
Abstract
Home garden interventions combining training in agriculture and nutrition have the potential to increase vegetable production and consumption in lower-income countries, but there remains a need for better evidence for impact. This study contributes to filling this gap by evaluating the impact and distributional effects of a home garden intervention in Cambodia. We used a cluster randomized controlled trial with before and after data for a sample of 500 rural households with children under five and women 16–49 years old. Impact was estimated using analysis of covariance (ANCOVA) and conditional quantile regressions with non-parametric bounds. The results show that the intervention significantly increased the adoption of nearly all promoted gardening methods. More households (+ 35%; p < 0.01) produced vegetables, and the production period was extended by five months on average. One-month recall data show an increase in vegetables harvested (+ 25 kg; p < 0.01) and consumed (+ 10 kg; p < 0.01) from the garden. Quantile regressions confirm these findings and show that nearly all households benefitted, but households that were already doing better at baseline tended to benefit more. Seven-day recall data show an increase in the quantity of vegetables consumed (+ 61 g/day/capita; p < 0.01) and an increased quantity of vitamin A, folate, iron, and zinc contained in these vegetables. Women contributed more to the garden work than men and their time spent in the garden increased by 29 min/day on average. These results add further evidence that integrated home garden interventions can contribute to nutrition outcomes and that almost all participants can benefit.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
Home gardens make an important contribution to the food and nutrition security of poor rural households in developing countries, but they are often overlooked in research and agricultural extension (Castañeda-Navarrete, 2021; Lal, 2020; Rybak et al., 2018; Schreinemachers et al., 2018; Tesfamariam et al., 2018). Despite their importance, common home gardens are not always very productive, suffering from neglect, insect pests and diseases, and general poor crop and soil management. Experience shows that many of these issues can be resolved with relative ease through hands-on training in garden management. If bundled with nutrition education, this can be a powerful tool to increase small-scale vegetable production and consumption among households most vulnerable to micronutrient malnutrition (Galhena et al., 2013; Iannotti et al., 2009; Weinberger, 2013).
Evidence is accumulating for the impact of home garden interventions (Bird et al., 2019; Ruel & Alderman, 2013; Ruel et al., 2018; Weinberger, 2013). A review of home gardens found 15 peer-reviewed journal papers in English that had studied its impact in developing countries (DFID, 2014). Ten of these 15 papers showed that home garden interventions increased household production and consumption of micronutrient-rich foods, and seven reported an improvement in micronutrient status. However, there remains a lack of high-quality evaluation designs using randomized controlled trials (DFID, 2014; Ruel et al., 2018) and some authors have questioned whether home gardens benefit the poorest of the poor (Pritchard et al., 2019) or can be sustained (Muñoz-Rodríguez et al., 2020; Nordhagen et al., 2019).
Recent impact evaluations of integrated home garden interventions have started to close this gap. In Bangladesh, a study showed that a home garden intervention significantly increased household vegetable production and consumption and that its effects were sustained at least three years after intervention support ended (Baliki et al., 2019; Schreinemachers et al., 2015, 2016). In Nepal, a randomized controlled trial (RCT) study showed that a home garden intervention reduced anemia among mothers and children (Osei et al., 2016). Another RCT study in Nepal showed that home gardens combined with school gardens significantly increased home garden productivity and the frequency of children's vegetable consumption (Schreinemachers et al., 2020). In Burkina Faso, an RCT study showed that a home garden project improved hemoglobin levels among children in one of two tested nutrition outreach designs (Olney et al., 2015). Yet, an RCT study of a home garden intervention in Tanzania, Kenya and Uganda showed an increase in the share of households producing vegetables and an extended production period in Tanzania, but not in Kenya and Uganda (Depenbusch et al., 2021).
This study adds to this literature by conducting an RCT of an integrated home garden-nutrition intervention in Cambodia. The study traces the whole chain of causal effects from people's participation in training events to technology adoption to increased production and consumption. More specifically, the study tests the hypothesis that an integrated home garden intervention—combining hands-on training in gardening with nutrition behavior change communication and targeted at poor rural households with children under five years and women of reproductive age—increases the production and consumption of nutrient-dense vegetables for the average household as well as those households most vulnerable to low vegetable consumption.
According to data from the Global Burden of Disease study, the mean vegetable consumption per person in Cambodia is about 91 g/day (Afshin et al., 2019). This is well below the estimated optimal of 360 g/day recommended by the same study as well as the recommendation of the World Health Organization of 3 portions a day (~ 240 g) (WHO/FAO, 2003). This challenge is not unique to Cambodia, as low vegetable consumption is a dietary risk factor that affects 90% of low-income and 83% of lower-middle-income countries globally (Afshin et al., 2019). Vegetable production in Cambodia is highly seasonal as it is challenging to grow vegetables during the monsoon and dry seasons.
The prevalence of hunger in Cambodia was 6% in 2020, but 45% of the population is severely or moderately food insecure, and about one-third of children under the age of five are stunted (FAO et al., 2021). Amongst mothers and children, the effects of food insecurity compound with poor eating and breastfeeding practices. A study of Phnom Penh and two rural provinces found that less than 25% of children aged 6–24 months met minimum acceptable diets, and low measures of the mid-upper arm circumference indicated malnutrition among 21% of pregnant women (Som et al., 2018). Marginal blood levels of provitamin A and deficient blood levels of folate and zinc amongst women and children are of particular concern (National Institute of Statistics et al., 2015; Wieringa et al., 2016).
Previously, Olney et al. (2009) studied the impact of the integrated homestead food production program of Helen Keller International (HKI) in Cambodia using pre- and post-intervention data for 500 households. They found that the program increased the production and consumption of micronutrient-rich foods, but there were no significant improvements in maternal and child health and nutrition. However, their treatment was not randomized and their baseline and endline data were collected in different seasons and over different samples of households—preventing them to apply a difference-in-difference (DD) or analysis of covariance (ANCOVA) estimator to control for selection bias. Dragojlovic et al. (2020) evaluated the effect of the HKI homestead food production program in Cambodia in a pragmatic field test, which showed positive effects on the production of fruits and livestock and the micronutrient intake of children. However, the control and intervention data were collected in different years and the study had a large sample attrition in the intervention group that was not controlled for.
