
Abstract
Purpose
We compared the feasibility of quantitative analysis methods using bone SPECT/CT with those using planar bone scans to assess active sacroiliitis.
Methods
We retrospectively reviewed whole-body bone scans and pelvic bone SPECT/CTs of 8 patients who had clinically confirmed sacroiliitis and enrolled 24 patients without sacroiliitis as references. The volume of interest of each sacroiliac joint, including both the ilium and sacrum, was drawn. Active arthritis zone (AAZ) was defined as the zone of voxels with higher SUV than sacral mean SUV within the VOI of SI joint. Then, the following SPECT/CT quantitative parameters, SUVmax (maximum SUV), SUV50% (mean SUV in highest 50% of SUV), and SUV-AAZ, and the ratio of those values to sacral mean SUV (SUVmax/S, SUV50%/S, SUV-AAZ/S) were calculated. For the planar bone scan, the mean count ratio of SI joint/sacrum (SI/S) was conventionally measured.
Results
Most of the SPECT/CT parameters of the sacroiliitis group were significantly higher than the normal group, whereas SI/S of the planar bone scan was not significantly different between the two groups. In receiver operating characteristic curve analysis, SUV-AAZ/S showed the highest AUC of 0.992, followed by SUV50%/S and SUVmax/S. All ratio parameters of the SPECT/CT showed higher AUC values than the SUV parameters of SI joint or SI/S of the planar scan.
Conclusions
The quantitative analyses of bone SPECT/CT showed better performance in assessing active sacroiliitis than the planar bone scan. SPECT/CT parameters using the ratio of the SI joint to sacrum showed more favorable results than SUV parameters such as SUVmax, SUV50%, and SUV-AAZ.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Axial spondyloarthritis (axial SpA) is an inflammatory arthritis primarily affecting the axial skeleton. Patients with axial SpA show a diverse spectrum of diseases, with the most common initial presentation being inflammatory back pain [1]. Axial SpA shows characteristic involvement of the spine and sacroiliac (SI) joints and is comprised of patients with radiographic sacroiliitis (ankylosing spondylitis or radiographic axial SpA) and without radiographic sacroiliitis (non-radiographic axial SpA) [2]. Thus, imaging confirmation of sacroiliitis plays an important role in the diagnosis and classification of patients with axial SpA [3].
Currently, the most utilized imaging tools for SI joint assessment in patients with sacroiliitis are simple radiography and magnetic resonance imaging (MRI). Although both modalities are included in the Assessment of Spondyloarthritis International Society (ASAS) axial SpA criteria, they show a limited evaluation of sacroiliitis. Simple radiography is used as the first-line imaging tool; however, it is not specific or sensitive enough, especially in patients with early sacroiliitis, because structural bone destruction takes up to 7 to 10 years to develop. Compared to a simple radiograph, MRI can show active inflammation before structural changes develop. However, even the sensitivity of MRI for such lesion detection is, at best, only up to 70% [4].
Bone scintigraphy has been used to detect acute sacroiliitis for decades. However, only a few studies have investigated the potential of radionuclide methods for diagnosing sacroiliitis [5]. Bone scintigraphy shows increased radionuclide uptake in the areas of accelerated bone turnover rate and inflammation. Using the intensity of radionuclide uptake in the SI joint and its ratio with adjacent background structure, usually the sacrum, allows quantitative evaluation of sacroiliitis. However, due to the complex anatomy of the SI joint, it shows low sensitivity and specificity [5]. Single-photon emission computed tomography (SPECT) combined with computed tomography (CT) provides additional information for the characterization of equivocal lesions and anatomic variations in SI joints. Moreover, with recent technical advances, CT-based attenuation correction of SPECT provides quantitative information on bone turnover, such as the standardized uptake value (SUV) in positron emission tomography [6].
