
Proteasome 26S subunit, non-ATPase 14
- PSMD2:
-
Proteasome 26S subunit, non-ATPase 2
- PSMD3:
-
Proteasome 26S subunit, non-ATPase 3
- PSMD4:
-
Proteasome 26S subunit, non-ATPase 4
- PSMD6:
-
Proteasome 26S subunit, non-ATPase 6
- PSMD7:
-
Proteasome 26S subunit, non-ATPase 7
- PSMD8:
-
Proteasome 26S subunit, non-ATPase 8
- PSMD9:
-
Proteasome 26S subunit, non-ATPase 9
- PSME1:
-
Proteasome activator subunit 1
- PSME2:
-
Proteasome activator subunit 2
- PSME3:
-
Proteasome activator subunit 3
- PSME4:
-
Proteasome activator subunit 4
- READ:
-
Rectum adenocarcinoma
- RNAss:
-
RNA expression-based stemness scores
- SARC:
-
Sarcoma
- SEM1:
-
SEM1 26S proteasome complex subunit
- SKCM:
-
Skin cutaneous melanoma
- STAD:
-
Stomach adenocarcinoma
- TCGA:
-
The Cancer Genome Atlas
- TGCT:
-
Testicular germ cell tumors
- THCA:
-
Thyroid carcinoma
- THYM:
-
Thymoma
- TMB:
-
Tumor mutation burden
- TME:
-
Tumor microenvironment
- UCEC:
-
Uterine corpus endometrial carcinoma
- UCS:
-
Uterine carcinosarcoma
- UVM:
-
Uveal melanoma
References
Spits M, Janssen LJ, Voortman LM, Kooij R, Neefjes ACM, Ovaa H, et al. Homeostasis of soluble proteins and the proteasome post nuclear envelope reformation in mitosis. J Cell Sci. 2019; 132. https://doi.org/10.1242/jcs.225524.
Limanaqi F, Biagioni F, Gambardella S, Familiari P, Frati A, Fornai F. Promiscuous roles of autophagy and proteasome in neurodegenerative proteinopathies. Int J Mol Sci. 2020; 21. https://doi.org/10.3390/ijms21083028.
Bard JAM, Goodall EA, Greene ER, Jonsson E, Dong KC, Martin A. Structure and function of the 26S proteasome. Annu Rev Biochem. 2018;87:697–724. https://doi.org/10.1146/annurev-biochem-062917-011931.
Gierisch ME, Giovannucci TA, Dantuma NP. Reporter-based screens for the ubiquitin/proteasome system. Front Chem. 2020;8:64. https://doi.org/10.3389/fchem.2020.00064.
Budenholzer L, Cheng CL, Li Y, Hochstrasser M. Proteasome structure and assembly. J Mol Biol. 2017;429:3500–24. https://doi.org/10.1016/j.jmb.2017.05.027.
Coux O, Zieba BA, Meiners S. The proteasome system in health and disease. Adv Exp Med Biol. 2020;1233:55–100. https://doi.org/10.1007/978-3-030-38266-7_3.
Harrigan JA, Jacq X, Martin NM, Jackson SP. Deubiquitylating enzymes and drug discovery: emerging opportunities. Nat Rev Drug Discov. 2018;17:57–78. https://doi.org/10.1038/nrd.2017.152.
Groll M, Huber R. Purification, crystallization, and X-ray analysis of the yeast 20S proteasome. Methods Enzymol. 2005;398:329–36. https://doi.org/10.1016/s0076-6879(05)98027-0.
Zhang S,Mao Y. AAA+ ATPases in protein degradation: structures, functions and mechanisms. Biomolecules. 2020; 10. https://doi.org/10.3390/biom10040629.
Thibaudeau TA, Smith DM. A practical review of proteasome pharmacology. Pharmacol Rev. 2019;71:170–97. https://doi.org/10.1124/pr.117.015370.
Rousseau A, Bertolotti A. Regulation of proteasome assembly and activity in health and disease. Nat Rev Mol Cell Biol. 2018;19:697–712. https://doi.org/10.1038/s41580-018-0040-z.