Verbowski et al. (2018) used endline data from an RCT in Cambodia to quantify the impact of home garden interventions with and without an aquaculture component on nutrient intake. Without aquaculture, they found significant effects on women's intake of vitamin A and zinc, but no effects on other nutrients and among children. Using the same data and applying a DD estimator, Michaux et al. (2019) found no effects on anemia in women or stunting, wasting, and underweight in children but a significant effect on anemia in children.
2 Methods and data
2.1 Intervention studied
The intervention studied here was implemented as part of a home garden scaling project funded by the United States Agency for International Development (USAID) and implemented by the World Vegetable Center and local partners in Cambodia. The primary aim of the project was to improve the nutritional status of small children and women of childbearing age. The project reached 3,507 households in the provinces of Battambang, Kampong Thom, Pursat, and Siem Reap.
Home gardens as a source of fruits, vegetables, herbs, and spices are common in rural Cambodia, and they play an important role in the livelihood of women (Nguyen et al., 2016). Traditionally garden tasks fall in women's domain, but men contribute as well, especially to some of the "heavier" tasks. Rural people value their gardens as they allow them to save money from having to buy vegetables, offer a small income opportunity, and provide vegetables that have not been sprayed with pesticides.
The intervention promoted household vegetable supply and demand in parallel, which is a common element of most home garden interventions (World Vegetable Center, 2016). The supply-side component aimed at increasing the availability of a diverse range of vegetables. A total of 272 demonstration gardens were established in the yards of lead gardeners and used for monthly community-based training sessions and informal visits by other households in the villages to learn about new varieties and appropriate gardening methods. Garden manuals were distributed to the households and training videos were shared through YouTube. Participants received seed packages of a set of nutritious and culturally accepted vegetables, including amaranth, bitter gourd, choy sum (Brassica rapa var. parachinensis), bok choy (Brassica rapa var. chinensis), chili, water spinach (Ipomoea aquatica), Chinese kale, Malabar spinach (basella alba), yard long bean, pumpkin, tomato, and okra. Commercially available varieties were used so that households could acquire the seed after project support ended. Technical backstopping and advice were provided by extension staff to each household about twice a month. Support was provided for one year.
The demand-side component consisted of providing nutrition information and raising people's awareness about the importance of nutritious diets for children and the family as a whole. It included awareness-raising through discussions and posters in villages, group training, personal visits by NGO staff, and cooking demonstrations with new recipes.
The theory of change builds upon the mutually reinforcing influence of training in gardening and nutrition. Nutrition training is expected to raise people's interest in eating vegetables and thereby increase the motivation to maintain a garden, eat its produce, and diversify the household diet. The agricultural training is expected to promote techniques that make it easier for households to successfully sustain a more extensive garden, increase the diversity of vegetables grown, and extend the production period. The larger quantity and diversity of vegetables produced over a longer period of the year, enables the household to eat more vegetables and a greater diversity of them. Income from selling surplus vegetables and reduced expenditures on buying vegetables could further improve the household diet if the additional income is used to buy other nutritious food items. Home gardens might also benefit and empower women if they gain more control over resources and the income from the garden. However, garden work can also burden women if they are already time-constrained.
Households eligible for receiving support had to: (a) have at least one child below the age of 5 or one woman of reproductive age; (b) have land close to their house unaffected by seasonal flooding and not shaded for most of the day; (c) have access to a reliable source of water throughout the year and; (d) show willingness to participate in the project and to produce vegetables for household consumption. Households had two weeks to identify a suitable space of at least 6 × 6 m and prepare the land for establishing the garden.
2.2 Randomized controlled trial design
Figure 1 shows the consort flow diagram for the study. Random allocation to a control and treatment group was done at the village level to reduce the likelihood of spillover effects between treatment and control (de Janvry et al., 2011). Power calculations suggested an appropriate sample size of 600 households, split equally between treatment and control. The primary respondent was the person managing the home garden or the person most likely to manage it. Questions about food consumption were asked to the person in charge of food preparation.

Consort flow diagram for the study; Percentages behind the sample size indicate the share of households included, compared to the planned sample size
The baseline survey took place in May 2017 and the endline was conducted one year later. The baseline survey provided data for 296 control and 295 treatment households. Sample attrition between baseline and endline was 12% for the treatment group and 19% for the control. Reasons for attrition included migration and refusal to participate. Only households with complete data on the outcome variables for baseline and endline were used in the analysis.
Before each interview, enumerators explained the purpose of the study to the respondents and asked for their verbal consent. Participation in the study was considered to impose no risks to the participants while providing a potentially large opportunity for improved nutrition to those in the treatment group. The study complied with relevant laws and institutional guidelines, but there was no option for an institutional ethical review at the World Vegetable Center before the establishment of a review board in 2018.
We quantified the average treatment effect (ATE), which is the average change in outcomes for the treatment group controlling for changes in the control group. This is a so-called “intent-to-treat analysis” as all households assigned to treatment or control are included in the analysis. Autocorrelation in the outcome variables is limited, with only one variable reaching a value larger than 0.5. Therefore, ANCOVA is preferred over DD as it provides estimates with a much lower variance (McKenzie, 2012). ANCOVA corrects for initial differences in outcomes, based on the observed effect of the baseline on endline values. In the given case with two time periods, the model is specified as:
where Yi, t is the outcome variable for household i at time t. Ti indicates whether a household is in the treatment or control group and εit is a mean-zero error term. As a robustness check, and to facilitate comparison to other studies, we also estimate the average treatment effect using a DD model, which assumes that the average change in the control group represents the counterfactual change in the treatment group in the absence of the project and is specified as:
where vt separates the observations between baseline and endline.