However, so far, the studies for diagnosing sacroiliitis using quantitative evaluation of bone SPECT/CT are limited, and among the various available quantitative parameters, the most useful parameter for diagnosis and evaluation of inflammatory activity is unknown. Therefore, for the clinical application of quantitative bone SPECT/CT in the diagnosis of active sacroiliitis, we performed this preliminary study to explore the best quantitative parameter of bone SPECT/CT for diagnosing active sacroiliitis and evaluate its feasibility in comparison with the parameters using conventional planar bone scan.
Materials and Methods
Subjects
We retrospectively reviewed the medical records of adult patients who underwent bone scintigraphy and pelvis SPECT/CT from March 2018 to January 2019. Among these patients, we enrolled 8 patients with sacroiliitis using the following inclusion criteria: (1) clinically diagnosed sacroiliitis according to the ASAS axial spondyloarthropathy criteria based on simple radiography, MRI, blood test, and clinical symptoms and (2) age 18–50 years. Exclusion criteria were as follows: (1) radiological findings of osteitis condensans ilii or degenerative arthritis, (2) history or radiological findings of fracture, tumor, or osteomyelitis of pelvic bones; (3) hematologic malignancy or malignant tumor, (4) severe acute or chronic renal disease, (5) severe acute or chronic liver disease, (6) heart failure, and (7) metabolic bone disease. As an age-matched normal reference group between 18 and 50 years, we enrolled 12 female and 12 male patients who had an extremely low possibility of pathologic conditions in pelvic bones, including the SI joint, based on simple radiographic findings of the SI joint with a normal range of blood test, clinical history, and symptoms. This study was approved by the Institutional Review Board (IRB No. 2021–0113), and the need for informed consent was waived.
Bone Scintigraphy and Bone SPECT/CT Acquisition
Bone scintigraphy and SPECT/CT images of the pelvis were obtained at 3–4 h (mean 215 min) after intravenous injection of approximately 740 MBq (20 mCi) 99mTc-hydroxy-diphosphonate or 99mTc-diphosphono-1,2-propanodicarboxylic acid using the hybrid SPECT/CT scanner (Symbia Intevo16®, Siemens, Erlangen, Germany). For quantitative analysis of SPECT images, accurate injected doses were measured after cross-calibration between the dose calibrator and scanner system. After obtaining the anterior and posterior planar whole-body bone scan images, bone SPECT/CT images covering L-pine and pelvis were obtained.
For SPECT, using a dual-head gamma camera equipped with low-energy, high-resolution parallel-hole collimators, the images were acquired using a step-and-shoot mode with a non-circular orbit using the following acquisition parameters: 15% energy window centered at 140 keV, 22 s per projection, and 90 projections over 360°. The CT images were acquired for the same field of view as the SPECT using the helical mode at 110 kVp and 40 reference mAs using adaptative dose modulation (CARE Dose 4D) with 2 mm slice thickness and a 512 × 512 matrix, pitch 1.5, and 0.8-s rotation time to correct attenuation and image fusion. After attenuation correction with CT, images were reconstructed to generate attenuation-corrected SPECT data using the xSPECT-Bone™ (Siemens, Erlangen, Germany) reconstruction algorithm (1 subset, 24 iterations), allowing quantification on post-processed images with a 256 × 256 matrix size.