Sharma A, Trivedi AK. Regulation of apoptosis by E3 ubiquitin ligases in ubiquitin proteasome system. Cell Biol Int. 2020;44:721–34. https://doi.org/10.1002/cbin.11277.
Neutzner A, Li S, Xu S, Karbowski M. The ubiquitin/proteasome system-dependent control of mitochondrial steps in apoptosis. Semin Cell Dev Biol. 2012;23:499–508. https://doi.org/10.1016/j.semcdb.2012.03.019.
Wójcik C, DeMartino GN. Intracellular localization of proteasomes. Int J Biochem Cell Biol. 2003;35:579–89. https://doi.org/10.1016/s1357-2725(02)00380-1.
Frezza M, Schmitt S, Dou QP. Targeting the ubiquitin-proteasome pathway: an emerging concept in cancer therapy. Curr Top Med Chem. 2011;11:2888–905. https://doi.org/10.2174/156802611798281311.
Drexler HC. The role of p27Kip1 in proteasome inhibitor induced apoptosis. Cell Cycle. 2003;2:438–41.
Bonet-Costa V, Pomatto LC, Davies KJ. The proteasome and oxidative stress in Alzheimer’s disease. Antioxid Redox Signal. 2016;25:886–901. https://doi.org/10.1089/ars.2016.6802.
Davies MJ. Protein oxidation and peroxidation. Biochem J. 2016;473:805–25. https://doi.org/10.1042/bj20151227.
Kammerl IE, Meiners S. Proteasome function shapes innate and adaptive immune responses. Am J Physiol Lung Cell Mol Physiol. 2016;311:L328–36. https://doi.org/10.1152/ajplung.00156.2016.
Kloetzel PM, Ossendorp F. Proteasome and peptidase function in MHC-class-I-mediated antigen presentation. Curr Opin Immunol. 2004;16:76–81. https://doi.org/10.1016/j.coi.2003.11.004.
Murata S, Takahama Y, Kasahara M, Tanaka K. The immunoproteasome and thymoproteasome: functions, evolution and human disease. Nat Immunol. 2018;19:923–31. https://doi.org/10.1038/s41590-018-0186-z.
Dragnev KH, Freemantle SJ, Spinella MJ, Dmitrovsky E. Cyclin proteolysis as a retinoid cancer prevention mechanism. Ann N Y Acad Sci. 2001;952:13–22. https://doi.org/10.1111/j.1749-6632.2001.tb02724.x.
Voutsadakis IA. Proteasome expression and activity in cancer and cancer stem cells. Tumour Biol. 2017;39:1010428317692248. https://doi.org/10.1177/1010428317692248.
Lu M, Zhan X. The crucial role of multiomic approach in cancer research and clinically relevant outcomes. EPMA J. 2018;9:77–102. https://doi.org/10.1007/s13167-018-0128-8.
Berryman K, Buhimschi CS, Zhao G, Axe M, Locke M, Buhimschi IA. Proteasome levels and activity in pregnancies complicated by severe preeclampsia and hemolysis, elevated liver enzymes, and thrombocytopenia (HELLP) syndrome. Hypertension. 2019;73:1308–18. https://doi.org/10.1161/hypertensionaha.118.12437.
Cheng T, Zhan X. Pattern recognition for predictive, preventive, and personalized medicine in cancer. EPMA J. 2017;8:51–60. https://doi.org/10.1007/s13167-017-0083-9.
Hu R, Wang X, Zhan X. Multi-parameter systematic strategies for predictive, preventive and personalised medicine in cancer. EPMA J. 2013;4:2. https://doi.org/10.1186/1878-5085-4-2.
Yamamoto H, Imai K. Microsatellite instability: an update. Arch Toxicol. 2015;89:899–921. https://doi.org/10.1007/s00204-015-1474-0.
