
Abstract
Purpose
Accidental dural puncture and post-dural puncture headache are well-known complications of neuraxial anesthesia in parturients. The primary goal of this study was to identify the rate of post-dural puncture headache and epidural blood patch in all parturients who received a neuraxial anesthetic during a ten-year period at an academic tertiary-care medical centre. A secondary goal was to identify any delay in hospital discharge due to a post-dural puncture headache.
Methods
We conducted a retrospective analysis of all patients who received a neuraxial anesthetic on the labour and delivery unit at Stony Brook Medical Center from 1 January, 2006 to 31 December, 2015. Standardized neuraxial anesthesia equipment was used throughout this period. Chart reviews were conducted on all patients who received a neuraxial anesthetic and had an accidental dural puncture and/or developed a post-dural puncture headache.
Results
Of the 32,655 neuraxial anesthetics performed, 298 (0.9%) patients experienced a post- dural puncture headache. Analysis of all patients who developed a post-dural puncture headache showed that 150 (50.3%) patients received one or more epidural blood patches. Overall, 19 (0.06%) patients had a delay in hospital discharge due to a post-dural puncture headache.
Conclusions
We showed a relatively low incidence (< 1%) of post-dural puncture headache following neuraxial anesthesia in parturients at an academic tertiary-care medical centre. Patients that rated their post-dural puncture headache as very severe were more likely to undergo at least one epidural blood patch procedure. Post-dural puncture headache is a well-known complication of neuraxial anesthesia, and may lead to a delay in hospital discharge.
Résumé
Objectif
La ponction accidentelle de la dure-mère et les céphalées post-ponction dure-mérienne (CPPD) sont des complications bien connues de l’anesthésie neuraxiale chez les parturientes. L’objectif premier de cette étude était d’identifier le taux de CPPD et de colmatages sanguins périduraux (couramment appelés epidural blood patch) chez toutes les parturientes ayant reçu une anesthésie neuraxiale au cours d’une période de dix ans dans un centre médical universitaire de soins tertiaires. Un objectif secondaire était d’identifier tout délai dans le congé de l’hôpital dû à des CPPD.
Méthode
Nous avons réalisé une analyse rétrospective de toutes les patientes ayant reçu une anesthésie neuraxiale à l’unité des naissances du Centre médical Stony Brook entre le 1er janvier 2006 et le 31 décembre 2015. De l’équipement standardisé pour l’anesthésie neuraxiale a été utilisé tout au long de cette période. Les dossiers médicaux de toutes les patientes ayant reçu une anesthésie neuraxiale et ayant subi une ponction dure-mérienne accidentelle et/ou ayant manifesté des CPPD ont été passés en revue.
Résultats
Sur les 32 655 anesthésies neuraxiales réalisées, 298 (0,9 %) patientes ont souffert de CPPD. L’analyse de toutes les patientes ayant manifesté des CPPD a montré que 150 (50,3 %) patientes ont reçu un ou plusieurs colmatages sanguins périduraux. Globalement, 19 (0,06 %) patientes ont vu leur congé de l’hôpital retardé en raison de CPPD.
Conclusion
Nous avons démontré une incidence relativement faible (< 1 %) de céphalées post-ponction dure-mérienne après une anesthésie neuraxiale chez les parturientes prises en charge dans un centre médical universitaire de soins tertiaires. Les patientes ayant évalué leur CPPD comme étant très sévère étaient plus susceptibles de subir au moins une intervention de colmatage sanguin péridural. Les céphalées post-ponction de la dure-mère sont une complication bien connue de l’anesthésie neuraxiale et peuvent entraîner un retard dans le congé de l’hôpital.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
The use of neuraxial anesthesia in parturients has greatly increased over the past 30 years.1,2 Bucklin et al. reported that in hospitals with ≥ 1,500 births performed per year, 22% of patients received epidurals for labour analgesia in 1981 compared with 61% in 2001.1 Compared with general anesthesia, the use of neuraxial anesthesia has contributed to a decrease in maternal morbidity and mortality, including a reduction in failed tracheal intubations, estimated blood loss, and postpartum hemorrhage.3,4,5 Accidental dural puncture (ADP) and post-dural puncture headache (PDPH) are well-described complications of neuraxial anesthesia in obstetric patients. Dural puncture may lead to intracranial hypotension from the excessive leakage of cerebrospinal fluid (CSF) into the epidural space, resulting in a reduction of CSF volume, with downward pressure exerted on cranial structures when sitting or standing.6 The development of a PDPH in the postpartum period can be debilitating, limiting a mother’s ability to care for her infant. It may also result in chronic headaches, and even lead to more serious morbidity such as reversible cerebral vasoconstriction syndrome and subdural hematoma.7,8,9,10,11 Post-dural puncture headache may also lead to a delay in hospital discharge.