Quantitative Analysis of Sacroiliac Joints
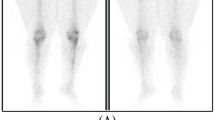
We performed the quantitative analyses of SI joints on both planar and SPECT images using in-house software (Asan J & AMC NM Toolkit for Image Quantification of Excellence (ANTIQUE)) [7]. For the planar bone scan, 2-dimensional regions of interest (ROIs) were drawn on each SI joint and the sacrum on the posterior planar image. The average counts of ROI were used to calculate the SI joint to sacrum uptake ratio (SI/S) in the conventional manner (Fig. 1). For bone SPECT/CT images, the volume of interest (VOI) of each SI joint was defined, including a 6 mm width of ilium and sacrum from the central line of each SI joint space along the entire joint on CT images. This was done by drawing the central line of each SI joint space on every three axial 2-dimensional slice covering the entire SI joint, which was then reconstructed as a 3-dimensional VOI (Fig. 2a–b) using the AMC-SPECT module of AsanJ (version 20,191,115, written by BP and WHS) that is developed on top of Java-based image processing libraries termed ImageJ (ver. 20,141,126 running on Java 1.8.0_112 (64-bit); URL = https://imagej.nih.gov/ij/). Visualization of SPECT/CT image and VOI fusion and all standardized uptake value (SUV) quantifications were conducted using ANTIQUE software running on Interactive Data Language (ver 8.7, Harris Geospatial, Boulder, CO). SUV for each voxel was calculated as follows: SUV [g/mL] = voxel-wise decay corrected radioactivity concentration measured by SPECT [Bq/mL] / injected radioactivity [Bq] × body weight [g], where brackets contain SI units. A spherical VOI with a diameter of 1.6 cm was drawn at the center of the sacral body (Fig. 2c) as the reference uptake to normalize the uptake values of the aforementioned SI joint VOIs. Using these VOIs, the active arthritis zone (AAZ) was defined as the “zone of voxels with higher SUV than sacral mean SUV within the VOI of the SI joints” (Fig. 2d). Then, the following quantitative SPECT/CT parameters were measured: SUVmax (maximum SUV), SUV50% (mean SUV in highest 50% of SUV), and SUV-AAZ (mean SUV of AAZ) of the SI joints and the ratio of those values to sacral mean SUV (SUVmax/S, SUV50%/S, SUV-AAZ/S).

The representative images of bone scan for quantitative analysis of SI joint activity. The regions of interest are drawn on both SI joints and the sacrum of the posterior planar bone scan image

The representative images of bone SPECT/CT images for quantitative analysis of SI joint activity. The volume of interest, which includes a 6 mm width of ilium and sacrum from the central line of each SI joint space along the entire joint, is shown on trans-axial and coronal SPECT/CT images (a, b). A sphere VOI with a diameter of 1.6 cm in the center of the S1 vertebral body is shown in the sagittal image (c). Active arthritis zone (AAZ) is defined as a “zone of voxels with higher SUV than sacral mean SUV within the VOIs of SI joints” (d)
Statistical Analysis
Demographic data (ESR, CRP) were expressed in median (range), and other continuous variables were expressed as mean ± standard deviation (SD). Normality of the continuous variables was verified, and the data were analyzed with student t test or one-way analysis of variance (ANOVA) with a post hoc Dunn’s test. Receiver operating characteristic (ROC) curve analysis was performed to compare the diagnostic performance of quantitative parameters using planar bone scan and SPECT/CT. DeLong’s method was used for comparing AUC values and their 95% confidence interval (CI). The optimal cut-off values were the exploratory cut-off values with the highest accuracy. P values ≤ 0.05 were considered statistically significant. All statistical analyses were performed using SPSS software version 17 (SPSS, Chicago, IL) and MedCalc version 19.2.3 (MedCalc Software Ltd, Ostend, Belgium).
Results
The sacroiliitis group consisted of 8 patients (2 men and 6 women) with a mean age of 34.7 ± 10.8 years. The normal reference group consisted of 12 men and 12 women with a mean age of 36.2 ± 8.7 years. Demographic data of the study subjects are summarized in Table 1. All SI joints of the normal reference and sacroiliitis groups were analyzed, except one SI joint of a patient with a normal appearance in the MR image and a unilateral joint symptom in the contralateral SI joint. Therefore, fifteen joints in the sacroiliitis group and forty-eight joints in the normal reference group were analyzed.