Mofers A, Pellegrini P, Linder S, D’Arcy P. Proteasome-associated deubiquitinases and cancer. Cancer Metastasis Rev. 2017;36:635–53. https://doi.org/10.1007/s10555-017-9697-6.
Catalgol B. Proteasome and cancer. Prog Mol Biol Transl Sci. 2012;109:277–93. https://doi.org/10.1016/b978-0-12-397863-9.00008-0.
Chen Y, Zhang Y, Guo X. Proteasome dysregulation in human cancer: implications for clinical therapies. Cancer Metastasis Rev. 2017;36:703–16. https://doi.org/10.1007/s10555-017-9704-y.
Ivanova EV, Cheremisina OV, Afanasiev SG, Kondakova IV. Proteasome and calpain activities in colon cancer: the relation with metastasis and prognosis. Vopr Onkol. 2016;62:794–800.
Kondakova IV, Spirina LV, Shashova EE, Koval VD, Kolomiets LA, Chernysheva AL, et al. Proteasome activity in tumors of female reproductive system. Bioorg Khim. 2012;38:106–10. https://doi.org/10.1134/s106816201201013x.
Rohondia SO, Ahmed ZSO, Dou QP. Updated review and perspective on 20S proteasome inhibitors in the treatment of lung cancer. Curr Cancer Drug Targets. 2020;20:392–409. https://doi.org/10.2174/1568009620666200226094000.
Raninga PV, Lee A, Sinha D, Dong LF, Datta KK, Lu X, et al. Marizomib suppresses triple-negative breast cancer via proteasome and oxidative phosphorylation inhibition. Theranostics. 2020;10:5259–75. https://doi.org/10.7150/thno.42705.
Köster F, Sauer L, Hoellen F, Ribbat-Idel J, Bräutigam K, Rody A, et al. PSMD9 expression correlates with recurrence after radiotherapy in patients with cervical cancer. Oncol Lett. 2020;20:581–8. https://doi.org/10.3892/ol.2020.11622.
Wu W, Zhong J, Chen J, Niu P, Ding Y, Han S, et al. Prognostic and therapeutic significance of adhesion-regulating molecule 1 in estrogen receptor-positive breast cancer. Clin Breast Cancer. 2020;20:131-144.e3. https://doi.org/10.1016/j.clbc.2019.07.009.
Li J, Zou C, Bai Y, Wazer DE, Band V, Gao Q. DSS1 is required for the stability of BRCA2. Oncogene. 2006;25:1186–94. https://doi.org/10.1038/sj.onc.1209153.
Bista R, Lee DW, Pepper OB, Azorsa DO, Arceci RJ, Aleem E. Disulfiram overcomes bortezomib and cytarabine resistance in Down-syndrome-associated acute myeloid leukemia cells. J Exp Clin Cancer Res. 2017;36:22. https://doi.org/10.1186/s13046-017-0493-5.
Zhang Z, Clawson A, Realini C, Jensen CC, Knowlton JR, Hill CP, et al. Identification of an activation region in the proteasome activator REGalpha. Proc Natl Acad Sci U S A. 1998;95:2807–11. https://doi.org/10.1073/pnas.95.6.2807.
Tafe LJ. Non-small cell lung cancer as a precision oncology paradigm: emerging targets and tumor mutational burden (TMB). Adv Anat Pathol. 2020;27:3–10. https://doi.org/10.1097/pap.0000000000000244.
Lee GY, Haverty PM, Li L, Kljavin NM, Bourgon R, Lee J, et al. Comparative oncogenomics identifies PSMB4 and SHMT2 as potential cancer driver genes. Cancer Res. 2014;74:3114–26. https://doi.org/10.1158/0008-5472.Can-13-2683.
Song L, Ma N, Han L, Yan H, Yan B, Yuan Z, et al. Association between LMP2/LMP7 genetic variability and the metastasis risk of ovarian cancer in Chinese women in Beijing. Hum Immunol. 2014;75:239–44. https://doi.org/10.1016/j.humimm.2013.12.006.
