
Article summary
Author
Lucas G.H.W.
Citation
Can Anaesth Soc J 1960; 7: 237-56.
Purpose
To review the history of the early development of cyclopropane
Principal findings
Cyclopropane was initially investigated because it was thought to be the toxic element in ethylene. Instead, it turned out to be an excellent anesthetic with very rapid onset and recovery while maintaining stable hemodynamics. Its use was ultimately limited because it was highly explosive. Development required collaboration among laboratory scientists and clinicians in Toronto, Canada, clinicians in Madison, USA, and industry in both countries.
Conclusions
The phenomenal success of cyclopropane in over 40 years of clinical use resulted from a lucky, but incorrect, hypothesis that it was a toxic contaminant.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
A brief history of cyclopropane
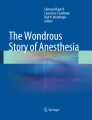
It is remarkable that profound and reversible anesthesia is reliably produced by inhalation of certain gases and vapours of volatile liquids. For its size and simplicity, cyclopropane (C3H6, molecular weight 42 g·mol−1, MAC 9.2%) is among the most potent volatile anesthetics (Figure). From 1930 to the late 1970s, cyclopropane was utilized with great success in operating rooms around the world. Were it not for tragedies due to its explosiveness, a property derived from the chemical strain inherent in its three-member carbon ring, the favourable hemodynamic profile and wide therapeutic index of cyclopropane would likely have secured its ongoing place in modern clinical practice.

Chemical structure of cyclopropane illustrating angle strain within the three-member carbon ring. The ideal bond angle for sp3-hybridized carbon is 109.5° (gray arrow). However, the carbon-carbon bond angles in cyclopropane are constrained to 60° (open arrow). This geometry yields a high chemical potential energy and gives rise to the explosiveness of the gas
The classic article by George H.W. Lucas, originally published in the June 1960 issue of the Journal (then, Canadian Anaesthetists’ Society Journal), recounts the discovery of the anesthetic properties of cyclopropane as well as the first application in patients.1 The story itself has much to teach us about the development of modern anesthesia, perseverance in the scientific method, and the value of collaboration, both with industry and the international academic medical community. It remains a classic example of serendipity.
Lucas was a chemist working in the laboratory of Professor Velyien E. Henderson (Department of Pharmacology, University of Toronto). In the course of investigations of the anesthetic properties of ethylene and propylene in 1928, Lucas hypothesized that cyclopropane was possibly a toxic contaminant in commercial propylene tanks. Much to his surprise, cyclopropane was not fatal to cats, but rather, it rapidly and reversibly anesthetized the felines with no apparent toxicity. In their original publication, Lucas and Henderson noted “a wide range between the concentration needed for surgical anesthesia (12 per cent) and the fatal concentration, (27 to 30 per cent)”, suggesting a wide therapeutic index for the gas.2 The Toronto team proceeded to human experiments - using themselves as the first subjects. Dr. W. Easson Brown, an anesthesiologist at Toronto General Hospital, had been collaborating with the team of chemists. He first delivered cyclopropane anesthesia to the principal investigator himself, Professor Henderson, followed by Lucas and several other members of the staff. Today, this experiment would make occupational health offices cringe, and it would be viewed as unethical by both institutional review boards and journals. At the time, the experiments rocketed cyclopropane from animal studies to clinical implementation.
The adoption of cyclopropane into clinical practice required several more years and an international friendship. Henderson, Brown, and Lucas were frustrated in their efforts to use cyclopropane in the operating rooms at Toronto General Hospital. The Department of Anaesthesia was reluctant to experiment with new agents given that three patients had recently died during administration of ethyl chloride. Professor Henderson then called on his friend, Dr. Ralph M. Waters, at University of Wisconsin to carry on the work. In 1930, after a brief test on a dog, Waters successfully used cyclopropane for three general surgery cases: an appendectomy, inguinal hernia repair, and cholecystectomy. Copies of these three anesthetic records, which Waters sent to Henderson, are among the gems of the 1960 article by Lucas (notice the graphs tracking depth of anesthesia as “Plane of 3d Stage” numbered one through four).1
Cyclopropane was used successfully for over forty years. Reports of use in patients for research purposes extend to at least the mid-1980s.3 Sadly, the end of cyclopropane had nothing to do with lack of quality as an anesthetic gas. While safe at inspired concentrations up to 50%, cyclopropane is extremely explosive in mixtures with oxidant gases (oxygen or nitrous oxide).4 Cyclopropane is flammable above approximately 2% (~0.2 MAC). By comparison, isoflurane is considerably safer and does not ignite below 5-7% (approximately the lethal dose).