Most of the SPECT/CT parameters of the sacroiliitis group were significantly higher than that of the normal group, whereas SI/S of the planar bone scan was not significantly different between the two groups (1.21 ± 0.18 vs. 1.12 ± 0.15, p = 0.5) (Fig. 3 and Table 2). In ROC curve analysis, SUV-AAZ/S showed the highest area under the curve (AUC) value of 0.992 among all quantitative parameters, followed by SUV50%/S and SUVmax/S (AUC, 0.979 and 0.978, respectively). However, SUV-AAZ/S did not show a significant difference when compared with SUV50%/S and SUVmax/S in the ROC comparison test. SUV-AAZ/S, as a diagnostic parameter for sacroiliitis, showed a sensitivity of 100% and specificity of 95.8%, with a cut-off of 1.17; the diagnostic performances of the other parameters are shown in Table 3. All ratio parameters of the SPECT/CT showed higher AUC values than the SUV parameters (SUVmax, 0.825; SUV50%, 0.771; SUV-AAZ, 0.686) or SI/S (0.650) of the planar scan (Fig. 4). The images and quantitative analysis results of a representative case are shown in Fig. 5.

Comparisons of quantitative parameters measured on planar and SPECT/CT images in normal and sacroiliitis groups. All SPECT/CT ratio parameters in the sacroiliitis group are significantly higher than those in the normal group, but planar bone scan parameters show no significant difference between the two groups (a). All SUV parameters measured on SPECT/CT also show significantly higher values in the sacroiliitis group (b)

Receiver operating characteristic curve analysis for SPECT/CT quantitative parameters. All the SPECT/CT ratio parameters show a larger AUC than SUV parameters, and SUV-AAZ/S shows the largest AUC of 0.992

Representative images and quantitative analysis of a 32-year-old woman with bilateral sacroiliitis. Pelvis plain radiograph (a) shows small localized areas with erosion or sclerosis, with no alteration in the joint width (New York grade II) in bilateral SI joints. Coronal T2 fat suppression MRI image (b) shows a signal change in the iliac side of bilateral SI joints with a more severe change on the right side. Planar bone scan image and SI/S ratio analysis (c) show increased uptake in bilateral SI joints. SPECT/CT image (d) and quantitative analysis (e–f) show erosive bone changes and joint space widening with increased tracer uptakes in periarticular bones
Discussion
In this retrospective study, we compared planar bone scan parameters and SPECT/CT quantitative parameters for SI joint assessment. Compared to the SI/S ratio in a planar bone scan, ROC curve analysis showed that all the SPECT/CT parameters had higher AUC values. This finding is consistent with another previous study showing the superiority of SPECT/CT compared to a planar bone scan. The VOI of SI joint on SPECT/CT images could more accurately reflect the distribution of tracer uptake in periarticular bones without overlapping with other bones, which allowed improved sensitivity and specificity of both qualitative and quantitative evaluation of SI joint. In contrast, the ROI of the SI joint on the posterior planar bone scan did not reflect joint activity well because the periarticular uptake of the SI joint was masked by high uptake of the posterior iliac crest.
For years, bone scan has been used to diagnose inflammation in the SI joint. However, it has shown low sensitivity in reports. A review article from Song et al. in 2008 reported that the overall sensitivity for a bone scan to detect sacroiliitis was 51.8% for patients with established axial SpA [8], and the main cause of low sensitivity is the complex anatomy of the SI joints. With recent technical advances, SPECT/CT imaging enables three-dimensional evaluation and quantitative analysis of SI joints. Furthermore, we implemented the “AAZ,” that is, “zone of voxels with higher SUV than sacral mean SUV within VOI of SI joints,” to easily include only the active inflammatory portion in the periarticular bone of each SI joint using sacral mean SUV of the corresponding normal patient as a reference with the aid of a software program. Therefore, SUV-AAZ/S could show improved diagnostic performance, which had the highest AUC value among all parameters in ROC analysis, and SUV-AAZ/S showed a sensitivity of 100% and specificity of 99%, with 1.17 as the optimal cut-off point value.
