
Abstract
Purpose of Review
The American Board of Internal Medicine Foundation’s Choosing Wisely (CW) campaign has promoted a dialogue about avoiding unnecessary medical services since 2012. We review the evidence base, trends in utilization, and implications of CW recommendations relevant to the routine workup of newly diagnosed early stage breast cancer patients.
Recent Findings
There are several CW recommendations addressing routine workup of newly diagnosed breast cancer:
• Do not perform PET, CT, and radionuclide bone scans in the staging of early breast cancer at low risk for metastasis
- These studies are obtained in 10–20% of patients, especially those with Stage IIB disease
• Do not routinely order breast MRI in new breast cancer patients with average risk
- Evidence of long-term benefit to preoperative MRI is lacking, but approximately 1 in 4 breast cancer patients receive one, often leading to additional interventions
• Do not routinely order specialized tumor gene testing in all new breast cancer patients
- Evolving guidelines are expanding eligible populations for genetic assay driven clinical decision-making, with mixed implications for adjuvant chemotherapy utilization
• Do not routinely use sentinel node biopsy in clinically node negative women ≥ 70 years of age with hormone receptor positive invasive breast cancer
- The vast majority of such patients—85–90%— undergo sentinel node biopsy despite questions about the benefit of axillary staging in an elderly population
Summary
CW recommendations offer a useful starting point for the discussion of optimal routine workup for breast cancer. Continued efforts are needed to define the marginal value of different tests and interventions and to develop mechanisms to incentivize and measure adoption of best practices.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Breast cancer care is the largest contributor to cancer-related costs in the USA and is projected to reach $20 billion in 2020 [1]. An estimated 25% of expenditures on breast cancer care is attributed to costs of initial workup and treatment in the year following diagnosis [2]. Increased per capita spending has not resulted in distinctly better outcomes for breast cancer patients and this suggests opportunities for more cost-effective clinical decision-making [3]. Key stakeholders have increasingly sought to maximize value in breast cancer care [4, 5•, 6].
The Choosing Wisely® campaign, founded by the American Board of Internal Medicine (ABIM) Foundation and Consumer Reports in 2012, focuses on the reduction of low-value practices that lack evidence of benefit, or may even be harmful [7, 8]. This initiative solicits medical specialty organizations to identify “Top Five” potentially unnecessary practices in order to encourage a national dialogue on improving quality of care and reducing costs. Since its launch, over 75 societies have submitted nearly 500 evidence-based recommendations regarding overused tests and treatments. The American Society for Clinical Oncology (ASCO), American Society of Breast Surgeons (ASBrS), and Society for Surgical Oncology (SSO) are among the groups who have contributed recommendations specific to breast cancer care.
This review examines Choosing Wisely (CW) recommendations relevant to the routine workup of newly diagnosed, early stage breast cancer. These recommendations address advanced preoperative imaging for staging (PET, CT, bone scans, and MRI), gene expression profiling (GEP), and surgical staging of the axilla. The target population includes patients with clinically early stage disease (Stage 0–II), which accounts for more than half of cases at diagnosis [9]. We review the evidence base for these recommendations, examine trends in utilization rates, and discuss potential explanations and implications for variation in care.
Are We Choosing Wisely in the Routine Workup of New Breast Cancer Patients?
Advanced Preoperative Imaging
Do Not Perform PET, CT, and Radionuclide Bone Scans in the Staging of Early Breast Cancer at Low Risk for Metastasis (ASCO 2012)
Evidence Base
ASCO submitted their inaugural CW recommendations in 2012 [10]. This included a recommendation against obtaining advanced imaging (PET, CT, and bone scan) for early breast cancer at low risk of metastasis (Table 1). ASCO cited the 2011 National Comprehensive Cancer Network (NCCN) guidelines which stated that for patients with stage I, stage II, or T3N1M0 (stage IIIA) disease, bone scans and chest or abdominal imaging should be pursued only as indicated for specific signs or symptoms. Furthermore, NCCN recommended against PET or PET/CT for these patients based on high false-positive scan rates overall and high false-negative rates for small lesions < 1 cm [11]. Absent clinical signs or symptoms to direct imaging, the potential harms of radiation exposure and unnecessary workup of false-positive findings outweigh the limited detection of metastases, estimated at 0.2 and 1.2% in clinical stage I and II disease, respectively [35,36,37]. These are category 2A recommendations, which are based on lower-level evidence but have uniform consensus from the NCCN panel.
Utilization
There are variable estimates of advanced imaging utilization to stage newly diagnosed breast cancer patients. Prior to ASCO’s CW submission in 2012, Barcenas et al. studied a national employer-based claims database and found 12% of patients had received PET and 6.5% underwent CT during the perioperative period. The use of advanced imaging was associated with certain geographic regions, receipt of mastectomy, and eventual systemic therapy [38]. A separate analysis of advanced imaging for early (DCIS to stage II) breast cancer using the Surveillance, Epidemiology, and End Results (SEER)–Medicare linked database through 2007 found significant regional variation in imaging rates; 41.8% of studies done were contrary to the ASCO recommendation, with 80% of these being CT scans [39]. A single-center study of 200 Canadian breast cancer patients looking at the year before and after ASCO’s CW submission found 63% underwent non-concordant imaging, and almost a third of these patients received additional imaging which was negative. There was no decline in the rate of non-concordant imaging in the year following guideline release [40].
Implications
Subsequent studies have sought to clarify factors that may contribute to the use of advanced imaging. A review of 10,010 stage 0–IIB breast cancer patients in two major healthcare systems found that 15% underwent CT, PET, or bone scans between diagnosis and 30 days after surgery [41]. On chart abstraction of a sample of those having advanced imaging, 48% of studies were in response to a specific sign or symptom, with CT most frequently ordered [41]. Ramsey et al. performed a subgroup analysis of non-adherence to ASCO recommendations and found that 19% of patients with clinical stage I and 59% with clinical stage II disease underwent advanced imaging [42•].
Of 34,078 patients in the Michigan Breast Oncology Quality Initiative (MiBOQI) diagnosed with stage 0–II breast cancer (2008–2015), 20.1% underwent advanced imaging within 90 days of diagnosis [43••]. Chart abstraction was performed for all patients receiving advanced imaging in 2014–2015, and 44.9% of cases were deemed non-concordant with CW recommendations. There was significant variation across 25 clinical sites; for example, the rate of bone scans for stage 0 disease varied from 0 to 19.7%. Overall rates of advanced imaging did decrease significantly over the time for stage 0–IIA, but not for stage IIB disease.