An epidural blood patch (EBP) remains the most reliable treatment or PDPH, with the resolution of symptoms often seen after one EBP procedure. Safa-Tisseront et al. showed that EBP led to complete relief of PDPH symptoms in 75% of non-parturient patients.12 The mechanism of action of EBP is not clearly understood. One theory suggests that the blood injected in the epidural space plugs the dural hole, causing clot formation and sealing it from further CSF leakage.13 Nevertheless, this theory does not explain the rapid onset of headache relief following an EBP. Another theory postulates that the blood injected into the epidural space increases lumbar CSF pressure, leading to reflex cerebral vasoconstriction by reestablishing the intracranial CSF pressure.14 Close patient follow-up by the anesthesia team provides improved identification and management of ADP and PDPH in obstetric patients.
There are a few contemporary large-scale longitudinal studies on obstetric patients and PDPH,15,16,17,18 but these studies do not report onset and severity of the PDPH, rates of EBP use, and delay in hospital discharge due to a PDPH. The primary goal of this study was to analyze the incidence of ADP and the rates of PDPH and EBP in parturients that received a neuraxial anesthetic during a ten-year period at an academic tertiary-care medical centre. A secondary goal was to examine if any delays in hospital discharge occurred as a result of a PDPH.
Methods
This project was authorized by the Stony Brook Medicine Division of Medical and Regulatory Affairs Office as part of its Surgical Quality Improvement Program (SQIP). Following de- identification and extraction of all SQIP patient records, a data analysis was performed as part of the Surgical Quality Data Users Group (SQDUG). The SQIP/SQDUG protocols were approved by our institution’s investigational review board Committee on Research Involving Human Subjects, Stony Brook University; CORIHS #170753-9), who waived the requirement for specific informed written consent. The SQIP/SQDUG is an institutional approval process for quality assurance studies and/or research, and it serves as an umbrella for all department databases. This manuscript adheres to the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) guidelines.19
We conducted a retrospective analysis of obstetric patients at Stony Brook Medical Center from 1 January, 2006 to 31 December, 2015. Our obstetric anesthesia department maintains a database of all patients who receive an anesthetic on our labour and delivery unit. We abstracted charts from all patients who received a neuraxial anesthetic and had an ADP or PDPH during the ten-year period. Our obstetric anesthesia service has a rigorous approach to collection of adverse events such as ADP and PDPH, and an extensive postoperative patient follow-up method. The chief of obstetric anesthesia was the same for all ten years, thus procedures for reporting and documenting complications such as ADPs and PDPH were standardized and consistent throughout the study period. All anesthesiology providers are trained to report any accidental or presumed dural puncture, and/or PDPH. All patients are examined by the obstetric anesthesia team 24–48 hr postpartum. In addition, the obstetric team and postpartum nurses are trained to contact the obstetric anesthesia team when a patient develops a positional headache. All patients who experienced an ADP and/or a PDPH were followed closely throughout their hospital stay, and contacted every day for two to three days immediately upon discharge until pproximately one-week postpartum or resolution of the PDPH. All patients were given verbal and written instructions on symptoms associated with PDPH, and how to contact the obstetric anesthesia team.