Although several previous studies showed that SPECT/CT images had better performance than planar images in quantitative analysis of arthritis activity, different VOI generation methods and parameters were used in each study, and the details of the quantitation method were not established. In the report by Kim et al., advantages of SPECT/CT over conventional bone scans for diagnosis of sacroiliitis in 20 patients with early axial SpA were shown [9]. The authors defined the SI joint VOI as “the space between the sacrum and iliac bone from the start to end of the SI joint” without including the iliac or sacral bones. On the other hand, we included periarticular iliac and sacral bones within a 6 mm width from the central line of the joint space in the joint VOI. Although sacroiliitis is raised from the inflammation of fibrous connective tissue or synovitis, we think that the inclusion of periarticular bones in the SI joint VOI is mandatory because the main uptake mechanism of bone-seeking radiopharmaceuticals is chemisorption into the hydroxyapatite structure of the bone. In another recent study reported by Ornilla et al., the VOI of the SI joint included the sacrum and iliac bones like our study [10]. However, instead of SUVmean of the sacrum, they applied SUVmax of the sacrum and the sacroiliac/sacral SUVmax ratio to evaluate SI joint activity. SUVmax from just one voxel value might not represent the bone activity of the whole reference region, and accordingly, SUVmean is usually preferred as the reference value in quantitative analysis of bone scans. Therefore, we used SUVmean for reference bone value. Furthermore, SUVmean-related values such as SUV50% or AAZ of the SI joint might be more representative for assessing the severity of arthritis compared with that of SUVmax. For example, as shown in the case of Fig. 5, the SUV50% or AAZ ratio showed a higher value on the right side when the SUVmax value was higher on the left side. In this case, the extent of bone marrow signal change on MR or structural change on simple radiography was more severe on the right side, which is presumed to be the more progressed active sacroiliitis involvement site. This could be explained by the fact that the SUVmax value reflects the highest one voxel value, whereas the AAZ or SUV50% values reflect the total volume of the active arthritic zone.
In order to discriminate normal SI joints from sacroiliitis-involved joints, we also compared the ratios of the SUV parameters of the SI joints to the SUVmean of the sacrum, namely, SUVmax/S, SUV50%/S, and SUV-AAZ/S. One of the notable findings in this study was that these ratio parameters showed higher diagnostic performance compared with mere SUV parameters. The quantitative value expressed as SUV is the process of calculating the osseous radioactivity concentration, which represents the osteoblastic activity and blood flow of the measured bone area. In active sacroiliitis, SUV of the periarticular bones showed increased values. However, SUV values on bone SPECT/CT may also be affected by many other factors, such as sex, age, site of the bone, body weight, uptake time, parathyroid hormone level, and so on [11]. Therefore, by eliminating the effect of these other factors affecting SUV in individual patients, ratio parameters of SI joint SUV to internal reference bone SUV value may show better diagnostic performance than mere SUV parameters. This means that eventually, we may not need to put effort into acquiring absolute quantitative SUV parameters, which require additional information and efforts such as knowing the exact injected dose; instead, we may use semi-quantitative ratio parameters to quantify SI joint activity on bone SPECT/CT.
Currently, quantitative SPECT/CT studies of SI joints are limited, but studies regarding other disease entities have shown the usefulness of SPECT/CT in quantification analysis. One study by Ogura et al. reported that SPECT/CT quantitative parameters such as SUVmax, SUVpeak, and SUVmean showed significantly higher values in patients with chronic osteomyelitis when compared with those with medication-related osteonecrosis of the jaw (MRONJ) [12]. Laroche et al. reported that SPECT/CT quantitative parameter SUVmax showed a correlation with the staging of pre-operative osteoarthritis [13]. Lee et al. reported that SUVmax from quantitative bone SPECT/CT was strongly related to disease activity of accessory navicular bone, which showed that SPECT/CT parameters could be applied as an objective criterion for surgical treatment of accessory navicular syndrome [14]. In another study, Kitajima et al. reported that quantitative analysis of SPECT/CT was useful in bone inflammatory activity and treatment response evaluation in a patient with mandibular osteomyelitis after antibiotic therapy, hyperbaric oxygen therapy, and sequestomy. SUVmax, SUVpeak, SUVmean, and metabolic bone volume values along with the main symptom, namely, pain, all decreased after treatment [15]. At present, the commonly used index for disease activity evaluation in sacroiliitis is the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) and Ankylosing Spondylitis Disease Activity Score with C-reactive protein (ASDAS-CRP). ASDAS-CRP is a relatively more recently suggested disease activity score, combining BASDAI, patient global assessment of disease activity, and CRP into one index. However, so far, it lacks validation and does not seem sensitive or objective enough for disease activity evaluation [11]. In the future, studies with a larger number of patients analyzing the relationship between patient pain scale, CRP, or ESR, and bone SPECT/CT parameters may help solve this problem. Bone SPECT/CT may play a crucial part in the treatment response evaluation of patients with sacroiliitis. Currently, the most frequently utilized imaging modality for early sacroiliitis evaluation is MRI. However, in this retrospective study, we could not analyze the correlation between the quantitative data of SPECT/CT and the severity of arthritis on MRI due to insufficient available data. This needs to be considered in future studies with larger series of patients.