Preoperative MRI
Do Not Routinely Order Breast MRI in New Breast Cancer Patients with Average Risk (ASBrS 2016)
Evidence Base
CW recommendations address MRI for both screening and staging in breast cancer [44, 45]. Because of a low positive predictive value of 66%, preoperative MRI for newly diagnosed breast cancer patients is controversial [15]. Advocates point to MRI as a means to detect indolent disease that can inform staging and management, while detractors note unnecessary biopsies and more aggressive surgical therapy that result from false-positive findings. The ASBrS inaugural top five list in 2016 includes a recommendation against routinely ordering breast MRI in new breast cancer patients with average risk (Table 1) [44]. ASBrS cited NCCN’s category 2B recommendation on preoperative MRI, which reflects the conflicting literature and non-uniform consensus of the panel surrounding this topic. MRI may be considered in staging of the ipsilateral or contralateral breast at time of initial diagnosis, but high-level data demonstrating improved local control or survival are lacking. NCCN guidelines also note the high rate of false-positive studies, stating that additional tissue sampling of suspicious lesions should precede surgical decision-making [12].
The impact of MRI on surgical outcomes has been demonstrated in a series of meta-analyses. These document an increased odds of mastectomy (OR 1.39–2.22) and contralateral prophylactic mastectomy (OR 1.91) following MRI, but decreased odds of re-excision after initial breast-conserving surgery (OR 0.56–0.65) [16, 46]. A separate meta-analysis of cancer-related outcomes showed no difference in local recurrence-free survival (97% MRI vs 95% no MRI) or distal recurrence-free survival (89% MRI vs 93% no MRI) [17]. A retrospective single-institution review of 755 patients undergoing breast-conserving therapy for DCIS or early stage breast cancer from 1992 to 2001 with a median follow-up of 13.8 years noted similar results, with the same local failure rate (8%) among patients receiving or not receiving preoperative MRI [47••]. Similarly, no difference was noted in 15-year overall survival (77% MRI vs 71% no MRI), freedom from distant metastases (86 vs 90%), and contralateral breast cancer (10 vs 8%) [47••].
Multiple randomized controlled trials have sought to bring clarity to the role of preoperative MRI. The COMICE trial focused on re-operation rates and found no difference (19%) between those who did and did not receive a preoperative MRI [18]. The smaller MONET trial noted an increased re-excision rate in patients who had received preoperative MRI [19]. Ongoing prospective trials are evaluating local-regional recurrence and conversion to mastectomy for those receiving and not receiving preoperative MRI (Alliance A011104/ACRIN 6694 for triple-negative and HER2-positive cancers; ECOG/ACRIN E4112 for DCIS).
Utilization
Baseline utilization of preoperative MRI has been assessed in various populations. In SEER–Medicare patients, a significant uptrend in preoperative MRI use is seen, from 0.8% in 2000 to 25.2% in 2009 [48]. Similar trends were observed in a population-based retrospective cohort in Canada, where use of preoperative MRI increased from 3% in 2003 to 24% in 2012 [49]. Younger age, higher socioeconomic status, higher Charlson comorbidity score, surgery performed in a teaching hospital, and fewer years of surgeon experience were all associated with use of MRI [49]. Use of preoperative MRI was also associated with higher likelihood of breast biopsy (OR 1.74), mastectomy (OR 1.73), contralateral prophylactic mastectomy (OR 1.48), and ≥ 30-day wait to surgery (OR 2.52) [49].
MRI utilization in community practices across five national Breast Cancer Surveillance Consortium registries nearly tripled from 4.2 to 11.5 per 1000 women (2005–2009) [50]. In a retrospective cohort of 10,518 women, there was a more than 20-fold increase in MRI use for breast cancer patients between 2000 and 2011. Of note, MRI use increased across clinical indications from 2003 to 2009 and then stabilized for screening purposes from 2009 to 2011, but has declined about 10% yearly for diagnostic or preoperative staging purposes [51].
Implications
Clinicians have demonstrated interest in the appropriate use of MRI for their patients. A qualitative survey of 377 surgeons on attitudes towards preoperative MRI found that most respondents were likely to order MRI for patients ≤ 45 years of age and those with infiltrating lobular carcinoma or triple-negative disease. However, 26% of the surgeons responded that they would obtain preoperative MRI for uncomplicated clinical stage I disease [52•]. Tan et al. reported a single-institution effort to optimize utilization of MRI for preoperative staging and high-risk screening. Consensus on appropriate use was established by a multidisciplinary breast team; in the year following implementation, high-risk screening moved from the least to most common indication for MRI, while the proportion of studies ordered for preoperative staging was cut in half [53••].
Gene-Expression Profiling
Do Not Routinely Order Specialized Tumor Gene Testing in All New Breast Cancer Patients (ASBrS 2016)
Evidence Base
Until the mid-2000s, estrogen/progesterone receptor and HER2 status were the only widely accepted genomic markers used as adjuncts to clinicopathological staging for prognosis and prediction in guiding adjuvant systemic therapy decisions [54]. This practice has resulted in the majority of estrogen receptor-positive (ER-positive), node-negative breast cancer patients being considered for adjuvant chemotherapy even though only 15% of patients who complete adjuvant hormonal therapy experience recurrence within 10 years [24]. More recently, gene-expression profiling (GEP) assays have been developed with the goal of further tailoring treatment decisions and reducing variation in the administration of chemotherapy [24, 55]. Oncotype Dx (ODX), a 21-gene assay, is the most studied and utilized GEP in the USA [56]. This test, designed for use in ER-positive, HER2-negative, node-negative invasive breast cancer, generates a recurrence score (RS) of 0 to 100, with higher scores indicating higher recurrence risk. Specifically, the addition of adjuvant chemotherapy to endocrine therapy is recommended for high-risk RS (RS > 30) while no benefit from chemotherapy is predicted for low-risk RS patients (RS < 18) [24, 57, 58].