Sample attrition was found to be non-random (p = 0.022) and a source of possible bias. Therefore, we used inverse probability weights as suggested by Gertler et al. (2016). The method assigns weights to observations based on their likelihood of being dropped from the sample; giving larger weights to households underrepresented in the endline. Weights were estimated from a logit model regressing attrition status on baseline household characteristics.Footnote 1
For continuous variables, equations were estimated using weighted least squares (WLS). A probit regression was used for binary outcomes, while a poisson regression was used for count variables if these fitted a poisson distribution (otherwise, WLS was used). Inverse probability weights were applied to all regressions and standard errors and p-values were cluster-adjusted. The degrees of freedom were set to the number of villages in the sample, as recommended by Angrist and Pischke (2009).
2.3 Quantile regression
Conditional quantile regression (Koenker & Bassett, 1978; Koenker & Hallock, 2001) was used to confirm the results of the WLS estimates and assess distributional effects. Quantile regression provides more reliable estimates than WLS if outcomes deviate from a normal distribution and is more robust to outliers. Quantile treatment effects (QTE) show how the status of a certain point in the distribution changes, conditional on being in the control or treatment group. The QTE can be estimated at any point in the distribution, but we estimated it for the upper limit of each quartile (i.e., the 25th, 50th, and 75th percentile). Quantile regressions were estimated using the endline data with treatment status included as covariate.
To account for potential sample attrition bias, we constructed upper and lower non-parametric bounds around the estimates (Lee, 2009). The method assumes that households in the control group do not have a lower likelihood of attrition than treatment households (Huber & Mellace, 2015). Standard errors were estimated using a blocked bootstrap approach with blocks defined as villages. The 95% confidence interval (CI) of the expected mean was calculated from these standard errors following Imbens and Manski (2004).
2.4 Outcome variables
Noninvasive and straightforward to measure outcome variables were selected along the intervention's impact pathway from technology adoption to an increase in year-round vegetable production, eventually leading to a greater volume and diversity of vegetable consumption. The primary outcomes are: (a) the number of different vegetable species consumed during the last seven days and their source (own garden, bought, other sources); and (b) dietary diversity quantified by recording all foods that the household ate or drank in the previous 24 h and organized in 16 food groups (Swindale & Bilinsky, 2006). We quantified the Household Dietary Diversity Score (HDDS) and the Individual Dietary Diversity Score (IDDS) for children aged 12 to 59 months following Swindale and Bilinsky (2006) and the Women's Dietary Diversity Score (WDDS) for women 16–49 years of age following FAO (2010). The HDDS is an indicator of household socioeconomic status rather than nutritional status. The IDDS and WDDS are indicators for nutrient intake and designed as population-level indicators.
Vegetable quantities, as recorded over a 7-day period, were also converted to nutrient values for provitamin A, folate, and zinc, for which there are known deficiencies in the Cambodian population (National Institute of Statistics et al., 2015; Wieringa et al., 2016). We also included iron, as it is a common target of nutrition interventions, although iron-deficiency anemia in Cambodia is compounded by hemoglobin disorders, hookworm infections, and other micronutrient deficiencies (Wieringa et al., 2016; National Institute of Statistics et al., 2015; Karakochuk et al., 2014). Nutrient conversion factors were taken from the dietary nutrient databases of Hulshof et al. (2019) and USDA (2016), with additions from MEXT (2015), Khan et al. (2007), and World Vegetable Center nutrition division. Comparisons to estimated average requirements (EAR) are based on Institute of Medicine (1998) and (2001).
The primary outcomes are assumed to be driven by an increase in garden production, which was measured as: (a) the number of different vegetable species produced over a 12-month period, split between species produced for selling and species produced for home consumption; (b) months in which vegetables were harvested from the home garden over a 12-month period as an indicator of year-round production; (c) the quantity of vegetables harvested in the last 30 days (converted from local units to kgs) and usage (home consumed, shared, sold); and (d) the revenues obtained from selling vegetables in the last 30 days (converted to US dollars).
Increased production, in turn, is assumed to be driven by changes in garden management, including: (a) the adoption of improved vegetable production methods taught in the training, such as the use of animal manure, raised planting beds, and mulches; (b) the size of the area allocated to vegetable production (expressed in square meters—sqm) and (c) time spent on vegetable production by male and female household members in minutes per day on average.
Previous studies have shown that home garden interventions can contribute to women's empowerment (Baliki et al., 2019; Patalagsa et al., 2015; van den Bold et al., 2015). We included a simple measure of women's empowerment based on a set of 13 statements. These statements were asked to a woman (the primary respondent or the spouse). The statements were divided into three categories of "decision-making", referring to women's ability to make decisions for their own and their household, "leadership", referring to their ability to participate in the community and voice their opinion, and "autonomy", referring to their control over their own time. Respondents answered how much they agreed on a five-point Likert scale, ranging from "strongly agree" to "strongly disagree". The values were expressed as a score from 0 to 1, with a higher score meaning more empowerment. Additionally, we asked about the time men and women had spent in the home garden, as an increased workload might affect women's well-being and ability to care for other household members (Patalagsa et al., 2015).
3 Results
3.1 Baseline characteristics and balance
The average household in the sample had 5.5 persons and owned 1.6 hectares (ha) of agricultural land (Table 1). More respondents in the treatment than in the control were women. Households in the treatment also owned more livestock, were more likely to produce vegetables, produced vegetables for a longer period of the year, and consumed a greater diversity of home-produced vegetables. It thus appeared that the treatment group had a slightly better performance in terms of vegetable production at baseline. Such differences could bias the impact estimates. It is noted that the mean vegetable consumption at baseline, as estimated using a 7-day recall, is slightly above the WHO/FAO recommendation.
3.2 Exposure
All households in the treatment group had participated in at least one production training and 96% had participated in the nutrition training. On average, households had participated in 8.7 of the 12 training events offered with 29% having attended all events.
3.3 Adoption of garden practices
The use of all 16 garden practices covered in the training increased significantly, except for chemical fertilizer use (Table 2), which may be because of the increased use of compost (+ 48 percentage points) and animal manure (+ 40 percentage points), which are alternative fertilizers. Own seed saving was likely affected by free handouts of packaged seeds during the project period (+ 52 percentage points) and therefore increased only a little (+ 12 percentage points). Unfortunately, there was also a significant increase in the use of chemical pesticides (+ 12 percentage points), which had not been promoted and is an unintended adverse effect of the intervention. However, the use of homemade and natural pesticides increased more (+ 34 percentage points), and so did the use of crop rotation (+ 49 percentage points).