This study has several limitations. Since this is a single-center retrospective study, referral bias could not be excluded, and the sample size of the sacroiliitis group was relatively small compared with the normal control group. The patients who underwent SPECT/CT were already at NY stage 2–3 with developed sacroiliitis in simple radiography with structural changes. Since we only included patients with definite sacroiliitis and excluded other SI joint abnormalities such as degenerative arthritis or osteitis condensans ilii, this may have caused some bias in the result. In the present study, there was no significant difference between SPECT/CT ratio parameters, and we could not pinpoint the best SPECT/CT parameter for sacroiliitis evaluation. This could be due to the small patient number included in the analysis. Further studies with larger series of patients with additional subgroup analysis applying optimal protocols for quantitative SPECT/CT imaging and correlation with additional clinical data such as CRP or ESR of patients are needed in the future.
Conclusions
The quantitative analyses of bone SPECT/CT showed better performance in assessing active sacroiliitis than the planar bone scan. SPECT/CT parameters using the ratio of the SI joint to sacrum showed more favorable results than mere SUV parameters such as SUVmax, SUV50%, and SUV-AAZ. Therefore, future studies utilizing SPECT/CT in SI joint evaluation should consider including parameters using the ratio of the SI joint to the sacrum.
Data Availability
The datasets generated during the current study are available from the corresponding author on request.
References
Lukas C, Landewe R, Sieper J, Dougados M, Davis J, Braun J, et al. Development of an ASAS-endorsed disease activity score (ASDAS) in patients with ankylosing spondylitis. Ann Rheum Dis. 2009;68:18–24.
van der Heijde D, Ramiro S, Landewe R, Baraliakos X, Van den Bosch F, Sepriano A, et al. 2016 update of the ASAS-EULAR management recommendations for axial spondyloarthritis. Ann Rheum Dis. 2017;76:978–91.
Slobodin G, Hussein H, Rosner I, Eshed I. Sacroiliitis - early diagnosis is key. J Inflamm Res. 2018;11:339–44.
Zilber K, Gorenberg M, Rimar D, Boulman N, Kaly L, Rozenbaum M, et al. Radionuclide methods in the diagnosis of sacroiliitis in patients with spondyloarthritis: an update. Rambam Maimonides Med J. 2016;7:e0037.
Zilber K, Gorenberg M, Boulman N, Kaly L, Slobodin G. Radionuclide methods in the diagnosis of sacroiliitis in patients with spondyloarthritis: an update. Rambam Maimonides Med J. 2016;73:1477–84.
Lee EJ, Kim JY, Park JM, Song BI, Choi H, Shim HK, et al. Computed tomography (CT) protocols associated with cardiac and bone single-photon emission computed tomography/CT (SPECT/CT) in Korea. Nucl Med Mol Imaging. 2020;54:139–46.
Han S, Oh M, Oh JS, Lee SJ, Oh SJ, Chung SJ, et al. Subregional pattern of striatal dopamine transporter loss on 18F FP-CIT positron emission tomography in patients with pure akinesia with gait freezing. JAMA Neurol. 2016;73:1477–84.