The 2011 NCCN guidelines recommend that ODX be considered for patients with intermediate clinical risk: 0.6–1 cm tumors with unfavorable features or tumors > 1 cm in node-negative, hormone receptor-positive, HER2-negative women [11]. In 2015, Sparano and colleagues reported interim findings from the Trial Assigning Individualized Options for Treatment (TAILORx) which evaluated the value of ODX in avoiding chemotherapy for low RS patients—those with a RS < 11 who went on to receive endocrine therapy alone had 98.7% freedom from local-regional or distal recurrence at 5 years [26•]. Of note, this trial, which is also randomizing the intermediate RS group to endocrine therapy ± adjuvant chemotherapy, is using different thresholds to define risk groups than was commercially designed (low-risk RS < 11, high-risk RS > 25). The West German Study Group Phase B trial similarly reported 98% disease-free survival at 3 years for the 15.3% of hormone receptor-positive (HR-positive), pN0-1 patients for whom chemotherapy was omitted due to a low RS [30].
ASBrS’ 2016 submission to Choosing Wisely recommended against routine use of GEP for newly diagnosed breast cancer patients, highlighting the importance of understanding patient preferences before pursuing this test (Table 1) [44]. The European Group on Tumor Markers provides an excellent summary of existing guidelines with respect to different tests and clinical populations [27•]. One important discrepancy relates to use of ODX for node-positive patients. ASCO guidelines recommend against this application [28] while current NCCN guidelines allow for consideration of testing patients with involvement of 1–3 ipsilateral nodes [12], citing one retrospective series [58]. The ongoing RxPonder trial, which will conclude in 2022, is evaluating whether adjuvant chemotherapy is beneficial in this HR-positive, HER2-negative, node-positive population with a RS of 25 or less [32].
A 70-gene signature test (MammaPrint) [59] approved by the FDA solely for prognosticating risk of recurrence has also been shown to help select those who may not need chemotherapy. Early results from the MINDACT (Microarray in Node-Negative and 1 to 3 Positive Lymph Node Disease May Avoid Chemotherapy) trial showed that, among patients with high clinical risk but low genomic risk, the 5-year distal metastasis-free survival was 94.7% in those not receiving chemotherapy, which was 1.5% lower than the group receiving chemotherapy [31]. ASCO provided a focused guideline update in response, stating that MammaPrint may be used for HR-positive, HER2-negative, node-negative or positive breast cancer patients with high clinical risk to inform decisions on withholding adjuvant systemic chemotherapy [29].
Utilization
ODX, first approved by the Centers for Medicare & Medicaid Services in 2006, is the most used and studied GEP in the USA [60]. Various studies have assessed the extent of guideline-concordant use with respect to NCCN’s 2011 recommendation to consider GEP testing and chemotherapy in clinically intermediate-risk patients (ER-positive, node-negative invasive breast cancer > 1 cm). An examination of the SEER–Medicare population noted increased utilization from 1% of incident cases in 2005 to 10% in 2009 [61]. For those cases that met NCCN’s intermediate-risk criteria to consider ODX, 26% received testing [61]. For the 39% of tests outside this population, most were for T1b (> 0.5 but ≤ 1 cm) or N1 disease [61].
In the Michigan Breast Oncology Quality Initiative (MiBOQI), testing doubled from 14.7 to 27.5% between 2006 and 2008 [62]. Of tests ordered, 20% were outside NCCN’s intermediate-risk group. There was a 6.9% decrease in chemotherapy use over the study period; of note, testing increased the odds of chemotherapy for clinically low-risk patients (OR = 11.13) while decreasing odds of chemotherapy in clinically high-risk patients (OR = 0.11). These findings were replicated in a National Cancer Data Base (NCDB) study, in which 22.5% of patients received ODX testing. T1b patients were considered eligible for ODX in this study; as such, the 24% of tests that were non-concordant with NCCN guidelines were mostly ordered for node-positive or T1a disease (> 0.1 but ≤ 0.5 cm) [63••].
Implications
The rapid uptake of GEP has prompted many to study disparities associated with the use of this new and costly prognostic test. The MiBOQI study found lower odds of testing for African Americans (OR = 0.70) and those with less than a high school education (OR = 0.63) [62]. Similarly, patients from the NCDB were significantly more likely to undergo testing if they were Caucasian or lived in more educated or wealthy regions [63••].
The potential and realized impact of ODX testing on clinical decision-making is more complex. One meta-analysis found that ODX changes the clinical-pathologic recommendation for adjuvant chemotherapy for 33% of HR-positive, node-negative, early stage patients [22]. Another meta-analysis of prospective studies for early stage node-negative patients found that treatment decision changed for 29.5% of patients with an overall 12% reduction in adjuvant chemotherapy (− 16% for low RS group, + 2% for high RS group) [23]. In a propensity score-matched analysis, testing was associated with a 6.2% absolute reduction in chemotherapy (95% CI, 2.9–9.5%) [64].
Broad-based testing of all patients could drive additional chemotherapy for clinically low-risk patients, while underutilization for intermediate- to high-risk patients may forgo the benefit of avoiding chemotherapy altogether. By one estimate, almost half of clinically high-risk women may be advised to avoid chemotherapy based on ODX results [31]. These tradeoffs will become only more pertinent with discussion of extending GEP use to DCIS and node-positive patients [13].
Surgical Sampling of the Axilla
Do Not Routinely Use Sentinel Node Biopsy in Clinically Node Negative Women ≥ 70 Years of Age with Hormone Receptor-Positive Invasive Breast Cancer (SSO 2016)
Evidence Base
Surgical management of the axilla for breast cancer has evolved dramatically in the last 20 years. Appreciation of the increased morbidity of axillary lymph node dissection (ALND) prompted a shift towards minimally invasive sentinel lymph node biopsy (SLNB) for staging of clinically node-negative patients [65]. By 2004, only 36% of this cohort underwent ALND down from 94% in 1998 [66]. At the same time, the American College of Surgeons Oncology Group Z0011 (ACOSOG Z0011) randomized clinical trial has demonstrated non-inferiority of SLNB in 10-year overall and disease-free survival for women with T1 (≤ 2 cm) or T2 (> 2 to ≤ 5 cm) invasive primary breast cancer, no palpable axillary adenopathy, and 1 or 2 sentinel lymph nodes containing metastasis [67]. While SLNB has become the standard for newly diagnosed breast cancer, questions have been raised about the best approach to the axilla for older patients.
Initial investigations compared ALND to no ALND for patients ≥ 70 years old given the stark tradeoff between the morbidity of this operation and limited impact on survival for older patients. One retrospective analysis with a median follow-up of 15 years demonstrated no significant difference in mortality for patients ≥ 70 years of age with early stage, clinically node-negative disease who underwent ALND or no ALND and at least 2 years of hormonal therapy; the crude 15-year incidence of axillary disease in those not receiving axillary dissection was 5.8% [33]. The Cancer and Leukemia Group B 9343 (CALGB 9343) trial randomized women ≥ 70 years old with clinical stage I, ER-positive disease treated with lumpectomy to tamoxifen, with or without radiation therapy. In this study, among the 62% of patients who did not have ALND, no patients treated with tamoxifen plus radiation experienced axillary recurrence at a median 12.6 years of follow-up, while 3% of 200 patients receiving only tamoxifen had axillary recurrence [34]. Importantly, 98% of patients in CALGB 9343 had T1 tumors.