3.4 Garden size and length of production
The intervention increased the average size of home gardens by 36 sqm, which is the size of the promoted standard design (Table 3). It had no significant effect on the total vegetable area, including plots used for commercial vegetable production. Yet, the quantile regression, which is less sensitive to outliers, shows a significant increase in the total vegetable area as well as the home garden area (Table 4). At the first quartile, representing households with no home garden, the intervention increased the garden size by 30 sqm; yet the effect was larger for the third quartile.
The intervention increased the proportion of households growing vegetables by 35 percentage points (Table 3). In line with this, the intervention increased the mean period of vegetable production by five months. These effect sizes are partly driven by a reduction in the control group (which also contributes to the large increase in the share of households producing vegetables). Figure 2 shows the seasonality of vegetable production. It shows that a large share of households in the control group did not grow vegetables in the endline. There was a small but positive effect on nutritional knowledge (+ 2.14 percentage points; p < 0.10). Households produced about six more vegetable species for home consumption and two more species for selling.

Share of households producing vegetables per month at baseline and endline. Shaded areas indicate months with challenging conditions for growing vegetables due to flooding (Sep-Oct) and hot-dry conditions (Mar-Apr). Weighted averages; N = 500
3.5 Effect on production during the last one-month period
The surveys were conducted in early May, which refers to the hot-dry period when it is challenging to produce vegetables, as shown in Fig. 2. Yet, if households in the treatment group would be able to show an increase in garden production during this month, then we could conclude with more confidence that the intervention enabled year-round production.
The results in Table 5 show a significant increase in the proportion of households producing vegetables (+ 45 percentage points). Again, the effect is mostly because of a reduction in the control group. The average quantity of vegetables produced from the garden increased by 25 kg, which is more than double the baseline mean. Including commercial plots, average vegetable production increased by 62 kg. The intervention increased the quantity of home-produced vegetables for own consumption during the preceding month by 10.5 kg over a baseline mean of 9.7 kg—a 108% increase. This corresponds to an additional supply of 63 g per capita per day.
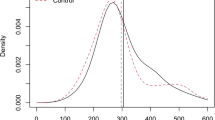
Quantile regressions show that almost all households significantly increased vegetable production and consumption (Fig. 3). The treatment effects are significant for all but the lowest decile, with higher deciles gaining more. The impact on home garden production is 41 kg higher for the third quartile than that for the first quartile (Table 4). The results are about the same when restricting the analysis to home gardens. The impact on consumption at the third quartile is 29 kg higher than at the first. The increase in vegetable production did not translate into higher revenues from vegetable selling for the average household (Table 5), although the effect was positive and significant for the third quartile (Table 4).

Quantile regression treatment effects on the quantity of vegetables produced (diagram A) and quantity of vegetables consumed (diagram B) during a one-month period (April 2018). Shaded area shows 95%-confidence intervals with non-parametric bounds. Standard errors block-bootstrapped. X-axis shows cumulative % of households sorted in ascending order on the outcome variable at baseline. X-axis restricted to lower 80% of households as wide confidence-intervals at 9th decile reduce readability of Y-axis. N = 500
3.6 Consumption during the last seven days
Analysis of the consumption data, recorded for a 7-day recall period, shows a 0.25 kg increase in the quantity of vegetables consumed per household, which corresponds to a mean increase of 61 g per person per day (Table 6). The diversity of vegetable species consumed did not change. The increase in the share of vegetables coming from the home garden is also associated with reduced expenditure on buying vegetables. Total food expenditures did not change. The quantile regressions confirm a positive effect on the share of vegetables from the own garden (Table 7). The other effects are statistically insignificant.
In terms of micronutrients, calculated from the consumed quantity of vegetables, there is a significant increase (ranging from 16 to 24% over baseline values), as shown in Table 6. Households with comparably low consumption of folate and vitamin A rich vegetables (i.e., those at the first quartile of these distributions) were able to increase their availability of and access to these micronutrients (Table 7).Footnote 2 At the median, only the effect on vitamin A consumption increased and there was no significant effect for the third quartile.
Assuming that vegetables are shared equally among household members, the additional supply of vitamin A contributes 16.1% of EAR for the first quartile of children 4–8 years and 8.0% of the EAR of pregnant adult women. For folate, the additional supply per person represents 9.5% of the EAR for children and 2.9% for pregnant women.
3.7 Dietary diversity
The results show no significant effect on the HDDS—an indicator of socioeconomic status (Table 8). At baseline, 93% of the households had consumed vegetables during the previous 24 h, which left little room for improvement. There was also no significant effect on the IDDS and WDDS.
3.8 Gender
The intervention had no significant effect on women's control over vegetable production (Table 9). However, this result might be biased as it can only be calculated for 297 households that produced vegetables in both years. Yet, our simple indicator of women's empowerment, which uses data for 400 households, also shows no significant effect, at least not in the short-term.
A well-managed home garden may increase the time-burden for household members. At the baseline, women spent on average 22 min/day on the home garden and men spent 18 min/day. The intervention significantly increased women's time in the garden by 29 min/day and men's time by 17 min/day. The difference is weakly significant, indicating that women's workload increased more than men's. The median woman worked 30 more minutes and at the third quartile the extra work was 60 min (Table 10). In contrast, the median man did not increase his workload in the garden while this was an extra 30 min at the third quartile. This shows that the increase in time spent on the garden was mostly supplied by women.
3.9 Robustness check
Impact evaluation using the DD method instead of the ANCOVA method provided similar results (Tables 11, 12, 13, 14, 15 16). However, the impact estimates of the ANCOVA method generally had a higher level of significance and for all but nine variables the effect size was also larger. Using the DD method, fewer variables were significant at the 90% confidence level or higher, especially among the consumption indicators from the 7-day recall data.