A recognized ADP was defined as the visualization of CSF either via the Tuohy needle or via the epidural catheter, or a positive test dose of the epidural catheter that showed a high level of anesthesia. A presumed ADP was defined as an epidural catheter placement that led to a PDPH, but where CSF was not visualized either via the Tuohy needle or epidural catheter during placement. The term ADP did not apply to spinal anesthetics, since dural puncture is intentional during the placement of a spinal. The definition of ADP also included recognized and presumed ADP during the placement of an epidural catheter for combined spinal-epidural (CSE) anesthesia. Post-dural puncture headache was defined as a positional headache following the use of a neuraxial anesthetic that displayed worsening symptoms when sitting or standing, with symptom reduction when recumbent.
Our obstetric anesthesia team used standardized and consistent anesthetic techniques during the time course of this analysis. We used a 17G Tuohy needle and a 20G
multi-orifice nylon epidural catheter for epidural placements, followed by a 3-mL test dose of 1.5% lidocaine with 1:200,000 epinephrine via the epidural catheter. Combined spinal-epidural anesthetics utilized a 17G Tuohy needle and a 25G Pencan needle, and a 24G Sprotte needle and 20G introducer were utilized for spinal anesthetics throughout the ten-year period. Epidural blood patches were performed using a 17G Tuohy needle, sterile peripheral blood draw, and varying amounts of blood injected via the Tuohy needle into the epidural space, as tolerated by the patient. Neuraxial procedures were primarily performed by anesthesia residents under the supervision of an attending anesthesiologist.
Data collected included demographic information such as age, race, gestational age, parity, body mass index (BMI), the type of anesthetic, whether CSF was observed during the procedure (via Tuohy, epidural catheter, or spinal introducer), and the development of a documented PDPH. For all patients who developed a PDPH, we analyzed documentation by the primary team and determined if the patient met discharge criteria but remained in the hospital because of symptoms associated with a PDPH. Hospital discharge delay due to PDPH was defined as the number of days following discharge criteria being met as per the obstetric team, but where the patient remained in the hospital for the treatment of PDPH symptoms. Discharge delays due to any other medical cause or social issues were excluded.
Statistical analysis
For calculation of the overall incidence of PDPH, all neuraxial anesthetics on labour and delivery during the study period were included. The analysis on demographics and risk factors associated with PDPH following dural puncture included all patients with an ADP during an epidural or CSE placement, and patients that received a spinal anesthetic and developed a PDPH. In our analysis of demographics associated with PDPH, all patients that developed a PDPH following a neuraxial anesthetic were included.
Wald confidence intervals (CIs) were generated for neuraxial anesthetic point estimates. Continuous variables were tested for normality using the Shapiro–Wilk test at P < 0.05. Normally distributed data are presented as mean (standard deviation [SD]) and non-normal data are reported as median [interquartile range (IQR)]. All bivariate analyses were performed using either Student’s t test or Wilcoxon rank sum for continuous variables, and Chi square or Fisher’s exact tests for categorical variables. The BMI was dichotomized below or above 31.5 kg·m−2, which is a cut-off established in previous literature.20 All calculations were performed at a 95% confidence interval using SAS© 9.4 (SAS Institute, Cary, NC, USA).
Results
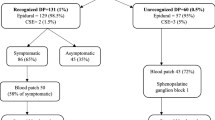
There were a total 37,491 live births and 32,655 neuraxial anesthetics performed on the labour and delivery unit at Stony Brook University Hospital from 1 January, 2006 to 31 December, 2015. Approximately 87.1% of the patients who had a live birth received a neuraxial anesthetic, with a Cesarean delivery in 38.2% of all live births during the study period. There were 21,795 (66.7%) epidurals, 611 (1.9%) CSEs, and 10,249 (31.4%) spinal anesthetics. Of all patients who received an epidural, 290 (1.3%) had an ADP (both recognized and presumed), 208 (1.0%) were recognized ADPs, and 224 (1.0%) developed a PDPH. There were 14 (2.3%) patients who received a CSE and had an ADP (both recognized and presumed), 13 (2.1%) of which were recognized by CSF return via either the Tuohy needle or epidural catheter, and 8 (1.3%) developed a PDPH. A total of 70 (0.7%) patients who had a spinal anesthetic developed a PDPH (Figure and Table 1).