Chung et al. focused on SLNB in a single-institution review of 140 patients ≥ 70 years old with T1 (74%) or T2 (26%), clinically node-negative breast cancer who underwent lumpectomy without SLNB. The 5-year overall survival rate was 70%, with ischemic heart disease the most common cause of death—the 5-year breast cancer-specific survival rate was 96%. Three of five total breast cancer-related events were in triple-negative patients, and only 41% of patients received hormonal therapy although 86% were ER-positive [68]. In this context, the SSO recommended in their 2016 CW recommendations that SLNB not be routinely performed for clinically node-negative women ≥ 70 years of age with HR-positive breast cancer (Table 1) [45].
Utilization
In the North American Fareston versus Tamoxifen Adjuvant (NAFTA) trial, which completed in 2002, 93.1% of 752 enrollees underwent SLNB and had a nodal positivity rate of 16% [69]. A contemporary assessment of utilization of SLNB in patients ≥ 70 years in age with HR-positive disease using data from the NCDB from 2004 to 2013 and the Mayo Clinic Rochester from 2008 to 2016 found that 86.8 and 91.2% underwent SLNB, respectively; rates of nodal positivity were 15.2 and 14.3% [70••]. Nodal positivity increased with advancing clinical T-stage and higher-grade disease, with approximately twice the nodal positivity rate in patients with ≥T2 disease [70••].
Implications
In the context of CW for newly diagnosed breast cancer patients, the use of SLNB for patients ≥ 70 years old with HR-positive breast cancer stands out as the most routinely performed intervention. This carries significant implications for subsequent treatment decisions when nodal metastasis is found. Among 193,728 clinically node-negative, HR-positive women in the NCDB between 2013 and 2014, the 15% found to be node-positive were about five times more likely to receive chemotherapy and/or post-mastectomy radiation therapy [71]. Optimizing surgical staging of the axilla for patients over 70 years old must be a priority given this accounts for nearly one in three breast cancer diagnoses [9].
Controversy over which patients can reasonably forgo SLNB persists. The risk of understaging approximately 15% of HR-positive patients over 70 years old who will have nodal involvement is tangible. There have been numerous efforts to generate predictive models to direct this operative decision [69, 72]. A model developed from the NCDB that defined a low-risk group of grade 1/cT1mi-T1c (≤ 2.0 cm) or grade 2/cT1mi-T1b (≤ 1.0 cm) predicted nodal positivity rates of 7.8% compared with 22.3% in patients not meeting these criteria [73•]. It has also been suggested that individual life expectancy, as opposed to a chronologic age cutoff, be considered by clinicians when discussing the role of SLNB with patients [70••].
Optimizing Wise Choices: Future Directions
This review documents widespread utilization of potentially low-value services relating to the workup of newly diagnosed, early stage breast cancer patients (Table 2). Advanced imaging (CT, PET, and bone scan) is currently used for staging in 10–20% of newly diagnosed patients, particularly those with clinical node positivity and stage IIB (T2N0) disease. The use of preoperative MRI has increased to about one in four patients without evidence supporting long-term survival benefit for patients of average risk. Similarly, a quarter of newly diagnosed patients undergo gene expression profiling; this is likely to rise as applications to DCIS and node-positive populations are explored. Finally, sentinel lymph node biopsy remains an integral component of surgical therapy for early breast cancer, even for older patients who may not experience any long-term benefit from axillary staging.
A critical caveat to this discussion is the distinction between low-value services at a societal level and optimal clinical decision-making at the patient level. Most of the studies reviewed were unable, for example, to differentiate high-risk genomic patients (e.g., BRCA1/2 carriers) from average risk patients. CW guidelines should not be applied to all patients uniformly and were not intended to be used for coverage decisions. Instead, they reflect the best efforts of clinical societies to review current research and highlight services that may not be necessary for most patients.
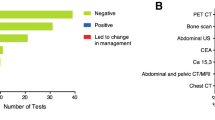
Despite these limitations, the variable utilization of low-value services suggests room to further optimize routine workup for new breast cancer patients. Patient and provider factors have been shown to impede the uptake of CW into clinical practice. A survey of breast cancer patients revealed a majority wanted low-yield imaging and would be uncomfortable if their physician did not order advanced imaging even if practice guidelines recommended against doing so [76]. Similar dynamics exist for providers when considering genomic testing. A mixed-methods examination of oncologists ordering serum tumor markers (carcinoembryonic antigen, cancer antigen 27.29, and cancer antigen 15.3) for post-treatment breast cancer surveillance found that 38% percent of stage 0–II breast cancer patients received this testing despite being contrary to 2012 ASCO recommendations [10]. Heavy users cited concerns for anxiety and need to maintain patient satisfaction. This is not surprising as patient satisfaction increasingly becomes a metric for physician reimbursement, even though there was no association identified in this study between satisfaction scores and patterns of use.
To this end, CW recommendations represent just one tool that must be paired with other innovative care redesign strategies. An ongoing trial is evaluating the effect of a statewide public reporting intervention targeting providers to reduce use of unproven or ineffective breast cancer care [77]. Others have found that public reporting of adherence to CW recommendations had limited impact on changing rates of advanced imaging for staging early breast cancer patients [78]. Ultimately, the onus remains on clinicians to incorporate Choosing Wisely recommendations into care pathways that are locally relevant, clinically credible, aligned with patient preferences, and integrated with provider workflow.
Conclusions
Choosing Wisely is a needed starting point to identify opportunities for improving value over the continuum of care. Further clinical investigations of alternative care pathways combined with innovations in reimbursement models, shared decision-making tools, medical education, and public reporting are needed to optimize care for patients with newly diagnosed breast cancer.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Mariotto AB, Robin Yabroff K, Shao Y, Feuer EJ, Brown ML. Projections of the cost of cancer Care in the United States: 2010–2020. J Natl Cancer Inst. 2011;103(2):117–28.
Yabroff KR, Lund J, Kepka D, Mariotto A. Economic burden of cancer in the United States: estimates, projections, and future research. Cancer Epidemiol Biomark Prev. 2011;20(10):2006.