4 Discussion
4.1 Reflection on the key findings
The results of this study show that an integrated home garden intervention in Cambodia significantly increased the production and consumption of vegetables for the average household selected into the intervention. We showed a chain of effects from training participation to the increased use of garden practices, which gave households a better ability to grow a diverse range of vegetables year-round and led to increased production even during the dry-season. This increased the supply of vegetables for home consumption during a one-month period around April–May, resulting in increased vegetable consumption and an increased consumption of micronutrients from vegetables as measured using a 7-day recall. The 24-h recall data showed no effect on dietary diversity. Most households already consumed vegetables before the program started and the program did not add new food categories to the daily diet. The positive effect on vegetable consumption confirms the improvements observed in a similar intervention in Cambodia (Michaux et al., 2019; Verbowski et al., 2018). The successful improvement of production during the dry season suggests that participants had sufficient access to irrigation, which can be a major impediment to home gardens (Hirvonen & Headey, 2018).
The study also identified some possible adverse effects such as increased use of chemical pesticides, which is not recommended for home gardens and usually also not needed because home gardens have a high diversity of plants and many insect pests can be controlled by hand-picking or natural pesticides such as plant extracts. Also, blemished produce can be accepted when used for home-consumption. Another finding was that the participants invested considerable time in the gardens. Men and women often worked together, but women contributed more time. The substantial increase in time-use goes beyond earlier observations of an increase by just six to seven minutes (Schreinemachers et al., 2016). This is something that warrants further study as it may impede on the sustainability of home gardens and limit women's empowerment.
There was no evidence for an effect on women's empowerment, at least not in the first year of the intervention. An in-depth qualitative gender study of the early phase of the project identified several possible explanations; for instance, many of the trainers were men, not all training events were convenient for women to attend, and participatory training methods could have been used more extensively (Nguyen et al., 2016). It is also possible that the endline study was conducted too early as empowerment takes longer to materialize through a home garden intervention. In any case, the non-significant effect on empowerment contradicts some previous studies that have found evidence of gradual improvements in women's empowerment (Patalagsa et al., 2015; van den Bold et al., 2015; Hillenbrand, 2010; Baliki et al., 2019).
Results of the quantile regressions show that almost all households were able to increase their vegetable production and their usage for consumption; however, treatment effects varied much. The lower quartile benefitted from increased vegetable production and consumption, but the higher quartiles benefitted more. Yet, the effects on nutrient availability from vegetables showed that households with a low intake of these nutrients benefitted more than households with a higher intake. This is at least partially due to a higher variation and high levels of vegetable consumption at baseline. As these households already reach the required consumption levels, there is less scope for improvement. While Baliki et al. (2019) and, to a lesser degree Depenbusch et al. (2021) also find the lowest levels of vegetable consumption to improve, their results do not indicate larger gains among participants with higher baseline consumption.
With regard to the methods, the ANCOVA results were generally supported by DD results, but more outcomes turned significant using ANCOVA. This appears to be mainly driven by the higher efficiency of the ANCOVA estimator, which is a well-understood advantage over DD (McKenzie, 2012). The larger effect sizes with ANCOVA are caused by a different correction for baseline differences between the treatment arms in the two models. The parallel paths assumption of the DD approach implies that the absolute difference between the treatment groups would have been preserved in absence of the treatment. The ANCOVA method assumes that the baseline value of a variable affects the endline value in both groups by the same factor. If this coefficient is below one, then the counterfactual is a reduced difference between the treatment groups (Kisbu-Sakarya et al., 2012). Combined with higher baseline values in the treatment group and positive treatment effects, this results in higher treatment effects. As we do not know the pre-treatment trends for the variables, we cannot judge which approach is better.
4.2 Strengths and weaknesses of the study
The use of a randomized controlled trial to quantify the impact of a home garden intervention is a clear strength of the study. The application of quantile regressions provides novel insights into the distribution of benefits and makes the results more robust. Another strength of the study is that it evaluated impact at a scaling stage, which gives a more realistic estimation of the effect size than when evaluating impact at a pilot stage when a relatively large amount of resources is spent on a relatively small number of households. In contrast to other studies, we focused on the causal chain of effects along the hypothesized impact pathway from training participation to dietary diversity, which allows identifying bottlenecks in the implementation as discussed in the next section. We focused on dietary diversity, food intake, and nutrient intake as they are more feasible and plausible targets for an agricultural project. We did not analyze the effect on nutritional status (e.g., stunting and wasting) as done by some other studies (Michaux et al., 2019; Olney et al., 2009, 2015). We think that the links between better diets and health outcomes are already well understood, while health outcomes are influenced by many other factors outside the scope of this intervention.
We used dietary diversity as one of our outcome variables, but it proved not very suitable because most households (> 90%) already consumed vegetables at the baseline, which limited the scope for impact. Another key weakness of our study is that data on vegetable consumption and dietary diversity were collected only once and referred to a period that is challenging for vegetable production. The estimated impact might have been different (likely to be higher) in another period of the year. Collecting data in multiple seasons is challenging but should be considered in future impact studies of home gardens. We also note that our 7-day recall method appears to have overestimated per capita vegetable consumption at baseline as the amount is rather high (Table 6). The collection of 24-h recall data should have been repeated at regular intervals, which is practically challenging. Another weakness is that there was only one year between baseline and endline—risking that some short-term effects may not be sustained without support. Furthermore, we experienced high sample attrition between baseline and endline and a sizeable intra-cluster correlation for some variables, which in combination, may reduce the detectable effect size. Lastly, as we used only quantitative methods, the study could not capture the potentially important cultural functions of home gardens and how interactions between the project design and local culture affected the measured impact (Trefry et al., 2014).
5 Conclusion
Integrated home garden interventions, combining training in vegetable gardening and nutrition, increase household-level vegetable production and consumption, as this study confirmed for Cambodia. The intervention increased not only the quantity of vegetables produced and consumed but also the diversity of production and the length of the production season. However, we did not find a significant effect on dietary diversity scores, measured using a 24 h recall method.