Number and type of neuraxial anesthetics performed between January 2006 and December 2015
Demographics for all patients that had either an ADP during an epidural or CSE placement as well as patients with a spinal anesthetic that developed a PDPH are shown in Table 2. Of note, the mean (SD) age was 29.4 (6.3) yr, and median [IQR] gestational age was 39 [38–40] weeks. In terms of parity, 195 (52.6%) of all patients with dural puncture were primigravida, 163 (43.9%) were Caucasian (including Hispanic patients), and 195 (52.6%) had a BMI < 31.5 kg·m−2. Of all patients with a dural puncture, 230 (62%) had a vaginal delivery, 130 (35%) had a Cesarean delivery, and 11 (3%) had a cerclage, dilation and curettage (D&C), or dilation and evacuation (D&E) (Table 2).
The total number of patients with PDPH following a spinal or an ADP (recognized and presumed) was 371, of which 73 (19.7%) did not develop a PDPH, and 298 (80.3%) developed a PDPH. Patients with a BMI < 31.5 kg·m−2 were more likely to develop a PDPH after dural puncture compared with patients with a BMI ≥ 31.5 kg·m−2 (P = 0.007; Chi square). Multiparous patients were more likely to develop a PDPH after dural puncture compared with nulliparous patients (P = 0.009, Chi square). There was no significant difference seen in gestational age between the two groups (P = 0.07, Wilcoxon rank sum) (Table 3).
Analysis of all patients (n = 298) that developed PDPH showed that 148 (49.7%) did not receive an EBP, 128 (42.9%) received one EBP, and 22 (7.4%) received more than one EBP. Body mass index was significantly different between the three groups. Patients with BMI < 31.5 kg·m−2 who had a PDPH were significantly more likely to receive more than one EBP (86.4% for BMI < 31.5 kg·m−2vs 13.6% for ≥ 31.5 kg·m−2; P = 0.001). Age, gestational age, parity (nulliparity vs multiparity), type of delivery (vaginal vs Cesarean delivery), day of onset of headache, and whether the dural puncture was recognized during the neuraxial (epidural or CSE) placement did not seem to differ significantly among the three groups. Differences were seen in the race category across the groups, with progressively greater numbers of Caucasian patients observed across the increasing blood patch groups (53%, 73%, 82% Caucasian for 0, 1, and > 1 blood patch groups, respectively; P = 0.003). Severity of headache (scores 1–10, with 10 being most severe) showed a significant difference between the three groups (P < 0.001); higher medians were observed in the blood patch groups. Patients with severe PDPHs (8–9/10 pain) were more likely to receive an EBP compared with less severe PDPHs (7/10 or less pain) (Table 4).
Finally, we examined whether the patients who developed a PDPH had a delay in their discharge from the hospital. Four (2.7%) PDPH patients with no EBP had their discharge delayed, ten (7.9%) patients who had a PDPH and received one EBP had their discharge delayed, and 5 (22.7%) patients who had a PDPH and more than one EBP had their discharge delayed (P = 0.003). Overall, 0.06% of all patients who received a neuraxial anesthetic on our labour and delivery unit during the ten-year period had a delay in hospital discharge due to a PDPH (Table 4).
Discussion
There are few contemporary large-scale longitudinal analyses of parturients in tertiary- care centres with ADP, PDPH, and other complications over an extended period of time.16,17,18,21
Our study presents recent data on the overall rate of ADP and PDPH in all parturients treated at an academic tertiary-care medical centre from 2006 to 2015. Recent studies have shown that 0.5–1.5% of epidurals result in an ADP, of which 52–88% develop a PDPH,16,22,23 whereas 0.33–1.7% of the patients receiving a subarachnoid anesthetic develop a PDPH.16,21,22,23 Our analysis revealed that 1.0% of all patients that received an epidural developed a PDPH. The risk of developing a PDPH was 0.7% following a spinal, and 1.3% following a CSE. Therefore, our rates are within the published range of PDPH following neuraxial anesthetics in parturients at tertiary-care teaching hospitals.