Soneji S, Yang J. New analysis reexamines the value of cancer care in the United States compared to Western Europe. Health Aff. 2015;34(3):390–7. https://doi.org/10.1377/hlthaff.2014.0174.
Shih Y-CT, Ganz PA, Aberle D, Abernethy A, Bekelman J, Brawley O, et al. Delivering high-quality and affordable care throughout the cancer care continuum. J Clin Oncol. 2013;31(32):4151–7. https://doi.org/10.1200/jco.2013.51.0651.
• Schnipper LE, Davidson NE, Wollins DS, Tyne C, Blayney DW, Blum D, et al. American Society of Clinical Oncology statement: a conceptual framework to assess the value of cancer treatment options. J Clin Oncol. 2015;33(23):2563–77. https://doi.org/10.1200/jco.2015.61.6706. A useful framework developed by the ASCO Value in Cancer Care Task Force is presented to facilitate defining value in cancer care and to promote patient-physician shared decision-making.
Kang R, Goodney PP, Wong SL. Importance of cost-effectiveness and value in cancer care and healthcare policy. J Surg Oncol. 2016;114(3):275–80. https://doi.org/10.1002/jso.24331.
Morgan DJ, Dhruva SS, Wright SM, Korenstein D. 2016 update on medical overuse: a systematic review. JAMA Intern Med. 2016;176(11):1687–92. https://doi.org/10.1001/jamainternmed.2016.5381.
Brownlee S, Chalkidou K, Doust J, Elshaug AG, Glasziou P, Heath I, et al. Evidence for overuse of medical services around the world. Lancet. 2017;390(10090):156–68. https://doi.org/10.1016/S0140-6736(16)32585-5.
Breast Cancer Facts & Figures 2015–2016. Atlanta: American Cancer Society, Inc.; 2015.
Schnipper LE, Smith TJ, Raghavan D, Blayney DW, Ganz PA, Mulvey TM, et al. American Society of Clinical Oncology identifies five key opportunities to improve care and reduce costs: the top five list for oncology. J Clin Oncol. 2012;30(14):1715–24. https://doi.org/10.1200/JCO.2012.42.8375.
Carlson RW, Allred DC, Anderson BO, Burstein HJ, Carter WB, Edge SB, et al. Invasive breast cancer. J Natl Compr Cancer Netw. 2011;9(2):136–222.
(NCCN). NCCN. Breast cancer version 2.2017 NCCN clinical practice guidelines in Oncology 2017.
Rakovitch E, Nofech-Mozes S, Hanna W, Baehner FL, Saskin R, Butler SM, et al. A population-based validation study of the DCIS Score predicting recurrence risk in individuals treated by breast-conserving surgery alone. Breast Cancer Res Treat. 2015;152(2):389–98. https://doi.org/10.1007/s10549-015-3464-6.
Pilewskie M, King TA. Magnetic resonance imaging in patients with newly diagnosed breast cancer: a review of the literature. Cancer. 2014;120(14):2080–9. https://doi.org/10.1002/cncr.28700.
Houssami N, Ciatto S, Macaskill P, Lord SJ, Warren RM, Dixon JM, et al. Accuracy and surgical impact of magnetic resonance imaging in breast cancer staging: systematic review and meta-analysis in detection of multifocal and multicentric cancer. J Clin Oncol. 2008;26(19):3248–58. https://doi.org/10.1200/jco.2007.15.2108.
Houssami N, Turner R, Morrow M. Preoperative magnetic resonance imaging in breast cancer: meta-analysis of surgical outcomes. Ann Surg. 2013;257(2):249–55. https://doi.org/10.1097/SLA.0b013e31827a8d17.
Houssami N, Turner R, Macaskill P, Turnbull LW, McCready DR, Tuttle TM, et al. An individual person data meta-analysis of preoperative magnetic resonance imaging and breast cancer recurrence. J Clin Oncol. 2014;32(5):392–401. https://doi.org/10.1200/jco.2013.52.7515.
Turnbull L, Brown S, Harvey I, Olivier C, Drew P, Napp V, et al. Comparative effectiveness of MRI in breast cancer (COMICE) trial: a randomised controlled trial. Lancet. 2010;375(9714):563–71. https://doi.org/10.1016/S0140-6736(09)62070-5.
Peters NH, van Esser S, van den Bosch MA, Storm RK, Plaisier PW, van Dalen T, et al. Preoperative MRI and surgical management in patients with nonpalpable breast cancer: the MONET—randomised controlled trial. Eur J Cancer. 2011;47(6):879–86. https://doi.org/10.1016/j.ejca.2010.11.035.
MRI and mammography before surgery in patients with stage I-II breast cancer. https://ClinicalTrials.gov/show/NCT01805076.
MRI and gene expression in diagnosing patients with ductal breast cancer in situ. https://ClinicalTrials.gov/show/NCT02352883.
Carlson JJ, Roth JA. The impact of the Oncotype Dx breast cancer assay in clinical practice: a systematic review and meta-analysis. Breast Cancer Res Treat. 2013;141(1):13–22. https://doi.org/10.1007/s10549-013-2666-z.
Augustovski F, Soto N, Caporale J, Gonzalez L, Gibbons L, Ciapponi A. Decision-making impact on adjuvant chemotherapy allocation in early node-negative breast cancer with a 21-gene assay: systematic review and meta-analysis. Breast Cancer Res Treat. 2015;152(3):611–25. https://doi.org/10.1007/s10549-015-3483-3.
Paik S, Shak S, Tang G, Kim C, Baker J, Cronin M, et al. A multigene assay to predict recurrence of tamoxifen-treated, node-negative breast cancer. N Engl J Med. 2004;351(27):2817–26. https://doi.org/10.1056/NEJMoa041588.
Dowsett M, Cuzick J, Wale C, Forbes J, Mallon EA, Salter J, et al. Prediction of risk of distant recurrence using the 21-gene recurrence score in node-negative and node-positive postmenopausal patients with breast cancer treated with anastrozole or tamoxifen: a TransATAC study. J Clin Oncol. 2010;28(11):1829–34. https://doi.org/10.1200/jco.2009.24.4798.