The degree to which households benefitted from the home garden intervention varied with their initial status. Households that initially produced and consumed more vegetables were able to increase production and consumption more, indicating a need to provide stronger support to less endowed households. However, the results also clearly showed that households with low access to nutritious vegetables were able to improve their vegetable consumption and increase their intake of vitamin A and folate from vegetables. This is important because micronutrient malnutrition and low vegetable consumption are key health risks in Cambodia and many other lower-income countries. Home gardens are an effective intervention to improve this. Our study provides further evidence on the effect size that can be expected from such intervention and the considerable co-investment of time that they require from men and especially women. Time-saving techniques should be a priority in the intervention design to ensure the long-term sustainability of the gardens.
Availability of data and material
Data are available from https://worldveg.tind.io/record/74439.
Code availability
Data were analyzed with the software package Stata 13.1. The code is available on request.
Notes
Covariates used: treatment assignment; livestock value; other household assets value; respondent age; household size; children below five; children 5–17 years; dummies for vegetable production, own employment income, and remittances. Covariates selected from a larger set of variables using the Akaike information criterion. Weights were applied using the svy-set of commands in Stata.
When controlling for baseline levels the effect on vitamin A at the first quartile loses significance at the 5% confidence level. At baseline, the intake of vitamin A from vegetables at the first quartile was on average 918 mcg/RAE/day and the intake of folate was 305 mcg/day.
References
Afshin, A., Sur, P. J., Fay, K. A., Cornaby, L., Ferrara, G., Salama, J. S. et al. (2019). Health effects of dietary risks in 195 countries, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. The Lancet, 393(10184), 1958–1972. https://doi.org/10.1016/S0140-6736(19)30041-8
Angrist, J. D., Pischke, J. S. (2009). Mostly harmless econometrics : An empiricist’s companion. Princeton University Press.
Baliki, G., Brück, T., Schreinemachers, P., & Uddin, M. N. (2019). Long-term behavioural impact of an integrated home garden intervention: Evidence from Bangladesh. Food Security. https://doi.org/10.1007/s12571-019-00969-0
Bird, F. A., Pradhan, A., Bhavani, R. V., & Dangour, A. D. (2019). Interventions in agriculture for nutrition outcomes: A systematic review focused on South Asia. Food Policy, 82, 39–49. https://doi.org/10.1016/j.foodpol.2018.10.015
Castañeda-Navarrete, J. (2021). Homegarden diversity and food security in southern Mexico. Food Security, 13(3), 669–683. https://doi.org/10.1007/s12571-021-01148-w
de Janvry, A., Dunstan, A., & Sadoulet, E. (2011). Recent Advances in Impact Analysis Methods for Ex-post Impact Assessments of Agricultural Technology: Options for the CGIAR. Rome, Italy: Independent Science and Partnership Council Secretariat.
Depenbusch, L., Schreinemachers, P., Roothaert, R., Namazzi, S., Onyango, C., Bongole, S. et al. (2021). Impact of home garden interventions in East Africa: Results of three randomized controlled trials. Food Policy, 104, 102140. https://doi.org/10.1016/j.foodpol.2021.102140
DFID. (2014). Can agriculture interventions promote nutrition: Agriculture and nutrition evidence paper. Department for International Development.
Dragojlovic, N., Michaux, K. D., Moumin, N. A., Li, K. H., Talukder, Z., Hou, K. et al. (2020). Economic evaluation of an enhanced homestead food production intervention for undernutrition in women and children in rural Cambodia. Global Food Security, 24, 100335. https://doi.org/10.1016/j.gfs.2019.100335
FAO. (2010). Guidelines for measuring household and individual dietary diversity. FAO.
FAO, IFAD, UNICEF, WFP & WHO. (2021). The State of Food Security and Nutrition in the World 2021. Transforming food systems for food security, improved nutrition and affordable healthy diets for all. Rome, Italy: FAO.
Galhena, D. H., Freed, R., & Maredia, K. M. (2013). Home gardens: A promising approach to enhance household food security and wellbeing. Agriculture & Food Security, 2(1), 8. https://doi.org/10.1186/2048-7010-2-8
Gertler, P., Martinez, S., Premand, P., Rawlings, L. B., & Vermeersch, C. M. J. (2016). Impact evaluation in practice (Second (Edition). World Bank Group.
Hillenbrand, E. (2010). Transforming gender in homestead food production. Gender & Development, 18(3), 411–425. https://doi.org/10.1080/13552074.2010.521987
Hirvonen, K., & Headey, D. (2018). Can governments promote homestead gardening at scale? Evidence from Ethiopia. Global Food Security, 19, 40–47. https://doi.org/10.1016/j.gfs.2018.09.001
Huber, M., & Mellace, G. (2015). Sharp Bounds on Causal Effects under Sample Selection. Oxford Bulletin of Economics and Statistics, 77(1), 129–151. https://doi.org/10.1111/obes.12056
Hulshof, P., Doets, E., Seyha, S., Bunthang, T., Vonglokham, M., Kounnavong, S. et al. (2019). Food Composition Tables in Southeast Asia: The Contribution of the SMILING Project. Maternal and Child Health Journal, 23(1), 46–54. https://doi.org/10.1007/s10995-018-2528-8
Iannotti, L., Cunningham, K., & Ruel, M. (2009). Diversifying into healthy diets: Homestead food production in Bangladesh. In D. J. Spielman, & R. Pandya-Lorch (Eds.), Millions fed : proven successes in agricultural development. Washington, DC: International Food Policy Research Institute.
Imbens, G. W., & Manski, C. F. (2004). Confidence Intervals for Partially Identified Parameters. Econometrica, 72(6), 1845–1857. https://doi.org/10.1111/j.1468-0262.2004.00555.x
Institute of Medicine. (1998). Dietary reference intakes for thiamin, riboflavin, niacin, vitamin B6, folate, vitamin B12, pantothenic acid, biotin, and choline. Food and Nutrition Board, Institute of Medicine.
Institute of Medicine. (2001). Dietary reference intakes for vitamin A, vitamin K, arsenic, boron, chromium, copper, iodine, iron, manganese, molybdenum, nickel, silicon, vanadium, and zinc. Food and Nutrition Board, Institute of Medicine.
