
Abstract
Aim
To highlight the unusual postoperative clinical presentation of a retained sponge.
Background
Recognition of postoperatively retained foreign bodies is essential but often delayed, either because of medicolegal implications or because of a confusing clinical presentation and non-specific imaging features. In contrast to radio-opaque materials which are detected at follow-up imaging, radiolucent objects like sponges create problems in identification.
Case Report
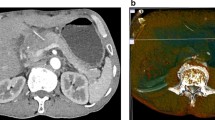
A 30-year-old lady presented with intermittent non-bilious vomiting, epigastric pain and fever. Contrast-enhanced computed tomography of the abdomen showed a heterogeneous mass in the duodenum with multiple air pockets. Surgical exploration revealed a full-size surgical sponge with one end embedded in the gallbladder fossa and the other perforating the antrum of the stomach, thus causing an obstruction. The sponge was retrieved, and distal gastrectomy with Billroth II anastomosis was performed. The postoperative course was uneventful.
Conclusion
A high degree of suspicion and awareness of non-specific symptomatology associated with retained sponges after surgery is essential for early diagnosis and correct treatment.
Article PDF
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
References
Gwande AA, Studdert DM, Orav JE, Brennan TA, Zinner MJ. Risk factors for retained instruments and sponges after surgery. N Engl J Med 2003; 348:229
Rappaport W, Haynes K. The retained surgical sponge following intra-abdominal surgery. Arch Surg 1990; 125:405
Kaiser CW, Freidman S, Spurling KP, Slowick T, Kaiser HA. The retained surgical sponge. Ann Surg 1996; 224:79
Gibbs VC, Coakley FD, Reines HD. Preventable errors in the operating room: retained foreign bodies after surgery-Part I. Curr Probl Surg 2007; 44:281–337
Menteş BB, Yilmaz E, Sen M, Kayhan B, Görgül A, Tatlicioğlu E. Transgastric migration of a surgical sponge. J Clin Gastroenterol 1997; 24:55–57
Hyslop JW, Maull KI. Natural history of the retained surgical sponge. Southern Med J 1982; 75:657
Gibbs VC, Auerbach AD. The retained surgical sponge. In: Shojania KG, Duncan BW, McDonald KM, Wachter RM, (eds). Making health care safer: a critical analysis of patient safety practices. Evidence/Report/Technology Assessment No. 43, AHQR Publication No. 01-E058; July 2001
McLeod RS, Bohnen MA. Canadian association of general surgeons evidence based reviews in Surgery: Nine risk factors for retained foreign body after surgery. Can J Surg 2004; 47:57
Fabian CE. Electronic tagging of surgical sponges to prevent their accidental retention. Surgery 2005; 137:298
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Singh, R., Godara, R., Verma, S. et al. Transmural migration of surgical sponge into the stomach with outlet obstruction: Rare Case. Hellenic J Surg 86, 166–168 (2014). https://doi.org/10.1007/s13126-014-0120-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13126-014-0120-2