During its history, cyclopropane was implicated in hundreds of operating room explosions in North America. Some were fatal to patients, surgeons, nurses, and anesthesiologists.5 The problem was even worse internationally, with many accidents occurring in Chile and Peru.Footnote 1 Static electricity was often the culprit. Sparks could be generated from flooring, surgical equipment, compressible anesthesia bags, or plastic tubing. John W. Severinghaus recalls a friend at the Massachusetts Institute of Technology who invented a grounding device called the “Horton Intercoupler” in response to a fatal cyclopropane explosion at the Lahey Clinic near Boston.Footnote 2 The Intercoupler was a spider-like set of wires. Each lead consisted of a clip and a megaohm resistor. The leads were attached to various pieces of operating room equipment (anesthesia machine, operating room table, etc.) and grounded to a floor plate to limit sparking that could ignite cyclopropane. While grounding methods such as conductive operating room flooring improved safety, the risk of explosions persisted. Cyclopropane thus fell out of clinical use, in part due to the advent of anesthetics such as halothane, which were less explosive and perceived to be “safer”.
A fundamentally different volatile agent
It is clear from his 1930 letter to Henderson that Waters recognized the unique anesthetic potential of cyclopropane. Was the long search for a rapidly acting, safe, complete anesthetic finally over? Nitrous oxide almost fits the bill; however, even when delivered under pressure, the intrinsic potency of nitrous oxide is too low to provide reliable surgical anesthesia at high inspired concentration without causing hypoxemia. Cyclopropane solved many problems of nitrous oxide. The potency allows easy delivery of supplemental oxygen and expands the utility of nitrous oxide.
Severinghaus describes a technique he taught at the University of California, San Francisco (UCSF) until the 1960s, which involved using a mixture of 2% cyclopropane/80% nitrous oxide for brief surgical procedures.B Induction and loss of consciousness was rapid. The depth of anesthesia was insufficient to allow endotracheal intubation, which was often foregone in those days even for abdominal and thoracic procedures. Others used cyclopropane effectively as the sole volatile agent. The potency allowed for creative induction techniques. Lawrence J. Saidman and Edmond I. Eger describe prefilling the anesthesia circuit with a 50/50 cyclopropane/oxygen mixture; patients were unconscious within two or three breaths.A, Footnote 3 Cyclopropane induction was faster than ether and less pungent to the airway.
The physical properties of cyclopropane are both a boon and a challenge. The gas is expensive to produce and store. Like nitrous oxide, cyclopropane is tanked as a liquid under pressure. Systems such as the Waters’ to-and-fro canister or low-flow circle systems were necessary to conserve gas.C Cyclopropane is also denser than air, another unique and useful feature. Bradley Smith recalls inducing children by simply holding the circuit tubing above their face.Footnote 4 The gas floats downwards, the child loses consciousness, and the anesthesiologist spares the child the fright of clamping a mask to the face.
Cyclopropane behaves in a fundamentally different way than our modern fluorinated gases with respect to the cardiovascular system.6 Waters recognized this feature after his first three deliveries of the agent. In his letter to Henderson, he wrote, “The blood pressure variations as a result of this agent… were surprisingly stable it seems to me.”1 Cyclopropane, like nitrous oxide and ether, stimulates the sympathetic nervous system. Cyclopropane and nitrous oxide have been shown to trigger a direct increase in the firing of sympathetic nerves.7,8 In healthy humans, cardiac output shows only slight depression at cyclopropane concentrations above 35%, while both peripheral vascular resistance and mean arterial pressure increase.9 Heart rate does not change, but there is a predisposition to ventricular arrhythmias.10 Given this hemodynamic profile, cyclopropane has a higher degree of cardiovascular stability than our modern fluorinated gases.A This property made it particularly useful in patients with cardiac lesions such as mitral stenosis.C Nevertheless, the sympathetic stimulation could have a paradoxical adverse effect at emergence, especially in hypovolemic patients. Rapid washout of cyclopropane can cause a precipitous drop in blood pressure during emergence that came to be known as “cyclopropane shock”.11 It remains a mystery why, at the molecular level, some inhaled anesthetics possess a sympathomimetic effect.
Lessons from the work of G.H.W. Lucas
There are many inspirational and scientific lessons to learn from Lucas’s account of the initial discovery of cyclopropane anesthesia. One of the most interesting facts is the rapidity with which Henderson and Lucas moved from animal to human studies. The first human trial of cyclopropane took Lucas only a few months to implement. In order to do this, with only minimal safety data in small mammals, they proceeded to test it on themselves. This would certainly never be allowed today but was common during the first 100 years of anesthesia.