• Sparano JA, Gray RJ, Makower DF, Pritchard KI, Albain KS, Hayes DF, et al. Prospective validation of a 21-gene expression assay in breast cancer. New Engl J Med. 2015;373(21):2005–14. https://doi.org/10.1056/NEJMoa1510764. Interim findings from the Trial Assigning Individualed Options for Treatment (TAILORx) using Oncotype Dx for patients with intermediate clinicopathologic risk. These interim findings related to patients with low-risk score (< 11) who completed endocrine therapy but no adjuvant chemotherapy; 5-year freedom from local-regional or distal recurrance was 98.7%.
• Duffy MJ, Harbeck N, Nap M, Molina R, Nicolini A, Senkus E, et al. Clinical use of biomarkers in breast cancer: updated guidelines from the European Group on Tumor Markers (EGTM). Eur J Cancer. 2017;75:284–98. https://doi.org/10.1016/j.ejca.2017.01.017. Excellent summary of current guidelines for most available biomarker assays across various clinical groups, such as node-negative/positive or HER2-negative/positive patients.
Harris LN, Ismaila N, McShane LM, Andre F, Collyar DE, Gonzalez-Angulo AM, et al. Use of biomarkers to guide decisions on adjuvant systemic therapy for women with early-stage invasive breast cancer: American Society of Clinical Oncology Clinical Practice Guideline. J Clin Oncol. 2016;34(10):1134–50. https://doi.org/10.1200/jco.2015.65.2289.
Krop I, Ismaila N, Andre F, Bast RC, Barlow W, Collyar DE, et al. Use of biomarkers to guide decisions on adjuvant systemic therapy for women with early-stage invasive breast cancer: American Society of Clinical Oncology clinical practice guideline focused update. J Clin Oncol. 2017;35(24):2838–47. https://doi.org/10.1200/jco.2017.74.0472.
Gluz O, Nitz UA, Christgen M, Kates RE, Shak S, Clemens M, et al. West German study group phase III PlanB trial: first prospective outcome data for the 21-gene recurrence score assay and concordance of prognostic markers by central and local pathology assessment. J Clin Oncol. 2016;34(20):2341–9. https://doi.org/10.1200/jco.2015.63.5383.
Cardoso F, van’t Veer LJ, Bogaerts J, Slaets L, Viale G, Delaloge S, et al. 70-gene signature as an aid to treatment decisions in early-stage breast cancer. N Engl J Med. 2016;375(8):717–29. https://doi.org/10.1056/NEJMoa1602253.
Tamoxifen citrate, letrozole, anastrozole, or exemestane with or without chemotherapy in treating patients with invasive RxPONDER breast cancer.
Martelli G, Miceli R, Daidone MG, Vetrella G, Cerrotta AM, Piromalli D, et al. Axillary dissection versus no axillary dissection in elderly patients with breast cancer and no palpable axillary nodes: results after 15 years of follow-up. Ann Surg Oncol. 2011;18(1):125–33. https://doi.org/10.1245/s10434-010-1217-7.
Hughes KS, Schnaper LA, Bellon JR, Cirrincione CT, Berry DA, McCormick B, et al. Lumpectomy plus tamoxifen with or without irradiation in women age 70 years or older with early breast cancer: long-term follow-up of CALGB 9343. J Clin Oncol. 2013;31(19):2382–7. https://doi.org/10.1200/JCO.2012.45.2615.
Brennan ME, Houssami N. Evaluation of the evidence on staging imaging for detection of asymptomatic distant metastases in newly diagnosed breast cancer. Breast. 21(2):112–23. https://doi.org/10.1016/j.breast.2011.10.005.
Smith-Bindman R, Lipson J, Marcus R, Kim KP, Mahesh M, Gould R, et al. Radiation dose associated with common computed tomography examinations and the associated lifetime attributable risk of cancer. Arch Intern Med. 2009;169(22):2078–86. https://doi.org/10.1001/archinternmed.2009.427.
Puglisi F, Follador A, Minisini AM, Cardellino GG, Russo S, Andreetta C, et al. Baseline staging tests after a new diagnosis of breast cancer: further evidence of their limited indications. Ann Oncology. 2005;16(2):263–6. https://doi.org/10.1093/annonc/mdi063.
Barcenas CH, Niu J, Valero V, Smith B, Giordano SH. Abstract P3–06-02: the use of imaging and tumor markers in the staging of patients age< 65 years with early-stage breast cancer. Cancer Res 2014;73(24 Supplement):P3-06-2.
Makarov DV, Soulos PR, Gold HT, et al. Regional-level correlations in inappropriate imaging rates for prostate and breast cancers: potential implications for the choosing wisely campaign. JAMA Oncol. 2015;1(2):185–94. https://doi.org/10.1001/jamaoncol.2015.37.
Simos D, Hutton B, Clemons M. Are physicians choosing wisely when imaging for distant metastases in women with operable breast cancer? J Oncol Pract. 2015;11(1):62–8. https://doi.org/10.1200/jop.2014.000125.
Hahn EE, Tang T, Lee JS, Munoz-Plaza C, Adesina JO, Shen E, et al. Use of imaging for staging of early-stage breast cancer in two integrated health care systems: adherence with a choosing wisely recommendation. J Oncol Pract. 2015;11(3):e320–e8. https://doi.org/10.1200/jop.2014.002998.
• Ramsey SD, Fedorenko C, Chauhan R, McGee R, Lyman GH, Kreizenbeck K, et al. Baseline estimates of adherence to American Society of Clinical Oncology/American Board of Internal Medicine Choosing Wisely initiative among patients with cancer enrolled with a large regional commercial health insurer. J Oncol Pract. 2015;11(4):338–43. https://doi.org/10.1200/jop.2014.002717. Retrospective cohort examination of adherence to all five of ASCO’s 2012 Choosing Wisely guidelines linking SEER records to 22,359 patients in Western Washington State. Across all 5 ASCO guidelines, nonadherence for this population amounted to $29 million in additional expenditure.
•• Henry NL, Braun TM, Breslin TM, Gorski DH, Silver SM, Griggs JJ. Variation in the use of advanced imaging at the time of breast cancer diagnosis in a statewide registry. Cancer. 2017;123(15):2975–83. https://doi.org/10.1002/cncr.30674. This retrospective cohort study of 34,078 patients in the Michigan Breast Oncology Quality Initiative offers an assessment of variation in use of advanced imaging studies for newly diagnosed Stage 0-II breast cancer patients. 20.1% of patients in their cohort received a CT, PET, or bone scan in the 90 days following diagnosis. This decreased over the study period except for Stage IIb patients, amounting to a 33% reduction in total imaging costs.