There are several studies that report ADP in the obstetric population, but only a few publications have revealed demographic information on the patients with ADP.15,16,17,18,21,23 Orbach-Zinger et al. reported multiple factors such as age, BMI, parity, type of delivery, etc. in patients with ADP, but identified advanced cervical dilation as the only factor associated with a higher rate of ADP.22 We were unable to report cervical dilation prior to neuraxial placement in labouring patients because of the lack of electronic medical records for labour and delivery parameters for a majority of the time period included in the study.
We identified BMI and parity as factors associated with the development of a PDPH in patients with dural puncture. A few studies have suggested an inverse relationship between BMI and PDPH following ADP. For example, Peralta et al. reported a lower incidence of PDPH in patients with BMI ≥ 31.5 kg·m−2 compared with patients with BMI < 31.5 kg·m−2.20
We analyzed our data on BMI using Peralta et al.’s BMI cut-off value of 31.5, and obtained similar results. As a sensitivity analysis, we also ran BMI as a continuous variable. Results did not vary; a significantly lower BMI was seen in the PDPH group.
Nevertheless, other studies have shown that BMI does not represent a risk factor for the development of a PDPH following neuraxial anesthesia.24,25
Multiparity was identified as a risk factor for the development of PDPH after an ADP, with parturients with one or more previous births having a higher risk of PDPH (59.4%) compared with nulliparous parturients (40.6%). Our results are in agreement with Orbach-Zinger et al. in that multiparity is a risk factor for the development of a PDPH.22 We hypothesize that this difference stems from the fact that parturients with other children at home are less likely to be able to rest, and need to be in an upright position more frequently.
Epidural blood patch remains the most effective treatment for PDPH.12,26 Approximately half of all patients who developed a PDPH received one or more EBP. We found that the severity of the headache and BMI had direct correlations to the number of PDPH patients that elected for an EBP. The early onset of PDPH symptoms (days 0 or 1) appears to indicate a more severe headache necessitating EBP, as 95.5% of patients that required more than one blood patch developed symptoms on post-neuraxial anesthesia placement days 0 or 1. Patients that had more than one EBP had a lower BMI than the other groups, a finding that may correlate with the lower incidence of PDPH in patients with a BMI ≥ 31.5 kg·m−2. In addition, patients with a PDPH that had a vaginal delivery were more likely to need more than one EBP compared with Cesarean delivery patients, which may indicate that pushing during a vaginal delivery may worsen symptoms of a PDPH. Nevertheless, we were unable to obtain data on pushing because of the lack of electronic medical records during most of the study period. Other factors that contribute to this finding may include unwillingness to undergo another epidural procedure for EBP, availability of help from family or friends upon discharge, and a strong desire to return home. Symptoms of a PDPH can be debilitating, limiting functional status in the immediate postpartum period, and may increase the hospital length of stay. Post-dural puncture headache led to a delay in hospital discharge in 19 patients, 15 of which received a least one EBP. Our finding that PDPH following neuraxial anesthesia contributes to an increased hospital length of stay is in agreement with Orbach-Zinger et al. and Angle et al.22,27 The fact that 77% of the PDPH patients who needed more than one EBP experienced a delay in hospital discharge is not surprising, since most anesthesiologists will wait at least 24 hr for improvement of symptoms after the first EBP before performing a second EBP. Even though a delayed hospital discharge due to a PDPH increases medical costs and inconvenience to the parturient and her family, the efficacy of EBPs in the prevention of PDPH following ADP has not been determined.28,29,30
A limitation of this study includes its retrospective and single centre design.
Another limitation is the lack of demographic data on all the patients who received a neuraxial anesthetic during the ten-year period, which limits our ability to identify specific risk factors for ADP. The lack of information in our data set on the use of intrathecal or epidural opioids and the percentage of Cesarean deliveries that had a spinal anesthetic is another limitation in our analysis of risk factors for PDPH. Electronic medical records were not fully implemented in our labour and delivery unit until the end of our study period. Therefore, we were unable to obtain data on the duration of second-stage pushing, and the degree of cervical dilation prior to neuraxial placement in labouring patients.