The Lucas story foreshadows the importance of collaboration and multidisciplinary research in anesthesia. V. E. Henderson’s group was well connected. In anesthesia research, collaboration between physical scientists (chemists and physicists) and physicians is imperative. Lucas and Henderson’s close relationship with W. Easson Brown exemplifies this model. Second, communication and sharing of ideas between institutions on the international level optimizes research. When Toronto General Hospital was unable to test cyclopropane, the group reached out to Waters at the University of Wisconsin. Finally, the development of cyclopropane would not have been possible without support from industrial partners. E. R. Squibb and Sons (now Bristol-Myers Squibb) provided commercial tanks of cyclopropane for the Toronto experiments. Similarly, the Ohio Chemical Company supplied gas to Waters. These companies facilitated the development of cyclopropane as a drug by providing a high-quality expensive reagent to the investigators. Without this industry support, the experiments may well have been cost prohibitive. Contemporary anesthesia research benefits from industry support as long as the sponsor has no bias towards a specific outcome.
It was good serendipitous fortune that Lucas decided to study cyclopropane in any depth. The initial motivation of his work was to identify a toxic contaminant in a different anesthetic gas: propylene. It was observed that propylene stored in tanks caused more postoperative nausea and possibly cardiac arrhythmias when compared with freshly synthesized gas.12 Tanked propylene also had a peculiar unpleasant odour. This led V.E. Henderson’s team to search for a contaminant, which Lucas hypothesized to be cyclopropane (an isomer of propylene).1 As it turns out, the contaminants proved to be hexenes, not cyclopropane.12 It seems that the phenomenal success of cyclopropane in over 40 years of clinical use resulted from a lucky, but incorrect, hypothesis.
Key points
-
Cyclopropane was initially investigated as a toxic contaminant but found to be a very safe anesthetic.
-
Development involved multinational collaboration among basic scientists in Toronto, Canada, clinicians in Toronto and in Madison, USA, and industry in both countries.
-
There was very rapid progression from limited animal studies to human trials.
-
Cyclopropane was associated with very rapid induction, recovery, and cardiovascular stability.
-
Its explosive properties ultimately ended its over 40 years of clinical use.
Notes
Eger EI. Personal communication; 2013.
Severinghaus JW. Personal communication; 2013.
Saidman LJ. Personal communication; 2013.
Smith BE. Personal communication; 2013.
References
Lucas GH. The discovery and pharmacology of cyclopropane. Can Anaesth Soc J 1960; 7: 237-56.
Lucas GH, Henderson VE. A new anaesthetic: cyclopropane: a preliminary report. Can Med Assoc J 1929; 21: 173-5.
Munson ES, Hoffman JC, Eger EI 2nd. Use of cyclopropane to test generality of anesthetic requirement in the elderly. Anesth Analg 1984; 63: 998-1000.
MacDonald AG. A short history of fires and explosions caused by anaesthetic agents. Br J Anaesth 1994; 72: 710-22.
Walter CW. Anesthetic explosions: a continuing threat. Anesthesiology 1964; 25: 505-14.
Eger EI 2nd, Smith NT, Cullen DJ, Cullen BF, Gregory GA. A comparison of the cardiovascular effects of halothane, fluroxene, ether and cyclopropane in man: a resumé. Anesthesiology 1971; 34: 25-41.
Price HL, Warden JC, Cooperman LH, Millar RA. Central sympathetic excitation caused by cyclopropane. Anesthesiology 1969; 30: 426-38.
Ebert TJ, Kampine JP. Nitrous oxide augments sympathetic outflow: direct evidence from human peroneal nerve recordings. Anesth Analg 1989; 69: 444-9.
Cullen DJ, Eger EI 2nd, Gregory GA. The cardiovascular effects of cyclopropane in man. Anesthesiology 1969; 31: 398-406.
Price HL, Lurie AA, Jones RE, Price ML, Linde HW. Cyclopropane anesthesia. II. Epinephrine and norepinephrine in initiation of ventricular arrhythmias by carbon dioxide inhalation. Anesthesiology 1958; 19: 619-30.
Dripps RD. The immediate decrease in blood pressure seen at the conclusion of cyclopropane anesthesia: cyclopropane shock. Anesthesiology 1947; 8: 15-35.
Henderson VE, Smith AH. Propylene impurities: hexenes and hexanes. J Pharmacol Exp Ther 1936; 58: 319-27.
Acknowledgements
The authors thank Edmond I. Eger, John W. Severinghaus, Ronald D. Miller, Merlin D. Larson (all UCSF), Lawrence J. Saidman (Stanford), and Bradley E. Smith (Vanderbilt) for their thoughts, recollections, and input to the manuscript.
Funding sources
None.
Conflicts of interest
None declared.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bokoch, M.P., Gelb, A.W. From the Journal archives: Cyclopropane: induction and recovery with a bang!. Can J Anesth/J Can Anesth 61, 763–766 (2014). https://doi.org/10.1007/s12630-014-0109-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12630-014-0109-x