Karakochuk, C. D., Whitfield, K. C., Barr, S. I., Lamers, Y., Devlin, A. M., Vercauteren, S. M. et al. (2014). Genetic Hemoglobin Disorders Rather Than Iron Deficiency Are a Major Predictor of Hemoglobin Concentration in Women of Reproductive Age in Rural Prey Veng. Cambodia. the Journal of Nutrition, 145(1), 134–142. https://doi.org/10.3945/jn.114.198945
Khan, N. C., Dao, H. T. A., Dung, L., Lam, N., Mai, L., & Sy, N. (2007). Vietnamese food composition Table. Medical, Hanoi.
Kisbu-Sakarya, Y., MacKinnon, D. P., & Aiken, L. S. (2012). A Monte Carlo Comparison Study of the Power of the Analysis of Covariance, Simple Difference, and Residual Change Scores in Testing Two-Wave Data. Educational and Psychological Measurement, 73(1), 47–62. https://doi.org/10.1177/0013164412450574
Koenker, R., & Bassett, G. (1978). Regression Quantiles. Econometrica, 46(1), 33–50. https://doi.org/10.2307/1913643
Koenker, R., & Hallock, K. F. (2001). Quantile Regression. Journal of Economic Perspectives, 15(4), 143–156. https://doi.org/10.1257/jep.15.4.143
Lal, R. (2020). Home gardening and urban agriculture for advancing food and nutritional security in response to the COVID-19 pandemic. Food Security, 12(4), 871–876. https://doi.org/10.1007/s12571-020-01058-3
Lee, D. S. (2009). Training, Wages, and Sample Selection: Estimating Sharp Bounds on Treatment Effects. The Review of Economic Studies, 76(3), 1071–1102. https://doi.org/10.1111/j.1467-937X.2009.00536.x
McKenzie, D. (2012). Beyond baseline and follow-up: The case for more T in experiments. Journal of Development Economics, 99(2), 210–221. https://doi.org/10.1016/j.jdeveco.2012.01.002
MEXT. (2015). Stanadard Tables of Food Composition in Japan 2015 (Seventh Revised Edition). Tokyo, Japan: Council for Science and Technology, Ministry of Education, Culture, Sports, Science and Technology.
Michaux, K. D., Hou, K., Karakochuk, C. D., Whitfield, K. C., Ly, S., Verbowski, V. et al. (2019). Effect of enhanced homestead food production on anaemia among Cambodian women and children: A cluster randomized controlled trial. Maternal & Child Nutrition, 15(S3), e12757. https://doi.org/10.1111/mcn.12757
Muñoz-Rodríguez, M., Fernández-González, C., Aguilar-Gallegos, N., & González-Santiago, M. V. (2020). The Primacy of Politics in Public Food Security Policies: The Case of Home Gardens. Sustainability, 12(10). https://doi.org/10.3390/su12104316
National Institute of Statistics, Directorate General for Health & ICF International. (2015). Cambodia Demographic and Health Survey 2014. Phnom Penh, Cambodia, and Rockville Maryland, USA: National Institute of Statistics, Directorate General for Health, and ICF International.
Nguyen, H., Ly, S., Biskupska, N., Pravalprukskul, P., Brown, S., Ro, A. et al. (2016). Understanding gender and power relations in home garden activities: Empowerment and sustainable home garden uptake: World Vegetable Center, Taiwan. Publication number 17–813.
Nordhagen, S., Thiam, K., & Sow, S. (2019). The sustainability of a nutrition-sensitive agriculture intervention: A case study from urban Senegal. Food Security, 11(5), 1121–1134. https://doi.org/10.1007/s12571-019-00948-5
Olney, D. K., Pedehombga, A., Ruel, M. T., & Dillon, A. (2015). A 2-year integrated agriculture and nutrition and health behavior change communication program targeted to women in Burkina Faso reduces anemia, wasting, and diarrhea in children 3–12.9 months of age at baseline: a cluster-randomized controlled trial. The Journal of Nutrition, 145(6), 1317–1324. https://doi.org/10.3945/jn.114.203539
Olney, D. K., Talukder, A., Iannotti, L. L., Ruel, M. T., & Quinn, V. (2009). Assessing Impact and Impact Pathways of a Homestead Food Production Program on Household and Child Nutrition in Cambodia. Food and Nutrition Bulletin, 30(4), 355–369. https://doi.org/10.1177/156482650903000407
Osei, A., Pandey, P., Nielsen, J., Pries, A., Spiro, D., Davis, D. et al. (2016). Combining Home Garden, Poultry, and Nutrition Education Program Targeted to Families With Young Children Improved Anemia Among Children and Anemia and Underweight Among Nonpregnant Women in Nepal. Food and Nutrition Bulletin, 38(1), 49–64. https://doi.org/10.1177/0379572116676427
Patalagsa, M. A., Schreinemachers, P., Begum, S., & Begum, S. (2015). Sowing seeds of empowerment: effect of women’s home garden training in Bangladesh. Agriculture & Food Security, 4(1). https://doi.org/10.1186/s40066-015-0044-2
Pritchard, B., Vicol, M., Rammohan, A., & Welch, E. (2019). Studying home gardens as if people mattered: Why don’t food-insecure households in rural Myanmar cultivate home gardens? The Journal of Peasant Studies, 46(5), 1047–1067. https://doi.org/10.1080/03066150.2018.1431623
Ruel, M. T., & Alderman, H. (2013). Nutrition-sensitive interventions and programmes: How can they help to accelerate progress in improving maternal and child nutrition? The Lancet, 382(9891), 536–551. https://doi.org/10.1016/S0140-6736(13)60843-0
Ruel, M. T., Quisumbing, A. R., & Balagamwala, M. (2018). Nutrition-sensitive agriculture: What have we learned so far? Global Food Security, 17, 128–153. https://doi.org/10.1016/j.gfs.2018.01.002
Rybak, C., Mbwana, H. A., Bonatti, M., Sieber, S., & Müller, K. (2018). Status and scope of kitchen gardening of green leafy vegetables in rural Tanzania: Implications for nutrition interventions. Food Security, 10(6), 1437–1447. https://doi.org/10.1007/s12571-018-0869-1
Schreinemachers, P., Baliki, G., Shrestha, R. M., Bhattarai, D. R., Gautam, I. P., Ghimire, P. L. et al. (2020). Nudging children toward healthier food choices: An experiment combining school and home gardens. Global Food Security, 26, 100454. https://doi.org/10.1016/j.gfs.2020.100454
Schreinemachers, P., Brown, S., Roothaert, R., Makamto Sobgui, C., & Toure, S. H. (2018). Research to impact: the World Vegetable Center's household garden model. 305–314. https://doi.org/10.17660/ActaHortic.2018.1205.36
Schreinemachers, P., Patalagsa, M. A., Islam, M. R., Uddin, M. N., Ahmad, S., Biswas, S. C., et al. (2015). The effect of women’s home gardens on vegetable production and consumption in Bangladesh. Food Security, 7(1), 97–107. https://doi.org/10.1007/s12571-014-0408-7
Schreinemachers, P., Patalagsa, M. A., & Uddin, N. (2016). Impact and cost-effectiveness of women’s training in home gardening and nutrition in Bangladesh. Journal of Development Effectiveness, 8(4), 473–488. https://doi.org/10.1080/19439342.2016.1231704
Som, S. V., Prak, S., Laillou, A., Gauthier, L., Berger, J., Poirot, E. et al. (2018). Diets and Feeding Practices during the First 1000 Days Window in the Phnom Penh and North Eastern Districts of Cambodia. Nutrients, 10(4). https://doi.org/10.3390/nu10040500
Swindale, A., & Bilinsky, P. (2006). Household Dietary Diversity Score (HDDS) for Measurement of Household Food Access: Indicator Guide (v.2). Washington, D.C.: FHI 360/FANTA.