Landercasper J, Bailey L, Berry TS, Buras RR, Degnim AC, Fayanju OM, et al. Measures of appropriateness and value for breast surgeons and their patients: the American Society of Breast Surgeons Choosing Wisely ((R)) initiative. Ann Surg Oncol. 2016;23(10):3112–8. https://doi.org/10.1245/s10434-016-5327-8.
Society of Surgical Oncology. Five things physicians and patients should question. 2016. http://www.surgonc.org/docs/default-source/default-document-library/sso-five-things-physicians-and-patients-should-question-7-11-2016.pdf?sfvrsn=2. Accessed July 22 2017.
Houssami N, Turner RM, Morrow M. Meta-analysis of pre-operative magnetic resonance imaging (MRI) and surgical treatment for breast cancer. Breast Cancer Res Treat. 2017;165(2):273–83. https://doi.org/10.1007/s10549-017-4324-3.
•• Vapiwala N, Hwang WT, Kushner CJ, Schnall MD, Freedman GM, Solin LJ. No impact of breast magnetic resonance imaging on 15-year outcomes in patients with ductal carcinoma in situ or early-stage invasive breast cancer managed with breast conservation therapy. Cancer. 2017;123(8):1324–32. https://doi.org/10.1002/cncr.30479. This retrospective cohort study from the University of Pennsylvania followed 755 women with early stage breast cancer who underwent breast-conserving therapy and radiotherapy between 1992 and 2001. They compared 15-year outcomes between the 28% of patients who had preoperative MRI and those who did not, finding no significant difference in overall survival, freedom from distant metastasis, and contralateral breast cancer.
Killelea BK, Long JB, Chagpar AB, Ma X, Soulos PR, Ross JS, et al. Trends and clinical implications of preoperative breast MRI in Medicare beneficiaries with breast cancer. Breast Cancer Res Treat. 2013;141(1):155–63. https://doi.org/10.1007/s10549-013-2656-1.
Arnaout A, Catley C, Booth CM, et al. Use of preoperative magnetic resonance imaging for breast cancer: a Canadian population-based study. JAMA Oncol. 2015;1(9):1238–50. https://doi.org/10.1001/jamaoncol.2015.3018.
Wernli KJ, DeMartini WB, Ichikawa L, Lehman CD, Onega T, Kerlikowske K, et al. Patterns of breast magnetic resonance imaging use in community practice. JAMA Intern Med. 2014;174(1):125–32. https://doi.org/10.1001/jamainternmed.2013.11963.
Stout NK, Nekhlyudov L, Li L, Malin ES, Ross-Degnan D, Buist DS, et al. Rapid increase in breast magnetic resonance imaging use: trends from 2000 to 2011. JAMA Intern Med. 2014;174(1):114–21. https://doi.org/10.1001/jamainternmed.2013.11958.
• Morrow M, Hawley ST, McLeod MC, Hamilton AS, Ward KC, Katz SJ, et al. Surgeon attitudes and use of MRI in patients newly diagnosed with breast cancer. Ann Surg Oncol. 2017;24(7):1889–96. https://doi.org/10.1245/s10434-017-5840-4. Survey of 377 breast surgeons which identified high and low MRI users via SEER registry and linked this to perceptions about MRI use. A quarter said they would obtain MRI for Stage I disease. High utilizers had significantly higher surgical volume and significantly more misconceptions about MRI benefits.
•• Tan S, David J, Lalonde L, El Khoury M, Labelle M, Younan R, et al. Breast magnetic resonance imaging: are those who need it getting it? Curr Oncol. 2017;24(3):e205–e13. https://doi.org/10.3747/co.24.3441. Excellent example from Quebec of operationalizing current evidence into best practice guidelines for MRI use in breast cancer patients, particularly for high-risk screening and preoperative staging. This involved a consensus meeting of the multisciplinary breast team followed by implementation of a new ordering form based on the consensus guidelines. In the year following implementation, use of MRI for preoperative staging dropped from 18 to 9% of studies even as total MRIs performed increased.
Harris L, Fritsche H, Mennel R, Norton L, Ravdin P, Taube S, et al. American Society of Clinical Oncology 2007 update of recommendations for the use of tumor markers in breast cancer. J Clin Oncol. 2007;25(33):5287–312. https://doi.org/10.1200/jco.2007.14.2364.
Buyse M, Loi S, van't Veer L, Viale G, Delorenzi M, Glas AM, et al. Validation and clinical utility of a 70-gene prognostic signature for women with node-negative breast cancer. J Natl Cancer Inst. 2006;98(17):1183–92. https://doi.org/10.1093/jnci/djj329.
Oncotype DX for breast cancer. http://www.genomichealth.com/en-US/oncotype_iq_products/oncotype_dx.aspx. Accessed 11 Dec 2017.
Paik S, Tang G, Shak S, Kim C, Baker J, Kim W, et al. Gene expression and benefit of chemotherapy in women with node-negative, estrogen receptor-positive breast cancer. J Clin Oncol. 2006;24(23):3726–34. https://doi.org/10.1200/jco.2005.04.7985.
Albain KS, Barlow WE, Shak S, Hortobagyi GN, Livingston RB, Yeh IT, et al. Prognostic and predictive value of the 21-gene recurrence score assay in postmenopausal women with node-positive, oestrogen-receptor-positive breast cancer on chemotherapy: a retrospective analysis of a randomised trial. Lancet Oncol. 2010;11(1):55–65. https://doi.org/10.1016/s1470-2045(09)70314-6.
Mammaprint 70-gene breast cancer recurrence assay http://www.agendia.com/healthcare-professionals/breast-cancer/mammaprint/. Accessed December 11 2017.
Trosman JR, Van Bebber SL, Phillips KA. Coverage policy development for personalized medicine: private payer perspectives on developing policy for the 21-gene assay. J Oncol Pract. 2010;6(5):238–42. https://doi.org/10.1200/JOP.000075.
Dinan MA, Mi X, Reed SD, Hirsch BR, Lyman GH, Curtis LH. Initial trends in the use of the 21-gene recurrence score assay for patients with breast cancer in the medicare population, 2005-2009. JAMA Oncol. 2015;1(2):158–66. https://doi.org/10.1001/jamaoncol.2015.43.
Hassett MJ, Silver SM, Hughes ME, Blayney DW, Edge SB, Herman JG, et al. Adoption of gene expression profile testing and association with use of chemotherapy among women with breast cancer. J Clin Oncol. 2012;30(18):2218–26. https://doi.org/10.1200/jco.2011.38.5740.