The proven benefits of neuraxial anesthesia, such as superior pain control during labour, decreased risk in developing postpartum depression,31,32 and greater patient satisfaction, outweigh the low (1.0%) risk of developing a PDPH. Obese patients (BMI ≥ 31.5 kg·m−2) and primigravida patients who had an ADP were less likely to develop a PDPH. Epidural blood patch remains the most effective treatment for PDPH, with approximately 50% of patients who developed a PDPH requiring one or more EBP. We suggest that obstetric patients with a recognized ADP who develop early onset and severe symptoms of PDPH be offered an EBP as early as possible. Lastly, the 0.06% risk of delayed hospital discharge due to a PDPH is extremely low when compared with the total number of patients who received neuraxial anesthesia for labour without complications.
References
Bucklin BA, Hawkins JL, Anderson JR, Ullrich FA. Obstetric anesthesia workforce survey: twenty-year update. Anesthesiology 2005; 103: 645-53.
Wong CA. Advances in labor analgesia. Int J Womens Health 2010; 1: 139-54.
Kinsella SM, Winton AL, Mushambi MC, et al. Failed tracheal intubation during obstetric general anaesthesia: a literature review. Int J Obstet Anesth 2015; 24: 356-74.
Afolabi BB, Lesi FE. Regional versus general anaesthesia for caesarean section. Cochrane Database Syst Rev 2012; 10: CD004350.
Heesen M, Hofmann T, Klohr S, et al. Is general anaesthesia for caesarean section associated with postpartum haemorrhage? Systematic review and meta-analysis. Acta Anaesthesiol Scand 2013; 57: 1092-102.
Turnbull DK, Shepherd DB. Post-dural puncture headache: pathogenesis, prevention and treatment. Br J Anaesth 2003; 91: 718-29.
Webb CA, Weyker PD, Zhang L, et al. Unintentional dural puncture with a Tuohy needle increases risk of chronic headache. Anesth Analg 2012; 115: 124-32.
Chaves C, Freidberg SR, Lee G, Zerris V, Ries S, Chavali R. Cerebral vasospasm following intracranial hypotension caused by cerebrospinal fluid leak from an incidental lumbar durotomy. Case report. J Neurosurg 2005; 102: 152-5.
Chik Y, Hoesch RE, Lazaridis C, Weisman CJ, Llinas RH. A case of postpartum cerebral angiopathy with subarachnoid hemorrhage. Nat Rev Neurol 2009; 5: 512-6.
Sachs A, Smiley R. Post-dural puncture headache: the worst common complication in obstetric anesthesia. Semin Perinatol 2014; 38: 386-94.
Zeidan A, Farhat O, Maaliki H, Baraka A. Does postdural puncture headache left untreated lead to subdural hematoma? Case report and review of the literature. Int J Obstet Anesth 2006; 15: 50-8.
Safa-Tisseront V, Thormann F, Malassine P, et al. Effectiveness of epidural blood patch in the management of post-dural puncture headache. Anesthesiology 2001; 95: 334-9.
Beards SC, Jackson A, Griffiths AG, Horsman EL. Magnetic resonance imaging of extradural blood patches: appearances from 30 min to 18 h. Br J Anaesth 1993; 71: 182-8.
Carrie LE. Epidural blood patch: why the rapid response? Anesth Analg 1991; 72: 129-30.
Sprigge JS, Harper SJ. Accidental dural puncture and post dural puncture headache in obstetric anaesthesia: presentation and management: a 23-year survey in a district general hospital. Anaesthesia 2008; 63: 36-43.
Van de Velde M, Schepers R, Berends N, Vandermeersch E, De Buck F. Ten years of experience with accidental dural puncture and post-dural puncture headache in a tertiary obstetric anaesthesia department. Int J Obstet Anesth 2008; 17: 329-35.
Martinez B, Canser E, Alonso A, et al. Postdural puncture headache and epidural blood patch in a large obstetric anaesthesia population. Asian J Anesthesiol 2018; 56: 23-32.
Tien JC, Lim MJ, Leong WL, Lew E. Nine-year audit of post-dural puncture headache in a tertiary obstetric hospital in Singapore. Int J Obstet Anesth 2016; 28: 34-8.
von Elm E, Altman DG, Egger M, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: guidelines for reporting observational studies. Int J Surg 2014; 12: 1495-9.
