
Abstract
Background
The hepatic hydatid cyst is a major public health concern in endemic areas. It presents a therapeutic challenge when it occurs in pregnant women and exposes the mother and the fetus to a high mortality risk in the case of complications. The main complication is communication with the biliary tree, which fortunately is rare.
Methods
A multi-center retrospective study was conducted spanning 7 years, from January 2009 to December 2015. In 17 departments of surgery across Tunisia, 24 cases were identified of pregnant women who were treated for complicated hepatic hydatid cyst. The data on their treatment and outcome were retrieved from the medical records.
Results
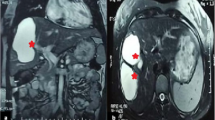
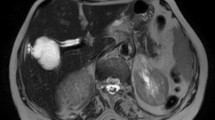
The age range of the 24 patients was 23 to 40 years, median 30 years. The median gestational age was 15 weeks (range 5 to 29 weeks).The patients complained of a variety of symptoms, mainly abdominal pain (87.5%), fever (50%), jaundice (50%) and vomiting (21%). The laboratory examination showed leukocytosis (54.2%), cholestasis (41.7%), elevated liver enzymes (12%), and positive blood culture (6%). On abdominal ultrasound (U/S), dilatation of the common bile duct was observed in 41% of the cases, dilatation of the intra-hepatic bile ducts in 50%, and hydatid material in the duct in 12% of the cases. Most of the cysts were located in the right lobe of the liver, in the hepatic dome. All of the patients were treated surgically, by one of three types of intervention: Largot intervention (18 cases), internal transfistulary drainage (4 cases), and the Perdromo procedure (2 cases). Postoperative follow-up was complication-free for 20 patients. In the remaining four, complications included: purulent retention (1 case), biliary fistula (2 cases), pneumonia (1 case). There was no maternal death. A tocolytic agent was administered to 16 women and 21 had a live full-term birth. One spontaneous miscarriage and 2 neonatal deaths occurred.
Conclusions
Complicated hydatid cyst in pregnancy is a serious condition which can be life-threatening for the mother and the fetus. The treatment is surgical, and patient management requires close collaboration between the surgeon, the anesthesiologist and the obstetrician-gynecologist.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
Gharbi HA, Ben Chehida F, Moussa N, et al. Hydatid cyst of the liver. Gastroenterol Clin Biol. 1995;19:B110–8.
Zaouche A, Haouet K, Jouini M, et al. Management of the liver hydatid cysts with large bilio-cystic fistula. A multicenter retrospective study. World J Surg 2001;25:28–40.
Beyrouti MI, Beyrouti R, Abbes I, et al. Rupture aiguë du kyste hydatique dans le péritoine: A propos de 17 observations. Presse Med 2004;33:378–84.
Rahman MS, Rahman J, Lysikiewicz A. Obstetric and gynaecological presentations of hydatid disease. Br J ObstetGynaecol 1982;89:665–70.
Ustunsoz B, Alemdaroglu A, Bulakbasi N, et al. Percutaneous treatment of hepatic hydatid cyst in pregnancy. Arch Gynecol Obstet 1999;262:181–4.
Candas Erçetin, Ilgin Özden, Cem Iyibozkur, et al. Hepatic hydatid disease requiring urgent treatment during pregnancy. Turkish Journal of Trauma & Emergency Surgery. 2013;19:119–22.
Ghosh JK, Goyal SK, Behera MK, et al. Hydatid cyst of liver presented as obstructive jaundice in pregnancy; Managed by PAIR. Journal of Clinical and Experimental Hepatology. 2014;4:366–9.
Curet MJ. Special problems in laparoscopic surgery. Previous abdominal surgery, obesity, and pregnancy. SurgClin North Am 2000;80:1093–110.
Van Vliet W, Scheele F, Sibinga-Mulder L, et al. Echinococcosis of the liver during pregnancy. Int J GynaecolObstet 1995;49:323–4.
Polat Coskun, Sivaci Remziye, Baki Elif, et al. Recurrent hepatic hydatid cyst in a pregnant woman. MedSciMonit 2007;13:CS27–9.
Haxhimolla HZ, Crowe P. Hydatid disease of the liver in pregnancy. ANZ J Surg 2001;71:692–3.
Ennabli K, Gharbi S, Farhat M, et al. A propos d’une expérience du traitement du kyste hydatique du foie à l’hôpital FarhatHached de Sousse. Tunisie Médicale, 1978;56:455–8.
Bouzidi A, Chehab F. Traitement chirurgical des fistules bilio kystiques d’origine hydatique. À propos de 83 cas. Chir 1997;134:114–8.
Daali M, Fakir Y, Hssouda R, et al. Les kystes hydatiques du foie rompus dans les voies biliaires. A propos de 64 cas. Ann Chir 2001;126:242–5.
Kayabali I, Kayabali M, Kaynak A, et al. Sur le diagnostic et le traitement des kystes hydatiques du foie. Clin Chir 1984;186–8.
Bouhaouala MH, Hendaoui L. Imagerie de la maladie hydatique. Centre de publication universitaire 2005.
Gharbi HA, Chehida F, Moussa N, et al. Kyste hydatique du foie. Gastroenterol Clin Biol 1995;19:B110–8.
Zouari K, Gargouri R, Selmi M, et al. Les examens complémentaires au cours du kyste hydatique du foie. Rapport du XVème congrès de la Société Tunisienne de Chirurgie Tunis 1994;41–58.
Buted C, Plainfosse M, Merran S. Apport de l'échotomographie à l'étude des kystes hydatiques dans leurs différentes localisations sus et sous diaphragmatiques. Ann Radiol 1980;23:7.
Kayabali I, Kayabali M, Kaynak A, et al. Sur le diagnostic et le traitement des kystes hydatiques du foie. Clin Chir 1984;186–8.
Abdessalem K, Hassine W, Gharbi HA. Complications biliaires des kystes hydatiques du foie Med Chir Digest 1982; 11:189–91.
Ayachi K, Oueslati A, Daoues A, et al. Les angiocholites graves. A propos d’une série de 24 cas colligés de 1979 à 1983. Med Chir Dig 1985;14:109–10.
Bendib A, Bendib S, Benmamar L, et al. La TDM du kyste hydatique du foie: Sémiologie et classification: à propos de 157 cas dont 146 vérifiés chirurgicalement. J Radiol 1985;6:367–75.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Baraket, O., Triki, W., Rebii, S. et al. Management of Complicated Hydatid Cyst in Pregnancy. A Multicenter Study. Hellenic J Surg 90, 172–176 (2018). https://doi.org/10.1007/s13126-018-0467-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13126-018-0467-x