•• Orucevic A, Heidel RE, Bell JL. Utilization and impact of 21-gene recurrence score assay for breast cancer in clinical practice across the United States: lessons learned from the 2010 to 2012 National Cancer Data Base analysis. Breast Cancer Res Treat. 2016;157:427–35. https://doi.org/10.1007/s10549-016-3833-9. Retrospective examination of genetic expression profile use from 2010–2012 in the National Cancer Data Base, which captures ~ 70% of new diagnoses in the USA annually. Oncotype Dx accounted for 94% of ordered tests, with about 1 in 5 ER-positive patients receiving testing.
Ray GT, Mandelblatt J, Habel LA, Ramsey S, Kushi LH, Li Y, et al. Breast cancer multigene testing trends and impact on chemotherapy use. Am J Manag Care. 2016;22(5):e153–e60.
Lucci A, McCall LM, Beitsch PD, Whitworth PW, Reintgen DS, Blumencranz PW, et al. Surgical complications associated with sentinel lymph node dissection (SLND) plus axillary lymph node dissection compared with SLND alone in the American College of Surgeons Oncology Group Trial Z0011. J Clin Oncol. 2007;25(24):3657–63. https://doi.org/10.1200/jco.2006.07.4062.
Rescigno J, Zampell JC, Axelrod D. Patterns of axillary surgical care for breast cancer in the era of sentinel lymph node biopsy. Ann Surg Oncol. 2009;16(3):687–96. https://doi.org/10.1245/s10434-008-0195-5.
Giuliano AE, Ballman KV, McCall L, Beitsch PD, Brennan MB, Kelemen PR, et al. Effect of axillary dissection vs no axillary dissection on 10-year overall survival among women with invasive breast cancer and sentinel node metastasis: the ACOSOG Z0011 (alliance) randomized clinical trial. JAMA. 2017;318(10):918–26. https://doi.org/10.1001/jama.2017.11470.
Chung A, Gangi A, Amersi F, Zhang X, Giuliano A. Not performing a sentinel node biopsy for older patients with early-stage invasive breast cancer. JAMA Surg. 2015;150(7):683–4. https://doi.org/10.1001/jamasurg.2015.0647.
Chagpar AB, McMasters KM, Edwards MJ. Can sentinel node biopsy be avoided in some elderly breast cancer patients? Ann Surg. 2009;249(3):455–60. https://doi.org/10.1097/SLA.0b013e318194d16b.
•• Boughey JC, Haffty BG, Habermann EB, Hoskin TL, Goetz MP. Has the time come to stop surgical staging of the axilla for all women age 70 years or older with hormone receptor-positive breast cancer? Ann Surg Oncol. 2017;24(3):614–7. https://doi.org/10.1245/s10434-016-5740-z. A discussion of the role of surgical staging of the axilla in patients 70 years or older accompanies contemporary estimates of axillary surgery in this population using the National Cancer Data Base (2004–2013 with 86.8% having axillary staging) and Mayo Clinic Rochester (2008–2016 with 91.% having axillary staging). Authors make note of the clinical need to distinguish age and life expectancy.
Chagpar AB, Horowitz N, Sanft T, Wilson LD, Silber A, Killelea B, et al. Does lymph node status influence adjuvant therapy decision-making in women 70 years of age or older with clinically node negative hormone receptor positive breast cancer? Am J Surg. 2017;214(6):1082–8. https://doi.org/10.1016/j.amjsurg.2017.07.036.
Greer LT, Rosman M, Charles Mylander W, Liang W, Buras RR, Chagpar AB. A prediction model for the presence of axillary lymph node involvement in women with invasive breast cancer: a focus on older women. Breast J. 2014;20(2):147–53. https://doi.org/10.1111/tbj.12233.
• Welsh JL, Hoskin TL, Day CN, Habermann EB, Goetz MP, Boughey JC. Predicting nodal positivity in women 70 years of age and older with hormone receptor-positive breast cancer to aid incorporation of a society of surgical oncology choosing wisely guideline into clinical practice. Ann Surg Oncol. 2017;24(10):2881–8. https://doi.org/10.1245/s10434-017-5932-1. A clinical and multivariate predictive model was developed from the National Cancer Data Base for hormone-receptor positive, node-negative women 70 years or older. Those who met a clinical rule for avoiding axillary surgery—grade 1, cT1mi-T1c, or grade 2, cT1mi-T1b—were almost three times less likely to have nodal positivity (7.8%) compared to those not meeting the criteria (22.3%).
Onega T, Tosteson ANA, Weiss J, Alford-Teaster J, Hubbard RA, Henderson LM, et al. Costs of diagnostic and preoperative workup with and without breast MRI in older women with a breast cancer diagnosis. BMC Health Serv Res. 2016;16:76. https://doi.org/10.1186/s12913-016-1317-6.
Roberts MC, Weinberger M, Dusetzina SB, Dinan MA, Reeder-Hayes KE, Carey LA, et al. Racial variation in the uptake of oncotype DX testing for early-stage breast cancer. J Clin Oncol. 2016;34(2):130–8. https://doi.org/10.1200/jco.2015.63.2489.
Simos D, Hutton B, Graham ID, Arnaout A, Caudrelier J-M, Mazzarello S, et al. Patient perceptions and expectations regarding imaging for metastatic disease in early stage breast cancer. SpringerPlus. 2014;3(1):176. https://doi.org/10.1186/2193-1801-3-176.
Pezzin LE, Laud P, Neuner J, Yen TW, Nattinger AB. A statewide controlled trial intervention to reduce use of unproven or ineffective breast cancer care. Contemp Clin Trials. 2016;50:150–6. https://doi.org/10.1016/j.cct.2016.08.005.
Bedford C, Arnaout A, Anas R, Catley C, Clemons M, Earle C, et al. Driving quality improvement with public reporting: use of imaging tests outside guidelines for early-stage breast cancer in Ontario. J Clin Oncol. 2017;35(8_suppl):193. https://doi.org/10.1200/JCO.2017.35.8_suppl.193.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no competing interests.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
This article is part of the Topical Collection on Local-Regional Evaluation and Therapy
Rights and permissions
About this article

Cite this article
Trooboff, S.W., Kang, R., Margenthaler, J. et al. Choosing Wisely: Optimizing Routine Workup for the Newly Diagnosed Breast Cancer Patient. Curr Breast Cancer Rep 10, 62–73 (2018). https://doi.org/10.1007/s12609-018-0268-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12609-018-0268-9