Rouette A, Trofimov A, Haberl D, Boucher G, Lavallée VP, D’Angelo G, et al. Expression of immunoproteasome genes is regulated by cell-intrinsic and -extrinsic factors in human cancers. Sci Rep. 2016;6:34019. https://doi.org/10.1038/srep34019.
Lee M, Song IH, Heo SH, Kim YA, Park IA, Bang WS, et al. Expression of immunoproteasome subunit LMP7 in breast cancer and its association with immune-related markers. Cancer Res Treat. 2019;51:80–9. https://doi.org/10.4143/crt.2017.500.
Li C, Dai S, Yan Z, Zhang X, Liu S, Wang X, et al. Genetic polymorphisms of proteasome subunit genes of the MHC-I antigen-presenting system are associated with cervical cancer in a Chinese Han population. Hum Immunol. 2020. https://doi.org/10.1016/j.humimm.2020.07.002.
Kalaora S, Lee JS, Barnea E, Levy R, Greenberg P, Alon M, et al. Immunoproteasome expression is associated with better prognosis and response to checkpoint therapies in melanoma. Nat Commun. 2020;11:896. https://doi.org/10.1038/s41467-020-14639-9.
Yi Z, Yang D, Liao X, Guo F, Wang Y, Wang X. PSME3 induces epithelial-mesenchymal transition with inducing the expression of CSC markers and immunosuppression in breast cancer. Exp Cell Res. 2017;358:87–93. https://doi.org/10.1016/j.yexcr.2017.05.017.
Seo D, Jung SM, Park JS, Lee J, Ha J, Kim M, et al. The deubiquitinating enzyme PSMD14 facilitates tumor growth and chemoresistance through stabilizing the ALK2 receptor in the initiation of BMP6 signaling pathway. EBioMedicine. 2019;49:55–71. https://doi.org/10.1016/j.ebiom.2019.10.039.
Cokic VP, Beleslin-Cokic BB, Noguchi CT, Schechter AN. Hydroxyurea increases eNOS protein levels through inhibition of proteasome activity. Nitric Oxide. 2007;16:371–8. https://doi.org/10.1016/j.niox.2007.01.001.
Takahashi K, Inukai T, Imamura T, Yano M, Tomoyasu C, Lucas DM, et al. Anti-leukemic activity of bortezomib and carfilzomib on B-cell precursor ALL cell lines. PLoS ONE. 2017;12: e0188680. https://doi.org/10.1371/journal.pone.0188680.
Ogura M. Current treatment strategy in mantle cell lymphoma. Nihon Rinsho. 2014;72:499–511.
Ji CH, Kwon YT. Crosstalk and interplay between the ubiquitin-proteasome system and autophagy. Mol Cells. 2017;40:441–9. https://doi.org/10.14348/molcells.2017.0115.
Qi SM, Cheng G, Cheng XD, Xu Z, Xu B, Zhang WD, et al. Targeting USP7-mediated deubiquitination of MDM2/MDMX-p53 pathway for cancer therapy: are we there yet? Front Cell Dev Biol. 2020;8:233. https://doi.org/10.3389/fcell.2020.00233.
Maliński M, Cichocki M. Proteasome inhibition as a new strategy in cancer therapy and chemoprevention. Postepy Hig Med Dosw (Online). 2013;67:90–106. https://doi.org/10.5604/17322693.1035963.
Bitzer A, Basler M, Groettrup M. Chaperone BAG6 is dispensable for MHC class I antigen processing and presentation. Mol Immunol. 2016;69:99–105. https://doi.org/10.1016/j.molimm.2015.11.004.
Cascio P, Hilton C, Kisselev AF, Rock KL, Goldberg AL. 26S proteasomes and immunoproteasomes produce mainly N-extended versions of an antigenic peptide. EMBO J. 2001;20:2357–66. https://doi.org/10.1093/emboj/20.10.2357.
Arata Y, Watanabe A, Motosugi R, Murakami R, Goto T, Hori S, et al. Defective induction of the proteasome associated with T-cell receptor signaling underlies T-cell senescence. Genes Cells. 2019;24:801–13. https://doi.org/10.1111/gtc.12728.