Peralta F, Higgins N, Lange E, Wong CA, McCarthy RJ. The relationship of body mass index with the incidence of postdural puncture headache in parturients. Anesth Analg 2015; 121: 451-6.
Hartopp R, Hamlyn L, Stocks G. Ten years of experience with accidental dural puncture and post-dural-puncture headache in a tertiary obstetric anaesthesia department. Int J Obstet Anesth 2010; 19: 118-28.
Orbach-Zinger S, Ashwal E, Hazan L, et al. Risk factors for unintended dural puncture in obstetric patients: a retrospective cohort study. Anesth Analg 2016; 123: 972-6.
Singh S, Chaudry SY, Phelps AL, Vallejo MC. A 5-year audit of accidental dural punctures, postdural puncture headaches, and failed regional anesthetics at a tertiary-care medical center. ScientificWorldJournal 2009; 9: 715-22.
Song J, Zhang T, Choy A, Penaco A, Joseph V. Impact of obesity on post-dural puncture headache. Int J Obstet Anesth 2017; 30: 5-9.
Miu M, Paech MJ, Nathan E. The relationship between body mass index and post-dural puncture headache in obstetric patients. Int J Obstet Anesth 2014; 23: 371-5.
Peralta F, Devroe S. Any news on the postdural puncture headache front? Best Pract Res Clin Anaesthesiol 2017; 31: 35-47.
Angle P, Tang SL, Thompson D, Szalai JP. Expectant management of postdural puncture headache increases hospital length of stay and emergency room visits. Can J Anesth 2005; 52: 397-402.
Apfel CC, Saxena A, Cakmakkaya OS, Gaiser R, George E, Radke O. Prevention of postdural puncture headache after accidental dural puncture: a quantitative systematic review. Br J Anaesth 2010; 105: 255-63.
Scavone BM, Wong CA, Sullivan JT, Yaghmour E, Sherwani SS, McCarthy RJ. Efficacy of a prophylactic epidural blood patch in preventing post dural puncture headache in parturients after inadvertent dural puncture. Anesthesiology 2004; 101: 1422-7.
Stein MH, Cohen S, Mohiuddin MA, Dombrovskiy V, Lowenwirt I. Prophylactic vs therapeutic blood patch for obstetric patients with accidental dural puncture–a randomised controlled trial. Anaesthesia 2014; 69: 320-6.
Ding T, Wang DX, Qu Y, Chen Q, Zhu SN. Epidural labor analgesia is associated with a decreased risk of postpartum depression: a prospective cohort study. Anesth Analg 2014; 119: 383-92.
Suhitharan T, Pham TP, Chen H, et al. Investigating analgesic and psychological factors associated with risk of postpartum depression development: a case-control study. Neuropsychiatr Dis Treat 2016; 12: 1333-9.
Support
James R. Satalich, B.S. was supported by a Foundation for Anesthesia Education and Research Medical Student Anesthesia Research Fellowship.
Declarations of interest
None declared.
Editorial responsibility
This submission was handled by Dr. Hilary P. Grocott, Editor-in-Chief, Canadian Journal of Anesthesia.
Author contributions
Ana C. Costa designed and conducted the study, reviewed data and analyses, and drafted the manuscript. James R. Satalich, Ehab Al-Bizri, and Shivam Shodhan collected the data and critically reviewed the manuscript. Jamie L. Romeiser performed all statistical analyses and critically reviewed the manuscript. Rishimani Adsumelli critically reviewed the data and manuscript. Ramon E. Abola and Ellen S. Steinberg critically reviewed the data and manuscript. Elliot Bennett-Guerrero helped design the study and reviewed the data and manuscript.
Financial disclosures
None.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Costa, A.C., Satalich, J.R., Al-Bizri, E. et al. A ten-year retrospective study of post-dural puncture headache in 32,655 obstetric patients. Can J Anesth/J Can Anesth 66, 1464–1471 (2019). https://doi.org/10.1007/s12630-019-01486-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12630-019-01486-6