Song IH, Carrasco-Fernandez J, Rudwaleit M, Sieper J. The diagnostic value of scintigraphy in assessing sacroiliitis in ankylosing spondylitis: a systematic literature research. Ann Rheum Dis. 2008;67:1535–40.
Kim YI, Suh M, Kim YK, Lee HY, Shin K. The usefulness of bone SPECT/CT imaging with volume of interest analysis in early axial spondyloarthritis. BMC Musculoskelet Disord. 2015;16:9.
Ornilla E, Sancho L, Beorlegui C, Ribelles MJ, Aquerreta D, Prieto E, et al. Diagnostic value of quantitative SPECT/CT in assessing active sacroiliitis in patients with axial spondylarthritis and/or inflammatory low back pain. An Sist Sanit Navar. 2022;45:e0953.
Qi N, Meng Q, You Z, Chen H, Shou Y, Zhao J. Standardized uptake values of (99m)Tc-MDP in normal vertebrae assessed using quantitative SPECT/CT for differentiation diagnosis of benign and malignant bone lesions. BMC Med Imaging. 2021;21:39.
Ogura I, Kobayashi E, Nakahara K, Igarashi K, Haga-Tsujimura M, Toshima H. Quantitative SPECT/CT imaging for medication-related osteonecrosis of the jaw: a preliminary study using volume-based parameters, comparison with chronic osteomyelitis. Ann Nucl Med. 2019;33:776–82.
De Laroche R, Simon E, Suignard N, Williams T, Henry MP, Robin P, et al. Clinical interest of quantitative bone SPECT-CT in the preoperative assessment of knee osteoarthritis. Medicine (Baltimore). 2018;97:e11943.
Kim JY, Kim JY, Park SB, Kim C, Lee WW. A retrospective multicenter study of quantitative bone SPECT/CT to predict the surgical removal of the accessory navicular bone. Nucl Med Commun. 2021;42:998–1004.
Kitajima K, Noguchi K, Moridera K, Kishimoto H, Tsuchitani T, Takahashi Y, et al. Usefulness of quantitative bone SPECT/CT for evaluating treatment response in a patient with mandibular osteomyelitis. Case Rep Oncol. 2021;14:820–5.
Acknowledgements
The authors would like to thank Youngwoong Ha and Jangwon Park, technologists in the Department of Nuclear Medicine, Asan Medical Center, for their excellent technical assistance.
Author information
Authors and Affiliations
Contributions
The study was designed by Jin-Sook Ryu and Yong-il Kim. Material preparation and data collection were performed by Koeun Lee, Seokchan Hong, Yong-Gil Kim, Bumwoo Park, and Woo Hyun Shim. The data analysis was performed by Koeun Lee and Jungsu S. Oh. The first draft of the manuscript was written by Koeun Lee, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of Interest
Author Koeun Lee, Author Hyunji Kim, Author Yong-il Kim, Author Bumwoo Park, Author Woo Hyun Shim, Author Jungsu S. Oh, Author Seokchan Hong, Author Yong-Gil Kim, and Author Jin-Sook Ryu declare that they have no competing interests.
Ethics Approval and Consent to Participate
The present study was approved by the institutional review board of the Asan Medical Center (IBR No: 2021–0113), and the requirement for written consent was waived by the institutional review board. All procedures performed in this study involving human participants were in accordance with the ethical standards of the respective Institutional Research Committee and with the 2013 Helsinki Declaration and its later amendments or comparable ethical standards.
Consent for Publication
The Institutional Review Board at our institute approved this retrospective study, and the requirement to obtain informed consent was waived.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Lee, K., Kim, H., Kim, Yi. et al. Preliminary Study for Quantitative Assessment of Sacroiliitis Activity Using Bone SPECT/CT: Comparison of Diagnostic Performance of Quantitative Parameters. Nucl Med Mol Imaging 56, 282–290 (2022). https://doi.org/10.1007/s13139-022-00766-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13139-022-00766-2