Jazirehi AR, Economou JS. Proteasome inhibition blocks NF-κB and ERK1/2 pathways, restores antigen expression, and sensitizes resistant human melanoma to TCR-engineered CTLs. Mol Cancer Ther. 2012;11:1332–41. https://doi.org/10.1158/1535-7163.Mct-11-0814.
Baloghova N, Lidak T, Cermak L. Ubiquitin ligases involved in the regulation of Wnt, TGF-β, and Notch signaling pathways and their roles in mouse development and homeostasis. Genes (Basel). 2019; 10. https://doi.org/10.3390/genes10100815.
Anastas JN, Moon RT. WNT signalling pathways as therapeutic targets in cancer. Nat Rev Cancer. 2013;13:11–26. https://doi.org/10.1038/nrc3419.
Fabre B, Livneh I, Ziv T, Ciechanover A. Identification of proteins regulated by the proteasome following induction of endoplasmic reticulum stress. Biochem Biophys Res Commun. 2019;517:188–92. https://doi.org/10.1016/j.bbrc.2019.07.040.
Ji L, Lu B, Zamponi R, Charlat O, Aversa R, Yang Z, et al. USP7 inhibits Wnt/β-catenin signaling through promoting stabilization of Axin. Nat Commun. 2019;10:4184. https://doi.org/10.1038/s41467-019-12143-3.
Espinoza I, Miele L. Notch inhibitors for cancer treatment. Pharmacol Ther. 2013;139:95–110. https://doi.org/10.1016/j.pharmthera.2013.02.003.
Yeh CH, Bellon M, Nicot C. FBXW7: a critical tumor suppressor of human cancers. Mol Cancer. 2018;17:115. https://doi.org/10.1186/s12943-018-0857-2.
Zhang F, Laiho M. On and off: proteasome and TGF-beta signaling. Exp Cell Res. 2003;291:275–81. https://doi.org/10.1016/j.yexcr.2003.07.007.
Wang T. The 26S proteasome system in the signaling pathways of TGF-beta superfamily. Front Biosci. 2003;8:d1109–27. https://doi.org/10.2741/1057.
Golubnitschaja O, Liskova A, Koklesova L, Samec M, Biringer K, Büsselberg D, Podbielska H, Kunin AA, Evsevyeva ME, Shapira N, Paul F, Erb C, Dietrich DE, Felbel D, Karabatsiakis A, Bubnov R, Polivka J, Polivka J Jr, Birkenbihl C, Fröhlich H, Hofmann-Apitius M, Kubatka P. Caution, “normal” BMI: health risks associated with potentially masked individual underweight—EPMA Position Paper 2021. EPMA J. 2021;17:1–22. https://doi.org/10.1007/s13167-021-00251-4.
Acknowledgements
We would like to thank The Cancer Genome Atlas (TCGA) project organizers as well as all study participants for providing the publically available TCGA RNA-seq data and clinical data.
Funding
This work was supported by the Shandong First Medical University Talent Introduction Funds (to X.Z.), the Hunan Provincial Hundred Talent Plan (to X.Z.), the National Natural Science Foundation of China (82172866), and the Academic Promotion Program of Shandong First Medical University (2019ZL002).
Author information
Authors and Affiliations
Contributions
N.L. designed, analyzed data, prepared figures and tables, and wrote the manuscript. X.Z. conceived the concept, supervised results, designed, wrote and critically revised manuscript, and was responsible for its financial supports and the corresponding works. All authors approved the final manuscript.
Corresponding author
Ethics declarations
Ethical approval
Not applicable.
Consent publication
Not applicable.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Li, N., Zhan, X. Integrated genomic analysis of proteasome alterations across 11,057 patients with 33 cancer types: clinically relevant outcomes in framework of 3P medicine. EPMA Journal 12, 605–627 (2021). https://doi.org/10.1007/s13167-021-00256-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13167-021-00256-z