Tesfamariam, B. Y., Owusu-Sekyere, E., Emmanuel, D., & Elizabeth, T. B. (2018). The impact of the homestead food garden programme on food security in South Africa. Food Security, 10(1), 95–110. https://doi.org/10.1007/s12571-017-0756-1
Trefry, A., Parkins, J. R., & Cundill, G. (2014). Culture and food security: A case study of homestead food production in South Africa. Food Security, 6(4), 555–565. https://doi.org/10.1007/s12571-014-0362-4
USDA. (2016). USDA National Nutrient Database for Standard Reference. (Vol. Release 28): US Department of Agriculture, Agricultural Research Service, Nutrient Data Laboratory.
van den Bold, M., Dillon, A., Olney, D., Ouedraogo, M., Pedehombga, A., & Quisumbing, A. (2015). Can Integrated Agriculture-Nutrition Programmes Change Gender Norms on Land and Asset Ownership? Evidence from Burkina Faso. The Journal of Development Studies, 51(9), 1155–1174. https://doi.org/10.1080/00220388.2015.1036036
Verbowski, V., Talukder, Z., Hou, K., Sok Hoing, L., Michaux, K., Anderson, V. et al. (2018). Effect of enhanced homestead food production and aquaculture on dietary intakes of women and children in rural Cambodia: A cluster randomized controlled trial. Maternal & Child Nutrition, 14(3), e12581. https://doi.org/10.1111/mcn.12581
Weinberger, K. (2013). Home and community gardens in Southeast Asia: Potential and opportunities for contributing to nutrition-sensitive food systems. Food Security, 5(6), 847–856. https://doi.org/10.1007/s12571-013-0299-z
WHO/FAO. (2003). Diet, nutrition and the prevention of chronic diseases. Report of a Joint FAO/WHO Expert Consultation. WHO Technical Report Series 916. Geneva: World Health Organization.
Wieringa, F. T., Dahl, M., Chamnan, C., Poirot, E., Kuong, K., Sophonneary, P. et al. (2016). The High Prevalence of Anemia in Cambodian Children and Women Cannot Be Satisfactorily Explained by Nutritional Deficiencies or Hemoglobin Disorders. Nutrients, 8(6), 348. https://doi.org/10.3390/nu8060348
World Vegetable Center. (2016). The World Vegetable Center approach to household gardening for nutrition. Shanhua, Taiwan: World Vegetable Center.
Acknowledgements
Funding for this research was provided by the United States Agency for International Development (USAID) under the project “Deploying Vegetable Seed Kits to Tackle Malnutrition in Cambodia, Kenya, Liberia, Tanzania and Uganda” (AID-BFS-IO-12–00,004) and long-term strategic donors to the World Vegetable Center: Taiwan, UK Aid from the UK government, USAID, Australian Centre for International Agricultural Research (ACIAR), Germany, Thailand, Philippines, Korea, and Japan. We acknowledge the essential work of all colleagues involved in the project implementation and data collection. We are grateful to all survey participants for the time and effort they dedicated to our interviews.
Funding
Funding for this research was provided by the United States Agency for International Development (USAID) under the project “Deploying Vegetable Seed Kits to Tackle Malnutrition in Cambodia, Kenya, Liberia, Tanzania and Uganda” (AID-BFS-IO-12–00004) and long-term strategic donors to the World Vegetable Center: Taiwan, UK Aid from the UK government, USAID, Australian Centre for International Agricultural Research (ACIAR), Germany, Thailand, Philippines, Korea, and Japan.
Author information
Authors and Affiliations
Contributions
Lutz Depenbusch: Methodology, Formal Analysis, Data Curation, Writing – Original Draft; Pepijn Schreinemachers: Conceptualization, Methodology, Writing – Original Draft, Supervision; Stuart Brown: Investigation, Project administration, Writing – Review & Editing; Ralph Roothaert: Project administration, Writing – Review & Editing.
Corresponding author
Ethics declarations
Conflicts of interest
The authors declare no conflict of interest in the preparation of this paper.
Appendix
Appendix
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Depenbusch, L., Schreinemachers, P., Brown, S. et al. Impact and distributional effects of a home garden and nutrition intervention in Cambodia. Food Sec. 14, 865–881 (2022). https://doi.org/10.1007/s12571-021-01235-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12571-021-01235-y